
Impact of Interleukin-17 Inhibitor Therapy on Arterial Intima-media Thickness among Severe Psoriatic Patients


 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Assessment of Clinical and Ultrasonographic Responsiveness
2.2. Administration of Anti-IL-17 Therapies
2.3. Evaluation of Data
3. Results
3.1. Patient Characteristics
3.2. Patients’ Comorbidities
3.3. Clinical Findings
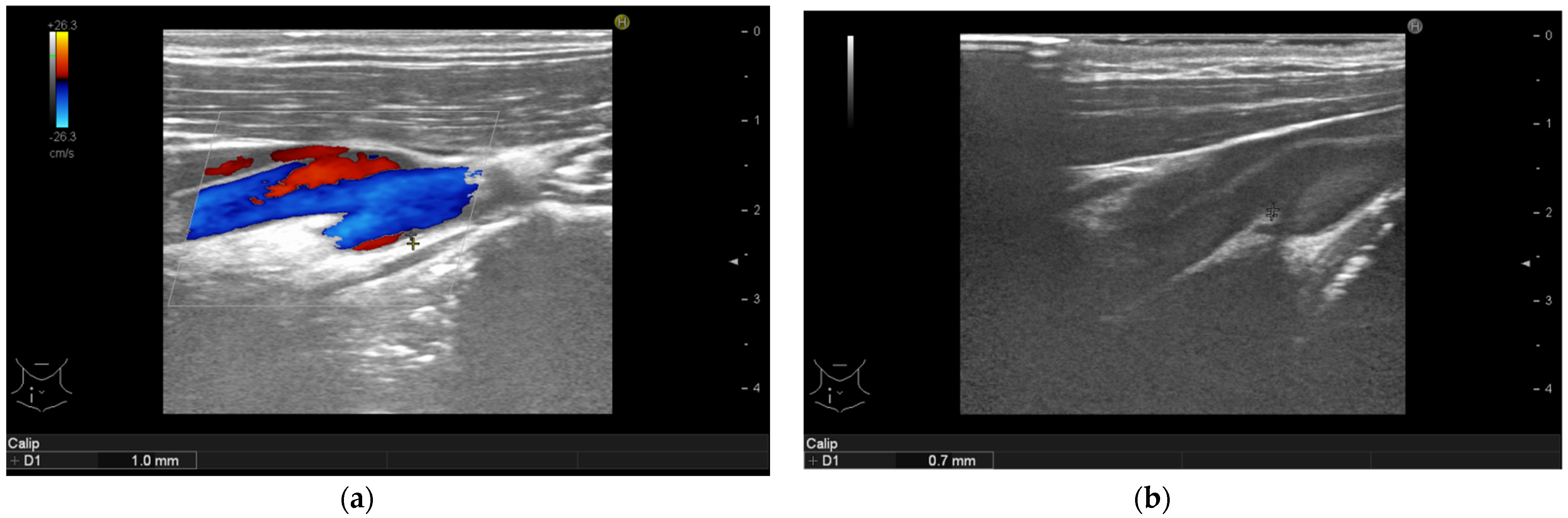
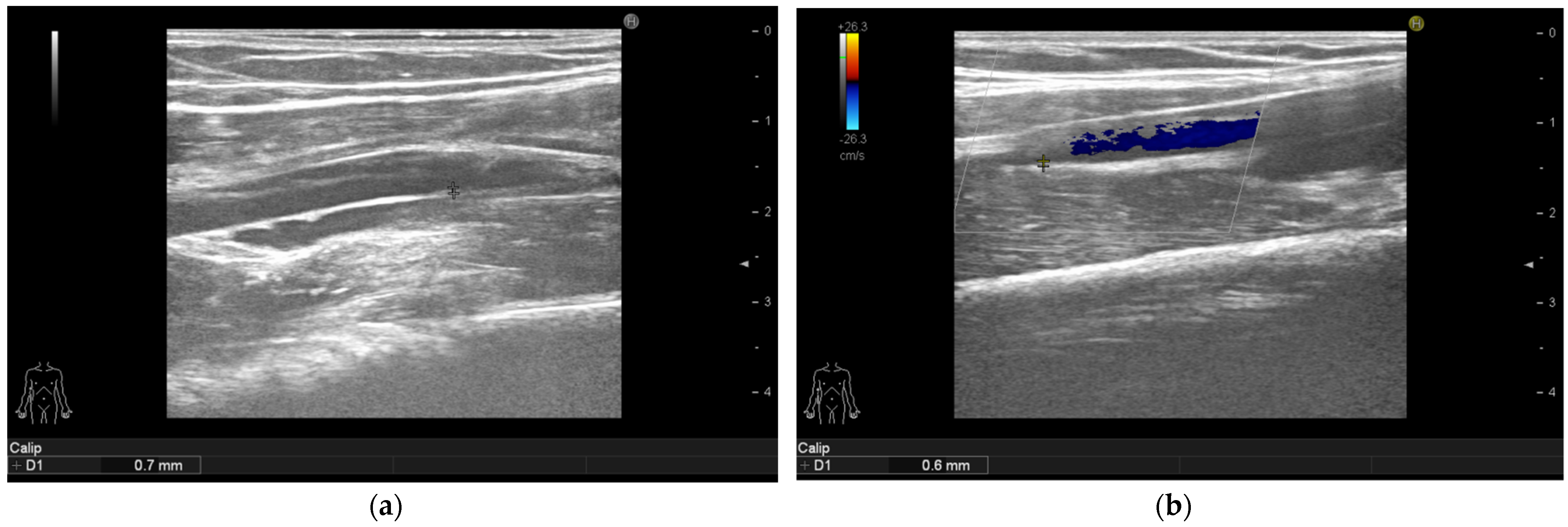
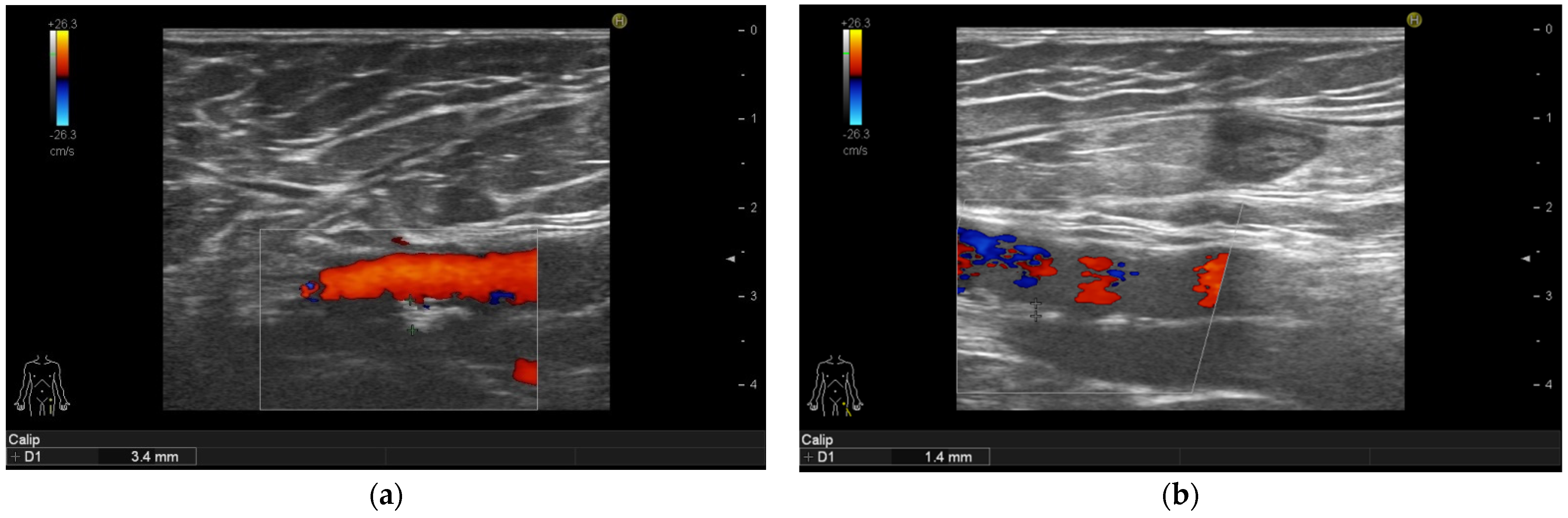
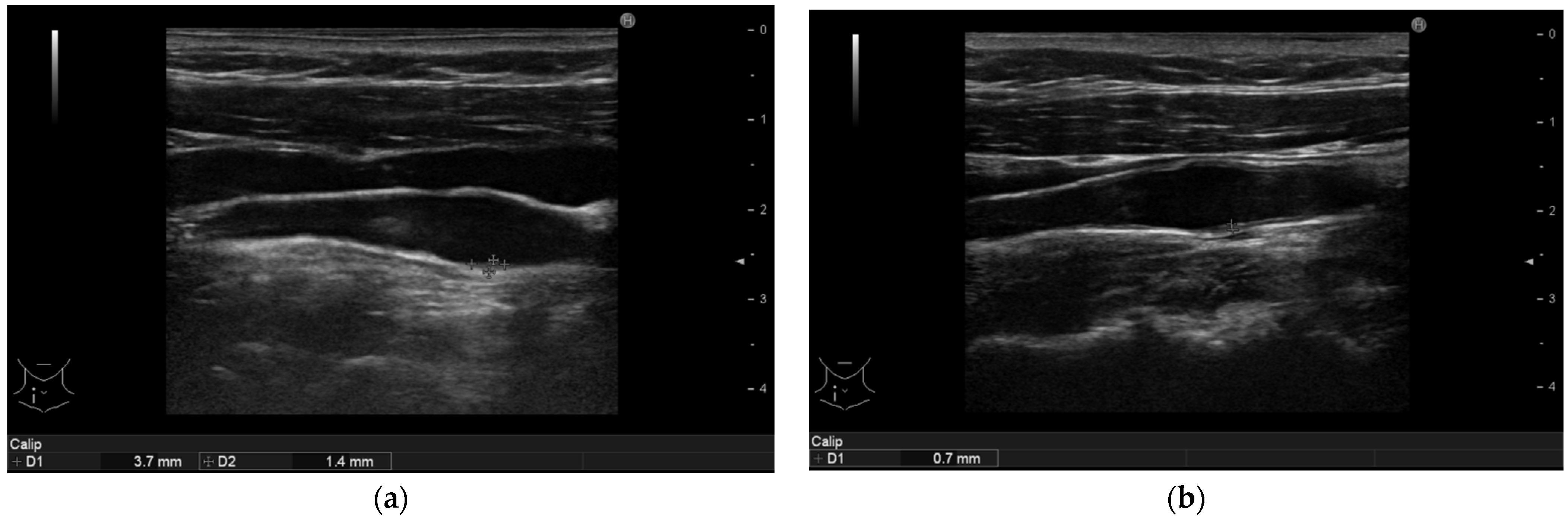
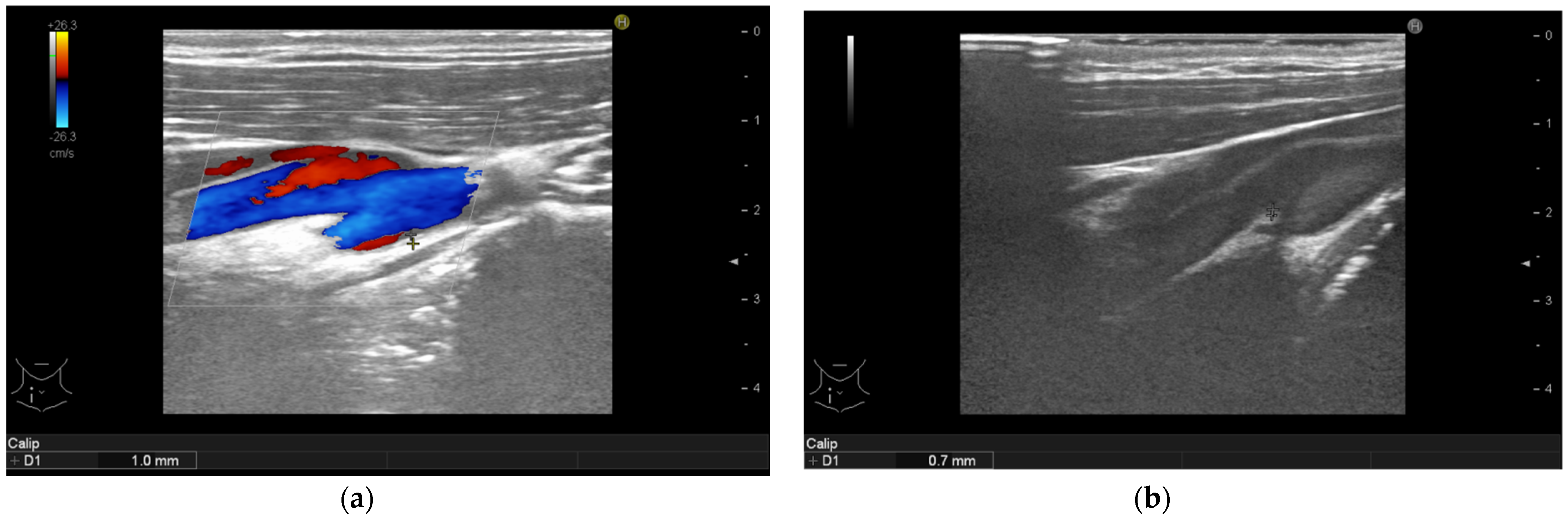
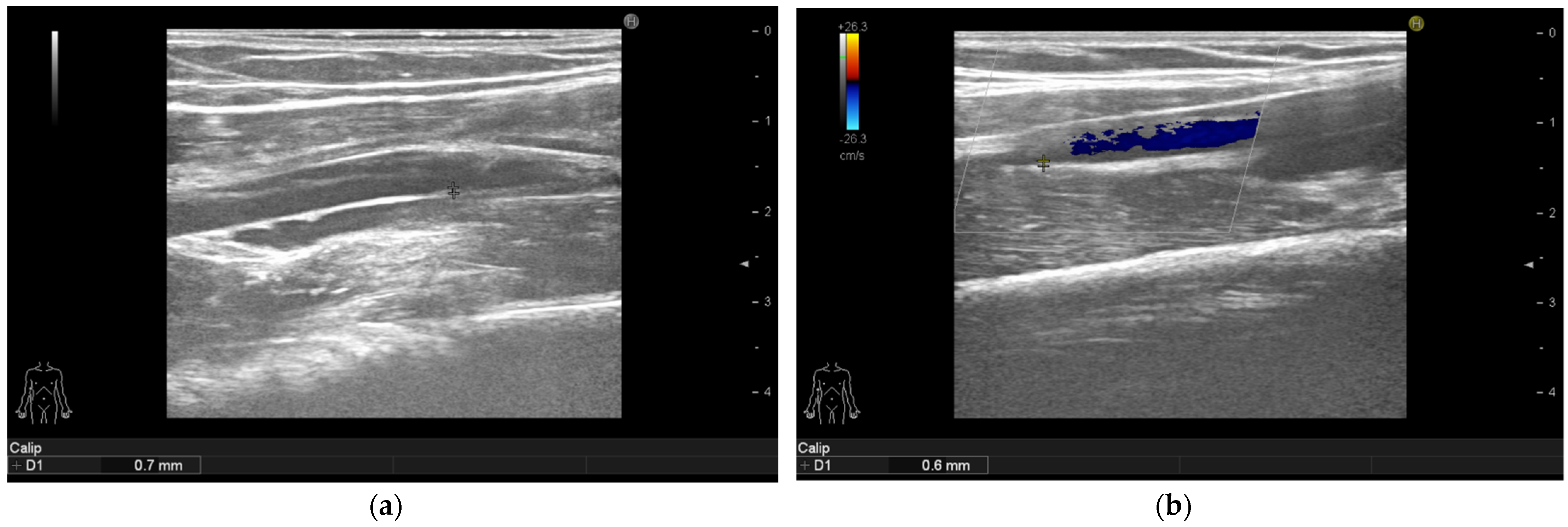
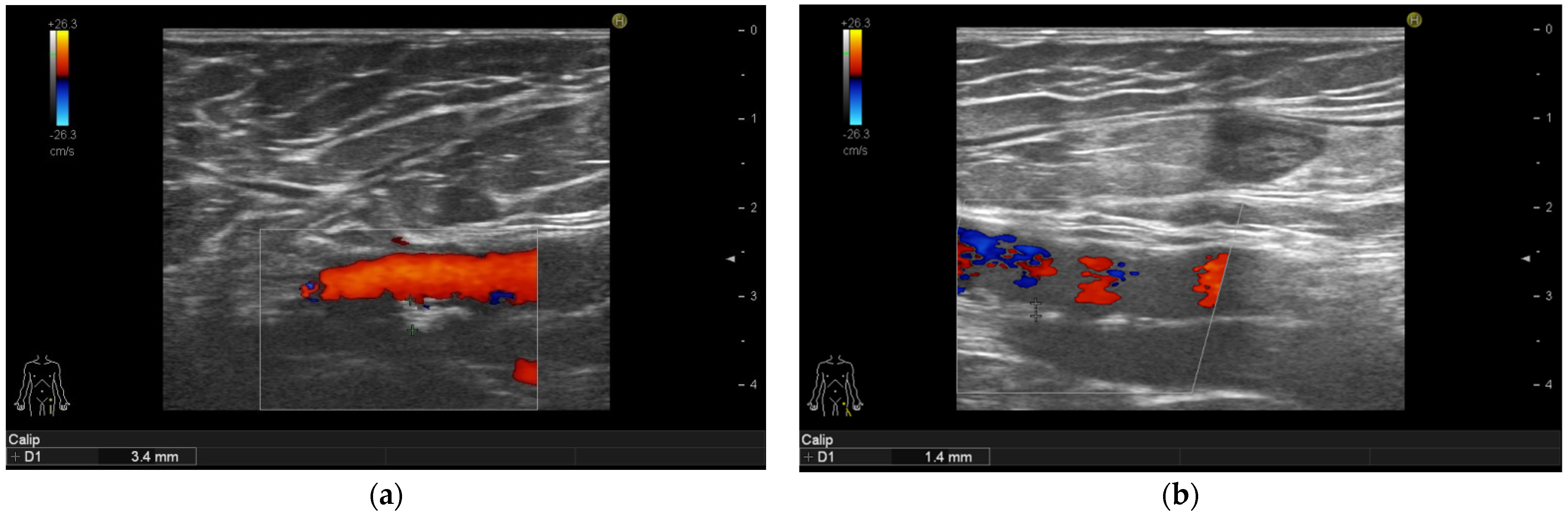
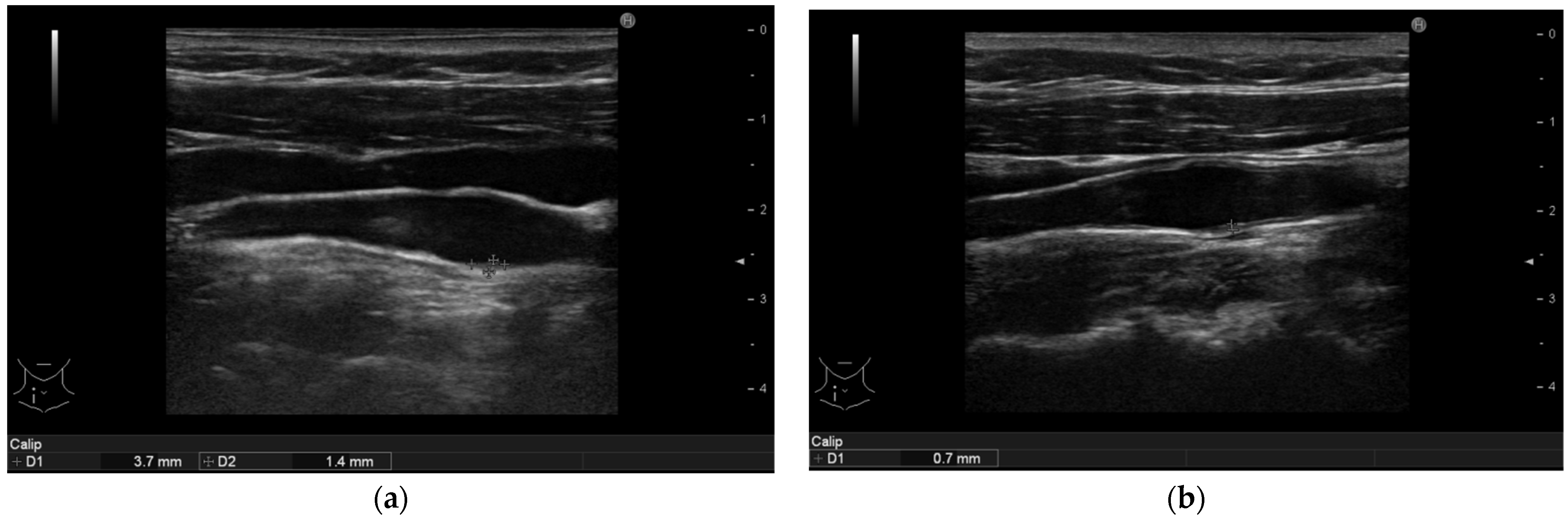
3.4. Ultrasonographic Findings
3.5. Comparing Ultrasonographic Findings between Subgroups of Patients Treated with Secukinumab or Ixekizumab Therapy
4. Discussion
5. Study Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| CVD | cardiovascular disease |
| Th cell | T helper cell |
| IL | interleukin |
| TNF | tumour necrosis factor |
| IFN-γ | interferon-gamma |
| MACE | major cardiac event |
| MI | myocardial infarct |
| HR | hazard ratio |
| CI | confidence interval |
| IMT | intima media thickness |
| cIMT | carotid intima media thickness |
| fIMT | femoral intima media thickness |
| bIMT | brachial intima media thickness |
| ICAM-1 | intercellular adhesion molecule 1 |
| ApoE | apolipoprotein E |
| ROR γt | retinoic acid-related orphan receptor γt |
| PKCß/ERK1/2/NF-κB | protein kinase C beta/extracellular signal-regulated kinase 1/2/nuclear factor kappa-light-chain-enhancer of activated B cells |
| VCAM-1 | vascular cell adhesion molecule 1 |
| QoL | quality of life |
| PASI | psoriasis area severity index |
| DLQI | dermatology life quality index |
| EQ VAS | euroQol visual analogue scale |
| IQR | interquartile range |
| MTX | methotrexate |
| BMI | body mass index |
| AHA/ACC/TOS | American Heart Association/ American College of Cardiology/ The Obesity Society |
| FMD | flow mediated dilatation |
| CARIMA | Evaluation of Cardiovascular Risk Markers in Psoriasis Patients Treated With Secukinumab |
| FAI | fat attenuation index |
| TGF-β | transforming growth factor–β |
| SMAD7 | mothers against decapentaplegic homolog 7 |
References
- McCormick, T.; Ayala-Fontanez, N.; Soler, D. Current knowledge on psoriasis and autoimmune diseases. Psoriasis Targets Ther. 2016, 6, 7–32. [Google Scholar] [CrossRef] [Green Version]
- Boehncke, W.-H. Systemic Inflammation and Cardiovascular Comorbidity in Psoriasis Patients: Causes and Consequences. Front. Immunol. 2018, 9, 579. [Google Scholar] [CrossRef] [PubMed]
- Egeberg, A.; Gisondi, P.; Carrascosa, J.; Warren, R.; Mrowietz, U. The role of the interleukin-23/Th17 pathway in cardiometabolic comorbidity associated with psoriasis. J. Eur. Acad. Dermatol. Venereol. 2020, 34, 1695–1706. [Google Scholar] [CrossRef]
- Boehncke, W.-H.; Boehncke, S.; Tobin, A.-M.; Kirby, B. The ‘psoriatic march’: A concept of how severe psoriasis may drive cardiovascular comorbidity. Exp. Dermatol. 2011, 20, 303–307. [Google Scholar] [CrossRef] [PubMed]
- Falk, E. Pathogenesis of atherosclerosis. J. Am. Coll. Cardiol. 2006, 47 (Suppl. S8), C7–C12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raaby, L.; Ahlehoff, O.; de Thurah, A. Psoriasis and cardiovascular events: Updating the evidence. Arch. Dermatol. Res. 2017, 309, 225–228. [Google Scholar] [CrossRef]
- Siegel, D.; Devaraj, S.; Mitra, A.; Raychaudhuri, S.P.; Raychaudhuri, S.K.; Jialal, I. Inflammation, Atherosclerosis, and Psoriasis. Clin. Rev. Allergy Immunol. 2012, 44, 194–204. [Google Scholar] [CrossRef] [PubMed]
- Lorenz, M.W.; Markus, H.S.; Bots, M.L.; Rosvall, M.; Sitzer, M. Prediction of Clinical Cardiovascular Events with Carotid Intima-Media Thickness. Circulation 2007, 115, 459–467. [Google Scholar] [CrossRef] [Green Version]
- Jókai, H.; Szakonyi, J.; Kontár, O.; Marschalkó, M.; Szalai, K.; Kárpáti, S.; Holló, P. Impact of effective tumor necrosis factor-alfa inhibitor treatment on arterial intima-media thickness in psoriasis: Results of a pilot study. J. Am. Acad. Dermatol. 2013, 69, 523–529. [Google Scholar] [CrossRef]
- Evensen, K.; Slevolden, E.; Skagen, K.; Rønning, O.M.; Brunborg, C.; Krogstad, A.-L.; Russell, D. Increased subclinical atherosclerosis in patients with chronic plaque psoriasis. Atherosclerosis 2014, 237, 499–503. [Google Scholar] [CrossRef] [PubMed]
- Sosnowski, C.; Pasierski, T.; Janeczko-Sosnowska, E.; Szulczyk, A.; Dabrowski, R.; Woźniak, J.; Sumiński, A.; Ruzyłło, W. Femoral rather than carotid artery ultrasound imaging predicts extent and severity of coronary artery disease. Kardiol. Polska 2007, 65, 7–8. [Google Scholar]
- Lekakis, J.P.; Papamichael, C.; Papaioannou, T.G.; Stamatelopoulos, K.S.; Cimponeriu, A.; Protogerou, A.D.; Kanakakis, J.; Stamatelopoulos, S.F. Intima-media thickness score from carotid and femoral arteries predicts the extent of coronary artery disease: Intima-media thickness and CAD. Int. J. Cardiovasc. Imaging 2005, 21, 495–501. [Google Scholar] [CrossRef]
- Martinez-Lopez, A.; Blasco-Morente, G.; Perez-Lopez, I.; Tercedor-Sanchez, J.; Arias-Santiago, S. Studying the effect of systemic and biological drugs on intima-media thickness in patients suffering from moderate and severe psoriasis. J. Eur. Acad. Dermatol. Venereol. 2018, 32, 1492–1498. [Google Scholar] [CrossRef]
- Marovt, M.; Marko, P.B.; Pirnat, M.; Ekart, R. Effect of biologics targeting interleukin-23/-17 axis on subclinical atherosclerosis: Results of a pilot study. Clin. Exp. Dermatol. 2020, 45, 560–564. [Google Scholar] [CrossRef]
- Bissonnette, R.; Harel, F.; Krueger, J.G.; Guertin, M.-C.; Chabot-Blanchet, M.; Gonzalez, J.; Maari, C.; Delorme, I.; Lynde, C.W.; Tardif, J.-C. TNF-α Antagonist and Vascular Inflammation in Patients with Psoriasis Vulgaris: A Randomized Placebo-Controlled Study. J. Investig. Dermatol. 2017, 137, 1638–1645. [Google Scholar] [CrossRef] [PubMed]
- Jovanovic, D.V.; Di Battista, J.A.; Martel-Pelletier, J.; Jolicoeur, F.C.; He, Y.; Zhang, M.; Mineau, F. IL-17 stimulates the production and expression of proinflammatory cytokines, IL-beta and TNF-alpha, by human macrophages. J. Immunol. 1998, 160, 3513–3521. [Google Scholar]
- Gao, Q.; Jiang, Y.; Ma, T.; Zhu, F.; Gao, F.; Zhang, P.; Guo, C.; Wang, Q.; Wang, X.; Ma, C.; et al. A Critical Function of Th17 Proinflammatory Cells in the Development of Atherosclerotic Plaque in Mice. J. Immunol. 2010, 185, 5820–5827. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Zhu, H.; Su, Z.; Sun, C.; Yin, J.; Yuan, H.; Sandoghchian, S.; Jiao, Z.; Wang, S.; Xu, H. IL-17 contributes to cardiac fibrosis following experimental autoimmune myocarditis by a PKCβ/Erk1/2/NF-κB-dependent signaling pathway. Int. Immunol. 2012, 24, 605–612. [Google Scholar] [CrossRef]
- Madhur, M.S.; Lob, H.E.; McCann, L.A.; Iwakura, Y.; Blinder, Y.; Guzik, T.J.; Harrison, D.G. Interleukin 17 Promotes Angiotensin II–Induced Hypertension and Vascular Dysfunction. Hypertension 2010, 55, 500–507. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simon, T.; Taleb, S.; Danchin, N.; Laurans, L.; Rousseau, B.; Cattan, S.; Montely, J.-M.; Dubourg, O.; Tedgui, A.; Kotti, S.; et al. Circulating levels of interleukin-17 and cardiovascular outcomes in patients with acute myocardial infarction. Eur. Heart J. 2012, 34, 570–577. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elnabawi, Y.A.; Dey, A.K.; Goyal, A.; Groenendyk, J.W.; Chung, J.H.; Belur, A.D.; Rodante, J.; Harrington, C.L.; Teague, H.L.; Baumer, Y.; et al. Coronary artery plaque characteristics and treatment with biologic therapy in severe psoriasis: Results from a prospective observational study. Cardiovasc. Res. 2019, 115, 721–728. [Google Scholar] [CrossRef]
- Yamazaki, F.; Takehana, K.; Tamashima, M.; Okamoto, H. Improvement in abnormal coronary arteries estimated by coronary computed tomography angiography after secukinumab treatment in a Japanese psoriatic patient. J. Dermatol. 2019, 46, e51–e52. [Google Scholar] [CrossRef] [PubMed]
- REQ Group. EuroQol—A new facility for the measurement of health-related quality of life. Health Policy 1990, 16, 199–208. [Google Scholar] [CrossRef]
- Finlay, A.Y.; Khan, G. Dermatology Life Quality Index (DLQI)-a simple practical measure for routine clinical use. Clin. Exp. Dermatol. 1994, 19, 210–216. [Google Scholar] [CrossRef]
- Mrowietz, U.; Kragballe, K.; Reich, K.; Spuls, P.; Griffiths, C.; Nast, A.; Franke, J.; Antoniou, C.; Arenberger, P.; Balieva, F.; et al. Definition of treatment goals for moderate to severe psoriasis: A European consensus. Arch. Dermatol. Res. 2010, 303, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Touboul, P.-J.T.; Hennerici, M.G.; Meairs, S.; Adams, H.P.; Amarenco, P.; Bornstein, N.M.; Csiba, L.; Desvarieux, M.; Ebrahim, S.; Hernandez, R.H.; et al. Mannheim Carotid Intima-Media Thickness and Plaque Consensus (2004–2006–2011). An update on behalf of the advisory board of the 3rd, 4th and 5th watching the risk symposia, at the 13th, 15th and 20th European Stroke Conferences, Mannheim, Germany, 2004, Brussels, Belgium, 2006, and Hamburg, Germany, 2011. Cerebrovasc. Dis. 2012, 34, 290–296. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wyman, R.A.; Mays, M.E.; McBride, P.E.; Stein, J. Ultrasound-detected carotid plaque as a predictor of cardiovascular events. Vasc. Med. 2006, 11, 123–130. [Google Scholar] [CrossRef]
- Jensen, M.D.; Ryan, D.H.; Apovian, C.M.; Ard, J.D.; Comuzzie, A.G.; Donato, K.A.; Hu, F.B.; Hubbard, V.S.; Jakicic, J.M.; Kushner, R.F.; et al. 2013 AHA/ACC/TOS Guideline for the Management of Overweight and Obesity in Adults. Circulation 2014, 129 (Suppl. S2), S102–S138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lim, T.K.; Lim, E.; Dwivedi, G.; Kooner, J.; Senior, R. Normal value of carotid intima-media thickness—A surrogate marker of atherosclerosis: Quantitative assessment by B-mode carotid ultrasound. J. Am. Soc. Echocardiogr. 2008, 21, 112–116. [Google Scholar] [CrossRef]
- Hu, S.C.-S.; Lan, C.-C.E. Psoriasis and Cardiovascular Comorbidities: Focusing on Severe Vascular Events, Cardiovascular Risk Factors and Implications for Treatment. Int. J. Mol. Sci. 2017, 18, 2211. [Google Scholar] [CrossRef] [Green Version]
- Armstrong, E.J.; Harskamp, C.T.; Armstrong, A.W. Psoriasis and Major Adverse Cardiovascular Events: A Systematic Review and Meta-Analysis of Observational Studies. J. Am. Heart Assoc. 2013, 2, e000062. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Armstrong, A.W.; Harskamp, C.T.; Armstrong, E.J. The association between psoriasis and hypertension: A systematic review and meta-analysis of observational studies. J. Hypertens. 2013, 31, 433–442. [Google Scholar] [CrossRef]
- Armstrong, A.W.; Lin, S.W.; Chambers, C.J.; Sockolov, M.E.; Chin, D. Psoriasis and Hypertension Severity: Results from a Case-Control Study. PLoS ONE 2011, 6, e18227. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Von Stebut, E.; Reich, K.; Thaci, D.; Koenig, W.; Pinter, A.; Korber, A.; Rassaf, T.; Waisman, A.; Mani, V.; Yates, D.; et al. Impact of Secukinumab on Endothelial Dysfunction and Other Cardiovascular Disease Parameters in Psoriasis Patients over 52 Weeks. J. Investig. Dermatol. 2019, 139, 1054–1062. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elnabawi, Y.A.; Oikonomou, E.; Dey, A.K.; Mancio, J.; Rodante, J.A.; Aksentijevich, M.; Choi, H.; Keel, A.; Erb-Alvarez, J.; Teague, H.L.; et al. Association of Biologic Therapy with Coronary Inflammation in Patients with Psoriasis as Assessed by Perivascular Fat Attenuation Index. JAMA Cardiol. 2019, 4, 885–891. [Google Scholar] [CrossRef]
- Gisterå, A.; Robertson, A.-K.L.; Andersson, J.; Ketelhuth, D.F.J.; Ovchinnikova, O.; Nilsson, S.K.; Lundberg, A.M.; Li, M.O.; Flavell, R.A.; Hansson, G.K. Transforming Growth Factor–β Signaling in T Cells Promotes Stabilization of Atherosclerotic Plaques Through an Interleukin-17–Dependent Pathway. Sci. Transl. Med. 2013, 5, 196ra100. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patients’ Characteristics | N (%) or Median (IQR) |
|---|---|
| Total sample | 31 (100) |
| Sex | |
| Women | 13 (41.9) |
| Men | 18 (58.1) |
| Age (years) | 49 (37–62) |
| Disease duration (years) | 24 (16–28) |
| BMI (kg/m2) | 33.1 (27.2–37.1) |
| Education | |
| Elementary school | 3 (9.7) |
| Secondary school | 18 (58.1) |
| Tertiary Education | 10 (32.2) |
| Employment | |
| Full-time job | 17 (54.8) |
| Retired | 4 (12.9) |
| Unemployed | 5 (16.1) |
| Disability pension | 5 (16.1) |
| Current smoker | 12 (38.7) |
| Former smoker | 7 (22.6) |
| Excessive alcohol consumption | 1 (3.2) |
| Treatments | |
| bionaive | 4 (12.9) |
| Secukinumab | 20 (64.5) |
| Ixekizumab | 11 (35.5) |
| Comorbidity | N (%) |
|---|---|
| Psoriatic arthritis | 17 (54.8) |
| Hypertension | 18 (58.1) |
| Diabetes mellitus | 6 (19.3) |
| Bronchial asthma | 2 (6.4) |
| Allergic rhinitis | 2 (6.4) |
| COPD | 1 (3.2) |
| GERD | 2 (6.4) |
| Hyperuricemia | 7 (22.6) |
| BPH | 1 (3.2) |
| Hyperthyroidism | 1 (3.2) |
| Hypothyroidism | 2 (6.4) |
| Psychiatric disorders | 4 (12.9) |
| Characteristics | Baseline Median (IQR) | 6-Month Follow-Up Median (IQR) | p-Value |
|---|---|---|---|
| Clinical Characteristics | |||
| PASI | 18 (14–24) | 0 (0–4) | <0.001 |
| DLQI | 17 (10–28) | 0 (0–1) | <0.001 |
| EQ VAS | 60 (50–80) | 90 (85–98) | <0.001 |
| Arterial Intima Media Thickness | Baseline Median (IQR) | 6-Month Follow-Up Median (IQR) | p-Value |
|---|---|---|---|
| Intima media thickness of the right carotid arteries (mm) | 1.1 (1.0–1.3) | 0.8 (0.6–0.9) | <0.001 |
| Intima media thickness of the left carotid arteries (mm) | 1.1 (0.9–1.35) | 0.7 (0.6–0.9) | <0.001 |
| Intima media thickness of the right brachial arteries (mm) | 0.75 (0.6–0.9) | 0.6 (0.5–0.7) | <0.001 |
| Intima media thickness of the left brachial arteries (mm) | 0.8 (0.6–0.9) | 0.5 (0.5–0.7) | <0.001 |
| Intima media thickness of the right femoral arteries (mm) | 0.9 (0.8–1.05) | 0.7 (0.5–0.9) | <0.001 |
| Intima media thickness of the left femoral arteries (mm) | 0.8 (0.6–1.1) | 0.7 (0.5–0.8) | <0.001 |
| Cumulative area of the non-calcified plaques in all arteries (mm2) | 3.0 (1.8–6.4) | 1.6 (1.1–7.5) | 0.062 |
| Localization | 35–39 Years | 40–49 Years | 50–59 Years | ≥60 Years |
|---|---|---|---|---|
| Common carotid artery | 0.6 mm | 0.64 mm | 0.71 mm | 0.81 mm |
| Bifurcation | 0.83 mm | 0.77 mm | 0.85 mm | 1.05 mm |
| Common Carotid Artery | Brachial Artery | Common Femoral Artery | ||||
|---|---|---|---|---|---|---|
| Right | Left | Right | Left | Right | Left | |
| Number of non-calcified plaques (N) | 7 | 8 | 0 | 0 | 3 | 0 |
| Number of calcified plaques (N) | 4 | 4 | 0 | 0 | 1 | 3 |
| Calcified Arteries | Non-Calcified Arteries | Baseline | 6-Month Follow-Up | |||
|---|---|---|---|---|---|---|
| Arterial Intima Media Thickness | Baseline Median (IQR) | 6-Month Follow-Up Median (IQR) | Baseline Median (IQR) | 6-Month Follow-Up Median (IQR) | p-Value (Mann Whitney U Test) * | p-Value (Mann Whitney U Test) * |
| Intima media thickness of the right carotid arteries (mm) | 1.2 (1.0–2.0) | 1.0 (0.6–1.1) | 1.1 (1.0–1.3) | 0.8 (0.6–0.8) | 0.385 | 0.044 |
| Intima media thickness of the left carotid arteries (mm) | 1.3 (1.3–1.5) | 1.0 (0.8–1.1) | 1.0 (0.9–1.3) | 0.7 (0.6–0.8) | 0.054 | 0.008 |
| Intima media thickness of the right brachial arteries (mm) | 0.9 (0.7–1.0) | 0.6 (0.6–0.8) | 0.7 (0.6–0.8) | 0.6 (0.5–0.7) | 0.200 | 0.452 |
| Intima media thickness of the left brachial arteries (mm) | 0.8 (0.7–0.9) | 0.5 (0.5–0.7) | 0.8 (0.6–0.9) | 0.5 (0.5–0.7) | 0.747 | 0.939 |
| Intima media thickness of the right femoral arteries (mm) | 1.4 (0.8–2.2) | 0.9 (0.6–1.2) | 0.9 (0.8–1.0) | 0.7 (0.5–0.9) | 0.344 | 0.136 |
| Intima media thickness of the left femoral arteries (mm) | 1.1 (0.9–2.9) | 0.8 (0.7–1.1) | 0.8 (0.6–1.0) | 0.6 (0.5–0.8) | 0.033 | 0.037 |
| Cumulative area of the non-calcified plaques in all arteries (mm2) | - | - | 6.0 (n/a) | 1.5 (n/a) | - | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Piros, É.A.; Szabó, Á.; Rencz, F.; Brodszky, V.; Szalai, K.; Galajda, N.; Szilveszter, B.; Dósa, E.; Merkely, B.; Holló, P. Impact of Interleukin-17 Inhibitor Therapy on Arterial Intima-media Thickness among Severe Psoriatic Patients. Life 2021, 11, 919. https://doi.org/10.3390/life11090919
Piros ÉA, Szabó Á, Rencz F, Brodszky V, Szalai K, Galajda N, Szilveszter B, Dósa E, Merkely B, Holló P. Impact of Interleukin-17 Inhibitor Therapy on Arterial Intima-media Thickness among Severe Psoriatic Patients. Life. 2021; 11(9):919. https://doi.org/10.3390/life11090919
Chicago/Turabian StylePiros, Éva Anna, Ákos Szabó, Fanni Rencz, Valentin Brodszky, Klára Szalai, Noémi Galajda, Bálint Szilveszter, Edit Dósa, Béla Merkely, and Péter Holló. 2021. "Impact of Interleukin-17 Inhibitor Therapy on Arterial Intima-media Thickness among Severe Psoriatic Patients" Life 11, no. 9: 919. https://doi.org/10.3390/life11090919
APA StylePiros, É. A., Szabó, Á., Rencz, F., Brodszky, V., Szalai, K., Galajda, N., Szilveszter, B., Dósa, E., Merkely, B., & Holló, P. (2021). Impact of Interleukin-17 Inhibitor Therapy on Arterial Intima-media Thickness among Severe Psoriatic Patients. Life, 11(9), 919. https://doi.org/10.3390/life11090919