
Cutaneous Metastases from Primary Liver Cancers: The Need for Knowledge and Differential Diagnosis

 ,
, 
 and
and 
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
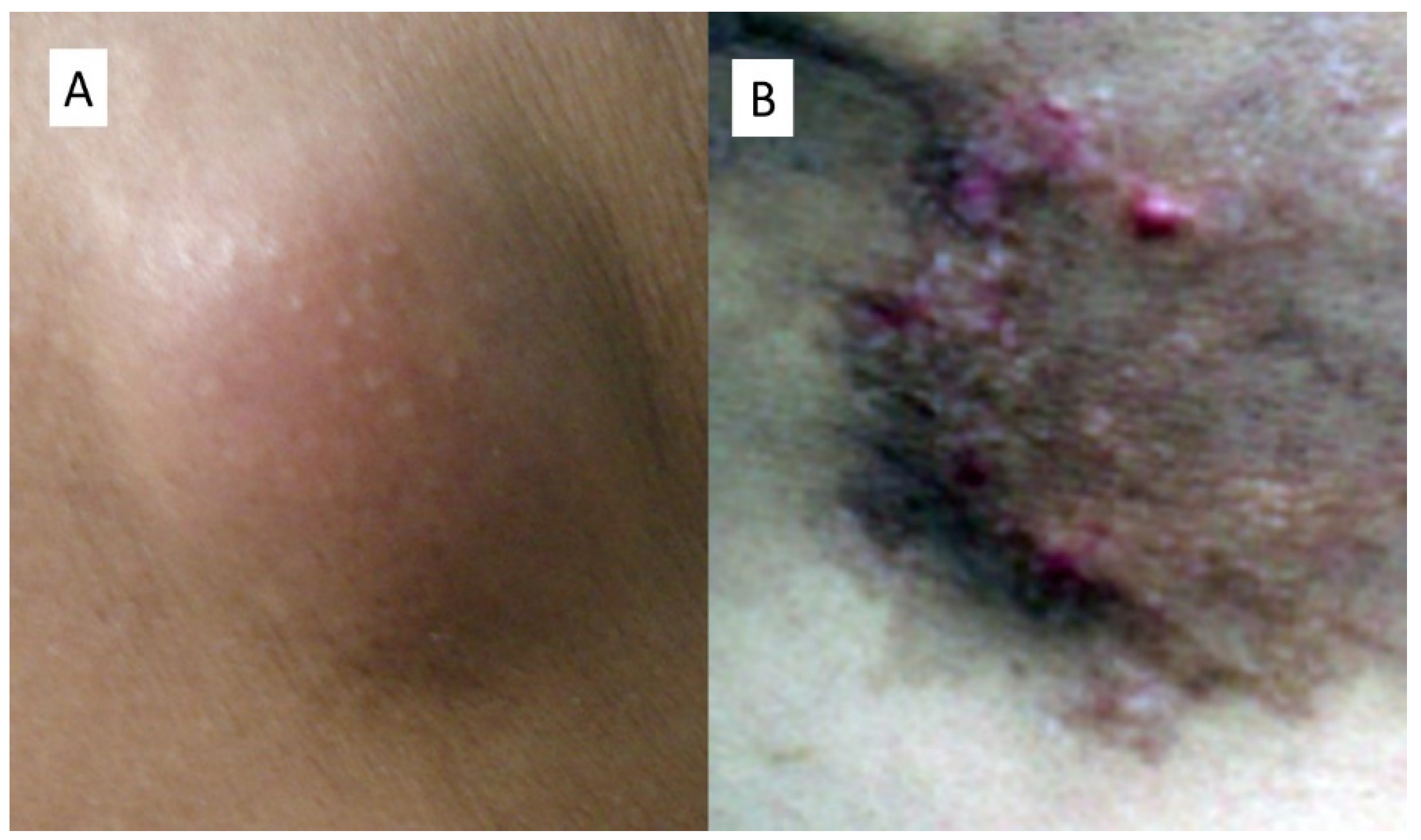
2. Cases Presentation
2.1. Case Number 1
2.2. Case Number 2
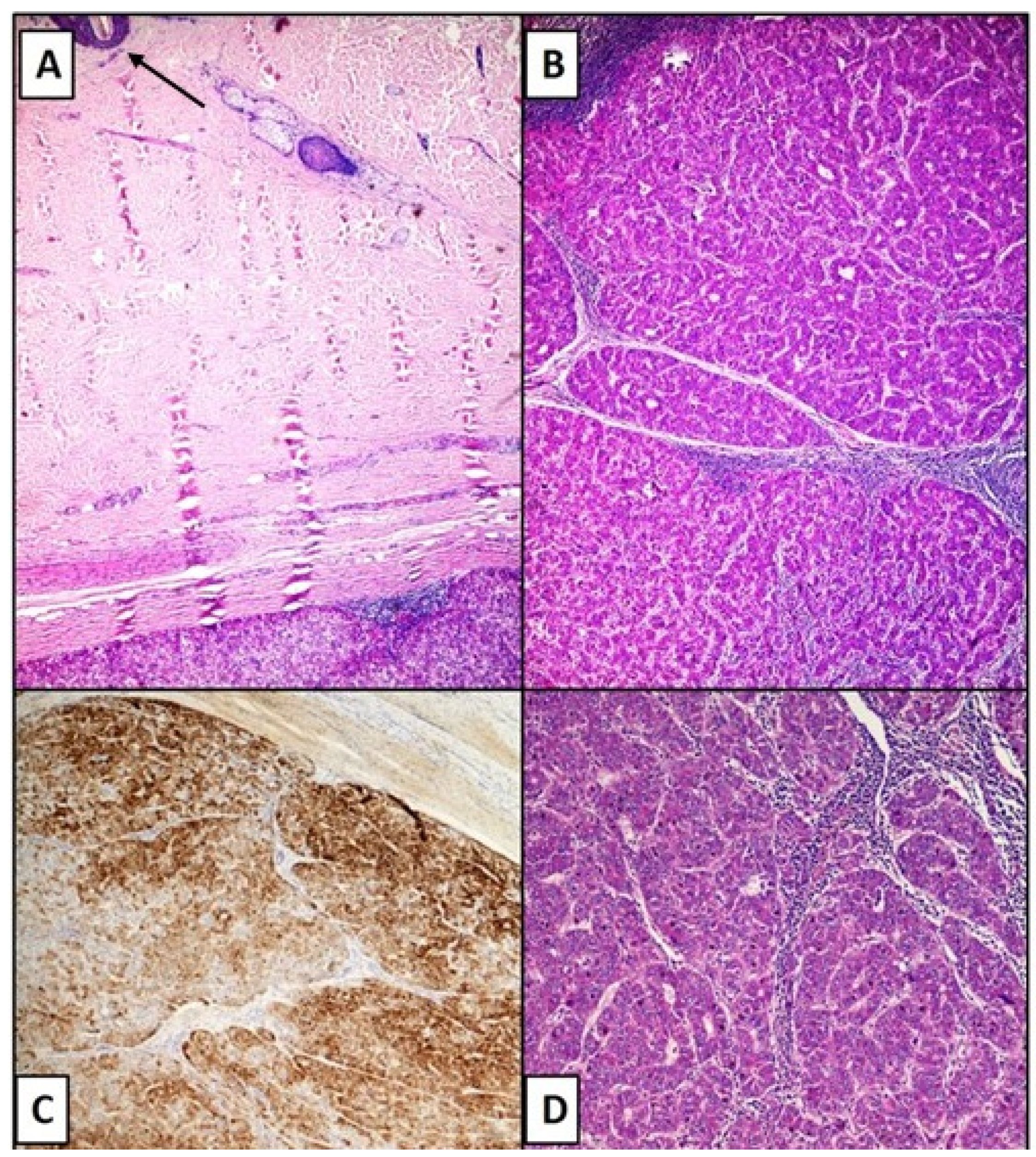
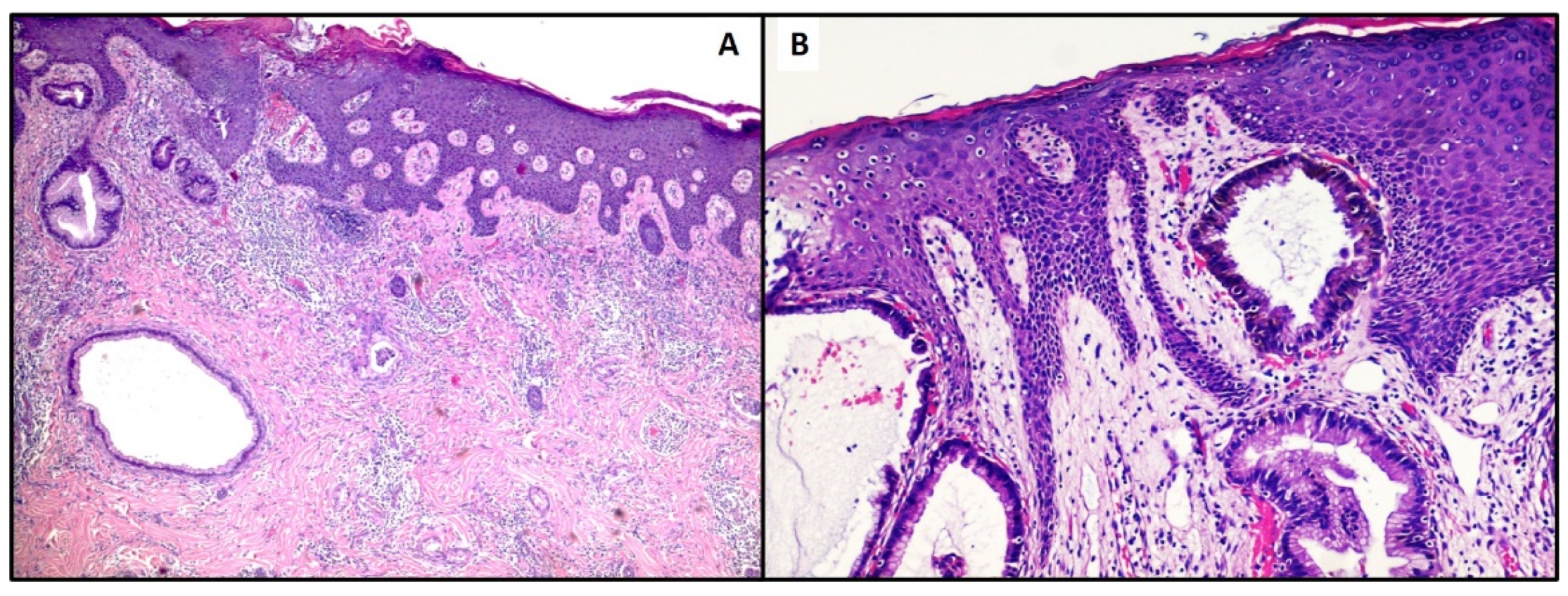
3. Material and Methods
4. Results
4.1. Case Number 1
4.2. Case Number 2
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Saeed, S.; Keehn, C.A.; Morgan, M.B. Cutaneous metastasis: A clinical, pathological, and immunohistochemical appraisal. J. Cutan. Pathol. 2004, 31, 419–430. [Google Scholar] [CrossRef] [PubMed]
- Cozzani, E.; Cecchi, F.; Ghigliotti, G.; Tavilla, P.; Cabiddu, F.; Drago, F.; Burlando, M.; Rongioletti, F.; Parodi, A. Primary cutaneous melanoma: Correlation between clinical and histologic aspects in a retrospective Italian study. G. Ital. Dermatol. Venereol. 2019, 154, 519–522. [Google Scholar] [CrossRef] [PubMed]
- Kanitakis, J.; Chouvet, B.; Claudy, A.; Scoazec, J.Y. Immunoreactivity of hepatocyte paraffin 1 monoclonal antibody in cutaneous metastatic tumors. Am. J. Clin. Pathol. 2004, 122, 85–89. [Google Scholar] [CrossRef]
- Turner, N.; Ware, O.; Bosenberg, M. Genetics of metastasis: Melanoma and other cancers. Clin. Exp. Metastasis. 2018, 35, 379–391. [Google Scholar] [CrossRef] [PubMed]
- Isa, N.M.; Bong, J.J.; Ghani, F.A.; Rose, I.M.; Husain, S.; Azrif, M. Cutaneous metastasis of hepatocellular carcinoma diagnosed by fine needle aspiration cytology and Hep Par 1 immunopositivity. Diagn Cytopathol. 2012, 40, 1010–1014. [Google Scholar] [CrossRef]
- Queen, D.; Fisher, J.; Husain, S.; Linos, K.; Niedt, G.W.; Samie, F.H. Cutaneous metastasis of hepatocellular carcinoma following liver transplantation. J. Cutan. Pathol. 2020, 47, 47–51. [Google Scholar] [CrossRef]
- Razumilava, N.; Gores, G.J. Cholangiocarcinoma. Lancet 2014, 383, 2168–2179. [Google Scholar] [CrossRef]
- Liu, M.; Liu, B.L.; Liu, B.; Guo, L.; Wang, Q.; Song, Y.Q.; Dong, L.H. Cutaneous metastasis of cholangiocarcinoma. World J. Gastroenterol. 2015, 14, 3066–3071. [Google Scholar] [CrossRef]
- Kubota, Y.; Koga, T.; Nakayama, J. Cutaneous metastasis from hepatocellular carcinoma resembling pyogenic granuloma. Clin. Exp. Dermatol. 1999, 24, 78–80. [Google Scholar] [CrossRef]
- Berbis, P.; Auffranc, J.C.; Andrac, L.; Fabre, J.F.; Arnaud, A.; Privat, Y. Angioma-like cutaneous metastasis disclosing a hepatocarcinoma. Ann. Dermatol. Venereol. 1986, 113, 563–567. [Google Scholar]
- Yamanishi, K.; Kishimoto, S.; Hosokawa, Y.; Yamada, K.; Yasuno, H. Cutaneous metastasis from hepatocellular carcinoma resembling granuloma teleangiectaticum. J. Dermatol. 1989, 16, 500–504. [Google Scholar] [CrossRef]
- Patel, N.; Sheehan-Dare, G.; Weir, J.; Verma, S.; Fearfield, L. Cutaneous metastasis as the first presentation of hepatocellular carcinoma. Hepatology 2018, 67, 1631–1633. [Google Scholar] [CrossRef] [PubMed]
- Paolino, G.; Pampena, R.; Grassi, S.; Mercuri, S.R.; Cardone, M.; Corsetti, P.; Moliterni, E.; Muscianese, M.; Rossi, A.; Frascione, P.; et al. Alopecia neoplastica as a sign of visceral malignancies: A systematic review. J. Eur. Acad. Dermatol. Venereol. 2019, 33, 1020–1028. [Google Scholar] [CrossRef]
- Amador, A.; Monforte, N.G.; Bejarano, N.; Martí, J.; Artigau, E.; Navarro, S.; Fuster, J. Cutaneous metastasis from hepatocellular carcinoma as the first clinical sign. J. Hepatobiliary Pancreat. Surg. 2007, 14, 328–330. [Google Scholar] [CrossRef]
- Cho, E.; Kim, H.S.; Park, Y.M.; Kim, H.O.; Lee, J.Y. Cutaneous metastasis of hepatocellular carcinoma following skin injury after transcatheter arterial chemoembolization. Ann. Dermatol. 2013, 25, 107–109. [Google Scholar] [CrossRef]
- De León, F.J.; Blanes, M.M.; Albares, M.P.; Berbegal, L. Cutaneous metastasis from hepatocellular carcinoma after a percutaneous interventional procedure. Actas Dermosifiliogr. 2015, 106, 440–441. [Google Scholar] [CrossRef]
- Nagaoka, Y.; Nakayama, R.; Iwata, M. Cutaneous seeding following percutaneous ethanol injection therapy for hepatocellular carcinoma. Intern. Med. 2004, 43, 268–269. [Google Scholar] [CrossRef]
- Hu, S.C.; Chen, G.S.; Wu, C.S.; Chai, C.Y.; Chen, W.T.; Lan, C.C. Rates of cutaneous metastases from different internal malignancies: Experience from a Taiwanese medical center. J. Am. Acad Dermatol. 2009, 60, 379–387. [Google Scholar] [CrossRef]
- Terada, T.; Sugiura, M. Metastatic hepatocellular carcinoma of skin diagnosed with hepatocyte paraffin 1 and a-fetoprotein immunostainings. Int. J. Surg. Pathol. 2010, 18, 433–436. [Google Scholar] [CrossRef] [PubMed]
- Dogan, G.; Karincaoglu, Y.; Karincaoglu, M.; Aydin, N.E. Scalp ulcer as first sign of cholangiocarcinoma. Am. J. Clin. Dermatol. 2006, 7, 387–389. [Google Scholar] [CrossRef] [PubMed]
- Fernández López, A.J.; Tamayo-Rodríguez, M.E.; Paniza-Mendoza, M.Á. Sternal cutaneous metastasis of hilar cholangiocarcinoma. Rev. Esp. Enferm. Dig. 2017, 109, 674. [Google Scholar] [CrossRef] [PubMed]
- Varma, K.; Singh, A.; Misra, V. Cutaneous Metastasis from Cholangiocarcinoma Presenting as Thigh Mass. J. Clin. Diagn. Res. 2016, 10, ED23–ED25. [Google Scholar] [CrossRef] [PubMed]
- Pasquali, P.; Fortuño, A.; Casañas, C.; Fonoll, M.; Landeyro, J.; Gonzalez, J. Scalp and chest cutaneous metastases of cholangiocarcinoma. Int. J. Dermatol. 2013, 52, 1414–1417. [Google Scholar] [CrossRef] [PubMed]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cazzato, G.; Colagrande, A.; Cimmino, A.; De Marco, A.; Romita, P.; Foti, C.; Resta, L.; Ingravallo, G. Cutaneous Metastases from Primary Liver Cancers: The Need for Knowledge and Differential Diagnosis. Life 2021, 11, 559. https://doi.org/10.3390/life11060559
Cazzato G, Colagrande A, Cimmino A, De Marco A, Romita P, Foti C, Resta L, Ingravallo G. Cutaneous Metastases from Primary Liver Cancers: The Need for Knowledge and Differential Diagnosis. Life. 2021; 11(6):559. https://doi.org/10.3390/life11060559
Chicago/Turabian StyleCazzato, Gerardo, Anna Colagrande, Antonietta Cimmino, Aurora De Marco, Paolo Romita, Caterina Foti, Leonardo Resta, and Giuseppe Ingravallo. 2021. "Cutaneous Metastases from Primary Liver Cancers: The Need for Knowledge and Differential Diagnosis" Life 11, no. 6: 559. https://doi.org/10.3390/life11060559
APA StyleCazzato, G., Colagrande, A., Cimmino, A., De Marco, A., Romita, P., Foti, C., Resta, L., & Ingravallo, G. (2021). Cutaneous Metastases from Primary Liver Cancers: The Need for Knowledge and Differential Diagnosis. Life, 11(6), 559. https://doi.org/10.3390/life11060559