
Compared to Individuals with Mild to Moderate Obstructive Sleep Apnea (OSA), Individuals with Severe OSA Had Higher BMI and Respiratory-Disturbance Scores


 ,
,  , and
, and 
Abstract
1. Introduction
2. Material and Methods
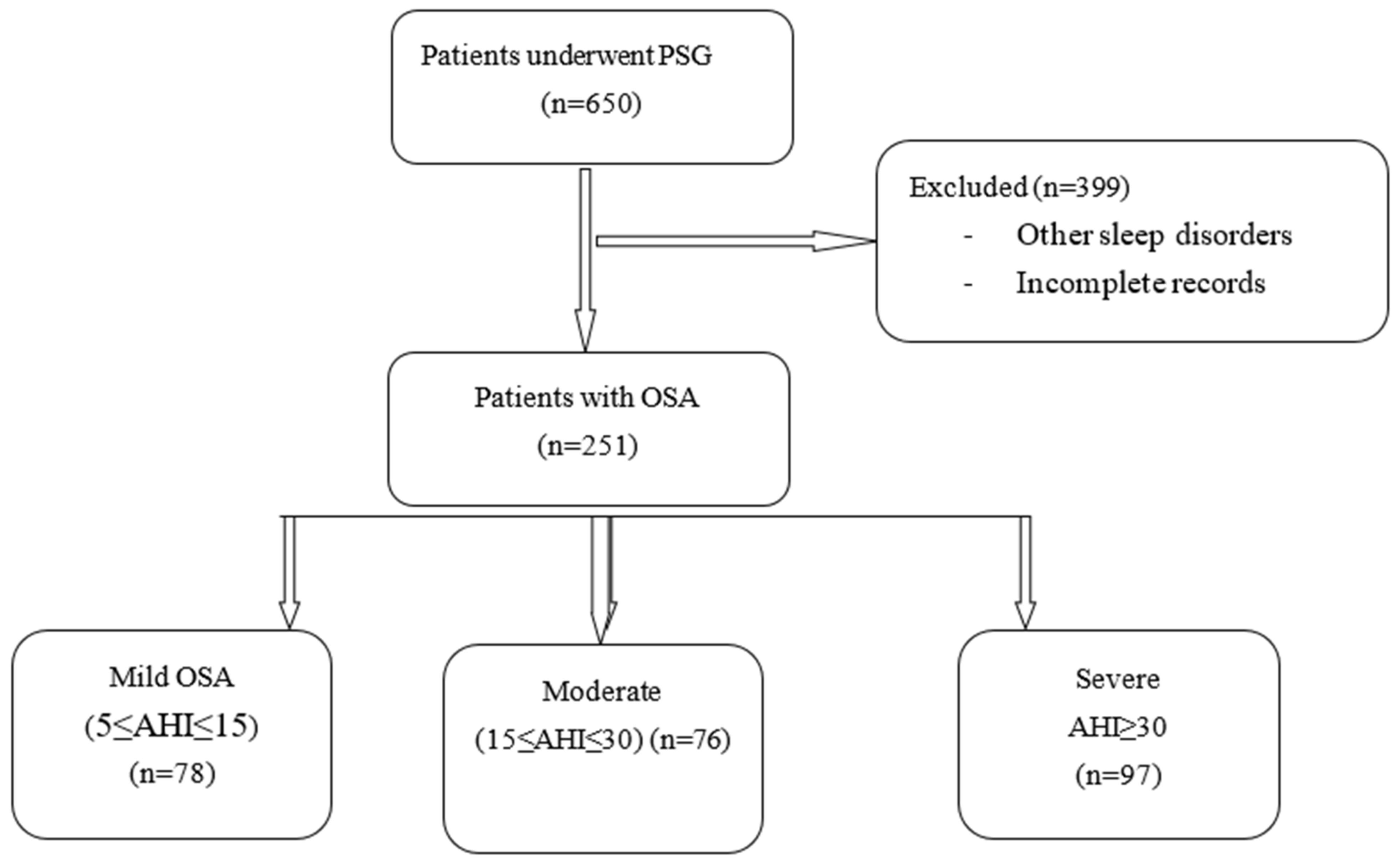
2.1. Study Design
2.2. Measures
2.2.1. Demographic and Anthropometric Data
2.2.2. Sleep Quality
2.2.3. Daytime Sleepiness
2.2.4. Self-Reported Breathing Issues; STOP-Bang Questionnaire
2.2.5. Polysomnography and Breathing-Related Information
2.2.6. Further Medical Complaints
2.2.7. Statistical Analysis
3. Results
3.1. General Observations
3.2. Associations between Age, BMI, Subjective and Objective Sleep Parameters, and Subjective and Objective Breathing-Related Parameters
3.3. Apnea/Hypopnea Index (Categorial), Gender, Tobacco-Smoking Status, Diabetes, Hypertension, and Cardiovascular Diseases (Categorical Variables)
3.4. Apnea/Hypopnea Index (Categorial) and Demographic, Anthropometric, and Sleep-Related Dimensions
3.5. Predicting Apnea/Hypopnea Index (Continuous Variable) by Sociodemographic, Anthropometric, and Subjective and Objective Sleep- and Breathing-Related Sleep Variables
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- American Academy of Sleep Medicine. The International Classification of Sleep Disorders, 3rd ed.; American Academy of Sleep Medicine: Darien, IL, USA, 2014. [Google Scholar]
- Peppard, P.E.; Young, T.; Barnet, J.H.; Palta, M.; Hagen, E.W.; Hla, K.M. Increased Prevalence of Sleep-Disordered Breathing in Adults. Am. J. Epidemiol. 2013, 177, 1006–1014. [Google Scholar] [CrossRef]
- Heinzer, R.; Vat, S.; Marques-Vidal, P.; Marti-Soler, H.; Andries, D.; Tobback, N.; Mooser, V.; Preisig, M.; Malhotra, A.; Waeber, G.; et al. Prevalence of sleep-disordered breathing in the general population: The HypnoLaus study. Lancet Respir. Med. 2015, 3, 310–318. [Google Scholar] [CrossRef]
- Tufik, S.; Santos-Silva, R.; Taddei, J.A.; Bittencourt, L.R.A. Obstructive sleep apnea syndrome in the Sao Paulo Epidemiologic Sleep Study. Sleep Med. 2010, 11, 441–446. [Google Scholar] [CrossRef]
- Khazaie, H.; Najafi, F.; Rezaie, L.; Tahmasian, M.; Sepehry, A.A.; Herth, F.J. Prevalence of symptoms and risk of obstructive sleep apnea syndrome in the general population. Arch. Iran. Med. 2011, 14, 335–338. [Google Scholar] [CrossRef]
- Al Lawati, N.M.; Patel, S.R.; Ayas, N.T. Epidemiology, risk factors, and consequences of obstructive sleep apnea and short sleep duration. Prog. Cardiovasc. Dis. 2009, 51, 285–293. [Google Scholar] [CrossRef]
- Tregear, S.; Reston, J.; Schoelles, K.; Phillips, B. Obstructive sleep apnea and risk of motor vehicle crash: Systematic review and meta-analysis. J. Clin. Sleep Med. 2009, 5, 573–581. [Google Scholar] [CrossRef]
- Imani, M.M.; Sadeghi, M.; Khazaie, H.; Emami, M.; Sadeghi Bahmani, D.; Brand, S. Evaluation of Serum and Plasma Interleukin-6 Levels in Obstructive Sleep Apnea Syndrome: A Meta-Analysis and Meta-Regression. Front. Immunol. 2020, 11, 1343. [Google Scholar] [CrossRef]
- Imani, M.M.; Sadeghi, M.; Khazaie, H.; Emami, M.; Sadeghi Bahmani, D.; Brand, S. Serum and Plasma Tumor Necrosis Factor Alpha Levels in Individuals with Obstructive Sleep Apnea Syndrome: A Meta-Analysis and Meta-Regression. Life 2020, 10, 87. [Google Scholar] [CrossRef]
- Mirrakhimov, A.E. Obstructive sleep apnea and autoimmune rheumatic disease: Is there any link? Inflamm. Allergy Drug Targets 2013, 12, 362–367. [Google Scholar] [CrossRef]
- McNicholas, W.T.; Bonsigore, M.R. Sleep apnoea as an independent risk factor for cardiovascular disease: Current evidence, basic mechanisms and research priorities. Eur. Respir. J. 2007, 29, 156–178. [Google Scholar] [CrossRef]
- Loke, Y.K.; Brown, J.W.; Kwok, C.S.; Niruban, A.; Myint, P.K. Association of obstructive sleep apnea with risk of serious cardiovascular events: A systematic review and meta-analysis. Circ. Cardiovasc. Qual. Outcomes 2012, 5, 720–728. [Google Scholar] [CrossRef] [PubMed]
- Gabryelska, A.; Łukasik, Z.M.; Makowska, J.S.; Białasiewicz, P. Obstructive Sleep Apnea: From Intermittent Hypoxia to Cardiovascular Complications via Blood Platelets. Front. Neurol. 2018, 9. [Google Scholar] [CrossRef]
- Wang, X.; Ouyang, Y.; Wang, Z.; Zhao, G.; Liu, L.; Bi, Y. Obstructive sleep apnea and risk of cardiovascular disease and all-cause mortality: A meta-analysis of prospective cohort studies. Int. J. Cardiol. 2013, 169, 207–214. [Google Scholar] [CrossRef]
- Mok, Y.; Tan, C.W.; Wong, H.S.; How, C.H.; Tan, K.L.; Hsu, P.P. Obstructive sleep apnoea and Type 2 diabetes mellitus: Are they connected? Singap. Med. J. 2017, 58, 179–183. [Google Scholar] [CrossRef] [PubMed]
- Zhang, R.; Guo, X.; Guo, L.; Lu, J.; Zhou, X.; Ji, L. Prevalence and associated factors of obstructive sleep apnea in hospitalized patients with type 2 diabetes in Beijing, China 2. J. Diabetes 2015, 7, 16–23. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Xing, Y.; Yuan, H.; Gang, X.; Guo, W.; Li, Z.; Wang, G. Impaired Glucose Metabolisms of Patients with Obstructive Sleep Apnea and Type 2 Diabetes. J. Diabetes Res. 2018, 2018, 6714392. [Google Scholar] [CrossRef]
- Sharifpour, P.; Dehvan, F.; Dalvand, S.; Ghanei Gheshlagh, R. Examination of the Relationship Between Metabolic Syndrome and Obstructive Sleep Apnea in Iranian Patients with Type 2 Diabetes: A Case-Control Study. Diabetes Metab. Syndr. Obes. 2020, 13, 2251–2257. [Google Scholar] [CrossRef]
- Fallahi, A.; Jamil, D.I.; Karimi, E.B.; Baghi, V.; Gheshlagh, R.G. Prevalence of obstructive sleep apnea in patients with type 2 diabetes: A systematic review and meta-analysis. Diabetes Metab. Syndr. 2019, 13, 2463–2468. [Google Scholar] [CrossRef]
- Carneiro, G.; Zanella, M.T. Obesity metabolic and hormonal disorders associated with obstructive sleep apnea and their impact on the risk of cardiovascular events. Metabolism 2018, 84, 76–84. [Google Scholar] [CrossRef]
- Imani, M.M.; Sadeghi, M.; Khazaie, H.; Sanjabi, A.; Brand, S.; Brühl, A.; Sadeghi Bahmani, D. Associations Between Morning Salivary and Blood Cortisol Concentrations in Individuals With Obstructive Sleep Apnea Syndrome: A Meta-Analysis. Front. Endocrinol. 2020, 11, 568823. [Google Scholar] [CrossRef]
- Daskalakis, N.P.; Lehrner, A.; Yehuda, R. Endocrine aspects of post-traumatic stress disorder and implications for diagnosis and treatment. Endocrinol. Metab. Clin. North Am. 2013, 42, 503–513. [Google Scholar] [CrossRef] [PubMed]
- Yehuda, R. Current status of cortisol findings in post-traumatic stress disorder. Psychiatr. Clin. N. Am. 2002, 25, 341–368. [Google Scholar] [CrossRef]
- Hobzova, M.; Prasko, J.; Vanek, J.; Ociskova, M.; Genzor, S.; Holubova, M.; Grambal, A.; Latalova, K. Depression and obstructive sleep apnea. Neuro Endocrinol. Lett. 2017, 38, 343–352. [Google Scholar]
- Rezaie, L.; Phillips, D.; Khazaie, H. Barriers to acceptance and adherence to continuous positive airway pressure therapy in patients with obstructive sleep apnea: A report from Kermanshah province, western Iran. Patient Prefer Adherence 2018, 12, 1299–1304. [Google Scholar] [CrossRef]
- Dredla, B.K.; Castillo, P.R. Cardiovascular Consequences of Obstructive Sleep Apnea. Curr. Cardiol. Rep. 2019, 21, 137. [Google Scholar] [CrossRef]
- Lin, C.M.; Davidson, T.M.; Ancoli-Israel, S. Gender differences in obstructive sleep apnea and treatment implications. Sleep Med. Rev. 2008, 12, 481–496. [Google Scholar] [CrossRef] [PubMed]
- Tarasiuk, A.; Reuveni, H. The economic impact of obstructive sleep apnea. Curr. Opin. Pulm. Med. 2013, 19, 639–644. [Google Scholar] [CrossRef]
- Senaratna, C.V.; Perret, J.L.; Lodge, C.J.; Lowe, A.J.; Campbell, B.E.; Matheson, M.C.; Hamilton, G.S.; Dharmage, S.C. Prevalence of obstructive sleep apnea in the general population: A systematic review. Sleep Med. Rev. 2017, 34, 70–81. [Google Scholar] [CrossRef] [PubMed]
- Punjabi, N.M. The epidemiology of adult obstructive sleep apnea. Proc. Am. Thorac. Soc. 2008, 5, 136–143. [Google Scholar] [CrossRef]
- Epstein, L.J.; Kristo, D.; Strollo, P.J., Jr.; Friedman, N.; Malhotra, A.; Patil, S.P.; Ramar, K.; Rogers, R.; Schwab, R.J.; Weaver, E.M.; et al. Clinical guideline for the evaluation, management and long-term care of obstructive sleep apnea in adults. J. Clin Sleep Med. 2009, 5, 263–276. [Google Scholar]
- Patil, S.P.; Ayappa, I.A.; Caples, S.M.; Kimoff, R.J.; Patel, S.R.; Harrod, C.G. Treatment of adult obstructive sleep apnea with positive airway pressure: An American Academy of Sleep Medicine systematic review, meta-analysis, and GRADE assessment. J. Clin. Sleep Med. 2019, 15, 301–334. [Google Scholar] [CrossRef]
- Mohammadi, H.; Aarabi, A.; Rezaie, L.; Khazaie, H.; Brand, S. Sleep spindle characteristrics in obstructive sleep apnea syndrome (OSAS). Front. Neurol. 2021. [Google Scholar] [CrossRef]
- Ondze, B.; Espa, F.; Dauvilliers, Y.; Billiard, M.; Besset, A. Sleep architecture, slow wave activity and sleep spindles in mild sleep disordered breathing. Clin. Neurophysiol. 2003, 114, 867–874. [Google Scholar] [CrossRef]
- Foroughi, M.; Malekmohammad, M.; Sharafkhaneh, A.; Emami, H.; Adimi, P.; Khoundabi, B. Prevalence of Obstructive Sleep Apnea in a High-Risk Population Using the Stop-Bang Questionnaire in Tehran, Iran. Tanaffos 2017, 16, 217–224. [Google Scholar]
- Amra, B.; Farajzadegan, Z.; Golshan, M.; Fietze, I.; Penzel, T. Prevalence of sleep apnea-related symptoms in a Persian population. Sleep Breath 2011, 15, 425–429. [Google Scholar] [CrossRef] [PubMed]
- Foroughi, M.; Razavi, H.; Malekmohammad, M.; Adimi Naghan, P.; Jamaati, H. Diagnosis of Obstructive Sleep Apnea Syndrome in Adults: A Brief Review of Existing Data for Practice in Iran. Tanaffos 2016, 15, 70–74. [Google Scholar] [PubMed]
- World Medical Association. World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. Jama 2013, 310, 2191–2194. [Google Scholar] [CrossRef]
- Buysse, D.J.; Reynolds, C.F., 3rd; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh Sleep Quality Index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Chehri, A.; Brand, S.; Goldaste, N.; Eskandari, S.; Brühl, A.; Sadeghi Bahmani, D.; Khazaie, H. Psychometric Properties of the Persian Pittsburgh Sleep Quality Index for Adolescents. Int. J. Environ. Res. Public Health 2020, 17, 95. [Google Scholar] [CrossRef]
- Chehri, A.; Nourozi, M.; Eskandari, S.; Khazaie, H.; Hemati, N.; Jalali, A. Validation of the Persian version of the Pittsburgh Sleep Quality Index in elderly population. Sleep Sci. 2020, 13, 119–124. [Google Scholar] [CrossRef] [PubMed]
- Farrahi, J.; Nakhaee, N.; Sheibani, V.; Garrusi, B.; Amirkafi, A. Psychometric properties of the Persian version of the Pittsburgh Sleep Quality Index addendum for PTSD (PSQI-A). Sleep Breath 2009, 13, 259–262. [Google Scholar] [CrossRef]
- Farrahi Moghaddam, J.; Nakhaee, N.; Sheibani, V.; Garrusi, B.; Amirkafi, A. Reliability and validity of the Persian version of the Pittsburgh Sleep Quality Index (PSQI-P). Sleep Breath. Schlaf Atm. 2012, 16, 79–82. [Google Scholar] [CrossRef]
- Alikhani, M.; Ebrahimi, A.; Farnia, V.; Khazaie, H.; Radmehr, F.; Mohamadi, E.; Davarinejad, O.; Dürsteler, K.; Sadeghi Bahmani, D.; Brand, S. Effects of treatment of sleep disorders on sleep, psychological and cognitive functioning and biomarkers in individuals with HIV/AIDS and under methadone maintenance therapy. J. Psychiatr. Res. 2020, 130, 260–272. [Google Scholar] [CrossRef]
- Haghighi, K.S.; Montazeri, A.; Mehrizi, A.K.; Aminian, O.; Golkhandan, A.R.; Saraei, M.; Sedaghat, M. The Epworth Sleepiness Scale: Translation and validation study of the Iranian version. Sleep Breath. 2013, 17, 419–426. [Google Scholar] [CrossRef]
- Johns, M.W. A new method for measuring daytime sleepiness: The Epworth sleepiness scale. Sleep 1991, 14, 540–545. [Google Scholar] [CrossRef]
- Shaygannejad, V.; Sadeghi Bahmani, D.; Soleimani, P.; Mirmosayyeb, O.; Barzegar, M.; Amra, B.; Brand, S. Comparison of prevalence rates of restless legs syndrome, self-assessed risks of obstructive sleep apnea, and daytime sleepiness among patients with multiple sclerosis (MS), clinically isolated syndrome (CIS) and Neuromyelitis Optica Spectrum Disorder (NMOSD). Sleep Med. 2020, 70, 97–105. [Google Scholar] [CrossRef]
- Farney, R.J.; Walker, B.S.; Farney, R.M.; Snow, G.L.; Walker, J.M. The STOP-Bang equivalent model and prediction of severity of obstructive sleep apnea: Relation to polysomnographic measurements of the apnea/hypopnea index. J. Clin. Sleep Med. 2011, 7, 459–465. [Google Scholar] [CrossRef]
- Larner, A.; B, Z. Screening for obstructive sleep apnoea using the STOPBANG questionnaire. Clin. Med. 2018, 18, 108–109. [Google Scholar] [CrossRef]
- Hair, J.F.; Black, C.W.; Babin, B.J.; Anderson, R.E. Multivariate Data Analysis, 7th ed.; Pearson Education Limited: Essex, UK, 2014. [Google Scholar]
- Brosius, F. SPSS; Umfassendes Handbuch zu Statistik und Datenanalyse—Comprehensive Textbook for Statistics and Data Analysis; Mitp Verlags GmBH & Co.: Frechen, Germany, 2018. [Google Scholar]
- Rudolf, M.; Müller, J. Multivariate Analyses; Hogrefe: Goettingen, Germany, 2004. [Google Scholar]
- Hall, K.A.; Singh, M.; Mukherjee, S.; Palmer, L.J. Physical activity is associated with reduced prevalence of self-reported obstructive sleep apnea in a large, general population cohort study. J. Clin. Sleep Med. 2020, 16, 1179–1187. [Google Scholar] [CrossRef] [PubMed]
- Gottlieb, D.J.; Punjabi, N.M. Diagnosis and Management of Obstructive Sleep Apnea: A Review. Jama 2020, 323, 1389–1400. [Google Scholar] [CrossRef]
- Lorenzi-Filho, G.; Almeida, F.R.; Strollo, P.J. Treating OSA: Current and emerging therapies beyond CPAP. Respirology 2017, 22, 1500–1507. [Google Scholar] [CrossRef]
- Van Offenwert, E.; Vrijsen, B.; Belge, C.; Troosters, T.; Buyse, B.; Testelmans, D. Physical activity and exercise in obstructive sleep apnea. Acta Clin. Belg. 2019, 74, 92–101. [Google Scholar] [CrossRef] [PubMed]
- Booth, F.W.; Roberts, C.K.; Laye, M.J. Lack of exercise is a major cause of chronic diseases. Compr. Physiol. 2012, 2, 1143–1211. [Google Scholar] [CrossRef] [PubMed]
- Brand, S.; Ebner, K.; Mikoteit, T.; Lejri, I.; Gerber, M.; Beck, J.; Holsboer-Trachsler, E.; Eckert, A. Influence of Regular Physical Activity on Mitochondrial Activity and Symptoms of Burnout-An Interventional Pilot Study. J. Clin. Med. 2020, 9, 667. [Google Scholar] [CrossRef] [PubMed]
- Cowan, R.E. Exercise Is Medicine Initiative: Physical Activity as a Vital Sign and Prescription in Adult Rehabilitation Practice. Arch. Phys. Med. Rehabil. 2016, 97, S232–S237. [Google Scholar] [CrossRef] [PubMed]
- Ekelund, U.; Steene-Johannessen, J.; Brown, W.J.; Fagerland, M.W.; Owen, N.; Powell, K.E.; Bauman, A.; Lee, I.M. Does physical activity attenuate, or even eliminate, the detrimental association of sitting time with mortality? A harmonised meta-analysis of data from more than 1 million men and women. Lancet 2016. [Google Scholar] [CrossRef]
- Every-Palmer, S.; Huthwaite, M.A.; Elmslie, J.L.; Grant, E.; Romans, S.E. Long-term psychiatric inpatients’ perspectives on weight gain, body satisfaction, diet and physical activity: A mixed methods study. BMC Psychiatry 2018, 18, 300. [Google Scholar] [CrossRef]
- Geneen, L.J.; Moore, R.A.; Clarke, C.; Martin, D.; Colvin, L.A.; Smith, B.H. Physical activity and exercise for chronic pain in adults: An overview of Cochrane Reviews. Cochrane Database Syst. Rev. 2017, 4, Cd011279. [Google Scholar] [CrossRef]
- Heath, G.W.; Kolade, V.O.; Haynes, J.W. Exercise is Medicine: A pilot study linking primary care with community physical activity support. Prev. Med. Rep. 2015, 2, 492–497. [Google Scholar] [CrossRef]
- Militello, L.K.; Kelly, S.; Melynk, B.M.; Smith, L.; Petosa, R. A Review of Systematic Reviews Targeting the Prevention and Treatment of Overweight and Obesity in Adolescent Populations. J. Adolesc. Health 2018. [Google Scholar] [CrossRef]
- Ranasinghe, C.D.; Ranasinghe, P.; Jayawardena, R.; Misra, A. Physical activity patterns among South-Asian adults: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2013, 10, 116. [Google Scholar] [CrossRef] [PubMed]
- Bailey, A.P.; Hetrick, S.E.; Rosenbaum, S.; Purcell, R.; Parker, A.G. Treating depression with physical activity in adolescents and young adults: A systematic review and meta-analysis of randomised controlled trials. Psychol. Med. 2017, 1–20. [Google Scholar] [CrossRef]
- Ochentel, O.; Humphrey, C.; Pfeifer, K. Efficacy of Exercise Therapy in Persons with Burnout. A Systematic Review and Meta-Analysis. J. Sports Sci. Med. 2018, 17, 475–484. [Google Scholar]
- Paluska, S.A.; Schwenk, T.L. Physical activity and mental health: Current concepts. Sports Med. 2000, 29, 167–180. [Google Scholar] [CrossRef] [PubMed]
- Zschucke, E.; Gaudlitz, K.; Strohle, A. Exercise and physical activity in mental disorders: Clinical and experimental evidence. J. Prev. Med. Public Health Yebang Uihakhoe Chi 2013, 46 (Suppl. S1), S12–S21. [Google Scholar] [CrossRef]
- Banno, M.; Harada, Y.; Taniguchi, M.; Tobita, R.; Tsujimoto, H.; Tsujimoto, Y.; Kataoka, Y.; Noda, A. Exercise can improve sleep quality: A systematic review and meta-analysis. PeerJ 2018, 6, e5172. [Google Scholar] [CrossRef]
- Chennaoui, M.; Arnal, P.J.; Sauvet, F.; Leger, D. Sleep and exercise: A reciprocal issue? Sleep Med. Rev. 2015, 20, 59–72. [Google Scholar] [CrossRef]
- Gerber, M.; Brand, S.; Holsboer-Trachsler, E.; Puhse, U. Fitness and exercise as correlates of sleep complaints: Is it all in our minds? Med. Sci. Sports Exerc. 2010, 42, 893–901. [Google Scholar] [CrossRef]
- Kredlow, M.A.; Capozzoli, M.C.; Hearon, B.A.; Calkins, A.W.; Otto, M.W. The effects of physical activity on sleep: A meta-analytic review. J. Behav. Med. 2015, 38, 427–449. [Google Scholar] [CrossRef]
- Lang, C.; Brand, S.; Feldmeth, A.K.; Holsboer-Trachsler, E.; Puhse, U.; Gerber, M. Increased self-reported and objectively assessed physical activity predict sleep quality among adolescents. Physiol. Behav. 2013, 120, 46–53. [Google Scholar] [CrossRef]
- Merrill, R.M.; Aldana, S.G.; Greenlaw, R.L.; Diehl, H.A.; Salberg, A. The effects of an intensive lifestyle modification program on sleep and stress disorders. J. Nutr. Health Aging 2007, 11, 242–248. [Google Scholar]
- Morgan, K. Daytime activity and risk factors for late-life insomnia. J. Sleep Res. 2003, 12, 231–238. [Google Scholar] [CrossRef]
- Rubio-Arias, J.; Marín-Cascales, E.; Ramos-Campo, D.J.; Hernandez, A.V.; Pérez-López, F.R. Effect of exercise on sleep quality and insomnia in middle-aged women: A systematic review and meta-analysis of randomized controlled trials. Maturitas 2017, 100, 49–56. [Google Scholar] [CrossRef]
- Sadeghi Bahmani, D.; Gonzenbach, R.; Motl, R.W.; Bansi, J.; Rothen, O.; Niedermoser, D.; Gerber, M.; Brand, S. Better Objective Sleep Was Associated with Better Subjective Sleep and Physical Activity; Results from an Exploratory Study under Naturalistic Conditions among Persons with Multiple Sclerosis. Int. J. Environ. Res. Public Health 2020, 17, 3522. [Google Scholar] [CrossRef]
- Labarca, G.; Dreyse, J.; Drake, L.; Jorquera, J.; Barbe, F. Efficacy of continuous positive airway pressure (CPAP) in the prevention of cardiovascular events in patients with obstructive sleep apnea: Systematic review and meta-analysis. Sleep Med. Rev. 2020, 52, 101312. [Google Scholar] [CrossRef]
- Ahmadpanah, M.; Paghale, S.J.; Bakhtyari, A.; Kaikhavani, S.; Aghaei, E.; Nazaribadie, M.; Holsboer-Trachsler, E.; Brand, S. Effects of psychotherapy in combination with pharmacotherapy, when compared to pharmacotherapy only on blood pressure, depression, and anxiety in female patients with hypertension. J. Health Psychol. 2016, 21, 1216–1227. [Google Scholar] [CrossRef]
- Nagele, E.; Jeitler, K.; Horvath, K.; Semlitsch, T.; Posch, N.; Herrmann, K.H.; Grouven, U.; Hermanns, T.; Hemkens, L.G.; Siebenhofer, A. Clinical effectiveness of stress-reduction techniques in patients with hypertension: Systematic review and meta-analysis. J. Hypertens. 2014, 32, 1936–1944, discussion 1944. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.; Johnson, B.T.; Acabchuk, R.L.; Chen, S.; Lewis, H.K.; Livingston, J.; Park, C.L.; Pescatello, L.S. Yoga as Antihypertensive Lifestyle Therapy: A Systematic Review and Meta-analysis. Mayo Clin. Proc. 2019, 94, 432–446. [Google Scholar] [CrossRef]
- Dickinson, H.O.; Campbell, F.; Beyer, F.R.; Nicolson, D.J.; Cook, J.V.; Ford, G.A.; Mason, J.M. Relaxation therapies for the management of primary hypertension in adults. Cochrane Database Syst. Rev. 2008. [Google Scholar] [CrossRef] [PubMed]
- Shao, C.; Qi, H.; Fang, Q.; Tu, J.; Li, Q.; Wang, L. Smoking history and its relationship with comorbidities in patients with obstructive sleep apnea. Tob. Induc. Dis. 2020, 18, 56. [Google Scholar] [CrossRef] [PubMed]
- Deleanu, O.-C.; Pocora, D.; Mihălcuţă, S.; Ulmeanu, R.; Zaharie, A.-M.; Mihălţan, F.D. Influence of smoking on sleep and obstructive sleep apnea syndrome. Pneumologia 2016, 65, 28–35. [Google Scholar] [PubMed]
- Bielicki, P.; Trojnar, A.; Sobieraj, P.; Wąsik, M. Smoking status in relation to obstructive sleep apnea severity (OSA) and cardiovascular comorbidity in patients with newly diagnosed OSA. Adv. Respir. Med. 2019, 87, 103–109. [Google Scholar] [CrossRef]
- Hsu, W.-Y.; Chiu, N.-Y.; Chang, C.-C.; Chang, T.-G.; Lane, H.-Y. The association between cigarette smoking and obstructive sleep apnea. Tob. Induc. Dis. 2019, 17, 27. [Google Scholar] [CrossRef]
- Casasola, G.G.; Marques, J.A.; Sánchez-Alarcos, J.M.; Tashkin, D.P.; Espinós, D. Cigarette smoking behavior and respiratory alterations during sleep in a healthy population. Sleep Breath. 2002, 6, 19–24. [Google Scholar] [CrossRef]
- Chang, E.T.; Baik, G.; Torre, C.; Brietzke, S.E.; Camacho, M. The relationship of the uvula with snoring and obstructive sleep apnea: A systematic review. Sleep Breath. 2018, 22, 955–961. [Google Scholar] [CrossRef] [PubMed]
- Rezaie, L.; Fobian, A.D.; McCall, W.V.; Khazaie, H. Paradoxical insomnia and subjective–objective sleep discrepancy: A review. Sleep Med. Rev. 2018, 40, 196–202. [Google Scholar] [CrossRef]
- Park, K.-M.; Kim, S.-Y.; Sung, D.; Kim, H.; Kim, B.-N.; Park, S.; Jung, K.-I.; Park, M.-H. The relationship between risk of obstructive sleep apnea and other sleep problems, depression, and anxiety in adolescents from a community sample. Psychiatry Res. 2019, 280, 112504. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Ren, R.; Lei, F.; Zhou, J.; Zhang, J.; Wing, Y.-K.; Sanford, L.D.; Tang, X. Worldwide and regional prevalence rates of co-occurrence of insomnia and insomnia symptoms with obstructive sleep apnea: A systematic review and meta-analysis. Sleep Med. Rev. 2019, 45, 1–17. [Google Scholar] [CrossRef]
- Akinci, B.; Aslan, G.K.; Kiyan, E. Sleep quality and quality of life in patients with moderate to very severe chronic obstructive pulmonary disease. Clin. Respir. J. 2018, 12, 1739–1746. [Google Scholar] [CrossRef] [PubMed]
- Garbarino, S.; Scoditti, E.; Lanteri, P.; Conte, L.; Magnavita, N.; Toraldo, D.M. Obstructive Sleep Apnea With or Without Excessive Daytime Sleepiness: Clinical and Experimental Data-Driven Phenotyping. Front. Neurol. 2018, 9, 505. [Google Scholar] [CrossRef] [PubMed]
- Srijithesh, P.; Aghoram, R.; Goel, A.; Dhanya, J. Positional therapy for obstructive sleep apnoea. Cochrane Database Syst. Rev. 2019. [Google Scholar] [CrossRef] [PubMed]
- Grace, K.P.; Hughes, S.W.; Horner, R.L. Identification of the mechanism mediating genioglossus muscle suppression in REM sleep. Am. J. Respir. Crit. Care Med. 2013, 187, 311–319. [Google Scholar] [CrossRef]
- Aurora, R.N.; Crainiceanu, C.; Gottlieb, D.J.; Kim, J.S.; Punjabi, N.M. Obstructive sleep apnea during REM sleep and cardiovascular disease. Am. J. Respir. Crit. Care Med. 2018, 197, 653–660. [Google Scholar] [CrossRef]
- Bradley, T.D.; Floras, J.S. Obstructive sleep apnoea and its cardiovascular consequences. Lancet 2009, 373, 82–93. [Google Scholar] [CrossRef]
- Drager, L.F.; McEvoy, R.D.; Barbe, F.; Lorenzi-Filho, G.; Redline, S. Sleep apnea and cardiovascular disease: Lessons from recent trials and need for team science. Circulation 2017, 136, 1840–1850. [Google Scholar] [CrossRef]
- Smith, G. Step away from stepwise. J. Big Data 2018, 5, 32. [Google Scholar] [CrossRef]
- Labarca, G.; Saavedra, D.; Dreyse, J.; Jorquera, J.; Barbe, F. Efficacy of CPAP for Improvements in Sleepiness, Cognition, Mood, and Quality of Life in Elderly Patients With OSA: Systematic Review and Meta-analysis of Randomized Controlled Trials. Chest 2020, 158, 751–764. [Google Scholar] [CrossRef] [PubMed]
- Zinchuk, A.V.; Gentry, M.J.; Concato, J.; Yaggi, H.K. Phenotypes in obstructive sleep apnea: A definition, examples and evolution of approaches. Sleep Med. Rev. 2017, 35, 113–123. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variables | Mean (SD) |
|---|---|
| Age (years) | 49.50 (12.70) |
| Height (cm) | 170.92 (9.90) |
| Weight (kg) | 88.18 (15.63) |
| BMI | 30.18 (5.07) |
| Neck circumference (cm) | 40.23 (3.58) |
| Waist circumference (cm) | 104.17 (13.14) |
| Gender | Frequency (%) |
| Female | 73 (29.1) |
| Male | 178 (70.9) |
| Medical history | Frequency (%) |
| No | 91 (36.3) |
| Cardiovascular diseases | 83 (33.1) |
| Respiratory diseases | 23 (9.2) |
| Neurologic diseases | 31 (12.4) |
| Diabetes | 23 (9.2) |
| Hypertension | 86 (34.3) |
| Smoking | Frequency (%) |
| Yes | 59 (23.5) |
| No | 192 (76.5) |
| Chief Sleep Complaints | Frequency (%) |
| Snoring | 190 (75.6) |
| Insomnia | 32 (12.3) |
| Excessive daytime sleepiness | 13 (5) |
| Sleepwalking | 5 (1.9) |
| Nightmare | 4 (1.5) |
| Nocturia | 4 (1.5) |
| Morning headache | 3 (1.2) |
| A | ||||||||||
| Dimensions | ||||||||||
| 1 Age | 2 BMI | 3 Neck | 4 Waist | 5 Daytime Sleepiness | 6 Sleep Quality | 7 Risk OSAa | 8 TST | 9 Wakenings | ||
| 1 | Age | - | .16 * | −.06 | .11 | .12 | .11 | .13 * | −.27 ** | .19 * |
| 2 | BMI | - | .33 *** | .58 *** | .15 * | −.16 * | .23 *** | −.17 * | .07 | |
| 3 | Neck circumference | - | .42 *** | .13 * | −.12 * | .04 | .00 | .00 | ||
| 4 | Waist circumference | - | .13 | −.07 | .23 ** | −.05 | .05 | |||
| 5 | Daytime sleepiness | - | −.04 | .63 *** | −.07 | .08 | ||||
| 6 | Sleep quality | - | .04 | −.04 | .08 | |||||
| 7 | Risk OSAS | - | .00 | .02 | ||||||
| 8 | TST | - | −.69 *** | |||||||
| Statistics | ||||||||||
| M (SD) | 49.50 (12.70) | 30.18 (5.07) | 40.23 (3.58) | 104.17 (13.14) | 8.96 (5.00) | 7.62 (4.77) | 4.69 (1.43) | 6.25 (1.16) | 5.08 (4.36) | |
| B | ||||||||||
| Dimensions | ||||||||||
| 10 Sleep efficiency | 11 N1 | 12 N2 | 13 N3 | 14 REM | 15 AHI | 16 RDI | 17 SpO2 | 18 SI | ||
| 1 | Age | −.27 *** | .00 | .04 | −.13 | .09 | .20 *** | .19 ** | −.32 *** | −.05 |
| 2 | BMI | −.23 *** | .02 | .01 | −.21 ** | .16 ** | .50 *** | .50 *** | −.38 *** | .28 *** |
| 3 | Neck circumference | .05 | .29 *** | −.18 ** | −.04 | −.15 * | .20 ** | .23 *** | .07 | .12 |
| 4 | Waist circumference | −.09 | .10 | .02 | −.25 ** | .07 | .29 *** | .30 *** | −.19 ** | .26 *** |
| 5 | Daytime sleepiness | −.10 | −.01 | .02 | −.02 | .06 | .21 *** | .22 *** | −.22 *** | .06 |
| 6 | Sleep quality | .02 | .01 | −.06 | .00 | .13* | −.09 | −.08 | .02 | −.09 |
| 7 | Risk OSAS | −.04 | .02 | .05 | −.15 | .00 | .25 *** | .24 *** | −.17 *** | .18 *** |
| 8 | TST | .91 *** | .20 *** | −.18 *** | .18 *** | −.28 *** | −.12 | −.07 | .26 *** | −.17 ** |
| 9 | Wakenings | −.78 *** | .07 | .02 | −.23 *** | .15 ** | .05 | .03 | −.17 ** | .13 * |
| 10 | Sleep efficiency | - | .16 * | −.17 ** | .26 ** | −.32 ** | −.14 ** | −.09 | .29 ** | .12 |
| 11 | N1 (%) | - | −.76 *** | −.09 | −.32 ** | −.02 | .07 | .12 | .03 | |
| 12 | N2 (%) | - | −.39 *** | −.02 | .05 | −.05 | −.06 | .08 | ||
| 13 | N3 (%) | - | −.23 *** | −.19 *** | −.16 *** | −.02 | −.09 | |||
| 14 | REM (%) | - | .21 ** | .19 ** | −.10 | −.14 * | ||||
| 15 | AHI | - | .97 *** | −.32 *** | .28 *** | |||||
| 16 | RDI | - | −.33 ** | .28 ** | ||||||
| 17 | SpO2 (mean) | - | −.05 | |||||||
| 18 | Snoring index | - | ||||||||
| Statistics | ||||||||||
| M (SD) | 82.19 (13.21) | 39.83 (22.11) | 33.03 (22.99) | 15.48 (14.82) | 11.35 (11.76) | 29.62 (20.61) | 33.91 (21.56) | 89.96 (6.91) | 2.17 (0.99) | |
| AHI | |||||
|---|---|---|---|---|---|
| Mild | Moderate | Severe | X2-Test | ||
| Gender | Female | 23 | 24 | 26 | X2(N = 251, df = 2) = 0.48 |
| Male | 55 | 52 | 71 | ||
| Smoking | Yes | 15 | 22 | 22 | X2(N = 251, df = 2) = 2.08 |
| No | 63 | 54 | 75 | ||
| Hypertension | Yes | 22 | 18 | 46 | X2(N = 251, df = 2) = 12.51 ** |
| No | 56 | 58 | 51 | ||
| Cardiovascular diseases | Yes | 22 | 20 | 41 | X2(N = 251, df = 2) = 6.11 * |
| No | 56 | 56 | 56 | ||
| Diabetes | Yes | 6 | 8 | 9 | X2(N = 251, df = 2) = 0.34 |
| No | 72 | 68 | 88 | ||
| AHI (Categories) | ||||||
|---|---|---|---|---|---|---|
| Mild | Moderate | Severe | F-Tests | Partial Eta-Squared | Post Hoc Comparisons | |
| N 78 | 75 | 97 | ||||
| Mean (SD) | Mean (SD) | Mean (SD) | ||||
| Age (years) | 47.10 (13.48) | 47.63 (13.14) | 52.73 (11.03) | 5.54 | .043 (S) | severe > mild |
| BMI | 27.12 (4.22) | 29.98 (3.79) | 32.80 (5.19) | 34.29 | .217 (L) | severe > moderate > mild |
| Neck circumference (cm) | 39.78 (3.62) | 39.68 (3.56) | 41.04 (3.45) | 4.10 | .032 (S) | severe > mild |
| Waist circumference (cm) | 100.09 (11.05) | 102.49 (11.43) | 108.93 (14.44) | 11.68 | .086 (L) | severe > mild |
| PSQI | 8.67 (5.16) | 6.95 (4.21) | 7.23 (4.71) | 3.01 | 0.24 (L) | severe = moderate = mild |
| ESS | 8.21 (4.87) | 8.52 (5.15) | 9.96 (4.89) | 3.15 | 0.25 (L) | severe = moderate = mild |
| STOP-Bang | 4.41 (1.33) | 4.48 (1.58) | 5.10 (1.29) | 6.61 | 0.051 (S) | Severe > mild |
| RDI (event/hour) | 14.37 (6.38) | 25.77 (6.33) | 56.04 (16.95) | 301.31 | 0.70 (L) | severe > moderate > mild |
| REM stage (%) | 9.28 (8.41) | 9.75 (10.61) | 14.24 (14.17) | 4.99 | 0.39 (L) | severe > mild |
| Stage N1 (%) | 38.20 (21.79) | 39.33 (21.26) | 41.20 (23.02) | 0.41 | 0.003 (T) | severe = moderate = mild |
| Stage N2 (%) | 35.46 (23.37) | 31.71 (23.25) | 32.31 (22.58) | 0.60 | 0.005 (T) | severe = moderate = mild |
| Stage N3 (%) | 16.63 (14.78) | 18.58 (14.87) | 12.12 (14.35) | 4.47 | 0.035 (S) | Moderate>severe |
| Total sleep time (h) | 6.31 (1.15) | 6.36 (1.21) | 6.09 (1.11) | 1.41 | 0.011 (T) | severe = moderate = mild |
| Sleep efficiency (%) | 83.85 (12.6) | 83.52 (13.9) | 79.82 (12.9) | 2.50 | 0.20 (L) | severe = moderate = mild |
| Wake index | 4.83 (4.20) | 4.80 (4.85) | 5.52 (4.09) | 0.76 | 0.006 (T) | severe = moderate = mild |
| Mean SpO2(%) | 92.37 (2.99) | 90.61 (6.95) | 87.55 (8.30) | 11.91 | 0.083 (M) | severe > mild |
| Snore index | 224.37 (167.04) | 286.50 (196.12) | 341.34 (199.50) | 8.29 | 0.63 (L) | severe > mild |
| Dimension | Variables | Coefficient | Standard Error | Coefficient β | t | p | R | R2 | Durbin–Watson |
|---|---|---|---|---|---|---|---|---|---|
| AHI | Intercept | −.085 | 2.026 | - | −.042 | .967 | .970 | .943 | 2.085 |
| RDI | .925 | .015 | .969 | 62.38 | .000 | ||||
| N2 sleep (%) | .078 | .014 | .087 | 5.524 | .000 | ||||
| Total sleep time (h) | −.677 | .281 | −.038 | −2.41 | .017 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rezaie, L.; Maazinezhad, S.; Fogelberg, D.J.; Khazaie, H.; Sadeghi-Bahmani, D.; Brand, S. Compared to Individuals with Mild to Moderate Obstructive Sleep Apnea (OSA), Individuals with Severe OSA Had Higher BMI and Respiratory-Disturbance Scores. Life 2021, 11, 368. https://doi.org/10.3390/life11050368
Rezaie L, Maazinezhad S, Fogelberg DJ, Khazaie H, Sadeghi-Bahmani D, Brand S. Compared to Individuals with Mild to Moderate Obstructive Sleep Apnea (OSA), Individuals with Severe OSA Had Higher BMI and Respiratory-Disturbance Scores. Life. 2021; 11(5):368. https://doi.org/10.3390/life11050368
Chicago/Turabian StyleRezaie, Leeba, Soroush Maazinezhad, Donald J. Fogelberg, Habibolah Khazaie, Dena Sadeghi-Bahmani, and Serge Brand. 2021. "Compared to Individuals with Mild to Moderate Obstructive Sleep Apnea (OSA), Individuals with Severe OSA Had Higher BMI and Respiratory-Disturbance Scores" Life 11, no. 5: 368. https://doi.org/10.3390/life11050368
APA StyleRezaie, L., Maazinezhad, S., Fogelberg, D. J., Khazaie, H., Sadeghi-Bahmani, D., & Brand, S. (2021). Compared to Individuals with Mild to Moderate Obstructive Sleep Apnea (OSA), Individuals with Severe OSA Had Higher BMI and Respiratory-Disturbance Scores. Life, 11(5), 368. https://doi.org/10.3390/life11050368