
Fascia Lata Alterations in Hip Osteoarthritis: An Observational Cross-Sectional Study


 , ,
, ,  ,
,  ,
,  ,
,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Immunohistochemistry
2.2. Image Analysis
2.3. Statistical Analysis
3. Results
3.1. Sample Characteristics
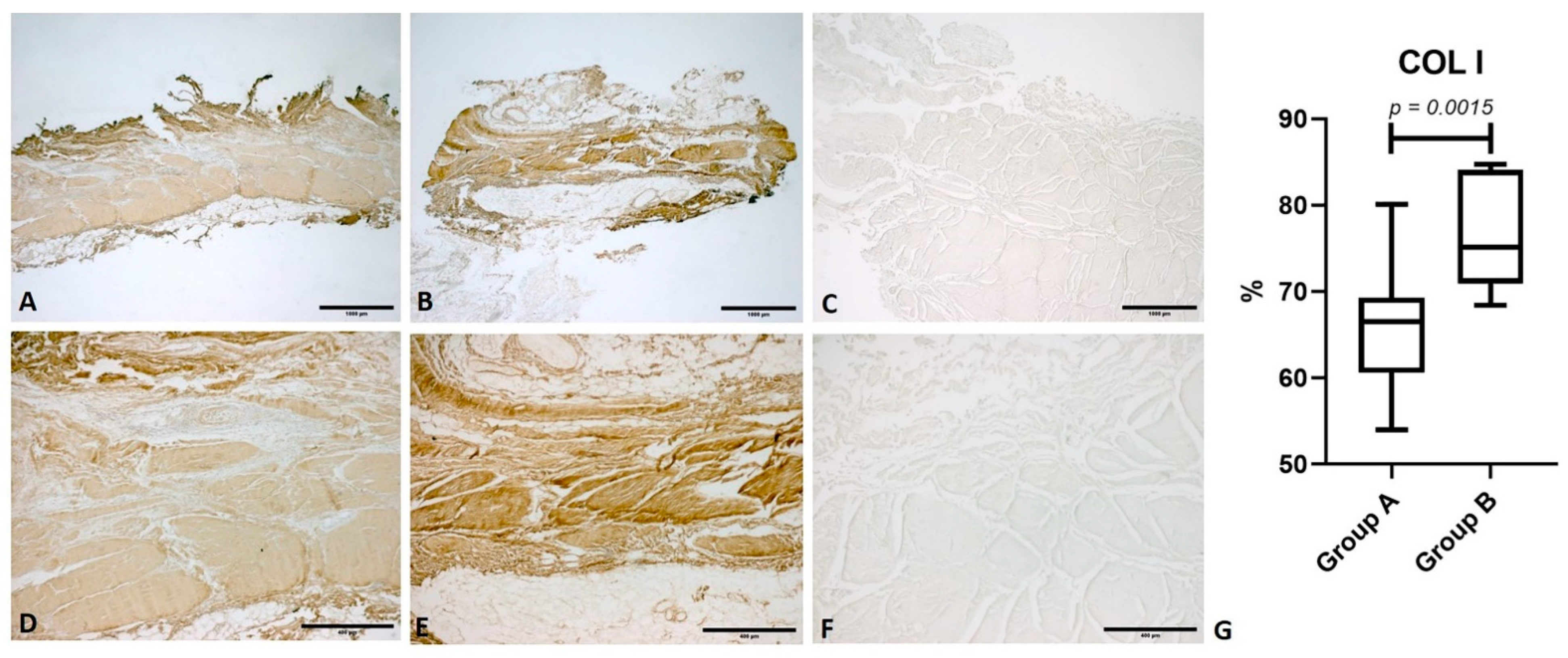
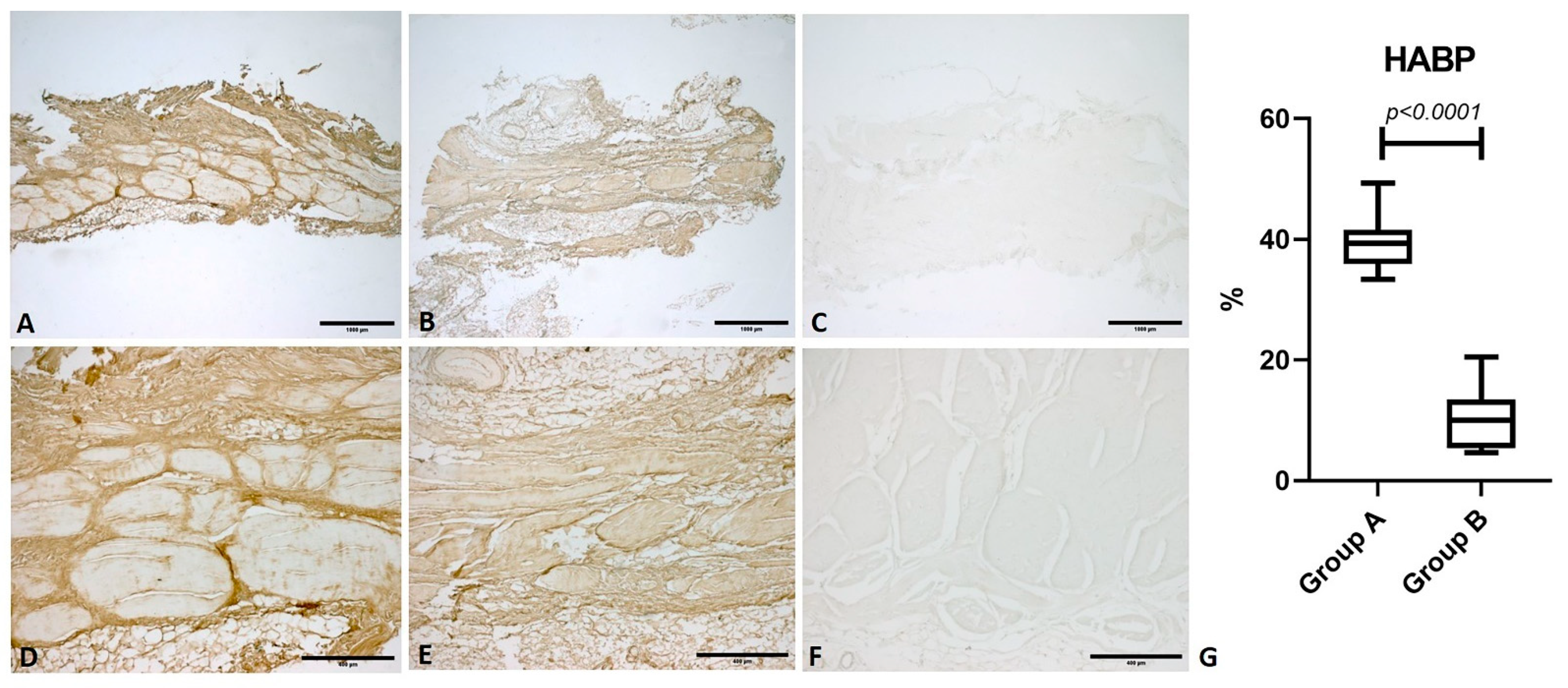
3.2. Immunohistochemical Analysis
4. Discussion
5. Study Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Berenbaum, F.; Walker, C. Osteoarthritis and inflammation: A serious disease with overlapping phenotypic patterns. Postgrad. Med. 2020, 132, 377–384. [Google Scholar] [CrossRef] [PubMed]
- Adatia, A.; Rainsford, K.D.; Kean, W.F. Osteoarthritis of the knee and hip. Part I: Aetiology and pathogenesis as a basis for pharmacotherapy. J. Pharm. Pharmacol. 2012, 64, 617–625. [Google Scholar] [CrossRef] [PubMed]
- Robinson, P.D.; McEwan, J.; Adukia, V.; Prabhakar, M. Osteoarthritis and arthroplasty of the hip and knee. Br. J. Hosp. Med. 2018, 79, C54–C59. [Google Scholar] [CrossRef] [PubMed]
- Dagenais, S.; Garbedian, S.; Wai, E.K. Systematic Review of the Prevalence of Radiographic Primary Hip Osteoarthritis. Clin. Orthop. Relat. Res. 2009, 467, 623–637. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barbour, K.E.; Lui, L.-Y.; Nevitt, M.C.; Murphy, L.B.; Helmick, C.G.; Theis, K.A.; Hochberg, M.C.; Lane, N.E.; Hootman, J.M.; Cauley, J.A.; et al. Hip Osteoarthritis and the Risk of All-Cause and Disease-Specific Mortality in Older Women: A Population-Based Cohort Study. Arthritis Rheumatol. 2015, 67, 1798–1805. [Google Scholar] [CrossRef] [Green Version]
- Jordan, J.M.; Helmick, C.G.; Renner, J.B.; Luta, G.; Dragomir, A.D.; Woodard, J.; Fang, F.; Schwartz, T.A.; Nelson, A.E.; Abbate, L.M.; et al. Prevalence of hip symptoms and radiographic and symptomatic hip osteoarthritis in African Americans and Caucasians: The Johnston County Osteoarthritis Project. J. Rheumatol. 2009, 36, 809–815. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, C.; Linsenmeyer, K.D.; Vlad, S.C.; Guermazi, A.; Clancy, M.M.; Niu, J.; Felson, D.T. Prevalence of radiographic and symptomatic hip osteoarthritis in an urban United States community: The Framingham osteoarthritis study. Arthritis Rheumatol. 2014, 66, 3013–3017. [Google Scholar] [CrossRef] [PubMed]
- Quintana, J.M.; Arostegui, I.; Escobar, A.; Azkarate, J.; Goenaga, J.I.; Lafuente, I. Prevalence of knee and hip osteoarthritis and the appropriateness of joint replacement in an older population. Arch. Intern. Med. 2008, 168, 1576–1584. [Google Scholar] [CrossRef] [PubMed]
- Park, J.H.; Hong, J.Y.; Han, K.; Suh, S.W.; Park, S.Y.; Yang, J.H.; Han, S.W. Prevalence of symptomatic hip, knee, and spine osteoarthritis nationwide health survey analysis of an elderly Korean population. Medicine 2017, 96, e6372. [Google Scholar] [CrossRef]
- Postler, A.; Ramos, A.L.; Goronzy, J.; Günther, K.P.; Lange, T.; Schmitt, J.; Zink, A.; Hoffmann, F. Prevalence and treatment of hip and knee osteoarthritis in people aged 60 years or older in Germany: An analysis based on health insurance claims data. Clin. Interv. Aging 2018, 13, 2339–2349. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Macías-Hernández, S.I.; Zepeda-Borbón, E.R.; Lara-Vázquez, B.I.; Cuevas-Quintero, N.M.; Morones-Alba, J.D.; Cruz-Medina, E.; Nava-Bringas, T.I.; Miranda-Duarte, A. Prevalence of clinical and radiological osteoarthritis in knee, hip, and hand in an urban adult population of Mexico City. Reumatol. Clin. 2020, 16 Pt 2, 156–160. [Google Scholar] [CrossRef]
- Rees, H.W. Management of Osteoarthritis of the Hip. J. Am. Acad. Orthop. Surg. 2020, 28, e288–e291. [Google Scholar] [CrossRef] [PubMed]
- Canetti, E.F.D.; Schram, B.; Orr, R.M.; Knapik, J.; Pope, R. Risk factors for development of lower limb osteoarthritis in physically demanding occupations: A systematic review and meta-analysis. Appl. Ergon. 2020, 86, 103097. [Google Scholar] [CrossRef] [PubMed]
- Lespasio, M.J.; Sultan, A.A.; Piuzzi, N.S.; Khlopas, A.; Husni, M.E.; Muschler, G.F.; Mont, M.A. Hip Osteoarthritis: A Primer. Perm. J. 2018, 22, 17–84. [Google Scholar] [CrossRef] [Green Version]
- Grässel, S.; Muschter, D. Recent advances in the treatment of osteoarthritis. F1000Research 2020, 9. [Google Scholar] [CrossRef] [PubMed]
- Bowden, J.L.; Hunter, D.J.; Deveza, L.A.; Duong, V.; Dziedzic, K.S.; Allen, K.D.; Chan, P.K.; Eyles, J.P. Core and adjunctive interventions for osteoarthritis: Efficacy and models for implementation. Nat. Rev. Rheumatol. 2020, 16, 434–447. [Google Scholar] [CrossRef]
- Murphy, N.J.; Eyles, J.P.; Hunter, D.J. Hip Osteoarthritis: Etiopathogenesis and Implications for Management. Adv. Ther. 2016, 33, 1921–1946. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aresti, N.; Kassam, J.; Nicholas, N.; Achan, P. Hip osteoarthritis. BMJ 2016, 354, i3405. [Google Scholar] [CrossRef]
- Urits, I.; Orhurhu, V.; Powell, J.; Murthy, A.; Kiely, B.; Shipon, S.; Kaye, R.J.; Kaye, A.D.; Arron, B.L.; Cornett, E.M.; et al. Minimally Invasive Therapies for Osteoarthritic Hip Pain: A Comprehensive Review. Curr. Pain Headache Rep. 2020, 24, 37. [Google Scholar] [CrossRef]
- Liao, C.D.; Chen, H.C.; Kuo, Y.C.; Tsauo, J.Y.; Huang, S.W.; Liou, T.H. Effects of Muscle Strength Training on Muscle Mass Gain and Hypertrophy in Older Adults with Osteoarthritis: A Systematic Review and Meta-Analysis. Arthritis Care Res. 2020, 72, 1703–1718. [Google Scholar] [CrossRef]
- Latourte, A.; Kloppenburg, M.; Richette, P. Emerging pharmaceutical therapies for osteoarthritis. Nat. Rev. Rheumatol. 2020, 16, 673–688. [Google Scholar] [CrossRef] [PubMed]
- Migliore, A.; Paoletta, M.; Moretti, A.; Liguori, S.; Iolascon, G. The perspectives of intra-articular therapy in the management of osteoarthritis. Expert Opin. Drug Deliv. 2020, 17, 1213–1226. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Z.; Ma, J.X.; Ma, X.L. Different Intra-articular Injections as Therapy for Hip Osteoarthritis: A Systematic Review and Network Meta-analysis. Arthroscopy 2020, 36, 1452–1464.e2. [Google Scholar] [CrossRef]
- Li, C.; Cao, Z.; Li, W.; Liu, R.; Chen, Y.; Song, Y.; Liu, G.; Song, Z.; Liu, Z.; Lu, C.; et al. A review on the wide range applications of hyaluronic acid as a promising rejuvenating biomacromolecule in the treatments of bone related diseases. Int. J. Biol. Macromol. 2020, 165 Pt A, 1264–1275. [Google Scholar] [CrossRef]
- National Clinical Guideline Centre (UK). Osteoarthritis: Care and Management in Adults. National Institute for Health and Care Excellence (UK). 2014. Available online: http://www.ncbi.nlm.nih.gov/books/NBK248069/ (accessed on 2 November 2020).
- Piuzzi, N.S.; Slullitel, P.A.I.; Bertona, A.; Oñativia, J.I.; Albergo, I.; Zanotti, G.; Buttaro, M.A.; Piccaluga, F.; Comba, F.M. Hip arthroscopy in osteoarthritis: A systematic review of the literature. Hip Int. 2016, 26, 8–14. [Google Scholar] [CrossRef] [PubMed]
- Vilabril, F.; Rocha-Melo, J.; Gonçalves, J.V.; Vilaça-Costa, J.; Brito, I. Hip osteoarthritis treatment with intra-articular injections: Hyaluronic acid versus glucocorticoid—A systematic review. Acta Reumatol. Port. 2020, 45, 127–136. [Google Scholar]
- Casato, G.; Stecco, C.; Busin, R. Role of fasciae in nonspecific low back pain. Eur. J. Transl. Myol. 2019, 29, 8330. [Google Scholar] [CrossRef]
- Bertoldo, D.; Pirri, C.; Roviaro, B.; Stecco, L.; Day, J.A.; Fede, C.; Guidolin, D.; Stecco, C. Pilot Study of Sacroiliac Joint Dysfunction Treated with a Single Session of Fascial Manipulation® Method: Clinical Implications for Effective Pain Reduction. Medicina 2021, 57, 691. [Google Scholar] [CrossRef]
- Day, J.A.; Stecco, C.; Stecco, A. Application of Fascial Manipulation technique in chronic shoulder pain—Anatomical basis and clinical implications. J. Bodyw. Mov. Ther. 2009, 13, 128–135. [Google Scholar] [CrossRef]
- Stecco, C. Functional Atlas of the Human Fascial System; Elsevier Health Sciences: London, UK, 2015. [Google Scholar]
- Stecco, C.; Schleip, R. A fascia and the fascial system. J. Bodyw. Mov. Ther. 2016, 20, 139–140. [Google Scholar] [CrossRef] [Green Version]
- Schleip, R.; Jäger, H.; Klingler, W. What is “fascia”? A review of different nomenclatures. J. Bodyw. Mov. Ther. 2012, 16, 496–502. [Google Scholar] [CrossRef]
- Kumka, M.; Bonar, J. Fascia: A morphological description and classification system based on a literature review. J. Can. Chiropr. Assoc. 2012, 56, 179–191. [Google Scholar] [PubMed]
- Fede, C.; Gaudreault, N.; Fan, C.; Macchi, V.; De Caro, R.; Stecco, C. Morphometric and dynamic measurements of muscular fascia in healthy individuals using ultrasound imaging: A summary of the discrepancies and gaps in the current literature. Surg. Radiol. Anat. 2018, 40, 1329–1341. [Google Scholar] [CrossRef] [PubMed]
- Pirri, C.; Fede, C.; Petrelli, L.; Guidolin, D.; Fan, C.; De Caro, R.; Stecco, C. An anatomical comparison of the fasciae of the thigh: A macroscopic, microscopic and ultrasound imaging study. J. Anat. 2021, 238, 999–1009. [Google Scholar] [CrossRef] [PubMed]
- Fede, C.; Angelini, A.; Stern, R.; Macchi, V.; Porzionato, A.; Ruggieri, P.; De Caro, R.; Stecco, C. Quantification of hyaluronan in human fasciae: Variations with function and anatomical site. J. Anat. 2018, 233, 552–556. [Google Scholar] [CrossRef] [PubMed]
- Fede, C.; Pirri, C.; Petrelli, L.; Guidolin, D.; Fan, C.; De Caro, R.; Stecco, C. Sensitivity of the Fasciae to the Endocannabinoid System: Production of Hyaluronan-Rich Vesicles and Potential Peripheral Effects of Cannabinoids in Fascial Tissue. Int. J. Mol. Sci. 2020, 21, 2936. [Google Scholar] [CrossRef]
- Fede, C.; Pirri, C.; Fan, C.; Albertin, G.; Porzionato, A.; Macchi, V.; De Caro, R.; Stecco, C. Sensitivity of the fasciae to sex hormone levels: Modulation of collagen-I, collagen-III and fibrillin production. PLoS ONE 2019, 14, e0223195. [Google Scholar] [CrossRef]
- Cowman, M.K.; Schmidt, T.A.; Raghavan, P.; Stecco, A. Viscoelastic Properties of Hyaluronan in Physiological Conditions. F1000Research 2015, 4, 622. [Google Scholar] [CrossRef] [Green Version]
- Stecco, C.; Stern, R.; Porzionato, A.; Macchi, V.; Masiero, S.; Stecco, A.; De Caro, R. Hyaluronan within fascia in the etiology of myofascial pain. Surg. Radiol. Anat. 2011, 33, 891–896. [Google Scholar] [CrossRef]
- Fede, C.; Porzionato, A.; Petrelli, L.; Fan, C.; Pirri, C.; Biz, C.; De Caro, R.; Stecco, C. Fascia and soft tissues innervation in the human hip and their possible role in post-surgical pain. J. Orthop. Res. 2020, 38, 1646–1654. [Google Scholar] [CrossRef] [PubMed]
- Huang, B.K.; Tan, W.; Scherer, K.F.; Rennie, W.; Chung, C.B.; Bancroft, L.W. Standard and Advanced Imaging of Hip Osteoarthritis. What the Radiologist Should Know. Semin. Musculoskelet. Radiol. 2019, 23, 289–303. [Google Scholar] [CrossRef] [PubMed]
- Kellgren, J.H.; Lawrence, J.S. Radiological assessment of osteo-arthrosis. Ann. Rheum. Dis. 1957, 16, 494–502. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schneider, C.A.; Rasband, W.S.; Eliceiri, K.W. NIH Image to ImageJ: 25 years of image analysis. Nat. Methods 2012, 9, 671–675. [Google Scholar] [CrossRef]
- Cohen, J. Things I have learned (so far). Am. Psychol. 1990, 45, 1304–1312. [Google Scholar] [CrossRef]
- Stecco, A.; Stern, R.; Fantoni, I.; De Caro, R.; Stecco, C. Fascial Disorders: Implications for Treatment. PMR J. Inj. Funct. Rehabil. 2016, 8, 161–168. [Google Scholar] [CrossRef]
- Pavan, P.; Monti, E.; Bondí, M.; Fan, C.; Stecco, C.; Narici, M.; Reggiani, C.; Marcucci, L. Alterations of Extracellular Matrix Mechanical Properties Contribute to Age-Related Functional Impairment of Human Skeletal Muscles. Int. J. Mol. Sci. 2020, 21, 3992. [Google Scholar] [CrossRef] [PubMed]
- Pratt, R.L. Hyaluronan and the Fascial Frontier. Int. J. Mol. Sci. 2021, 22, 6845. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Group A | Sex | Age (y.) | Height (cm) | Weight (kg) | BMI | Group B | Sex | Age (y.) | Height (cm) | Weight (kg) | BMI |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | F | 73 | 180 | 80 | 24.69 | 1 | F | 90 | 184 | 72 | 21.27 |
| 2 | F | 62 | 172 | 69 | 23.32 | 2 | F | 83 | 185 | 80 | 23.37 |
| 3 | F | 91 | 170 | 70 | 24.22 | 3 | F | 92 | 168 | 65 | 23.03 |
| 4 | M | 89 | 172 | 62 | 20.96 | 4 | M | 90 | 175 | 79 | 25.80 |
| 5 | M | 56 | 180 | 83 | 25.62 | 5 | F | 94 | 182 | 65 | 19.62 |
| 6 | M | 68 | 185 | 78 | 22.79 | 6 | M | 59 | 175 | 93 | 30.37 |
| 7 | M | 89 | 175 | 80 | 26.12 | 7 | F | 86 | 176 | 89 | 28.73 |
| 8 | F | 84 | 185 | 82 | 23.96 | 8 | F | 91 | 177 | 84 | 26.81 |
| 9 | F | 78 | 168 | 70 | 24.80 | 9 | F | 88 | 177 | 84 | 26.81 |
| 10 | F | 79 | 183 | 76 | 22.69 | 10 | M | 93 | 177 | 77 | 24.58 |
| 11 | F | 78 | 175 | 74 | 24.16 | ||||||
| Mean ± SD | 76.9 ± 12 | 177 ± 6.4 | 75 ± 7 | 24 ± 1.53 | Mean ± SD | 85.82 ± 10.1 | 177 ± 5 | 79 ± 9.24 | 25.33 ± 3.1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fantoni, I.; Biz, C.; Fan, C.; Pirri, C.; Fede, C.; Petrelli, L.; Ruggieri, P.; De Caro, R.; Stecco, C. Fascia Lata Alterations in Hip Osteoarthritis: An Observational Cross-Sectional Study. Life 2021, 11, 1136. https://doi.org/10.3390/life11111136
Fantoni I, Biz C, Fan C, Pirri C, Fede C, Petrelli L, Ruggieri P, De Caro R, Stecco C. Fascia Lata Alterations in Hip Osteoarthritis: An Observational Cross-Sectional Study. Life. 2021; 11(11):1136. https://doi.org/10.3390/life11111136
Chicago/Turabian StyleFantoni, Ilaria, Carlo Biz, Chenglei Fan, Carmelo Pirri, Caterina Fede, Lucia Petrelli, Pietro Ruggieri, Raffaele De Caro, and Carla Stecco. 2021. "Fascia Lata Alterations in Hip Osteoarthritis: An Observational Cross-Sectional Study" Life 11, no. 11: 1136. https://doi.org/10.3390/life11111136
APA StyleFantoni, I., Biz, C., Fan, C., Pirri, C., Fede, C., Petrelli, L., Ruggieri, P., De Caro, R., & Stecco, C. (2021). Fascia Lata Alterations in Hip Osteoarthritis: An Observational Cross-Sectional Study. Life, 11(11), 1136. https://doi.org/10.3390/life11111136