
Comparison of the Effect of Resistance and Balance Training on Isokinetic Eversion Strength, Dynamic Balance, Hop Test, and Ankle Score in Ankle Sprain



Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Rehabilitation Program
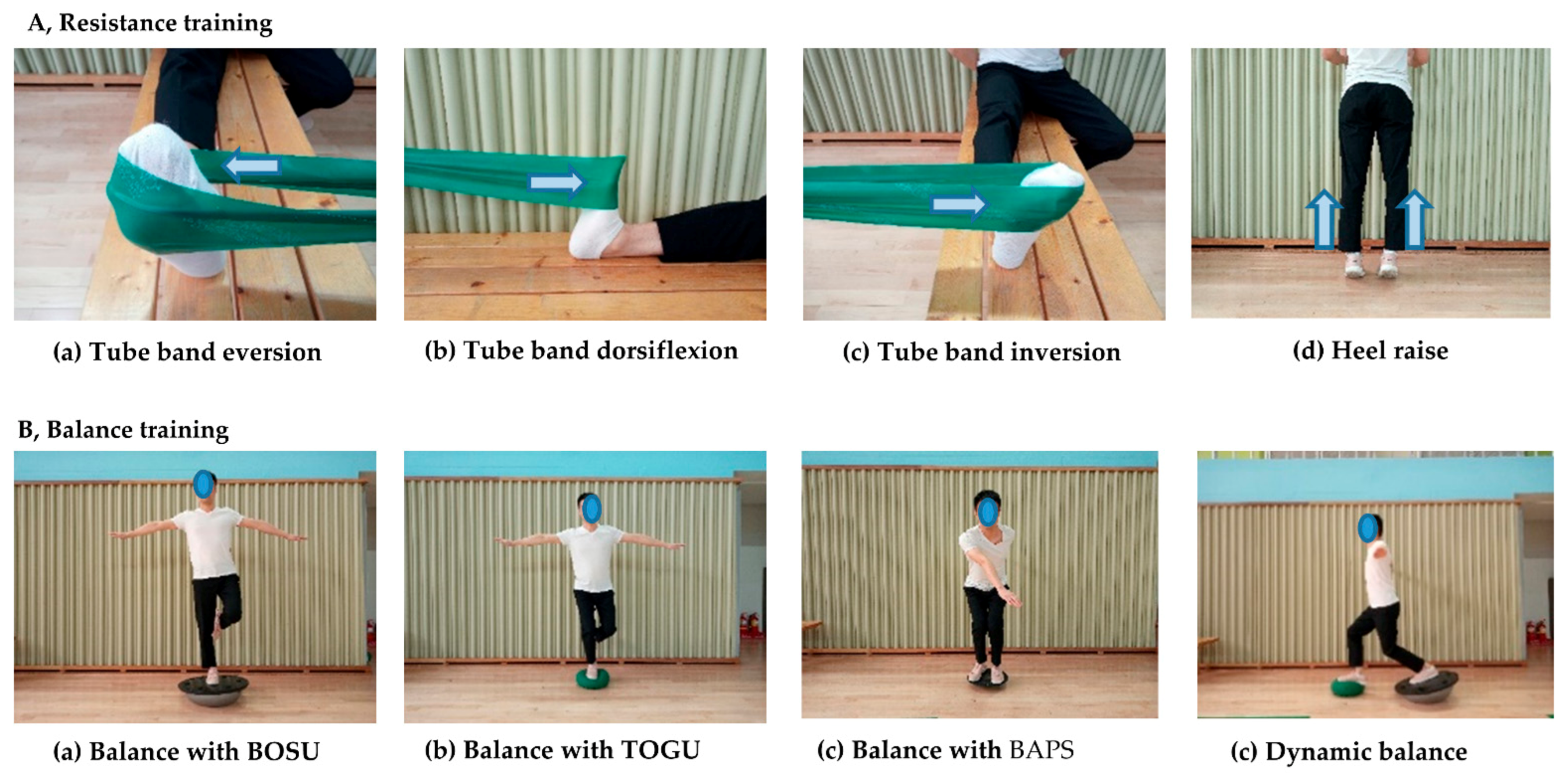
2.2.1. Resistance Training
2.2.2. Balance Training (BT)
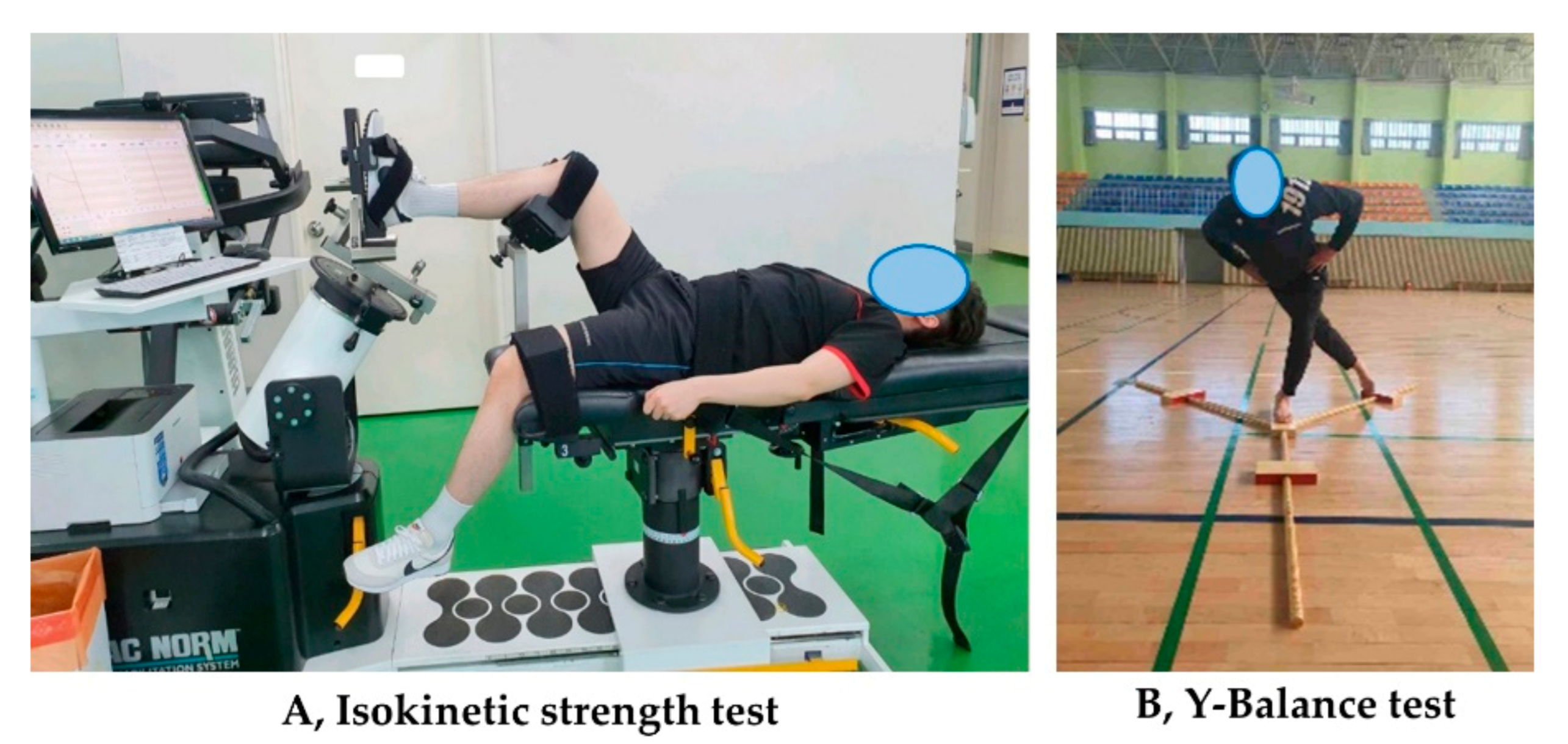
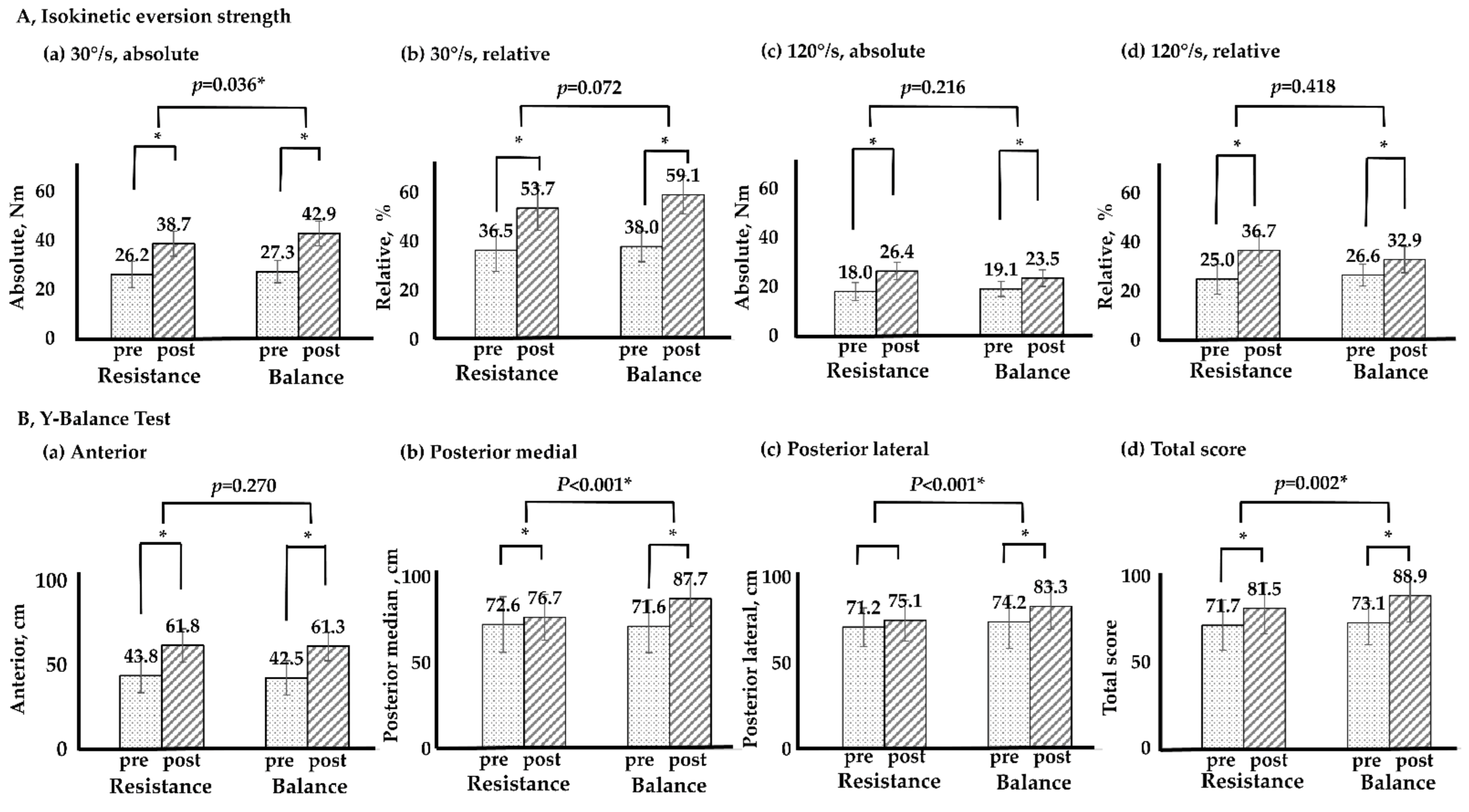
2.3. Isokinetic Eversion Strength Test
2.4. Y-Balance Test
2.5. Hop Tests
2.6. Foot and Ankle Outcome Score (FAOS)
2.7. Data Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Waterman, B.R.; Owens, B.D.; Davey, S.; Zacchilli, M.A.; Belmont, P.J., Jr. The epidemiology of ankle sprains in the United States. J. Bone Jt. Surg. 2010, 92, 2279–2284. [Google Scholar] [CrossRef] [PubMed]
- Herzog, M.M.; Kerr, Z.Y.; Marshall, S.W.; Wikstrom, E.A. Epidemiology of ankle sprains and chronic ankle instability. J. Athl. Train. 2019, 54, 603–610. [Google Scholar] [CrossRef] [PubMed]
- Hertel, J.; Corbett, R.O. An updated model of chronic ankle instability. J. Athl. Train. 2019, 54, 572–588. [Google Scholar] [CrossRef]
- Bonnel, F.; Toullec, E.; Mabit, C.; Tourné, Y. Chronic ankle instability: Biomechanics and pathomechanics of ligaments injury and associated lesions. Orthop. Traumatol. Surg. Res. 2010, 96, 424–432. [Google Scholar] [CrossRef] [PubMed]
- Doherty, C.; Bleakley, C.; Hertel, J.; Caulfield, B.; Ryan, J.; Delahunt, E. Recovery from a first-time lateral ankle sprain and the predictors of chronic ankle instability: A prospective cohort analysis. Am. J. Sports Med. 2016, 44, 995–1003. [Google Scholar] [CrossRef]
- Lee, K.; Kim, Y.H.; Lee, S.; Seo, S.G. Characteristics of the balance ability and isokinetic strength in ankle sprain. Isokinet. Exerc. Sci. 2020, 28, 239–245. [Google Scholar] [CrossRef]
- Hall, E.A.; Chomistek, A.K.; Kingma, J.J.; Docherty, C.L. Balance-and strength-training protocols to improve chronic ankle instability deficits, part I: Assessing clinical outcome measures. J. Athl. Train. 2018, 53, 568–577. [Google Scholar] [CrossRef]
- Hung, Y.-J. Neuromuscular control and rehabilitation of the unstable ankle. World J. Orthop. 2015, 6, 434–438. [Google Scholar] [CrossRef]
- Chinn, L.; Hertel, J. Rehabilitation of ankle and foot injuries in athletes. Clin. Sports Med. 2010, 29, 157–167. [Google Scholar] [CrossRef]
- Smith, B.I.; Docherty, C.L.; Simon, J.; Klossner, J.; Schrader, J. Ankle strength and force sense after a progressive, 6-week strength-training program in people with functional ankle instability. J. Athl. Train. 2012, 47, 282–288. [Google Scholar] [CrossRef]
- Rivera, M.J.; Winkelmann, Z.K.; Powden, C.J.; Games, K.E. Proprioceptive training for the prevention of ankle sprains: An evidence-based review. J. Athl. Train. 2017, 52, 1065–1067. [Google Scholar] [CrossRef] [PubMed]
- Schiftan, G.S.; Ross, L.A.; Hahne, A.J. The effectiveness of proprioceptive training in preventing ankle sprains in sporting populations: A systematic review and meta-analysis. J. Sci. Med. Sport 2015, 18, 238–244. [Google Scholar] [CrossRef] [PubMed]
- Owoeye, O.B.; Palacios-Derflingher, L.M.; Emery, C.A. Prevention of ankle sprain injuries in youth soccer and basketball: Effectiveness of a neuromuscular training program and examining risk factors. Clin. J. Sport Med. 2018, 28, 325–331. [Google Scholar] [CrossRef] [PubMed]
- Ismail, M.M.; Ibrahim, M.M.; Youssef, E.F.; Shorbagy, K.M.E. Plyometric training versus resistive exercises after acute lateral ankle sprain. Foot Ankle Int. 2010, 31, 523–530. [Google Scholar] [CrossRef] [PubMed]
- Hale, S.A.; Hertel, J.; Olmsted-Kramer, L.C. The effect of a 4-week comprehensive rehabilitation program on postural control and lower extremity function in individuals with chronic ankle instability. J. Orthop. Sports Phys. Ther. 2007, 37, 303–311. [Google Scholar] [CrossRef]
- Hubbard-Turner, T. Lack of Medical Treatment From a Medical Professional After an Ankle Sprain. J. Athl. Train. 2019, 54, 671–675. [Google Scholar] [CrossRef] [PubMed]
- Heller, G.Z.; Manuguerra, M.; Chow, R. How to analyze the Visual Analogue Scale: Myths, truths and clinical relevance. Scand. J. Pain 2016, 13, 67–75. [Google Scholar] [CrossRef]
- Dvir, Z. Isokinetics: Muscle Testing, Interpretation, and Clinical Applications, 2nd ed.; Churchill Livingstone: London UK, 2004. [Google Scholar]
- Hübscher, M.; Zech, A.; Pfeifer, K.; Hänsel, F.; Vogt, L.; Banzer, W. Neuromuscular training for sports injury prevention: A systematic review. Med. Sci. Sports Exerc. 2010, 42, 413–421. [Google Scholar] [CrossRef]
- Lin, C.-W.C.; Delahunt, E.; King, E. Neuromuscular training for chronic ankle instability. Phys. Ther. 2012, 92, 987–991. [Google Scholar] [CrossRef]
- CSMi. Humac Norm Users Guide; Computer Sports Medicine, Inc.: Stoughton, MA, USA, 2019. [Google Scholar]
- Shaffer, S.W.; Teyhen, D.S.; Lorenson, C.L.; Warren, R.L.; Koreerat, C.M.; Straseske, C.A.; Childs, J.D. Y-balance test: A reliability study involving multiple raters. Mil. Med. 2013, 178, 1264–1270. [Google Scholar] [CrossRef]
- Ageberg, E.; Zätterström, R.; Moritz, U. Stabilometry and one‐leg hop test have high test‐retest reliability. Scand. J. Med. Sci. Sports 1998, 8, 198–202. [Google Scholar] [CrossRef]
- Roos, E.M.; Brandsson, S.; Karlsson, J. Validation of the foot and ankle outcome score for ankle ligament reconstruction. Foot Ankle Int. 2001, 22, 788–794. [Google Scholar] [CrossRef] [PubMed]
- Tapaninaho, K.; Uimonen, M.M.; Saarinen, A.J.; Repo, J.P. Minimal important change for Foot and Ankle Outcome Score (FAOS). Foot Ankle Surg. 2021. [Google Scholar] [CrossRef] [PubMed]
- Cameron, K.L.; Owens, B.D.; DeBerardino, T.M. Incidence of ankle sprains among active-duty members of the United States Armed Services from 1998 through 2006. J. Athl. Train. 2010, 45, 29–38. [Google Scholar] [CrossRef]
- Son, B.; Cho, Y.J.; Jeong, H.S.; Lee, S.Y. Injuries in Korean elite taekwondo athletes: A prospective study. Int. J. Environ. Res. Public Health 2020, 17, 5143–5152. [Google Scholar] [CrossRef]
- Doherty, C.; Delahunt, E.; Caulfield, B.; Hertel, J.; Ryan, J.; Bleakley, C. The incidence and prevalence of ankle sprain injury: A systematic review and meta-analysis of prospective epidemiological studies. Sports Med. 2014, 44, 123–140. [Google Scholar] [CrossRef]
- Alghadir, A.H.; Iqbal, Z.A.; Iqbal, A.; Ahmed, H.; Ramteke, S.U. Effect of Chronic Ankle Sprain on Pain, Range of Motion, Proprioception, and Balance among Athletes. Int. J. Environ. Res. Public Health 2020, 17, 5318–5327. [Google Scholar] [CrossRef]
- Emery, C.; Meeuwisse, W. The effectiveness of a neuromuscular prevention strategy to reduce injuries in youth soccer: A cluster-randomised controlled trial. Br. J. Sports Med. 2010, 44, 555–562. [Google Scholar] [CrossRef]
- Sefton, J.M.; Yarar, C.; Hicks-Little, C.A.; Berry, J.W.; Cordova, M.L. Six weeks of balance training improves sensorimotor function in individuals with chronic ankle instability. J. Orthop. Sports Phys. Ther. 2011, 41, 81–89. [Google Scholar] [CrossRef]
- Anguish, B.; Sandrey, M.A. Two 4-week balance-training programs for chronic ankle instability. J. Athl. Train. 2018, 53, 662–671. [Google Scholar] [CrossRef]
- O’Driscoll, J.; Kerin, F.; Delahunt, E. Effect of a 6-week dynamic neuromuscular training programme on ankle joint function: A case report. Sports Med. Arthrosc. Rehabil. Ther. Technol. 2011, 3, 13–19. [Google Scholar] [CrossRef]
- Laudner, K.G.; Koschnitzky, M.M. Ankle muscle activation when using the Both Sides Utilized (BOSU) balance trainer. J. Strength Cond. Res. 2010, 24, 218–222. [Google Scholar] [CrossRef] [PubMed]
- Seidler, R.D. Neural correlates of motor learning, transfer of learning, and learning to learn. Exerc. Sport Sci. Rev. 2010, 38, 3. [Google Scholar] [CrossRef]
- Granacher, U.; Muehlbauer, T.; Maestrini, L.; Zahner, L.; Gollhofer, A. Can balance training promote balance and strength in prepubertal children? J. Strength Cond. Res. 2011, 25, 1759–1766. [Google Scholar] [CrossRef]
- Dubin, J.C.; Comeau, D.; McClelland, R.I.; Dubin, R.A.; Ferrel, E. Lateral and syndesmotic ankle sprain injuries: A narrative literature review. J. Chiropr. Med. 2011, 10, 204–219. [Google Scholar] [CrossRef]
- Holviala, J.H.; Sallinen, J.M.; Kraemer, W.J.; Alen, M.J.; Häkkinen, K.K. Effects of strength training on muscle strength characteristics, functional capabilities, and balance in middle-aged and older women. J. Strength Cond. Res. 2006, 20, 336. [Google Scholar]
- Schlicht, J.; Camaione, D.N.; Owen, S.V. Effect of intense strength training on standing balance, walking speed, and sit-to-stand performance in older adults. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2001, 56, M281–M286. [Google Scholar] [CrossRef] [PubMed]
- Hess, J.A.; Woollacott, M. Effect of high-intensity strength-training on functional measures of balance ability in balance-impaired older adults. J. Manip. Phys. Ther. 2005, 28, 582–590. [Google Scholar] [CrossRef]
- Lee, I.-H.; Park, S.-Y. Balance improvement by strength training for the elderly. J. Phys. Ther. Sci. 2013, 25, 1591–1593. [Google Scholar] [CrossRef]
- Kibele, A.; Behm, D.G. Seven weeks of instability and traditional resistance training effects on strength, balance and functional performance. J. Strength Cond. Res. 2009, 23, 2443–2450. [Google Scholar]
- Lee, D.-K.; Kang, M.-H.; Lee, T.-S.; Oh, J.-S. Relationships among the Y balance test, Berg Balance Scale, and lower limb strength in middle-aged and older females. Braz. J. Phys. Ther. 2015, 19, 227–234. [Google Scholar] [CrossRef]
- Hall, E.A.; Docherty, C.L.; Simon, J.; Kingma, J.J.; Klossner, J.C. Strength-training protocols to improve deficits in participants with chronic ankle instability: A randomized controlled trial. J. Athl. Train. 2015, 50, 36–44. [Google Scholar] [CrossRef]
- Coughlan, G.F.; Fullam, K.; Delahunt, E.; Gissane, C.; Caulfield, B.M. A comparison between performance on selected directions of the star excursion balance test and the Y balance test. J. Athl. Train. 2012, 47, 366–371. [Google Scholar] [CrossRef]
- Sipe, C.L.; Ramey, K.D.; Plisky, P.P.; Taylor, J.D. Y-balance test: A valid and reliable assessment in older adults. J. Aging Phys. Act. 2019, 27, 663–669. [Google Scholar] [CrossRef]
- Greenberg, E.T.; Barle, M.; Glassmann, E.; Jung, M.-K. Interrater and test-retest reliability of the Y balance test in healthy, early adolescent female athletes. Int. J. Sports Phys. Ther. 2019, 14, 204–213. [Google Scholar] [CrossRef]
- Docherty, C.L.; Arnold, B.L.; Gansneder, B.M.; Hurwitz, S.; Gieck, J. Functional-performance deficits in volunteers with functional ankle instability. J. Athl. Train. 2005, 40, 30–34. [Google Scholar]
- Eechaute, C.; Vaes, P.; Duquet, W. The dynamic postural control is impaired in patients with chronic ankle instability: Reliability and validity of the multiple hop test. Clin. J. Sport Med. 2009, 19, 107–114. [Google Scholar] [CrossRef] [PubMed]
- Caffrey, E.; Docherty, C.L.; Schrader, J.; Klossner, J. The ability of 4 single-limb hopping tests to detect functional performance deficits in individuals with functional ankle instability. J. Orthop. Sports Phys. Ther. 2009, 39, 799–806. [Google Scholar] [CrossRef]
- Cain, M.S.; Ban, R.J.; Chen, Y.-P.; Geil, M.D.; Goerger, B.M.; Linens, S.W. Four-Week Ankle-Rehabilitation Programs in Adolescent Athletes With Chronic Ankle Instability. J. Athl. Train. 2020, 55, 801–810. [Google Scholar] [CrossRef]
- De Ridder, R.; Willems, T.; Vanrenterghem, J.; Roosen, P. Effect of a home-based balance training protocol on dynamic postural control in subjects with chronic ankle instability. Int. J. Sports Med. 2015, 36, 596–602. [Google Scholar] [CrossRef]
- Hall, E.A.; Chomistek, A.K.; Kingma, J.J.; Docherty, C.L. Balance-and Strength-training protocols to improve chronic ankle instability deficits, part II: Assessing patient-reported outcome measures. J. Athl. Train. 2018, 53, 578–583. [Google Scholar] [CrossRef] [PubMed]
- Ortega-Avila, A.B.; Cervera-Garvi, P.; Marchena-Rodriguez, A.; Chicharro-Luna, E.; Nester, C.J.; Starbuck, C.; Gijon-Nogueron, G. Conservative treatment for acute ankle sprain: A systematic review. J. Clin. Med. 2020, 9, 3128–3145. [Google Scholar] [CrossRef] [PubMed]
- Bellows, R.; Wong, C.K. The effect of bracing and balance training on ankle sprain incidence among athletes: A systematic review with meta-analysis. Int. J. Sports Phys. Ther. 2018, 13, 379–388. [Google Scholar] [CrossRef] [PubMed]
- Janssen, K.W.; van Mechelen, W.; Verhagen, E.A. Bracing superior to neuromuscular training for the prevention of self-reported recurrent ankle sprains: A three-arm randomised controlled trial. Br. J. Sports Med. 2014, 48, 1235–1239. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| RT | BT | |
|---|---|---|
| 1 week | Band color: yellow | Balance instrument: floor |
| Inversion and eversion, 20 rep × 3 sets | One leg stand, 20 s × 3 sets | |
| 2 weeks | Band color: red | Balance instrument: BOSU, hard side |
| Inversion and eversion, 20 rep × 4 sets | Both leg stand, 20 s × 3 sets | |
| Plantar and dorsi flexion, 20 rep × 4 sets | Up and down with one leg, 10 rep × 3 sets | |
| 3 weeks | Band color: green | Balance instrument: BOSU, soft side |
| Inversion and eversion, 20 rep × 5 sets | Both leg stand, 20 s × 3 sets | |
| Plantar and dorsi flexion, 20 rep × 5 sets | Up and down with one leg, 20 rep × 3 sets | |
| Heel raise, 20 rep × 3 sets | Twist with both leg stand, 10 rep × 3 sets | |
| 4 weeks | Band color: blue | Balance instrument: BAPS |
| Inversion and eversion, 30 rep × 4 sets | Both leg stand, 30 s × 3 sets | |
| Plantar and dorsi flexion, 30 rep × 4 sets | Up and down with one leg, 20 rep × 3 sets | |
| Heel raise/forefoot raise, 20 rep × 4 sets | Both leg stand (twist), 20 rep × 3 sets | |
| 5 weeks | Band color: black | Balance instrument: TOGU |
| Inversion and eversion, 30 rep × 5 sets | Both leg stand, 30 s × 3 sets | |
| Plantar and dorsi flexion, 30 rep × 5 sets | Up and down with one leg, 20 rep × 3 sets | |
| Heel raise/forefoot raise, 20 rep × 5 sets | Twist with both leg stand, 20 rep × 3 sets | |
| Squat, 10 rep × 3 sets | Balance instrument: TOGU | |
| 6 weeks | Band color: gray | Balance instrument: TOGU |
| Inversion and eversion, 30 rep × 5 sets | Both leg stand, 30 s × 3 sets | |
| Plantar and dorsi flexion, 30 rep × 5 sets | Up and down with one leg, 20 rep × 5 sets | |
| Heel raise/forefoot raise, 30 rep × 5 sets | Twist with both leg stand, 20 rep × 5 sets | |
| Squat, 20 rep × 3 sets | Balance instrument: TOGU |
| Variables | Resistance Training (n = 27) | Balance Training (n = 27) | p |
|---|---|---|---|
| Age, years | 28.5 ± 5.5 | 28.0 ± 5.7 | 0.739 |
| Height, cm | 174.9 ± 6.6 | 174.4 ± 6.3 | 0.787 |
| Weight, kg | 72.6 ± 5.7 | 72.0 ± 5.3 | 0.677 |
| BMI, kg/m2 | 23.8 ± 2.9 | 23.7 ± 2.0 | 0.820 |
| Preference side, left/right | 2/25 | 4/23 | 0.541 |
| Injury side, left/right | 10/17 | 12/15 | 0.419 |
| Injury cause, contact/non-contact | 8/19 | 10/17 | 0.845 |
| Variables | Group | Pre | Post | p | T × G, p |
|---|---|---|---|---|---|
| Single, cm | Resistance training | 136.4 ± 20.5 | 163.4 ± 22.3 | 0.004 * | 0.549 |
| Balance training | 137.4 ± 27.0 | 164.6 ± 25.5 | 0.004 * | ||
| p | 0.725 | 0.314 | |||
| Triple, cm | Resistance training | 450.3 ± 51.5 | 483.7 ± 49.6 | <0.001 * | 0.225 |
| Balance training | 444.4 ± 63.1 | 475.6 ± 64.4 | 0.006 * | ||
| p | 0.604 | 0.224 | |||
| Crossover, cm | Resistance training | 401.9 ± 25.7 | 412.6 ± 30.6 | 0.070 | 0.008 * |
| Balance training | 405.5 ± 66.4 | 455.4 ± 63.1 | 0.002 * | ||
| p | 0.851 | 0.025 * | |||
| 6 m, s | Resistance training | 2.28 ± 0.19 | 2.11 ± 0.15 | 0.022 * | 0.233 |
| Balance training | 2.29 ± 0.15 | 2.08 ± 0.09 | <0.001 * | ||
| p | 0.784 | 0.150 |
| Variables | Group | Pre | Post | p | T × G, p |
|---|---|---|---|---|---|
| Total score | Resistance training | 70.3 ± 16.4 | 91.2 ± 6.6 | <0.001 * | 0.155 |
| Balance training | 65.0 ± 16.3 | 93.5 ± 5.6 | <0.001 * | ||
| p | 0.257 | 0.101 | |||
| Pain | Resistance training | 69.0 ± 16.3 | 90.0 ± 7.1 | <0.001 * | 0.022 * |
| Balance training | 65.0 ± 21.4 | 94.5 ± 5.6 | <0.001 * | ||
| p | 0.584 | 0.034 * | |||
| Symptoms | Resistance training | 73.0 ± 16.6 | 93.7 ± 5.1 | <0.001 * | 0.316 |
| Balance training | 72.8 ± 20.9 | 96.0 ± 3.7 | <0.001 * | ||
| p | 0.641 | 0.551 | |||
| ADL | Resistance training | 78.9 ± 19.2 | 88.1 ± 6.8 | <0.001 * | 0.250 |
| Balance training | 75.9 ± 14.0 | 90.4 ± 7.8 | <0.001 * | ||
| p | 0.414 | 0.106 | |||
| Sports | Resistance training | 75.9 ± 14.0 | 87.4 ± 7.8 | <0.001 * | 0.027 * |
| Balance training | 74.3 ± 17.3 | 93.0 ± 5.4 | <0.001 * | ||
| p | 0.479 | 0.012 * | |||
| QoL | Resistance training | 58.9 ± 16.0 | 89.2 ± 4.7 | <0.001 * | 0.033 * |
| Balance training | 57.0 ± 15.2 | 95.0 ± 4.9 | <0.001 * | ||
| p | 0.159 | 0.011 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, H.; Yu, H.; Kim, Y.H.; Kan, W. Comparison of the Effect of Resistance and Balance Training on Isokinetic Eversion Strength, Dynamic Balance, Hop Test, and Ankle Score in Ankle Sprain. Life 2021, 11, 307. https://doi.org/10.3390/life11040307
Wang H, Yu H, Kim YH, Kan W. Comparison of the Effect of Resistance and Balance Training on Isokinetic Eversion Strength, Dynamic Balance, Hop Test, and Ankle Score in Ankle Sprain. Life. 2021; 11(4):307. https://doi.org/10.3390/life11040307
Chicago/Turabian StyleWang, Haifang, Hailong Yu, Yong Hwan Kim, and Wencong Kan. 2021. "Comparison of the Effect of Resistance and Balance Training on Isokinetic Eversion Strength, Dynamic Balance, Hop Test, and Ankle Score in Ankle Sprain" Life 11, no. 4: 307. https://doi.org/10.3390/life11040307
APA StyleWang, H., Yu, H., Kim, Y. H., & Kan, W. (2021). Comparison of the Effect of Resistance and Balance Training on Isokinetic Eversion Strength, Dynamic Balance, Hop Test, and Ankle Score in Ankle Sprain. Life, 11(4), 307. https://doi.org/10.3390/life11040307