
Association between Vascular Inflammation and Inflammation in Adipose Tissue, Spleen, and Bone Marrow in Patients with Psoriasis

 , and
, and
Abstract
1. Introduction
2. Materials and Methods
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Takeshita, J.; Grewal, S.; Langan, S.M.; Mehta, N.N.; Ogdie, A.; Van Voorhees, A.S.; Gelfand, J.M. Psoriasis and comorbid diseases: Epidemiology. J. Am. Acad. Dermatol. 2017, 76, 377–390. [Google Scholar] [CrossRef]
- Reich, K. The concept of psoriasis as a systemic inflammation: Implications for disease management. J. Eur. Acad. Dermatol. Venereol. 2012, 26, 3–11. [Google Scholar] [CrossRef]
- Armstrong, E.J.; Harskamp, C.T.; Armstrong, A.W. Psoriasis and major adverse cardiovascular events: A systematic review and meta-analysis of observational studies. J. Am. Heart Assoc. 2013, 2, e000062. [Google Scholar] [CrossRef]
- Mehta, N.N.; Yu, Y.D.; Saboury, B.; Foroughi, N.; Krishnamoorthy, P.; Raper, A.; Baer, A.; Antigua, J.; Van Voorhees, A.S.; Torigian, D.A.; et al. Systemic and vascular inflammation in patients with moderate to severe psoriasis as measured by [18F]-fluorodeoxyglucose positron emission tomography-computed tomography (FDG-PET/CT): A pilot study. Arch. Dermatol. 2011, 147, 1031–1039. [Google Scholar] [CrossRef]
- Hjuler, K.F.; Gormsen, L.C.; Vendelbo, M.H.; Egeberg, A.; Nielsen, J.; Iversen, L. Increased global arterial and subcutaneous adipose tissue inflammation in patients with moderate-to-severe psoriasis. Br. J. Dermatol. 2017, 176, 732–740. [Google Scholar] [CrossRef] [PubMed]
- Hjuler, K.; Gormsen, L.; Vendelbo, M.; Egeberg, A.; Nielsen, J.; Iversen, L. Systemic inflammation and evidence of a cardio-splenic axis in patients with psoriasis. Acta Derm. Venereol. 2018, 98, 390–395. [Google Scholar] [CrossRef] [PubMed]
- Goyal, A.; Dey, A.K.; Chaturvedi, A.; Elnabawi, Y.A.; Aberra, T.M.; Chung, J.H.; Belur, A.D.; Groenendyk, J.W.; Lerman, J.B.; Rivers, J.P.; et al. Chronic stress-related neural activity associates with subclinical cardiovascular disease in psoriasis: A prospective cohort study. JACC Cardiovasc. Imaging 2020, 13, 465–477. [Google Scholar] [CrossRef] [PubMed]
- Joshi, A.A.; Lerman, J.B.; Dey, A.K.; Sajja, A.P.; Belur, A.D.; Elnabawi, Y.A.; Rodante, J.A.; Aberra, T.M.; Chung, J.; Salahuddin, T.; et al. Association between aortic vascular inflammation and coronary artery plaque characteristics in psoriasis. JAMA Cardiol. 2018, 3, 949–956. [Google Scholar] [CrossRef]
- Talman, A.H.; Psaltis, P.J.; Cameron, J.D.; Meredith, I.T.; Seneviratne, S.K.; Wong, D.T.L. Epicardial adipose tissue: Far more than a fat depot. Cardiovasc. Diagn. Ther. 2014, 4, 416–429. [Google Scholar] [CrossRef]
- Fitzgibbons, T.P.; Czech, M.P. Epicardial and perivascular adipose tissues and their influence on cardiovascular disease: Basic mechanisms and clinical associations. J. Am. Heart Assoc. 2014, 3, e000582. [Google Scholar] [CrossRef]
- Iacobellis, G.; Ribaudo, M.C.; Assael, F.; Vecci, E.; Tiberti, C.; Zappaterreno, A.; Di Mario, U.; Leonetti, F. Echocardiographic epicardial adipose tissue is related to anthropometric and clinical parameters of metabolic syndrome: A new indicator of cardiovascular risk. J. Clin. Endocrinol. Metab. 2003, 88, 5163–5168. [Google Scholar] [CrossRef] [PubMed]
- Bulbul Sen, B.; Atci, N.; Rifaioglu, E.N.; Ekiz, O.; Kartal, I.; Buyukkaya, E.; Kurt, M.; Karakas, M.F.; Buyukkaya, S.; Akcay, A.B.; et al. Increased epicardial fat tissue is a marker of subclinical atherosclerosis in patients with psoriasis. Br. J. Dermatol. 2013, 169, 1081–1086. [Google Scholar] [CrossRef] [PubMed]
- Torres, T.; Bettencourt, N.; Mendonça, D.; Vasconcelos, C.; Gama, V.; Silva, B.M.; Selores, M. Epicardial adipose tissue and coronary artery calcification in psoriasis patients. JEADV 2015, 29, 270–277. [Google Scholar] [CrossRef]
- Wang, X.; Guo, Z.; Zhu, Z.; Bao, Y.; Yang, B. Epicardial fat tissue in patients with psoriasis:a systematic review and meta-analysis. Lipids Health Dis. 2016, 15, 103. [Google Scholar] [CrossRef]
- Bucerius, J.; Hyafil, F.; Verberne, H.J.; Slart, R.H.J.A.; Lindner, O.; Sciagra, R.; Agostini, D.; Übleis, C.; Gimelli, A.; Hacker, M. Position paper of the cardiovascular committee of the european association of nuclear medicine (EANM) on PET imaging of atherosclerosis. Eur. J. Nucl. Med. Mol. Imaging 2016, 43, 780–792. [Google Scholar] [CrossRef] [PubMed]
- Ahn, S.S.; Hwang, S.H.; Jung, S.M.; Lee, S.-W.; Park, Y.-B.; Yun, M.; Song, J.J. Evaluation of spleen glucose metabolism using 18F-FDG PET/CT in patients with febrile autoimmune disease. J. Nucl. Med. 2017, 58, 507–513. [Google Scholar] [CrossRef] [PubMed]
- Touboul, P.J.; Hennerici, M.G.; Meairs, S.; Adams, H.; Amarenco, P.; Bornstein, N.; Csiba, L.; Desvarieux, M.; Ebrahim, S.; Hernandez Hernandez, R.; et al. Mannheim carotid intima-media thickness and plaque consensus (2004–2006–2011). Cerebrovasc. Dis. 2012, 34, 290–296. [Google Scholar] [CrossRef]
- Emami, H.; Singh, P.; Macnabb, M.; Vucic, E.; Lavender, Z.; Rudd, J.H.F.; Fayad, Z.A.; Lehrer-Graiwer, J.; Korsgren, M.; Figueroa, A.L.; et al. Splenic metabolic activity predicts risk of future cardiovascular events: Demonstration of a cardiosplenic axis in humans. JACC Cardiovasc. Imaging 2015, 8, 121–130. [Google Scholar] [CrossRef] [PubMed]
- Poller, W.C.; Nahrendorf, M.; Swirski, F.K. Hematopoiesis and cardiovascular disease. Circ. Res. 2020, 126, 1061–1085. [Google Scholar] [CrossRef]
- Bucerius, J.; Mani, V.; Wong, S.; Moncrieff, C.; Izquierdo-Garcia, D.; Machac, J.; Fuster, V.; Farkouh, M.E.; Rudd, J.H.F.; Fayad, Z.A. Arterial and fat tissue inflammation are highly correlated: A prospective 18F-FDG PET/CT study. Eur. J. Nucl. Med. Mol. Imaging 2014, 41, 934–945. [Google Scholar] [CrossRef] [PubMed]
- Figueroa, A.L.; Abdelbaky, A.; Truong, Q.A.; Corsini, E.; MacNabb, M.H.; Lavender, Z.R.; Lawler, M.A.; Grinspoon, S.K.; Brady, T.J.; Nasir, K.; et al. Measurement of arterial activity on routine FDG PET/CT images improves prediction of risk of future CV events. JACC Cardiovasc. Imaging 2013, 6, 1250–1259. [Google Scholar] [CrossRef] [PubMed]
- Zhou, W.; Dey, A.; Manyak, G.; Teklu, M.; Patel, N.; Teague, H.; Mehta, N.N. The application of molecular imaging to advance translational research in chronic inflammation. J. Nucl. Cardiol. 2020, 1–13, [Epub 346 ahead of print]. [Google Scholar] [CrossRef]
- Christen, T.; Sheikine, Y.; Rocha, V.Z.; Hurwitz, S.; Goldfine, A.B.; Di Carli, M.; Libby, P. Increased glucose uptake in visceral versus subcutaneous adipose tissue revealed by PET imaging. JACC Cardiovasc. Imaging 2010, 3, 843–851. [Google Scholar] [CrossRef] [PubMed]
- Antonopoulos, A.S.; Sanna, F.; Sabharwal, N.; Thomas, S.; Oikonomou, E.K.; Herdman, L.; Margaritis, M.; Shirodaria, C.; Kampoli, A.M.; Akoumianakis, I.; et al. Detecting human coronary inflammation by imaging perivascular fat. Sci. Transl. Med. 2017, 9, eaal2658. [Google Scholar] [CrossRef]
- Oikonomou, E.K.; Marwan, M.; Desai, M.Y.; Mancio, J.; Alashi, A.; Hutt Centeno, E.; Thomas, S.; Herdman, L.; Kotanidis, C.P.; Thomas, K.E.; et al. Non-invasive detection of coronary inflammation using computed tomography and prediction of residual cardiovascular risk (the CRISP CT study): A post-hoc analysis of prospective outcome data. Lancet 2018, 392, 929–939. [Google Scholar] [CrossRef]
- Elnabawi, Y.A.; Oikonomou, E.K.; Dey, A.K.; Mancio, J.; Rodante, J.A.; Aksentijevich, M.; Choi, H.; Keel, A.; Erb-Alvarez, J.; Teague, H.L.; et al. Association of biologic therapy with coronary inflammation in patients with psoriasis as assessed by perivascular fat attenuation index. JAMA Cardiol. 2019, 4, 885–891. [Google Scholar] [CrossRef]
- Kaiser, H.; Abdulla, J.; Henningsen, K.M.A.; Skov, L.; Hansen, P.R. Coronary artery disease assessed by computed tomography in patients with psoriasis: A systematic review and meta-analysis. Dermatology 2019, 235, 478–487. [Google Scholar] [CrossRef]
- Mazurek, T.; Kiliszek, M.; Kobylecka, M.; Skubisz-Głuchowska, J.; Kochman, J.; Filipiak, K.; Królicki, L.; Opolski, G. Relation of proinflammatory activity of epicardial adipose tissue to the occurrence of atrial fibrillation. Am. J. Cardiol. 2014, 113, 1505–1508. [Google Scholar] [CrossRef]
- Ahlehoff, O.; Gislason, G.H.; Jorgensen, C.H.; Lindhardsen, J.; Charlot, M.; Olesen, J.B.; Abildstrom, S.Z.; Skov, L.; Torp-Pedersen, C.; Hansen, P.R. Psoriasis and risk of atrial fibrillation and ischaemic stroke: A Danish Nationwide Cohort Study. Eur. Heart J. 2012, 33, 2054–2064. [Google Scholar] [CrossRef]
- Tahara, N.; Kai, H.; Nakaura, H.; Mizoguchi, M.; Ishibashi, M.; Kaida, H.; Baba, K.; Hayabuchi, N.; Imaizumi, T. The prevalence of inflammation in carotid atherosclerosis: Analysis with fluorodeoxyglucose-positron emission tomography. Eur. Heart J. 2007, 28, 2243–2248. [Google Scholar] [CrossRef]
- Peters, S.A.E.; Den Ruijter, H.M.; Bots, M.L.; Moons, K.G.M. Improvements in risk stratification for the occurrence of cardiovascular disease by imaging subclinical atherosclerosis: A systematic review. Heart 2012, 98, 177–184. [Google Scholar] [CrossRef]
- Zhang, Y.; Guallar, E.; Qiao, Y.; Wasserman, B.A. Is carotid intima-media thickness as predictive as other noninvasive techniques for the detection of coronary artery disease? Arter. Thromb. Vasc. Biol. 2014, 34, 1341–1345. [Google Scholar] [CrossRef] [PubMed]
- Tawakol, A.; Fayad, Z.A.; Mogg, R.; Alon, A.; Klimas, M.T.; Dansky, H.; Subramanian, S.S.; Abdelbaky, A.; Rudd, J.H.F.; Farkouh, M.E.; et al. Intensification of statin therapy results in a rapid reduction in atherosclerotic inflammation: Results of a multicenter fluorodeoxyglucose- positron emission tomography/computed tomography feasibility study. J. Am. Coll. Cardiol. 2013, 62, 909–917. [Google Scholar] [CrossRef]
- Huang, Y.; Li, W.; Dong, L.; Li, R.; Wu, Y. Effect of statin therapy on the progression of common carotid artery intima-media thickness: An updated systematic review and meta-analysis of randomized controlled trials. J. Atheroscler. Thromb. 2013, 20, 108–121. [Google Scholar] [CrossRef]
- Kaiser, H.; Kvist-Hansen, A.; Krakauer, M.; Gørtz, P.; Henningsen, K.; Wang, X.; Becker, C.; Skov, L.; Hansen, P. Statin therapy and vascular inflammation detected by positron emission tomography computed tomography in patients with psoriasis. Acta Derm. Venereol. 2021, 101, adv00406. [Google Scholar] [CrossRef] [PubMed]
- Naik, H.B.; Natarajan, B.; Stansky, E.; Ahlman, M.A.; Teague, H.; Salahuddin, T.; Ng, Q.; Joshi, A.A.; Krishnamoorthy, P.; Dave, J.; et al. Severity of psoriasis associates with aortic vascular inflammation detected by FDG PET/CT and neutrophil activation in a prospective observational study. Arter. Thromb. Vasc. Biol. 2015, 35, 2667–2676. [Google Scholar] [CrossRef] [PubMed]
- Dey, A.K.; Joshi, A.A.; Chaturvedi, A.; Lerman, J.B.; Aberra, T.M.; Rodante, J.A.; Teague, H.L.; Harrington, C.L.; Rivers, J.P.; Chung, J.H.; et al. Association between skin and aortic vascular inflammation in patients with psoriasis: A case-cohort study using positron emission tomography/computed tomography. JAMA Cardiol. 2017, 2, 1013–1018. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| All Patients (n = 83) | |
|---|---|
| Sex, Male, n (%) Age (years) | 60 (72.3) 59.6 ± 10.9 |
| BMI (kg/m2) | 30.0 ± 5.6 |
| Waist-to-hip ratio | 0.99 ± 0.07 |
| PASI | 3.5 (1.1–10.8) |
| PsA, n (%) | 20 (24.1) |
| Medically treated hypertension, n (%) | 36 (43.4) |
| Medically treated diabetes, n (%) | 20 (24.1) |
| Systemic antipsoriatic treatment, n (%) | 44 (53.0) |
| Statin treatment, n (%) | 41 (49.4) |
| Prior CVD, n (%) | 39 (47.0) |
| Smoking, present or previous, n (%) | 61 (73.5) |
| HbA1c (mmol/mol) | 36.0 (34.0–41.0) |
| Total cholesterol (mmol/L) | 4.43 ± 0.98 |
| LDL-C (mmol/L) | 2.39 ± 0.84 |
| HDL-C (mmol/L) | 1.24 ± 0.38 |
| Triglycerides (mmol/L) | 1.87 ± 0.97 |
| Blood glucose (mmol/L) | 5.9 (5.4–6.7) |
| hs-CRP (mg/L) | 1.41 (0.68–3.83) |
| Entire aorta (TBRmax) | 2.27 ± 0.39 |
| Visceral adipose tissue (TBRmean) | 0.17 (0.15–0.21) |
| Subcutaneous adipose tissue (TBRmean) | 0.13 (0.11–0.16) |
| Pericardial adipose tissue (TBRmean) | 0.34 (0.26–0.52) |
| Spleen (SLRmean) | 0.94 ± 0.10 |
| Bone marrow (BLRmean) | 1.00 ± 0.20 |
| Carotid intima-media thickness (mm) | 0.73 ± 0.13 |
| Carotid atherosclerotic plaques, n (%) | 50 (60.2) |
| All Patients (n = 83) | No CVD (n = 44) | |
|---|---|---|
| β (p-Value) | β (p-Value) | |
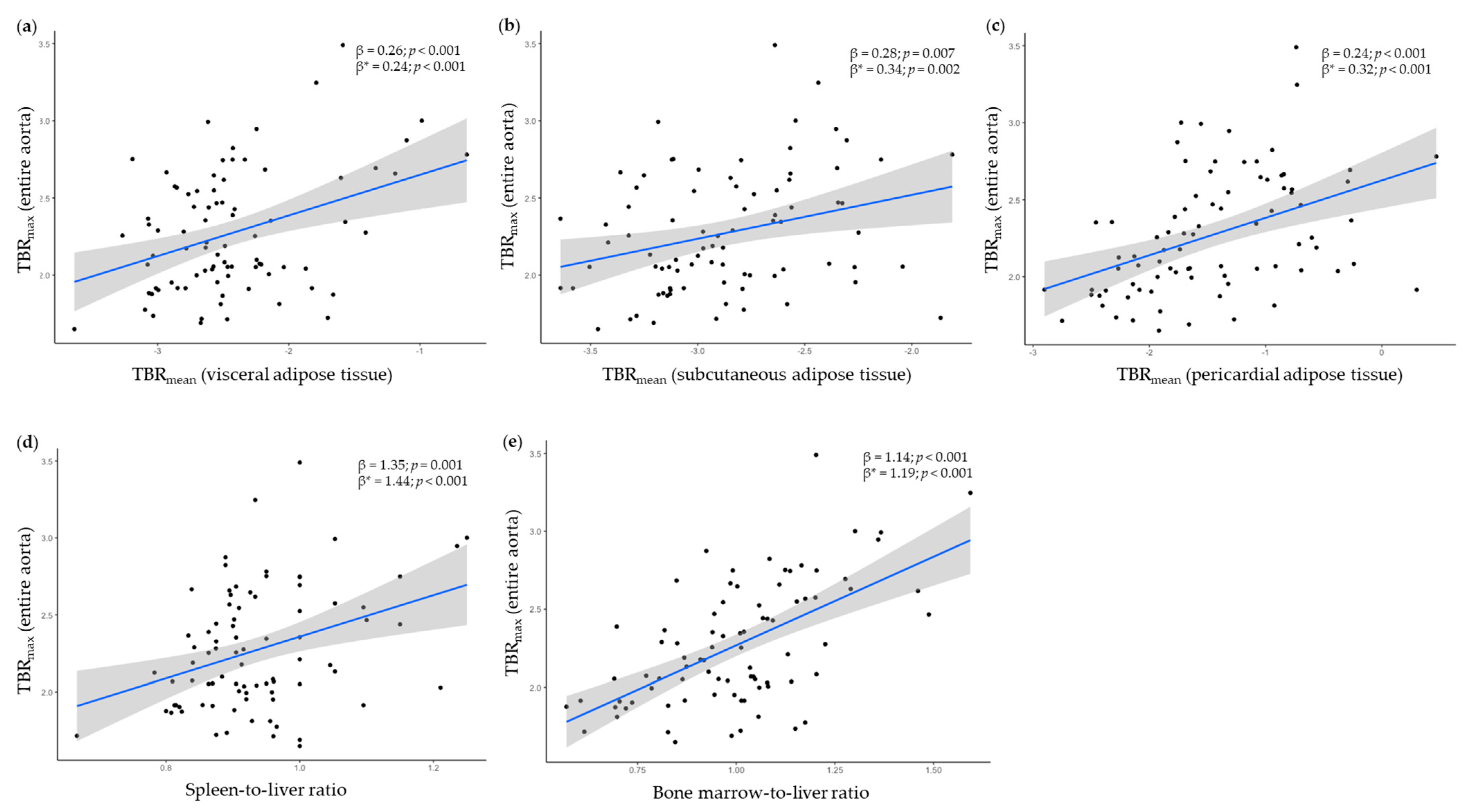
| Visceral adipose tissue 1 Unadjusted Adjusted | 0.26 (<0.001) 0.24 (0.001) | 0.29 (0.002) 0.27 (0.011) |
| Subcutaneous adipose tissue 1 Unadjusted Adjusted | 0.28 (0.007) 0.34 (0.002) | 0.39 (0.010) 0.42 (0.011) |
| Pericardial adipose tissue 1 Unadjusted Adjusted | 0.24 (<0.001) 0.32 (<0.001) | 0.32 (<0.001) 0.40 (<0.001) |
| Spleen-to-liver ratio Unadjusted Adjusted | 1.35 (0.001) 1.44 (< 0.001) | 0.49 (0.491) 0.86 (0.262) |
| Bone marrow-to-liver ratio Unadjusted Adjusted | 1.14 (<0.001) 1.19 (<0.001) | 1.24 (<0.001) 1.36 (<0.001) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kaiser, H.; Kvist-Hansen, A.; Krakauer, M.; Gørtz, P.M.; Henningsen, K.M.A.; Wang, X.; Becker, C.; Zachariae, C.; Skov, L.; Hansen, P.R. Association between Vascular Inflammation and Inflammation in Adipose Tissue, Spleen, and Bone Marrow in Patients with Psoriasis. Life 2021, 11, 305. https://doi.org/10.3390/life11040305
Kaiser H, Kvist-Hansen A, Krakauer M, Gørtz PM, Henningsen KMA, Wang X, Becker C, Zachariae C, Skov L, Hansen PR. Association between Vascular Inflammation and Inflammation in Adipose Tissue, Spleen, and Bone Marrow in Patients with Psoriasis. Life. 2021; 11(4):305. https://doi.org/10.3390/life11040305
Chicago/Turabian StyleKaiser, Hannah, Amanda Kvist-Hansen, Martin Krakauer, Peter Michael Gørtz, Kristoffer Mads Aaris Henningsen, Xing Wang, Christine Becker, Claus Zachariae, Lone Skov, and Peter Riis Hansen. 2021. "Association between Vascular Inflammation and Inflammation in Adipose Tissue, Spleen, and Bone Marrow in Patients with Psoriasis" Life 11, no. 4: 305. https://doi.org/10.3390/life11040305
APA StyleKaiser, H., Kvist-Hansen, A., Krakauer, M., Gørtz, P. M., Henningsen, K. M. A., Wang, X., Becker, C., Zachariae, C., Skov, L., & Hansen, P. R. (2021). Association between Vascular Inflammation and Inflammation in Adipose Tissue, Spleen, and Bone Marrow in Patients with Psoriasis. Life, 11(4), 305. https://doi.org/10.3390/life11040305