
The Impact of Epigallocatechin Gallate and Coconut Oil Treatment on Cortisol Activity and Depression in Multiple Sclerosis Patients



 ,
, 
 ,
,  and
and 
Abstract
1. Introduction
2. Materials and Methods
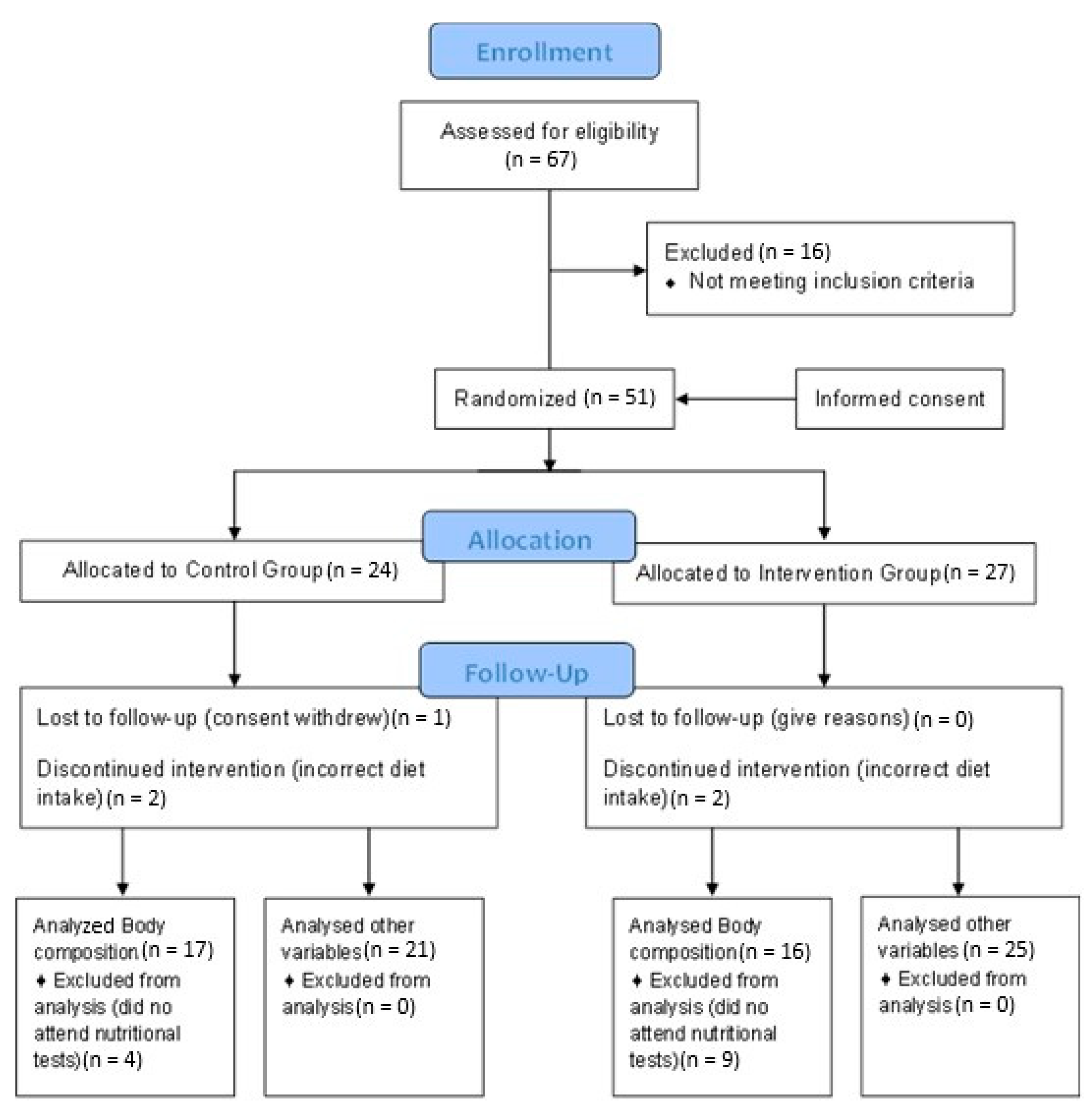
2.1. Subjects
2.2. Statistical Analysis
2.3. Procedure
2.4. Intervention
2.5. Measurements
2.6. Ethical Concerns
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Kutzelnigg, A.; Lassmann, H. Pathology of multiple sclerosis and related inflammatory demyelinating diseases. Handb. Clin. Neurol. 2014, 122, 15–58. [Google Scholar] [CrossRef] [PubMed]
- Fetisova, E.; Chernyak, B.; Korshunove, G.; Muntyan, M.; Skulachev, V. Mitochondria-targeted antioxidants as a prospective therapeutic strategy for multiple sclerosis. Curr. Med. Chem. 2017, 24, 2086–2114. [Google Scholar] [CrossRef] [PubMed]
- Spiers, J.G.; Chen, H.J.; Sernia, C.; Lavidis, N.A. Activation of the hypothalamic-pituitary-adrenal stress axis induces cellular oxidative stress. Front. Neurosci. 2014, 8, 456. [Google Scholar] [CrossRef]
- Holsboer, F. The corticosteroid receptor hypothesis of depression. Neuropsychopharmacology 2000, 23, 477–501. [Google Scholar] [CrossRef]
- Gold, P.W.; Drevets, W.C.; Charney, D.S. New insights into the role of cortisol and the glucocorticoid receptor in severe depression. Biol. Psychiatry 2002, 52, 381–385. [Google Scholar] [CrossRef]
- Pandya, R.; Metz, L.; Patten, S.B. Predictive value of the CES-D in detecting depression among candidates for disease-modifying multiple sclerosis treatment. Psychosomatics 2005, 46, 131–134. [Google Scholar] [CrossRef] [PubMed]
- Feinstein, A.; Magalhaes, S.; Richard, J.F.; Audet, B.; Moore, C. The link between multiple sclerosis and depression. Nat. Rev. Neurol. 2014, 10, 507–517. [Google Scholar] [CrossRef] [PubMed]
- Melief, J.; de Wit, S.J.; van Eden, C.G.; Teunissen, C.; Hamann, J.; Uitdehaag, B.M.; Swaab, D.; Huitinga, I. HPA axis activity in multiple sclerosis correlates with disease severity, lesion type and gene expression in normal-appearing white matter. Acta Neuropathol. 2013, 126, 237–249. [Google Scholar] [CrossRef]
- Lisieski, M.J.; Eagle, A.L.; Conti, A.C.; Liberzon, I.; Perrine, S.A. Single-prolonged stress: A review of two decades of progress in a rodent model of post-traumatic stress disorder. Front. Psychiatry 2018, 9, 248–255. [Google Scholar] [CrossRef]
- Zhang, L.; Zhou, R.; Li, X.; Ursano, R.J.; Li, H. Stress-induced change of mitochondria membrane potential regulated by genomic and non-genomic GR signalling: A possible mechanism for hippocampus atrophy in PTSD. Med. Hypotheses 2006, 66, 1205–1208. [Google Scholar] [CrossRef]
- Vogelzangs, N.; Kritchevsky, S.B.; Beekman, A.T.; Newman, A.B.; Satterfield, S.; Simonsick, E.M.; Yaffe, K.; Harris, T.B.; Penninx, B.W. Depressive symptoms and change in abdominal obesity in older persons. Arch. Gen. Psychiatry 2008, 65, 1386–1393. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez, A.C.I.; Epel, E.S.; White, M.L.; Standen, E.C.; Seckl, J.R.; Tomiyama, A.J. Hypothalamic-pituitery-adrenal axis dysregulation and cortisol activity in obesity: A systematic review. Psychoneuroendocrinology 2015, 63, 301–318. [Google Scholar] [CrossRef] [PubMed]
- Tettey, P.; Simpson, S.; Taylor, B.; Ponsonby, A.L.; Lucas, R.M.; Dwyer, T.; Kostner, K.; group, A.i.; van der Mei, I.A. An adverse lipid profile and increased levels of adiposity significantly predict clinical course after a first demyelinating event. J. Neurol. Neurosurg. Psychiatry 2017, 88, 395–401. [Google Scholar] [CrossRef]
- Khan, Q.U.; Zaffar, S.; Rehan, A.M.; Rashid, R.R.; Ashraf, H.; Hafeez, F. Relationship of major depression with body mass index and salivary cortisol. Cureus 2020, 12. [Google Scholar] [CrossRef] [PubMed]
- Engeli, S.; Bohnke, J.; Feldpausch, M.; Gorzelniak, K.; Heintze, U.; Janke, J.; Luft, F.C.; Sharma, A.M. Regulation of 11beta-HSD genes in human adipose tissue: Influence of central obesity and weight loss. Obes. Res. 2004, 12, 9–17. [Google Scholar] [CrossRef] [PubMed]
- Keenan, D.M.; Roelfsema, F.R.; Veldhuis, J.D. Endogenous ACTH concentration-dependent drive of cortisol secretion in the human. Am. J. Physiol. Endocrinol. Metab. 2004, 287, 652–661. [Google Scholar] [CrossRef] [PubMed]
- Lin, H.Y.; Muller, Y.A.; Hammond, G.L. Molecular and structural basis of steroid hormone binding and release from corticosteroid-binding globulin. Mol. Cell Endocrinol. 2010, 316, 3–12. [Google Scholar] [CrossRef] [PubMed]
- Harper, M.E.; Dugaiczyk, A. Linkage of the evolutionarily-related serum albumin and alpha-fetoprotein genes within q11-22 of human chromosome 4. Am. J. Hum. Genet. 1983, 35, 565–572. [Google Scholar]
- Kessing, L.V.; Harhoff, M.; Andersen, P.K. Increased rate of treatment with antidepressants in patients with multiple sclerosis. Int. Clin. Psychopharmacol. 2008, 23, 54–59. [Google Scholar] [CrossRef] [PubMed]
- Cordeau, D.; Courtois, F. Sexual disorders in women with MS: Assessment and management. Ann. Phys. Rehabil. Med. 2014, 57, 337–347. [Google Scholar] [CrossRef]
- Lew-Starowicz, M.; Rola, R. Sexual dysfunctions and sexual quality of life in men with multiple sclerosis. J. Sex. Med. 2014, 11, 1294–1301. [Google Scholar] [CrossRef]
- Farkhondeh, T.; Yazdi, H.S.; Samarghandian, S. The Protective Effects of Green Tea Catechins in the Management of Neurodegenerative Diseases: A Review. Curr. Drug Discov. Technol. 2019, 16, 57–65. [Google Scholar] [CrossRef] [PubMed]
- Morris, G.; Maes, M.; Berk, M.; Carvalho, A.F.; Puri, B.K. Nutritional ketosis as an intervention to relieve astrogliosis: Possible therapeutic applications in the treatment of neurodegenerative and neuroprogressive disorders. Eur. Psychiatry 2020, 63, e8. [Google Scholar] [CrossRef]
- Loftis, J.M.; Wilhelm, C.J.; Huckans, M. Effect of epigallocatechin gallate supplementation in schizophrenia and bipolar disorder: An 8-week, randomized, double-blind, placebo-controlled study. Ther. Adv. Psychopharmacol. 2013, 3, 21–27. [Google Scholar] [CrossRef] [PubMed]
- Rai, A.; Gill, M.; Kinra, M.; Shetty, R.; Krishnadas, N.; Rao, C.M.; Sumalatha, S.; Kumar, N. Catechin ameliorates depressive symptoms in spraguedawley rats subjected to chronic unpredictable mild stress by decreasing oxidative stress. Biomed. Rep. 2019, 11, 79–84. [Google Scholar] [CrossRef] [PubMed]
- Brietzke, E.; Mansur, R.B.; Subramaniapillai, M.; Balanzá-Martínez, V.; Vinberg, M.; González-Pinto, A.; Rosenblat, J.D.; Ho, R.; McIntyre, R.S. Ketogenic diet as a metabolic therapy for mood disorders: Evidence and developments. Neurosci. Biobehav. Rev. 2018, 94, 11–16. [Google Scholar] [CrossRef]
- Guan, Y.F.; Huang, G.B.; Xu, M.D.; Gao, F.; Lin, S.; Huang, J.; Wang, J.; Li, Y.Q.; Wu, C.H.; Yao, S.; et al. Anti-depression effects of ketogenic diet are mediated via the restoration of microglial activation and neuronal excitability in the lateral habenula. Brain Behav. Immun. 2020, 88, 748–762. [Google Scholar] [CrossRef]
- Klaus, S.; Pültz, S.; Thöne-Reineke, C.; Wolfram, S. Epigallocatechin gallate attenuates diet-induced obesity in mice by decreasing energy absorption and increasing fat oxidation. Int. J. Obes. 2005, 29, 615–623. [Google Scholar] [CrossRef]
- Basu, A.; Sanchez, K.; Leyva, M.J.; Wu, M.; Betts, N.M.; Aston, C.E.; Lyons, T.J. Green tea supplementation affects body weight, lipids, and lipid peroxidation in obese subjects with metabolic syndrome. J. Am. Coll. Nutr. 2010, 29, 31–40. [Google Scholar] [CrossRef] [PubMed]
- Chen, I.J.; Liu, C.; Chiu, J.P.; Hsu, C.H. Therapeutic effect of high-dose green tea extract on weight reduction: A randomized, double-blind, placebo-controlled clinical trial. Clin. Nutr. 2016, 35, 592–599. [Google Scholar] [CrossRef]
- Bueno, N.B.; de Melo, I.S.; de Oliveira, S.L.; da Rocha Ataide, T. Very-low-carbohydrate ketogenic diet v. Low-fat diet for long-term weight loss: A meta-analysis of randomised controlled trials. Br. J. Nutr. 2013, 110, 1178–1187. [Google Scholar] [CrossRef] [PubMed]
- Moreno, B.; Crujeiras, A.B.; Bellido, D.; Sajoux, I.; Casanueva, F.F. Obesity treatment by very low-calorie-ketogenic diet at two years: Reduction in visceral fat and on the burden of disease. Endocrine 2016, 54, 681–690. [Google Scholar] [CrossRef]
- Volek, J.S.; Phinney, S.D. The Art and Science of Low Carbohydrate Living, Beyond Obesity; LLC: New York, NY, USA, 2011. [Google Scholar]
- Esparza-Ros, F.; Vaquero-Cristóbal, R.; Marfell-Jones, M. Protocolo Internacional Para la Valoración Antropométrica. In Perfil Completo. Murcia: International Society for the Advancement of Kinanthropometry-ISAK, 3rd ed.; Universidad Católica San Antonio de Murcia: Murcia, Spain, 2019. [Google Scholar]
- Huxley, R.; Mendis, S.; Zheleznyakov, E.; Reddy, S.; Chan, J. Body mass index, waist circumference and waist: Hip ratio as predictors of cardiovascular risk—A review of the literature. Eur. J. Clin. Nutr. 2010, 64, 16–22. [Google Scholar] [CrossRef]
- Sanz, J.; Perdigón, A.L.; Vázquez, C. Adaptación española del Inventario para la Depresión de Beck-II (BDI-II): 2. Propiedades psicométricas en población general. Clin. Sal. 2003, 14, 249–280. [Google Scholar]
- Michalos, A.C. Encyclopedia of Quality of Life and Well-Being Research; Springer: Dordrecht, The Netherlands, 2014. [Google Scholar]
- World Medical Association. World medical association declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA 2013, 10, 2191–2194. [Google Scholar] [CrossRef]
- Patten, S.B.; Marrie, R.A.; Carta, M.G. Depression in multiple sclerosis. Int. Rev. Psychiatry 2017, 29, 463–472. [Google Scholar] [CrossRef] [PubMed]
- Wens, I.; Dalgas, U.; Vandenabeele, F.; Krekels, M.; Grevendonk, L.; Eijnde, B.O. Multiple sclerosis affects skeletal muscle characteristics. PLoS ONE 2014, 9, 1–5. [Google Scholar] [CrossRef]
- Stetler, C.; Miller, G.E. Depression and hypothalamic-pituitary-adrenal activation: A quantitative summary of four decades of research. Psychosom. Med. 2011, 73, 114–126. [Google Scholar] [CrossRef] [PubMed]
- Lee, B.; Shim, I.; Lee, H.; Hahm, D.H. Effects of epigallocatechin gallate on behavioural and cognitive impairments, hypothalamic-pituitary-adrenal axis dysfunction, and alternations in hippocampal BDNF expression under single prolonged stress. J. Med. Food 2018, 21, 979–989. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.Q.; Zhao, X.L.; Wang, D.L.; Li, S.T.; Hou, Y.; Hong, Y.; Cheng, Y.Y. Effects of epigallocatechin-3-gallate on behavioral impairments induced by psychological stress in rats. Exp. Biol. Med. 2010, 235, 577–583. [Google Scholar] [CrossRef]
- Hintzpeter, J.; Stapelfeld, C.; Loerz, C.; Martin, H.J.; Maser, E. Green tea and one of its constituents, Epigallocatechine-3-gallate, are potent inhibitors of human 11beta-hydroxysteroid dehydrogenase type 1. PLoS ONE 2014, 9, e84468. [Google Scholar] [CrossRef] [PubMed]
- Hamrahian, A.H.; Oseni, T.S.; Arafah, B.M. Measurements of serum free cortisol in critically ill patients. N. Engl. J. Med. 2004, 350, 1629–1638. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.; Shinzawa, H.; Togashi, H.; Takahashi, T.; Kuzumaki, T.; Otsu, K.; Ishikawa, K. Interleukin-6 down-regulates expressions of the aldolase B and albumin genes through a pathway involving the activation of tyrosine kinase. Arch. Biochem. Biophys. 1995, 320, 203–209. [Google Scholar] [CrossRef]
- Visser, M.; Kritchevsky, S.B.; Newman, A.B.; Goodpaster, B.H.; Tylavsky, F.A.; Nevitt, M.C.; Harris, T.B. Lower serum albumin concentration and change in muscle mass: The health, aging and body composition study. Am. J. Clin. Nutr. 2005, 82, 531–537. [Google Scholar] [CrossRef]
- Hryhorczuk, C.; Sharma, S.; Fulton, S.E. Metabolic disturbances connecting obesity and depression. Front. Neurosci. 2013, 7, 1–14. [Google Scholar] [CrossRef]
- Wiltink, J.; Michal, M.; Wild, P.S.; Zwiener, I.; Blettner, M.; Münzel, T.; Schulz, A.; Kirschner, Y.; Beutel, M.E. Associations between depression and different measures of obesity (BMI, WC, WHtR, WHR). BMC Psychiatry 2013, 13, 1–7. [Google Scholar] [CrossRef]
- Carrasco-Pozo, C.; Cires, M.J.; Gotteland, M. Prevention and treatment of obesity: From molecular to clinical studies. J. Med. Food 2019, 22, 753–770. [Google Scholar] [CrossRef] [PubMed]
- Li, F.; Gao, C.; Zhang, M.; Wang, Y.; Hu, Y.; Wu, X.; Wang, X.; Sheng, J. EGCG reduces obesity and white adipose tissue gain partly through AMPK activation in mice. Front. Pharmacol. 2018, 9, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Ettinger, S.; Mahan, L.K.; Escott-Stump, S. Macronutrimentos: Carbohidratos, Proteínas y Lípidos. In Nutrición y Dietoterapia de Krause, 10th ed.; Mc Graw-Hill: Girona, Spain, 2001; pp. 46–59. [Google Scholar]
- DiNicolantionio, J.J.; O’Keele, J.H. Good fats versus bad fats: A comparison of fatty acids in the promotion of insulin resistance, inflammation and obesity. Mol. Med. 2017, 114, 303–307. [Google Scholar]
- Gibson, A.A.; Seimon, R.V.; Lee, C.M.Y.; Ayre, J.; Franklin, J.; Markovic, T.P.; Caterson, I.D.; Sainsbury, A. Do ketogenic diets really suppress appetite? A systematic review and meta-analysis. Obes. Rev. 2015, 16, 64–76. [Google Scholar] [CrossRef] [PubMed]
- Sussman, D.; Germann, J.; Henkelman, M. Gestational ketogenic diet programs brain structure and susceptibility to depression and anxiety in the adult mouse offspring. Brain Behav. 2015, 5, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Murphy, P.; Likhodii, S.; Nylen, K.; Burnham, V.M. The antidepressant properties of the ketogenic diet. Biol. Psych. 2004, 56, 981–983. [Google Scholar] [CrossRef]
- Alcocer-Gómez, E.; de Miguel, M.; Casas-Barquero, N.; Núñez-Vasco, J.; Sánchez-Alcazar, A.; Fernández-Rodríguez, A.; Cordero, M.D. NLRP3 inflammasome is activated in mononuclear blood cells form patients with major depressive disorder. Brain Behav. Immun. 2014, 36, 111–117. [Google Scholar] [CrossRef] [PubMed]
- Kaufmann, F.N.; Costa, A.P.; Ghisleni, G.; Diaz, A.P.; Rodrigues, A.L.S.; Peluffo, H.; Kaster, M.P. NLRP3 inflammasome-driven pathways in depression: Clinical and preclinical findings. Brain Behav. Immun. 2017, 64, 367–383. [Google Scholar] [CrossRef]
- Boeschoten, R.E.; Braamse, A.M.J.; Beekman, A.T.F.; Cuijpers, P.; van Oppen, P.; Dekker, J.; Uitdehaag, B.M.J. Prevalence of depression and anxiety in Multiple Sclerosis: A systematic review and meta-analysis. J. Neurol. Sci. 2017, 372, 331–341. [Google Scholar] [CrossRef]
- Gay, M.C.; Bungener, C.; Thomas, S.; Vrignaud, P.; Thomas, P.W.; Baker, R.; Montel, S.; Heinzlef Papeix, C.; Assouad, R.; Montreuil, M. Anxiety, emotional processing and depression in people with multiple sclerosis. BMC Neurol. 2017, 17, 43. [Google Scholar] [CrossRef] [PubMed]
- Wallis, O.; Bol, Y.; Köhler, S.; van Heugten, C. Anxiety in multiple sclerosis is related to depressive symptoms and cognitive complaints. Acta Neurol. Scand. 2020, 141, 212–218. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Control Group N = 24 | Intervention Group N = 27 | Chi2 | p | ||||
|---|---|---|---|---|---|---|---|
| Count | % | Count | % | ||||
| Relapsing-remitting MS | 17 | 70.8% | 20 | 74.1% | 0.067 | 0.796 | |
| Secondary-progressive MS | 7 | 29.2% | 7 | 25.9% | |||
| Men | 10 | 41.7% | 5 | 18.5% | 3.279 | 0.070 | |
| Women | 14 | 58.3% | 22 | 81.5% | |||
| Mean | SD | Mean | SD | Z | p | ||
| Age (years) | 49.83 | 12.42 | 44.56 | 11.27 | −1.558 | 0.119 | |
| Time since diagnosis (years) | 14.21 | 8.40 | 11.89 | 9.74 | −1.418 | 0.156 | |
| Pre-test | Albumin (g/dL) | 4.66 | 0.41 | 4.69 | 0.29 | −0.414 | 0.679 |
| Cortisol (µg/dL) | 15.50 | 5.86 | 12.22 | 4.59 | −1.930 | 0.054 | |
| BHB (Mmol/L) | 0.05 | 0.02 | 0.06 | 0.04 | −0.932 | 0.351 | |
| Depression | 11.17 | 8.66 | 13.59 | 8.70 | −1.096 | 0.273 | |
| Waist-to-hip ratio | 0.95 | 0.08 | 0.89 | 0.10 | −1.625 | 0.104 | |
| Body fat mass (%) | 18.85 | 5.00 | 19.53 | 3.78 | −0.764 | 0.445 | |
| Fat weight | 14.27 | 7.47 | 13.65 | 5.26 | −0.311 | 0.755 | |
| Muscle mass (%) | 38.38 | 4.15 | 39.39 | 2.88 | −0.547 | 0.584 | |
| Weight (kg) | 70.44 | 18.13 | 68.63 | 13.56 | −0.245 | 0.806 | |
| Control Group | Pre (N = 21) | Post (N = 21) | ||||
|---|---|---|---|---|---|---|
| Median | Range | Median | Range | Z | p | |
| Cortisol (µg/dl) | 16.30 | 23.85 | 13.10 | 29.36 | −1.731 | 0.884 |
| Albumin (g/dL) | 4.65 | 1.43 | 4.69 | 1.80 | −1.469 | 0.142 |
| Depression | 9.50 | 34.00 | 9.00 | 27.00 | −2.508 | 0.072 |
| BHB (Mmol/L) | 0.04 | 0.06 | 0.03 | 0.17 | −1.254 | 0.210 |
| Pre (N = 25) | Post (N = 25) | |||||
| Intervention Group | Median | Range | Median | Range | Z | p |
| Cortisol (µg/dL) | 11.90 | 18.44 | 11.05 | 18.01 | −0.317 | 0.751 |
| Albumin (g/dL) | 4.65 | 1.14 | 4.81 | 0.86 | −2.375 | 0.018 * |
| Depression | 12.00 | 28.00 | 8.00 | 24.00 | −2.704 | 0.007 * |
| BHB (Mmol/L) | 0.05 | 0.16 | 0.05 | 0.33 | −2.005 | 0.045 * |
| Control Group | Pre (N = 17) | Post (N = 17) | ||||
|---|---|---|---|---|---|---|
| Median | Range | Median | Range | Z | p | |
| WHR | 0.93 | 0.39 | 0.94 | 0.40 | −0.492 | 0.623 |
| Body fat mass (%) | 18.19 | 16.19 | 17.72 | 19.22 | −0.644 | 0.520 |
| Fat weight | 12.61 | 26.77 | 12.71 | 28.10 | −0.355 c | 0.723 |
| Muscle mass (%) | 38.88 | 16.30 | 39.10 | 17.69 | −1.738 | 0.082 |
| Weight (kg) | 62.45 | 68.60 | 61.00 | 63.00 | −2.723 | 0.006 * |
| Pre (N = 16) | Post (N = 16) | |||||
| Intervention Group | Median | Range | Median | Range | Z | p |
| WHR | 0.90 | 0.35 | 0.88 | 0.30 | −2.183 | 0.029 * |
| Body fat mass (%) | 19.40 | 14.50 | 17.63 | 13.34 | −4.421 | 0.000 *** |
| Fat weight | 12.95 | 20.85 | 11.17 | 18.51 | −4.373 | 0.000 *** |
| Muscle mass (%) | 39.77 | 12.68 | 40.68 | 11.97 | −2.955 | 0.003 ** |
| Weight (kg) | 64.50 | 56.10 | 65.50 | 53.00 | −3.076 | 0.002 ** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Platero, J.L.; Cuerda-Ballester, M.; Sancho-Cantus, D.; Benlloch, M.; Ceron, J.J.; Peres Rubio, C.; García-Pardo, M.P.; López-Rodríguez, M.M.; de la Rubia Ortí, J.E. The Impact of Epigallocatechin Gallate and Coconut Oil Treatment on Cortisol Activity and Depression in Multiple Sclerosis Patients. Life 2021, 11, 353. https://doi.org/10.3390/life11040353
Platero JL, Cuerda-Ballester M, Sancho-Cantus D, Benlloch M, Ceron JJ, Peres Rubio C, García-Pardo MP, López-Rodríguez MM, de la Rubia Ortí JE. The Impact of Epigallocatechin Gallate and Coconut Oil Treatment on Cortisol Activity and Depression in Multiple Sclerosis Patients. Life. 2021; 11(4):353. https://doi.org/10.3390/life11040353
Chicago/Turabian StylePlatero, Jose Luis, María Cuerda-Ballester, David Sancho-Cantus, María Benlloch, Jose Joaquin Ceron, Camila Peres Rubio, María Pilar García-Pardo, María Mar López-Rodríguez, and Jose Enrique de la Rubia Ortí. 2021. "The Impact of Epigallocatechin Gallate and Coconut Oil Treatment on Cortisol Activity and Depression in Multiple Sclerosis Patients" Life 11, no. 4: 353. https://doi.org/10.3390/life11040353
APA StylePlatero, J. L., Cuerda-Ballester, M., Sancho-Cantus, D., Benlloch, M., Ceron, J. J., Peres Rubio, C., García-Pardo, M. P., López-Rodríguez, M. M., & de la Rubia Ortí, J. E. (2021). The Impact of Epigallocatechin Gallate and Coconut Oil Treatment on Cortisol Activity and Depression in Multiple Sclerosis Patients. Life, 11(4), 353. https://doi.org/10.3390/life11040353