Abstract
Chronic kidney disease (CKD) is one of the most important risk factors for cardiovascular disease (CVD). Despite the kidney having no direct implications for lipoproteins metabolism, advanced CKD dyslipidemia is usually present in patients with CKD, and the frequent lipid and lipoprotein alterations occurring in these patients play a role of primary importance in the development of CVD. Although hypertriglyceridemia is the main disorder, a number of lipoprotein abnormalities occur in these patients. Different enzymes pathways and proteins involved in lipoprotein metabolism are impaired in CKD. In addition, treatment of uremia may modify the expression of lipoprotein pattern as well as determine acute changes. In renal transplantation recipients, the main lipid alteration is hypercholesterolemia, while hypertriglyceridemia is less pronounced. In this review we have analyzed lipid and lipoprotein disturbances in CKD and also their relationship with progression of renal disease. Hypolipidemic treatments may also change the natural history of CVD in CKD patients and may represent important strategies in the management of CKD patients.
1. Introduction
Chronic kidney disease (CKD) is one of the most important risk factors for cardiovascular disease (CVD) [1]. Several studies have established that cardiovascular (CV) mortality increases with decreasing glomerular filtration rate (GFR), and all recent guidelines have included patients with CKD among those who have a defined high or very high risk in relation to the value of GFR [2,3]. In patients with CKD, the prevalence of major CV risk factors such as diabetes mellitus and hypertension is particularly high; also, many of the so-called “emerging” risk factors (e.g., endothelial dysfunction, inflammation, oxidative stress, etc.) are present in patients with CKD and can contribute to negatively modulate cardiovascular risk [4]. However, the frequent lipid (cholesterol and triglycerides) and lipoprotein (chylomicrons; very low-density lipoprotein-VLDL; intermediate-density lipoprotein-IDL; low-density lipoprotein-LDL; and high-density lipoprotein-HDL) alterations occurring in these patients play a role of primary importance in this context [5].
2. Chronic Renal Failure (CRF)
Although the kidney has no direct implications for lipoproteins metabolism CRF dyslipidemia is usually present in patients with CRF [6]. This metabolic alteration is characterized by both quantitative and qualitative modifications of lipoproteins that significantly impact the development of accelerated atherosclerotic lesions of these subjects and probably influence the progression of the renal disease itself [7,8]. Main lipids and lipoprotein abnormalities in CRF are summarized in the Table 1 and Table 2. CRF patients exhibit high triglyceride levels, low high-density lipoprotein (HDL) levels, and normal or even low total cholesterol and low-density lipoprotein (LDL) cholesterol levels, but an atherogenic profile is hidden behind this spectrum of lipoprotein derangement [9]. This profile includes the increase in apolipoprotein (apo) B, lipoprotein (a) (Lp (a)), intermediate (IDL) and very low-density lipoproteins (VLDL), small and dense LDL and the reduction of HDL [10,11]. Furthermore, in patients with more severe CRF, LDL are often modified, leading to the increased formation of oxidized LDL [12].

Table 1.
Lipids and lipoprotein abnormalities in CKD patients.
Table 2.
Comparison in the main lipid and lipoprotein abnormalities between different types of CKD.
2.1. Triglyceride Rich Lipoprotein (TRL) Particles and CKD
Hypertriglyceridemia is a common feature in patients with CKD and this is due to an increased concentration of triglyceride-rich lipoproteins (TRL) (VLDL, chylomicrons and their remnants) [13,14,15]. Hypertriglyceridemia occurs both due to an increased production in the liver and to a delayed peripheral catabolism of TRL [16,17,18]. Figure 1 summarizes the main pathways involved on hypertriglyceridemia in Chronic Kidney Disease. An increased hepatic overproduction of VLDL may contribute to the increase in triglyceride levels in CKD patients [19,20]. Liver directly synthesizes VLDL, which, by the triglyceride hydrolase properties of lipoprotein (LPL) and hepatic lipase (HL), finally turns out to LDL [21]. LPL is an essential enzyme in the lipolysis of the triglyceride-rich lipoproteins (VLDL and chylomicrons), binds to the endothelial surface of the capillaries by interacting with the heparin sulfate proteoglycans and through the endothelium-derived glycosylphosphatidylinositol-anchored binding protein-1 (GPIHBP-1): this factor anchors LPL and acts as a ligand for chylomicrons [22]. LPL initially leads to the production of intermediated-sized lipoproteins (IDL and remnants), which may be either further processed by HL to form LDL or to be removed from plasma by receptor-mediated mechanisms [23]. Lipoproteins are actually heterogenous particles with discrete subspecies migrating in the same density interval and having a different atherogenetic role. IDL and remnants are rapidly removed from plasma in normal subjects, but represent potentially dangerous lipoprotein subpopulations [24]. Smaller and denser TRL particles are likely to better represent remnant lipoproteins as well as particles rich in apoE, and these specific TRL subspecies have been documented to be raised in CHD patients [25,26]. Enhanced hepatic lipoprotein synthesis and secretion should be induced by the hyperinsulinemia and insulin resistance often associated with CKD [27]. Insulin resistance activates the transport of free fatty acids (FFAs) to the liver and consequently promotes the oxidation or esterification of FFAs to cytosolic triglycerides or VLDL [28]. However the delayed catabolism seems to be the main mechanism responsible for the elevated concentration of TRL [29,30]. Despite secondary hyperparathyroidism playing a role in this impaired removal of TRL, this probably occurs due to a decrease in LPL and HL activities [31,32,33]. In addition, the presence of lipase inhibitors can further impair TRL catabolism [34]. CKD patients show higher levels of apolipoprotein CIII (apoC-III), which represent the physiological inhibitor of LPL [35,36]. It has been also demonstrated that VLDL of CRF patients is a poor substrate for bovine LPL in vitro [37]. Beyond low LPL and HL activities, these data suggest that structural alterations of LPL substrate might impair LPL activity in CKD [38,39], though CRF patients accumulate remnant particles and these abnormalities are commonly not detectable when fasting lipid profile is determined [40,41]. The causes underlying remnant accumulation in CKD patients are not completely understood. Although a down-regulation of hepatic receptors involved in IDL and remnant uptake may contribute to increase plasma residence time of these particles, impaired lipolysis might determine the accumulation of atherogenic remnants [42]. CKD patients have also a significant trigger of overproduction of TRL, which may potentially jeopardize the metabolism of remnant particles [43]. Combing both mechanisms, in a such defective lipolytic system, the remnant overloading could no longer permit an efficient removal of those particles, finally resulting in the accumulation of atherogenic TRL remnant fractions into the bloodstream. Since advanced CKD lipoprotein abnormalities mainly affect TRL, these are poorly modified by statins, having in the LDL the main target by decreasing hepatic cholesterol synthesis and enhancing apolipoprotein B (apoB) receptor expression [44,45].
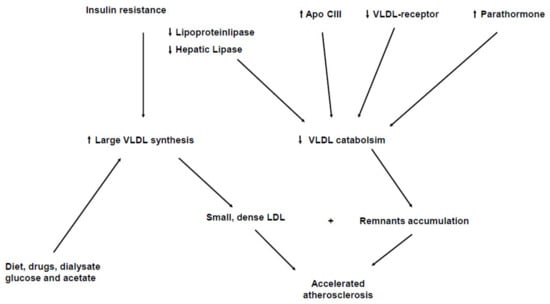
Figure 1.
Mechanisms underlying hypertrigliceridemia in Chronic Kidney Disease.
2.2. Other Lipoprotein Abnormalities and CKD
Although LDL cholesterol is generally not elevated in CKD patients, a higher prevalence of small, dense LDL has been found [46]. These particles are more easily oxidized and penetrate more easily into the endothelial wall; for this reason they are more atherogenic, and thus, subjects who have higher, smaller and denser lipoproteins are at higher atherogenic risk [47]. In CKD is also observed a significant increase of plasma levels of Lp(a), which is also affected by the GFR [11,48,49]. Lp(a) levels are genetically determined and represent a strong risk factor for cardiovascular and cerebrovascular diseases [50]. Even if the mechanisms underlying the increase of Lp(a) in CKD are not completed clarified, it has been hypothesized that the kidney is involved in the catabolism of this particle [51]. In a homogeneous population of nondiabetic subjects without lipid-lowering therapy, serum proprotein convertase subtilisin kexin type 9 (PCSK9), which physiologically induces the degradation of LDL receptor, was not associated with GFR at several stages of CKD. However, PCSK9 was involved in the altered metabolism of TRL observed in CKD [52]. Thus, even if kidney function per se does not directly influence significantly PCSK9 metabolism, the real role of PCSK9 inhibitors in CKD should be considered. Another lipoprotein abnormality in CKD patients concerns HDL. The main function of HDL is the reverse transport of cholesterol, a process that includes the transport of cholesterol from the arterial wall to the liver for further excretion. Patients with CKD exhibit reduced HDL-cholesterol levels [53,54]. This is due to lower levels of apolipoprotein AI and AII, major components of HDL, but also to impaired activity of lecithin-cholesterol acyltransferase (LCAT), the key enzyme for the esterification of free cholesterol into HDL [55]. Moreover other processes involved in HDL metabolism are altered in CKD, such as an increased transfer of cholesterol esters to triglyceride-rich lipoproteins by the cholesterol ester transfer protein (CETP), a reduced activity of HDL-associated enzymes, such as paraoxonases, which may be responsible for the altered antioxidant and anti-inflammatory function of HDL [56,57]. All of these factors may contribute to reduce the antiatherosclerotic properties of HDL in this patient population.
A recent study has analyzed the association between the change of lipoprotein and the kidney outcomes in patients with stage 3–5 CKD over 3.2 years of follow-up. It has been shown that stage 3 CKD subjects with increased and high variable LDL-C levels exhibit an increased risk of progression to advanced CKD stages to dialysis. No significant difference on this correlation was found in patients with CKD stage 4 or 5. These results suggest that an efficacious lipid-lowering treatment is crucial to improve clinical outcomes, especially in patients with CKD stage 3 [58].
2.3. Lipid Abnormalities in CKD Patients on Hemodialysis and Peritoneal Dialysis
Patients with end-stage renal failure (ESRF) treated with different dialytic procedures (hemodialysis–HD–or continuous ambulatory peritoneal dialysis–CAPD) exhibit a different pattern of dyslipidemia. It was found that ESRF subjects on HD mainly present with hypertriglyceridemia, high apoB levels, low HDL-C and low apoA-I levels, while in patients on CAPD cholesterol serum levels also are increased [15]. Lp(a) levels are a 3-fold increase both on HD and CAPD compared to nonadvanced CKD patients [15]. Hemodialysis also determines acute relevant changes of lipoprotein profile, leading to a massive reduction of plasma triglyceride and increase of HDL-cholesterol level [59,60,61]. This is due to the acute lipolysis stimulation determined by heparin [62]. Heparin solubilizes LPL from the vascular endothelium and only the released enzyme exerts the metabolic effect on TRL [63]. It is not clear if these represent positive changes. LPL activity during heparin administration increases rapidly in ESRF subjects during the first hour, with a consequent triglyceride reduction, but still remains only half of that of normal controls [64]. In a previous work, we reported a selective decrease of the large triglyceride-rich particles with a concomitant raise of smaller VLDL and IDL together with apoE-rich fractions and non-HDL cholesterol levels [65]. Thus, at the end of dialysis procedure, there is an acute production of atherogenic TRL particles. CRF patients have to be treated by hemodialysis three to four times/week, so the adverse effect of the periodical heparin infusion should be accurately considered [66]. In EDRF patients treated by CAPD patients, an increased lipoprotein production appears to be the prevalent pathogenetic mechanism. In this category of subjects there are also higher levels of total and LDL cholesterol in comparison with other CKD patients [67,68]; the high absorption of glucose from the dialysis fluid probably lead to an increase in insulin levels resulting in the liver overproduction of lipoproteins [69]. In addition, acetate present in CAPD dialysis fluids might influence lipogenetic biochemical pathways and enhance VLDL secretion with a higher prevalence of hyperapobetalipoproteinemia [15]. HD and CAPD are usually similar in terms of long-term survival even though the risk factors for cardiometabolic syndrome are different between the two procedures. It has been demonstrated that patients on CAPD have a high prevalence of metabolic syndrome with weight gain and BMI increase, high fasting blood glucose, high HbA1c levels, insulin resistance and LDL-C increase, mainly due to extra calories from the dialysis fluid when compared to subjects on HD [70]. Recently it was shown that CKD patients on CAPD exhibit higher systolic and diastolic blood pressure than HD subjects regardless of slow and continuous manner of their procedure [71]. This is probably due to the hypervolemia condition consequent to high sodium intake, insufficient ultrafiltration or wrong evaluation of their dry weight [72]. On the contrary, Tonbul et al. reported that patients on HD present often with higher left ventricular mass index and are frequently nondippers compared with patients on CAPD [73]. Serum albumin is lower in CAPD patients due to several factors: among these, the significant loss of albumin during the procedure, the increased protein catabolic state and often the small protein intake typical of CKD patients [71]. Glucose-based dialysates exert systemic glucotoxic effects that may increase the risk of inflammation, oxidative stress and atherosclerosis [73]. In addition, on CAPD, plasma fibrinogen and serum homocysteine levels are significantly higher than on HD, even though there are not differences in subclinical atherosclerosis [70] as well as in hs-CRP and Lp(a) levels [74]. CRP indirectly promotes cardiovascular events through the activation of monocytes and complement factors, thus exposing patients on CAPD to high prevalence of major acute cardiovascular events compared with subjects on HD [71]. Further studies in this field are needed to elucidate if additional factors may be involved in the pathogenesis of cardiovascular disease in CKD patients regardless of the dialysis procedure applied.
3. Nephrotic Syndrome
Nephrotic syndrome is one of the most common manifestations of glomerular damage characterized by proteinuria (>3.5 g/1.73 m2/day), low albuminemia levels, edema and hyperlipidemia. The latter is the result of different modifications of lipoprotein metabolism in terms of both qualitative and quantitative changes [75,76], independently of any progression to CKD. Plasma cholesterol, triglycerides as well as all apo B-containing lipoproteins (VLDL, IDL, LDL and Lp(a)), are increased in nephrotic syndrome; on the contrary HDL are normal or decreased [75]. These disorders are mainly caused by alterations in the activity of the key factors that are candidates in the regulation of the physiological steps (assembly, transport, secretion, catabolism) of lipoproteins. Nephrotic syndrome is characterized by an important increase of serum total cholesterol and LDL cholesterol due to alterations of the mechanisms of production/clearance of LDL and apoB-100 [77,78]. PCSK9 and the liver tissue inducible degrader of the LDL receptor (IDOL) are increased in this specific kidney disease and together determine an important LDL receptor deficiency, a decreased hepatic uptake of LDL and consequently increased LDL cholesterol plasma levels [79]. In addition, nephrotic syndrome determines a significant increase of the activity of the acyl-CoA cholesterol acyltransferase-2 (ACAT-2) in the liver, thus inducing a growth of the cholesterol esterification, a decrease of the intracellular free cholesterol and the activation of 3-hydroxy-3-methylglutaryl-CoA (HMG-CoA) reductase, thus enhancing the cholesterol production and consequently hypercholesterolemia [80]. Several studies have shown a lack of LPL in nephrotic syndrome probably due to post-transcriptional or post-translational alterations involving also its cofactor GPIHBP1 [81]. LPL and GPIHBP1 downregulation are also associated with the apolipoprotein E and apolipoprotein CII decrease and apo CIII/ CII ratio increase in TRL [81]. Another intermediary in LPL deficiency is represented by ANGPTL4, a glycoprotein expressed in several tissues that physiologically inhibits LPL activity and is upregulated in nephrotic syndrome as emerging studies have demonstrated [82], thus contributing to hypertriglyceridemia pathogenesis. Consequently LPL-mediated lipolysis of VLDL and chylomicrons is inadequate and causes the progressive accumulation of serum triglycerides, the increase of VLDL triglycerides content, the impaired clearance of chylomicrons and the lipemia post-meal observed over nephrotic syndrome [76]. Hypertriglyceridemia is also related to HL and VLDL receptor deficiency. HL is involved in the IDL hydrolysis and their clearance of the TG content to be transformed in LDL. It has been shown that also in nephrotic syndrome the dysfunction of these factors induces an increase of atherogenic IDL and triglyceride accretion of LDL and HDL content [83,84]. Nephrotic syndrome determines several alterations in the morphology and functions of HDL, mainly due to impairment of their key structural proteins and of the reverse cholesterol transport process [85], thus influencing the atherogenic manifestations of this renal injury. Furthermore, Lp(a) is marked increased in nephrotic syndrome [86], mainly due to hypoalbuminemia through a process requiring apoB enhanced production, which determines an augmented synthesis of LDL particles to be combined into Lp(a) [87].
4. Renal Transplantation
Renal transplantation is usually characterized by a whole variation of lipid profile [88]. Triglyceride levels decrease, while total and HDL-cholesterol levels significantly increase [88]. It has been shown there is an enhanced production of VLDL by the liver associated with a normal conversion to LDL since LPL activity comes back to normal [88]. On the other hand, lipoprotein abnormalities in renal transplant recipients (RTR) look to depend essentially to the considerable pharmacological interventions to which these patients are exposed; they do not regress automatically and they may affect a large number of subjects over time [89]. In RTR, the main lipid alteration is hypercholesterolemia [87,90], while hypertriglyceridemia is less pronounced. HDL cholesterol levels has been found normal or high in this category of subjects; HDL subfractions are variable since some researchers have demonstrated low levels of HDL2 [91] while others failed to show any decrease of HDL2 particles [92]. Lp(a) are only slightly increased when kidney function improves [15], but its metabolism is not completely known. ApoA-I and apoB are significantly high, and apoC-II, apoC-III and apoE are significantly low. These observations suggest an increased cardiovascular risk in these subjects, and the increase of HDL-C and apoA-I might not be a protective factor. On the other hand, it has been shown that a Mediterranean diet may benefit by inducing an inversion of the increased trend of total cholesterol levels [93]. Recently, a study by Kim JE et al. analyzed the ratio of triglyceride to HDL-C and major cardiovascular events (MACE) in RTR, and showed a significant correlation: based on their findings, the maintenance of acceptable TG/HDL-C levels in these patients may decrease CV risk and increase long-term graft survival [94]. Further studies are needed to clarify the correlation between the lipid abnormalities described and the risk for cardiovascular diseases.
5. Hypolipidemic Treatments and CKD
Three large randomized clinical trials have been specifically carried out in patients with CKD to assess the effect of lipid-lowering treatment with statins on clinical outcomes: Die Deutsche Diabetes Dialyse Studie (4D), A Study to Evaluate the Use of Rosuvastatin in Subjects on Regular Haemodialysis: An Assessment of Survival and Cardiovascular Events (AURORA) and Study of Heart and Renal Protection (SHARP) [95,96,97] (see Table 3). While 4D and AURORA included only patients on hemodialysis, the SHARP trial enrolled patients with CKD at different stages. 4D and AURORA, despite a significant reduction of LDL-cholesterol by atorvastatin and rosuvastatin, respectively, failed to demonstrate effects on major CV events. In the SHARP trial, treatment with simvastatin/ezetimibe reduced the rate of major atherosclerotic events in all subjects except those on hemodialysis at the time of study inclusion [97]. Thus, lowering of LDL-C with statins appears to reduce atherosclerotic CV events in CKD patients who are not in hemodialysis. A more recent meta-analysis confirmed that the rate of reduction of CV events becomes smaller when GFR declines [98]. It is possible that in hemodialysis, atherosclerotic patients are so advanced to eliminate the effectiveness of any lipid-lowering intervention. The ESC/EAS guidelines have taken into account this information, recommending treatment with statins/ezetimibe in patients with CKD still in conservative therapy [2]. The study ALERT (Assessment of Lescol in Renal Transplantation) showed the significant effect of fluvastatin in preventing and decreasing the risk for CV events in kidney transplant recipients [99].
Table 3.
Trials evaluating the reduction of cholesterol-LDL and cardiovascular risk in specific CKD populations.
Moreover, lipid management in CKD subjects is based on recommendations from the major clinical practice guidelines as KDIGO and ACC/AHA, which suggest the use of statins rather than other lipid-lowering therapies, since their efficacy has been already tested in randomized controlled trials (RCTs) [100]. According to the KDIGO guideline, subjects with CKD stages 3–5 (not on dialysis) as well as patients with CKD stages 1–2 (eGFR > 60 mL/min/1.73 m2) aged ≥50 years who have pathological albuminuria (urinary albumin:creatinine ratio >30 mg/g) should be treated with a statin or statin plus ezetimibe combination [99].
KDIGO recommends treatment of dyslipidemia on the basis of CHD risk, which depends maximally by age. However this guideline does not have an upper age limit for therapy recommendations contrary to ACC/AHA guidelines that suggest avoiding statin therapy for primary prevention in CKD patients older than 79. Moreover, KDIGO suggests a statin dose decrease in subjects with an eGFR < 60 mL/min/1.73 m2. So far, there are not randomized trials indicating the benefits of statins in patients with nephrotic syndrome. The effect of statin treatment on mortality in CKD subjects depends on the CKD stage. Patients with stages 2–4 CKD on statin therapy, do not exhibit any difference in terms of mortality compared to placebo. However it has been shown that statins can reduce the mortality in stage 5 CKD subjects [101].
Subgroups of FOURIER and ODYSSEY Outcomes trials have also demonstrated a similar benefit of PCSK9 inhibition independent of kidney function, despite subjects with severely reduced kidney function being excluded [54,102,103], confirming that PCSK9 inhibition might represent an alternative treatment approach in patients with moderate CKD.
There are limited data on PCSK9 inhibitors in CKD. The FOURIER trial evaluated the efficacy and safety of Evolocumab in CKD patients, and a recent analysis of 8 randomized trials on Alirocumab reported that these agents decrease LDL-C and reduce the CV risk among subjects with mild to moderate CKD spectrum. However these studies have some limitations that reflect the small number of patients with stage 3b and 4 CKD and the exclusion of patients with eGFR < 20 mL/min/1.73 m2. Furthermore, their benefits are dependent of the degree of cholesterol lowering and it seems that their efficacy decreases as CKD turns into more severe stages. Further studies are needed to prove the suitability of PCSK9 inhibitors in the treatment of CKD patients [99].
Other lipid-lowering agents are fibrates but to date, very little proofs recommend their use in subjects with CKD, especially in those with eGFR < 30 mL/min//1.73 m2. The only exception might be very high triglyceride levels (>11.3 mmol/L (>1,000 mg/dL) in which these drugs should be used reasonably by adjusting the dose according to kidney function [99].
Bile acid sequestrants such as cholestyramine, colestipol and colesevelam are actually administered as second-line options in subjects with atherosclerotic CV disease, but there is only a little evidence for their use in CKD population. Moreover, since these agents might increase triglyceride levels, their utility in subjects with CKD or ESRF is very limited. To date, there is poor evidence to support the use of omega-3 fatty acids to decrease CV outcomes or ameliorate mortality in patients with CKD or ESRF. On the other hand, two placebo-controlled RCTs, REDUCE-IT (Reduction of Cardiovascular Events with EPA-Intervention Trial) and STRENGTH (Outcomes Study to Assess Statin Residual Risk Reduction with Epanove in High CV Risk Patients with Hypertriglyceridemia), are evaluating the effect of high-dose (4 g) eicosapentaenoic acid on CV outcomes in subjects with hypertriglyceridaemia [99].
6. Lipoprotein Abnormalities and Progression of CKD
Taken together, all these events contribute to the development of cardiovascular diseases (i.e., atherosclerosis) and, at the same time, to the progression of kidney disease [76]. Indeed, more than 30 years ago, the “lipid nephrotoxicity hypothesis” was proposed, in which dyslipidemia may increase the risk of atherothrombotic events, nephrotoxicity, glomerulosclerosis and progressive kidney disease [104]. Hyperlipidemia, particularly TRL and oxidized LDL, induces the production of cytotoxic metabolites, cytokines and reactive oxygen species (ROS) by mesangial cells, causing an injury of the glomerular epithelial and endothelial cells, thus resulting in glomerulosclerosis [105]. It was observed that, in nephrotic syndrome, the free fatty acids are increased and bind to albumin, causing podocyte damage with consequent loss of their morphology and tubulointerstitial injury [104], but the role of dyslipidemia in the pathophysiology of the nephrotic syndrome is still poorly understood [104]. In animal models, lipid alterations induce glomerular and tubular damage, with positive effects induced by hypolipidemic therapy [105,106,107,108]. The mechanisms are not fully understood, but the main hypothesized explanation is related to the inhibition of mevalonate, a known stimulant of cell replication and glomerular proliferation [109]. This accounts for the potential beneficial effect of statins. In humans, association between high LDL levels and decline in renal function in dyslipidemic patients was reported [110]. Conversely, others have shown that high triglyceride levels and low HDL levels are independent risk factors for renal dysfunction but LDL cholesterol levels were not predictive of kidney damage in a relatively short time [111]. Over a longer follow-up period, a significant association between abnormal lipoprotein parameters and the development of renal dysfunction was shown [112]. Moreover, the effects of hypolipidemic treatment on renal disease progression are controversial. In particular, only high-intensity statin therapy seems to improve GFR decline, while low- and moderate-intensity statins did not achieve the same positive results, and statin therapy did not reduce, or even increase, proteinuria in CKD patients [113,114,115,116].
7. Conclusions
Metabolism of lipids and lipoproteins is substantially altered in CKD and the frequent alterations occurring in these patients may promote atherogenesis, playing a role of primary importance in the development of CVD. Elevated plasma levels of apoC-III, apoA-I and the apoB-containing lipoproteins may modify lipoprotein metabolism, leading to the accumulation of atherogenic particles and a profile characterized by elevated triglycerides, Lp(a), dense LDL and low HDL cholesterol. Different enzymes pathways and proteins involved in lipoprotein metabolism are impaired in CKD, and these changes are mainly dependent of the different setting of kidney disease as well as the kidney transplant recipient state. These modifications may be controlled and, although there are limited data on CKD population, lipid-lowering therapies including statin or statin plus ezetimibe combination, PCSK9 inhibitors, omega 3 and fibrates (in selected cases and based on eGFR value) represent important strategies in the management of CKD patients and in the prevention of CV events.
Author Contributions
Writing—original draft preparation, C.M.B., A.B.C., A.G.; Writing—review and editing D.N., M.C., R.C., Supervision M.R.A., E.N. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Go, A.S.; Chertow, G.M.; Fan, D.; McCulloch, C.E.; Hsu, C.Y. Chronic kidney disease and the risks of death, cardiovas-cular events, and hospitalization. New Engl. J. Med. 2004, 351, 1296–1305. [Google Scholar] [CrossRef] [PubMed]
- Gansevoort, R.T.; Correa-Rotter, R.; Hemmelgarn, B.R.; Jafar, T.H.; Heerspink, H.J.L.; Mann, J.F.; Matsushita, K.; Wen, C.P. Chronic kidney disease and cardiovascular risk: Epidemiology, mechanisms, and prevention. Lancet 2013, 382, 339–352. [Google Scholar] [CrossRef]
- Mach, F.; Baigent, C.; Catapano, A.L.; Koskinas, K.C.; Casula, M.; Badimon, L.; Chapman, M.J.; De Backer, G.G.; Delgado, V.; Ference, B.A.; et al. 2019 ESC/EAS Guidelines for the management of dyslipidaemias: Lipid modification to reduce cardiovascular risk: The Task Force for the management of dyslipidaemias of the European Society of Cardiology (ESC) and European Atherosclerosis Society (EAS). Eur. Heart J. 2020, 41, 111–188. [Google Scholar] [CrossRef] [PubMed]
- Drüeke, T.B.; Massy, Z.A. Atherosclerosis in CKD: Differences from the general population. Nat. Rev. Nephrol. 2010, 6, 723–735. [Google Scholar] [CrossRef]
- Kwan, B.C.H.; Kronenberg, F.; Beddhu, S.; Cheung, A.K. Lipoprotein Metabolism and Lipid Management in Chronic Kidney Disease. J. Am. Soc. Nephrol. 2007, 18, 1246–1261. [Google Scholar] [CrossRef]
- Speer, T.; Zewinger, S.; Fliser, D. Uraemic dyslipidaemia revisited: Role of high-density lipoprotein. Nephrol. Dial. Transplant. 2013, 28, 2456–2463. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Vaziri, N.D. Dyslipidemia of chronic renal failure: The nature, mechanisms, and potential consequences. Am. J. Physiol. Physiol. 2006, 290, F262–F272. [Google Scholar] [CrossRef] [PubMed]
- Quaschning, T.; Krane, V.; Metzger, T.; Wanner, C. Abnormalities in uremic lipoprotein metabolism and its impact on cardiovascular disease. Am. J. Kidney Dis. 2001, 38, S14–S19. [Google Scholar] [CrossRef] [PubMed]
- Attman, P.O.; Alaupovic, P.; Tavella, M.; Knight-Gibson, C. Abnormal lipid and apolipoprotein composition of ma-jor lipoprotein density classes in patients with chronic renal failure. Nephrol. Dial. Transplant 1996, 11, 63–69. [Google Scholar] [CrossRef] [PubMed]
- Deighan, C.J.; Caslake, M.J.; McConnell, M.; Boulton-Jones, J.; Packard, C.J. Atherogenic lipoprotein phenotype in end-stage renal failure: Origin and extent of small dense low-density lipoprotein formation. Am. J. Kidney Dis. 2000, 35, 852–862. [Google Scholar] [CrossRef]
- Hopewell, J.C.; Haynes, R.; Baigent, C. The role of lipoprotein (a) in chronic kidney disease. J. Lipid Res. 2018, 59, 577–585. [Google Scholar] [CrossRef] [PubMed]
- Mathur, S.; Devaraj, S.; Jialal, I. Accelerated atherosclerosis, dyslipidemia, and oxidative stress in end-stage renal disease. Curr. Opin. Nephrol. Hypertens. 2002, 11, 141–147. [Google Scholar] [CrossRef] [PubMed]
- Wanner, C.; Quaschning, T. Dyslipidemia and renal disease: Pathogenesis and clinical consequences. Curr. Opin. Nephrol. Hypertens. 2001, 10, 195–201. [Google Scholar] [CrossRef] [PubMed]
- Mesquita, J.; Varela, A.; Medina, J.L. Dyslipidemia in renal disease: Causes, consequences and treatment. Endocrinol. Nutr. 2010, 57, 440–448. [Google Scholar] [CrossRef] [PubMed]
- Barbagallo, C.M.; Averna, M.R.; Sparacino, V.; Galione, A.; Caputo, F.; Scafidi, V.; Amato, S.; Mancino, C.; Cefalù, A.B.; Notarbartolo, A. Lipoprotein (a) levels in end-stage renal failure and renal transplantation. Nephron 1993, 64, 560–564. [Google Scholar] [CrossRef]
- Vaziri, N.D.; Moradi, H. Mechanisms of dyslipidemia of chronic renal failure. Hemodial. Int. 2006, 10, 1–7. [Google Scholar] [CrossRef]
- Lacquaniti, A.; Bolignano, D.; Donato, V.; Bono, C.; Fazio, M.R.; Buemi, M. Alterations of Lipid Metabolism in Chronic Nephropathies: Mechanisms, Diagnosis and Treatment. Kidney Blood Press. Res. 2010, 33, 100–110. [Google Scholar] [CrossRef]
- Chan, M.K.; Persaud, J.; Varghese, Z.; Moorhead, J.F. Pathogenic roles of post-heparin lipases in lipid abnormalities in hemodialysis patients. Kidney Int. 1984, 25, 812–818. [Google Scholar] [CrossRef]
- Keane, W.F.; Tomassini, J.E.; Neff, D.R. Lipid Abnormalities in Patients with Chronic Kidney Disease: Implications for the Pathophysiology of Atherosclerosis. J. Atheroscler. Thromb. 2013, 20, 123–133. [Google Scholar] [CrossRef]
- Vaziri, N.D. Causes of Dysregulation of Lipid Metabolism in Chronic Renal Failure. Semin. Dial. 2009, 22, 644–651. [Google Scholar] [CrossRef]
- Mahley, R.W.; Innerarity, T.L.; Rall, S.C., Jr.; Weisgraber, K.H. Plasma lipoproteins: Apolipoprotein structure and function. J. Lipid Res. 1984, 25, 1277–1294. [Google Scholar] [CrossRef]
- Beigneux, A.P.; Davies, B.; Gin, P.; Weinstein, M.M.; Farber, E.; Qiao, X.; Peale, F.; Bunting, S.; Walzem, R.L.; Wong, J.S.; et al. Glyco-sylphosphatidylinositol-anchored binding protein-1plays a critical role in the lipolytic processing of chylomicrons. Cell Metab. 2007, 5, 279–291. [Google Scholar] [CrossRef] [PubMed]
- Dallinga-Thie, G.M.; Franssen, R.; Mooij, H.L.; Visser, M.E.; Hassing, H.C.; Peelman, F.; Kastelein, J.J.; Péterfy, M.; Nieuwdorp, M. The metabolism of triglyceride-rich lipoproteins revisited: New players, new insight. Atherosclerosis 2010, 211, 1–8. [Google Scholar] [CrossRef]
- Cohn, J.S.; Marcoux, C.; Davignon, J. Detection, Quantification, and Characterization of Potentially Atherogenic Triglyceride-Rich Remnant Lipoproteins. Arter. Thromb. Vasc. Biol. 1999, 19, 2474–2486. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Nordestgaard, B.G.; Tybjaerg-Hansen, A. IDL, VLDL, chylomicrons and atherosclerosis. Eur. J. Epidemiol. 1992, 8, 92–98. [Google Scholar] [CrossRef]
- Barbagallo, C.M.; Rizzo, M.; Noto, D.; Frasheri, A.; Pernice, V.; Rubino, A.; Pieri, D.; Pinto, V.; Cefalù, A.B.; Giordano, C.; et al. Accumulation of ApoE-enriched triglyceride-rich lipoproteins in patients with coro-nary artery disease. Metabolism 2006, 55, 662–668. [Google Scholar] [CrossRef]
- Reaven, G.M. Compensatory Hyperinsulinemia and the Development of an Atherogenic Lipoprotein Profile: The Price Paid to Maintain Glucose Homeostasis in Insulin-Resistant Individuals. Endocrinol. Metab. Clin. N. Am. 2005, 34, 49–62. [Google Scholar] [CrossRef]
- Samouilidou, E.C.; Karpouza, A.P.; Kostopoulos, V.; Bakirtzi, T.; Pantelias, K.; Petras, D.; Tzanatou-Exarchou, H.; Grapsa, E.J. Lipid abnormalities and oxidized LDL in chronic kidney disease patients on hemodialysis and peritoneal dialy-sis. Ren. Fail. 2012, 34, 724–727. [Google Scholar] [CrossRef]
- Stegmayr, B.; Olivecrona, T.; Olivecrona, G. Lipoprotein Lipase Disturbances Induced by Uremia and Hemodialysis. Semin. Dial. 2009, 22, 442–444. [Google Scholar] [CrossRef] [PubMed]
- Huttunen, J.K.; Pasternack, A.; Vänttinen, T.; Ehnholm, C.; A Nikkilä, E. Lipoprotein metabolism in patients with chronic uremia. Effect of hemodialysis on serum lipoproteins and postheparin plasma triglyceride lipases. Acta Medica Scand. 1978, 204, 211–218. [Google Scholar] [CrossRef]
- Liang, K.; Oveisi, F.; Vaziri, N.D. Role of secondary hyperparathyroidism in the genesis of hypertriglyceridemia and VLDL receptor deficiency in chronic renal failure. Kidney Int. 1998, 53, 626–630. [Google Scholar] [CrossRef] [PubMed]
- Vaziri, N.D.; Liang, K. Down-regulation of tissue lipoprotein lipase expression in experimental chronic renal failure. Kidney Int. 1996, 50, 1928–1935. [Google Scholar] [CrossRef] [PubMed]
- Näsström, B.; Stegmayr, B.; Gupta, J.; Olivecrona, G.; Olivecrona, T. A single bolus of a low molecular weight hepa-rin to patients on haemodialysis depletes lipoprotein lipase stores and retards triglyceride clearing. Nephrol. Dial. Transplant. 2005, 20, 1172–1179. [Google Scholar] [CrossRef]
- Cheung, A.K.; Parker, C.J.; Ren, K.; Iverius, P.H. Increased lipase inhibition in uremia: Identification of pre-beta-HDL as a major inhibitor in normal and uremic plasma. Kidney Int. 1996, 49, 1360–1371. [Google Scholar] [CrossRef] [PubMed]
- Averna, M.R.; Barbagallo, C.M.; Galione, A.; Carroccio, A.; Labisi, M.; Marino, G.; Montalto, G.; Notarbartolo, A. Serum apolipoprotein profile of hypertriglyceridemic patients with chronic renal failure on hemodialysis: A comparison with type IV hyperlipoproteinemic patients. Metabolism 1989, 38, 601–602. [Google Scholar] [CrossRef]
- Ooi, E.M.; Chan, D.T.; Watts, G.F.; Chan, D.C.; Ng, T.W.; Dogra, G.K.; Irish, A.B.; Barrett, P.H.R. Plasma apolipoprotein C-III metabolism in patients with chronic kidney disease. J. Lipid Res. 2011, 52, 794–800. [Google Scholar] [CrossRef]
- Arnadottir, M.; Dallongeville, J.; Fruchart, J.C.; Nilsson-Ehle, P. Very-low-density lipoprotein of uremic patients is a poor substrate for bovine lipoprotein lipase in vitro. Metabolism 1996, 45, 686–690. [Google Scholar] [CrossRef]
- Chan, D.T.; Dogra, G.K.; Irish, A.B.; Ooi, E.M.; Barrett, P.H.; Chan, D.C.; Watts, G.F. Chronic kidney disease delays VLDL-apoB-100 particle catabolism: Potential role of apolipoprotein C-III. J. Lipid. Res. 2009, 50, 2524–2531. [Google Scholar] [CrossRef]
- Dautin, G.; Soltani, Z.; Ducloux, D.; Gautier, T.; De Barros, J.P.; Gambert, P.; Lagrost, L.; Masson, D. Hemodialysis reduces plasma apolipoprotein C-I concentration making VLDL a better substrate for lipoprotein lipase. Kidney Int. 2007, 72, 871–878. [Google Scholar] [CrossRef]
- Ikewaki, K.; Schaefer, J.R.; Frischmann, M.E.; Okubo, K.; Hosoya, T.; Mochizuki, S.; Dieplinger, B.; Trenkwalder, E.; Schweer, H.; Kronenberg, F.; et al. Delayed in vivo catabolism of intermediate-density lipoprotein and low-density lipoprotein in hemodialysis patients as potential cause of premature atherosclerosis. Arterioscler. Thromb. Vasc. Biol. 2005, 25, 2615–2622. [Google Scholar] [CrossRef] [PubMed]
- Van Nguyen, S.; Nakamura, T.; Uematsu, M.; Fujioka, D.; Watanabe, K.; Watanabe, Y.; Obata, J.-E.; Nakamura, K.; Kugiyama, K. Remnant lipoproteinemia predicts cardiovascular events in patients with type 2 diabetes and chronic kidney disease. J. Cardiol. 2017, 69, 529–535. [Google Scholar] [CrossRef]
- Kim, C.; Vaziri, N.D.; Hoong, K.M.; Osratola, V.D. Aziri Down-regulation of hepatic LDL receptor-related protein (LRP) in chronic renal failure. Kidney Int. 2005, 67, 1028–1032. [Google Scholar] [CrossRef]
- Levey, A.S.; Astor, B.C.; Stevens, L.A.; Coresh, J. Chronic kidney disease, diabetes, and hypertension: What’s in a name? Kidney Int. 2010, 78, 19–22. [Google Scholar] [CrossRef]
- Vega, G.-L.; Grundy, S.M. Effect of Statins on Metabolism of Apo-B–Containing Lipoproteins in Hypertriglyceridemic Men. Am. J. Cardiol. 1998, 81, 36B–42B. [Google Scholar] [CrossRef]
- Shurraw, S.; Tonelli, M. Statins for treatment of dyslipidemia in chronic kidney disease. Perit. Dial. Int. 2006, 26, 523–539. [Google Scholar] [CrossRef] [PubMed]
- Chu, M.; Wang, A.Y.M.; Chan, I.H.S.; Chui, S.H.; Lam, C.W.K. Serum small-dense LDL abnormalities in chronic renal disease patients. Br. J. Biomed. Sci. 2012, 69, 99–102. [Google Scholar] [CrossRef] [PubMed]
- Berneis, K.K.; Krauss, R.M. Metabolic origins and clinical significance of LDL heterogeneity. J. Lipid Res. 2002, 43, 1363–1379. [Google Scholar] [CrossRef] [PubMed]
- Barbagallo, C.; Averna, M.; Scafidi, V.; Galione, A.; Notarbartolo, A. Increased Lipoprotein (a) Levels in Subjects with Chronic Renal Failure on Hemodialysis. Nephron 1992, 62, 471–472. [Google Scholar] [CrossRef]
- Bajaj, A.; Damrauer, S.M.; Anderson, A.H.; Xie, D.; Budoff, M.J.; Go, A.S.; He, J.; Lash, J.P.; Ojo, A.; Post, W.S.; et al. Chronic Renal Insufficiency Cohort Study I. Lipoprotein(a) and Risk of Myocardial Infarction and Death in Chronic Kidney Disease: Findings from the CRIC Study (Chronic Renal Insufficiency Cohort). Arterioscler. Thromb. Vasc. Biol. 2017, 37, 1971–1978. [Google Scholar] [CrossRef]
- Nordestgaard, B.G.; Langsted, A. Lipoprotein (a) as a cause of cardiovascular disease: Insights from epidemiolo-gy, genetics, and biology. J. Lipid Res. 2016, 57, 1953–1975. [Google Scholar] [CrossRef]
- Frischmann, M.E.; Kronenberg, F.; Trenkwalder, E.; Schaefer, J.R.; Schweer, H.; Dieplinger, B.; Koenig, P.; Ikewaki, K.; Dieplinger, H. In vivo turnover study demonstrates diminished clearance of lipoprotein(a) in hemodialysis patients. Kidney Int. 2007, 71, 1036–1043. [Google Scholar] [CrossRef]
- Morena, M.; Le May, C.; Chenine, L.; Arnaud, L.; Dupuy, A.M.; Pichelin, M.; Leray-Moragues, H.; Chalabi, L.; Canaud, B.; Cristol, J.P.; et al. Plasma PCSK9 concentrations during the course of nondiabetic chronic kidney disease: Rela-tionship with glomerular filtration rate and lipid metabolism. J. Clin. Lipidol. 2017, 11, 87–93. [Google Scholar] [CrossRef]
- Kronenberg, F. HDL in CKD—The Devil Is in the Detail. J. Am. Soc. Nephrol. 2018, 29, 1356–1371. [Google Scholar] [CrossRef] [PubMed]
- Silbernagel, G.; Genser, B.; Drechsler, C.; Scharnagl, H.; Grammer, T.B.; Stojakovic, T.; Krane, V.; Ritz, E.; Wanner, C.; März, W. HDL Cholesterol, Apolipoproteins, and Cardiovascular Risk in Hemodialysis Patients. J. Am. Soc. Nephrol. 2014, 26, 484–492. [Google Scholar] [CrossRef] [PubMed]
- Vaziri, N.D.; Liang, K.; Parks, J.S. Down-regulation of hepatic lecithin: Cholesterolacyltransferase gene expression in chronic renal failure. Kidney Int. 2001, 59, 2192–2196. [Google Scholar] [CrossRef] [PubMed]
- Mikolasevic, I.; Žutelija, M.; Mavrinac, V.; Orlic, L. Dyslipidemia in patients with chronic kidney disease: Etiology and management. Int. J. Nephrol. Renov. Dis. 2017, 10, 35–45. [Google Scholar] [CrossRef] [PubMed]
- Himmelfarb, J. Relevance of Oxidative Pathways in the Pathophysiology of Chronic Kidney Disease. Cardiol. Clin. 2005, 23, 319–330. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.H.; Huang, J.C.; Wu, P.Y.; Chen, S.C.; Chiu, Y.W.; Chang, J.M.; Chen, H.C. Greater low-density lipoprotein cholester-ol variability is associated with increased progression to dialysis in patients with chronic kidney disease stage. Oncotarget 2018, 9, 3242–3253. [Google Scholar] [CrossRef] [PubMed]
- Ambrosch, A.; Domroese, U.; Westphal, S.; Dierkes, J.; Augustin, W.; Neumann, K.H.; Luley, C. Compositional and functional changes of low-density lipoprotein during hemodialysis in patients with ESRD11This work is dedicated to Professor Dr. Dietrich Seidel, Klinikum Groβhadern, University of Munich, on the occasion of his 60th birthday. Kidney Int. 1998, 54, 608–617. [Google Scholar] [CrossRef][Green Version]
- Wanner, C.; Krane, V.; Metzger, T.; Quaschning, T. Lipid changes and statins in chronic renal insufficiency and di-alysis. J. Nephrol. 2001, 14, S76–S80. [Google Scholar]
- Attman, P.-O.; Samuelsson, O.; Johansson, A.-C.; Moberly, J.B.; Alaupovic, P. Dialysis modalities and dyslipidemia. Kidney Int. 2003, 63, S110–S112. [Google Scholar] [CrossRef] [PubMed]
- Schrader, J.; Andersson, L.O.; Armstrong, V.W.; Kundt, M.; Stibbe, W.; Scheler, F. Lipolytic effects of heparin and low molecular weight heparin and their importance in hemodialysis. Semin. Thromb. Hemost. 1990, 16, 41–45. [Google Scholar] [PubMed]
- Näsström, B.; Olivecrona, G.; Olivecrona, T.; Stegmayr, B.G. Lipoprotein lipase during continuous heparin infusion: Tissue stores become partially depleted. J. Lab. Clin. Med. 2001, 138, 206–213. [Google Scholar] [CrossRef] [PubMed]
- Näsström, B.; Olivecrona, G.; Olivecrona, T.; Stegmayr, B.G. Lipoprotein lipase during heparin infusion: Lower ac-tivity in hemodialysis patients. Scand. J. Clin. Lab. Investig. 2003, 63, 45–53. [Google Scholar] [CrossRef] [PubMed]
- Barbagallo, C.M.; Noto, D.; Cefalu’, A.B.; Ganci, A.; Giammarresi, C.; Panno, D.; Cusumano, G.; Greco, M.; Di Gaudio, F.; Averna, M.R. Heparin induces an accumulation of atherogenic lipoproteins during hemodialysis in normolipidemic end-stage renal disease patients. Hemodial. Int. 2014, 19, 360–367. [Google Scholar] [CrossRef] [PubMed]
- Ng, D. Heparin in hypertriglyceridemia: Friend or foe? J. Lab. Clin. Med. 2001, 138, 356–358. [Google Scholar] [CrossRef]
- O’Neal, D.; Lee, P.; Murphy, B.; Best, J. Low-density lipoprotein particle size distribution in end-stage renal disease treated with hemodialysis or peritoneal dialysis. Am. J. Kidney Dis. 1996, 27, 84–91. [Google Scholar] [CrossRef]
- Krediet, R.T.; Balafa, O. Cardiovascular risk in the peritoneal dialysis patient. Nat. Rev. Nephrol. 2010, 6, 451–460. [Google Scholar] [CrossRef]
- Fortes, P.C.; De Moraes, T.P.; Mendes, J.G.; Stinghen, A.E.; Ribeiro, S.C.; Pecoits-Filho, R. Insulin resistance and glucose homeostasis in peritoneal dialysis. Perit. Dial. Int. 2009, 29, 145–148. [Google Scholar] [CrossRef]
- Harmankaya, O.; Akalin, N.; Akay, H.; Okuturlar, Y.; Erturk, K.; Kaptanogullari, H.; Kocoglu, H. Comparison of risk factors for cardiovascular disease in hemodialysis and peritoneal dialysis patients. Clinics 2015, 70, 601–605. [Google Scholar] [CrossRef]
- Zamiah, S.A.K.S.; Draman, C.R.; Seman, M.R.; Safhan, A.F.; Rozalina, R.; Ruzni, N.I.N. The cardiovascular risk factor pro-files among end-stage renal failure patients treated with continuos ambulatory peritoneal dialysis and intermittent emodialysis. Saudi J. Kidney Dis. Transpl. 2018, 29, 114–119. [Google Scholar]
- Tonbul, Z.; Altintepe, L.; Sozlu, C.; Yeksan, M.; Yildiz, A.; Türk, S. Ambulatory blood pressure monitoring in haemo-dialysisand coninuos ambulatori peritoneal dialisi (CAPD) patients. J. Hum. Hypertens. 2002, 16, 585–589. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.W.; Yang, C.Y.; Wu, H.Y.; Liu, K.L.; Su, C.T.; Wu, C.K.; Lee, J.K.; Chiang, C.K.; Cheng, H.T.; Lien, Y.C.; et al. Metabolic syndrome and abdominal fat are associated with inflammation, but not with clinical outcomes, in peritoneal dialysis patients. Cardiovasc. Diabetol. 2013, 12, 86. [Google Scholar] [CrossRef]
- Yilmaz, F.M.; Yilmaz, G.; Duranay, M.; Parpucu, H.; Senes, M.; Tekeli, N.; Yücel, D. Cardiovascular risk factors in he-modialysis and peritoneal dialysis patients. Scan. J. Clin. Lab. Invest. 2005, 65, 739–745. [Google Scholar] [CrossRef] [PubMed]
- Kronenberg, F. Dyslipidemia and nephrotic syndrome: Recent avances. J. Renal Nutr. 2005, 15, 195–203. [Google Scholar] [CrossRef]
- Vaziri, N.D. Disorders of lipid metabolism in nephrotic syndrome: Mechanisms and consequences. Kidney Int. 2016, 90, 41–52. [Google Scholar] [CrossRef] [PubMed]
- Warwick, G.L.; Packard, C.J.; Demant, T.; Bedford, D.K.; Boulton-Jones, J.M.; Shepherd, J. Metabolism of apolipoprotein B-containing lipoproteins in subjects with nephrotic-range proteinuria. Kidney Int. 1991, 40, 129–138. [Google Scholar] [CrossRef]
- Warwick, G.L.; Caslake, M.J.; Boulton-Jones, J.M.; Dagen, M.; Packard, C.J.; Shepherd, J. Low-density lipoprotein me-tabolism in the nephrotic syndrome. Metabolism 1990, 39, 187–192. [Google Scholar] [CrossRef]
- Liu, S.; Vaziri, N.D. Role of PCSK9 and IDOL in the pathogenesis of acquired LDL receptor deficiency and hy-percholesterolemia in nephritic syndrome. Nephrol. Dial. Transplant. 2014, 29, 538–543. [Google Scholar] [CrossRef]
- Vaziri, N.D.; Liang, K.H. Hepatic HMG-CoA reductase gene expression during the course of puromycin-induced nephrosis. Kidney Int. 1995, 48, 1979–1985. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Vaziri, N.D.; Yuan, J.; Ni, Z.; Nicholas, S.B.; Norris, K.C. Lipoprotein lipase deficiency in chronic kidney disease is compounded by downregulation of endothelial GPIHBP1 expression. Clin. Exp. Nephrol. 2012, 16, 238–243. [Google Scholar] [CrossRef] [PubMed]
- Clement, L.C.; Macè, C.; Avila-Casado, C.; Joles, J.A.; Kersten, S.; Chugh, S.S. Circulating angiopoietin-like 4 links pro-teinuria with hypertrigliceridemia in nephrotic syndrome. Nat. Med. 2014, 20, 37–46. [Google Scholar] [CrossRef] [PubMed]
- Liang, K.; Vaziri, N.D. Down-regulation of hepatic lipase expression in experimental nephrotic syndrome. Kidney Int. 1997, 51, 1933–1937. [Google Scholar] [CrossRef]
- Sato, T.; Liang, K.; Vaziri, N.D. Protein restriction and AST-120 improve lipoprotein lipase, hepatic lipase and VLDL receptor in focal glomerulosclerosis. Kidney Int. 2003, 64, 1780–1786. [Google Scholar] [CrossRef]
- Vaziri, N.D. HDL abnormalities in nephrotic syndrome and chronic kidney disease. Nat. Rev. Nephrol. 2015, 12, 37–47. [Google Scholar] [CrossRef]
- Kronenberg, F.; Utermann, G.; Dieplinger, H. Lipoprotein(a) in renal disease. Am. J. Kidney Dis. 1996, 27, 1–25. [Google Scholar] [CrossRef]
- Noto, D.; Barbagallo, C.M.; Cascio, A.L.; Cefalu’, A.B.; Cavera, G.; Caldarella, R.; Marino, G.; Travali, S.; Cutaia, I.; Maringhini, S.; et al. Lipoprotein(a) levels in relation to albumin concentration in childhood nephrotic syndrome. Kidney Int. 1999, 55, 2433–2439. [Google Scholar] [CrossRef][Green Version]
- Cassader, M.; Ruiu, G.; Gambino, R.; Alemanno, N.; Triolo, G.; Pagano, G. Lipoprotein-apolipoprotein changes in renal transplant recipients: A 2-year follow-up. Metabolism 1991, 40, 922–925. [Google Scholar] [CrossRef]
- Chan, M.K.; Varghese, Z.; Persaud, J.W.; Fernando, O.N.; Moorhead, J.F. The role of multiple pharmaco-therapy in the pathogenesis of hyperlipidemia after renal transplantation. Clin. Nephrol. 1981, 15, 309–313. [Google Scholar]
- Moore, R.A.; Callahan, M.F.; Cody, M.; Adams, P.L.; Litchford, M.; Buckner, K.; Galloway, J. The Eeffect of the American Heart Association Step One Diet on Hyperlipidemia Following Renal Transplantation. Transplantation 1990, 49, 60–62. [Google Scholar] [CrossRef] [PubMed]
- Ettinger, W.H.; Bender, W.L.; Goldberg, A.P.; Hazzard, W.R. Lipoprotein lipid abnormalities in healthy renal trans-plant recipients: Persistence of low HDL2 cholesterol. Nephron 1987, 47, 17–21. [Google Scholar] [CrossRef] [PubMed]
- Barbagallo, C.M.; Averna, M.R.; Sparacino, V.; Cefalù, A.B.; Caputo, F.; Noto, D.; Verghi, F.; Notarbartolo, A. HDL sub-fractions distribution in renal transplant recipients: Lack of evidence of a reduction of HDL2 particles. Nephron 1996, 72, 407–412. [Google Scholar] [CrossRef] [PubMed]
- Barbagallo, C.M.; Cefalù, A.B.; Gallo, S.; Rizzo, M.; Noto, D.; Cavera, G.; Rao Camemi, A.; Marino, G.; Caldarella, R.; Notarbartolo, A.; et al. Effects of Mediterranean diet on lipid levels and cardiovascular risk in renal trans-plant recipients. Nephron 1999, 82, 199–204. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.E.; Yu, M.Y.; Kim, Y.C.; Min, S.I.; Ha, J.; Lee, J.P.; Kim, D.K.; Oh, K.H.; Joo, K.W.; Ahn, C.; et al. Ratio of triglyc-eride to high-density lipoprotein cholesterol and risk of major cardiovascular events in kidney transplant recipients. Clin. Exp. Nephrol. 2019, 23, 1407–1417. [Google Scholar] [CrossRef] [PubMed]
- Fellstrom, B.C.; Jardine, A.G.; Schmieder, R.E.; Holdaas, H.; Bannister, K.; Beutler, J.; Chae, D.-W.; Chevaile, A.; Cobbe, S.M.; Grönhagen-Riska, C.; et al. Rosuvastatin and Cardiovascular Events in Patients Undergoing Hemodialysis. N. Engl. J. Med. 2009, 360, 1395–1407. [Google Scholar] [CrossRef]
- Wanner, C.; Krane, V.; Marz, W.; Olschewski, M.; Mann, J.F.; Ruf, G.; Ritz, E.; German, D.; German Diabetes and Dialysis Study Investigators. Atorvastatin in patients with type 2 diabetes mellitus undergoing hemodialysis. N. Engl. J. Med. 2005, 353, 238–248. [Google Scholar] [CrossRef]
- Baigent, C.; Landray, M.J.; Reith, C.; Emberson, J.; Wheeler, D.C.; Tomson, C.; Wanner, C.; Krane, V.; Cass, A.; Craig, J.; et al. The effects of lowering LDL cholesterol with simvastatin plus ezetimibe in patients with chronic kidney disease (Study of Heart and Renal Protection): A randomised placebo controlledtrial. Lancet 2011, 377, 2181–2192. [Google Scholar] [CrossRef]
- Cholesterol Treatment Trialists’ (CTT) Collaboration; Herrington, W.G.; Emberson, J.; Mihaylova, B.; Blackwell, L.; Reith, C.; Solbu, M.D.; Mark, P.B.; Fellström, B.; Jardine, A.G.; et al. Impact of renal function on the effects of LDL cholesterol lowering with statin-based regimens: A meta-analysis of individual participant data from 28 randomised trials. Lancet Diabetes Endocrinol. 2016, 4, 829–839. [Google Scholar]
- Ferro, C.J.; Mark, P.B.; Kanbay, M.; Sarafidis, P.; Heine, G.H.; Rossignol, P.; Massy, Z.A.; Mallamaci, F.; Valdivielso, J.M.; Malyszko, J.; et al. Lipid management in patients with chronic kidney disease. Nat. Rev. Nephrol. 2018, 14, 727–749. [Google Scholar] [CrossRef]
- Sarnak, M.J.; Bloom, R.; Muntner, P.; Rahman, M.; Saland, J.M.; Wilson, P.W.; Fried, L. KDOQI US Commentary on the 2013 KDIGO Clinical Practice Guideline for Lipid Management in CKD. Am. J. Kidney Dis. 2015, 65, 354–366. [Google Scholar] [CrossRef]
- Bulbul, M.C.; Dagel, T.; Afsar, B.; Ulusu, N.N.; Kuwabara, M.; Covic, A.; Kanbay, M. Disorders of Lipid Metabolism in Chronic Kidney Disease. Blood Purif. 2018, 46, 144–152. [Google Scholar] [CrossRef] [PubMed]
- Schmit, D.; Fliser, D.; Speer, T. Proprotein convertase subtilisin/kexin type 9 in kidney disease. Nephrol. Dial. Transplant. 2019, 34, 1266–1271. [Google Scholar] [CrossRef]
- Charytan, D.M.; Sabatine, M.S.; Pedersen, T.R.; Im, K.; Park, J.-G.; Pineda, A.L.; Wasserman, S.M.; Deedwania, P.; Olsson, A.G.; Sever, P.S.; et al. Efficacy and Safety of Evolocumab in Chronic Kidney Disease in the FOURIER Trial. J. Am. Coll. Cardiol. 2019, 73, 2961–2970. [Google Scholar] [CrossRef] [PubMed]
- Agrawal, S.; Zaritsky, J.J.; Fornoni, A.; Smoyer, W.E. Dyslipidemia in nephrotic syndrome: Mechanisms and treat-ment. Nat. Rev. Nephrol. 2018, 14, 57–70. [Google Scholar] [CrossRef] [PubMed]
- Gyebi, L.; Soltani, Z.; Reisin, E. Lipid nephrotoxicity: New concept fora n old disease. Curr. Hypertens. Rep. 2012, 14, 177–181. [Google Scholar] [CrossRef] [PubMed]
- Vaziri, N.D.; Sato, T.; Liang, K. Molecular mechanisms of altered cholesterol metabolism in rats with spontaneous focal glomerulosclerosis. Kidney Int. 2003, 63, 1756–1763. [Google Scholar] [CrossRef] [PubMed]
- Keane, W.F.; Mulcahy, W.S.; Kasiske, B.L.; Kim, Y.; O’Donnell, M.P. Hyperlipidemia and progressive renal disease. Kidney Int Suppl. 1991, 31, S41–S48. [Google Scholar]
- Kasiske, B.L.; O’Donnell, M.P.; Cleary, M.P.; Keane, W.F. Treatment of hyperlipidemia reduces glomerular injury in obese Zucker rats. Kidney Int. 1988, 33, 667–672. [Google Scholar] [CrossRef]
- Yoshimura, A.; Inui, K.; Nemoto, T.; Uda, S.; Sugenoya, Y.; Watanabe, S.; Yokota, N.; Taira, T.; Iwasaki, S.; Ideura, T. Simvastatin suppresses glomerular cell proliferation and macrophage infiltration in rats with mesangial prolifera-tive nephritis. J. Am. Soc. Nephrol. 1998, 9, 2027–2039. [Google Scholar]
- Mänttäri, M.; Tiula, E.; Alikoski, T.; Manninen, V. Effects of Hypertension and Dyslipidemia on the Decline in Renal Function. Hypertension 1995, 26, 670–675. [Google Scholar] [CrossRef]
- Muntner, P.; Coresh, J.; Smith, J.C.; Eckfeldt, J.; Klag, M.J. Plasma lipids and risk of developing renal dysfunction: The Atherosclerosis Risk in Communities Study. Kidney Int. 2000, 58, 293–301. [Google Scholar] [CrossRef]
- Schaeffner, E.S.; Kurth, T.; Curhan, G.C.; Glynn, R.J.; Rexrode, K.M.; Baigent, C.; Buring, J.E.; Gaziano, J.M. Cholesterol and the risk of renal dysfunction in apparently healthy men. J. Am. Soc. Nephrol. 2003, 14, 2084–2091. [Google Scholar]
- Haynes, R.; Lewis, D.; Emberson, J.; Reith, C.; Agodoa, L.; Cass, A.; Craig, J.C.; De Zeeuw, D.; Feldt-Rasmussen, B.; Fellström, B.; et al. Effects of Lowering LDL Cholesterol on Progression of Kidney Disease. J. Am. Soc. Nephrol. 2014, 25, 1825–1833. [Google Scholar] [CrossRef]
- Rahman, M.; Yang, W.; Akkina, S.; Alper, A.; Anderson, A.H.; Appel, L.J.; He, J.; Raj, D.S.; Schelling, J.; Strauss, L.; et al. Relation of Serum Lipids and Lipoproteins with Progression of CKD: The CRIC Study. Clin. J. Am. Soc. Nephrol. 2014, 9, 1190–1198. [Google Scholar] [CrossRef]
- Sanguankeo, A.; Upala, S.; Cheungpasitporn, W.; Ungprasert, P.; Knight, E.L. Effects of Statins on Renal Outcome in Chronic Kidney Disease Patients: A Systematic Review and Meta-Analysis. PLoS ONE 2015, 10, e0132970. [Google Scholar] [CrossRef]
- Su, X.; Zhang, L.; Lv, J.; Wang, J.; Hou, W.; Xie, X.; Zhang, H. Effect of Statins on Kidney Disease Outcomes: A Systematic Review and Meta-analysis. Am. J. Kidney Dis. 2016, 67, 881–892. [Google Scholar] [CrossRef]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).