
Evaluation of a Novel Dorsal-Cemented Technique for Atlantoaxial Stabilisation in 12 Dogs

 ,
,  ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Criteria for Case Selection and Data Collection
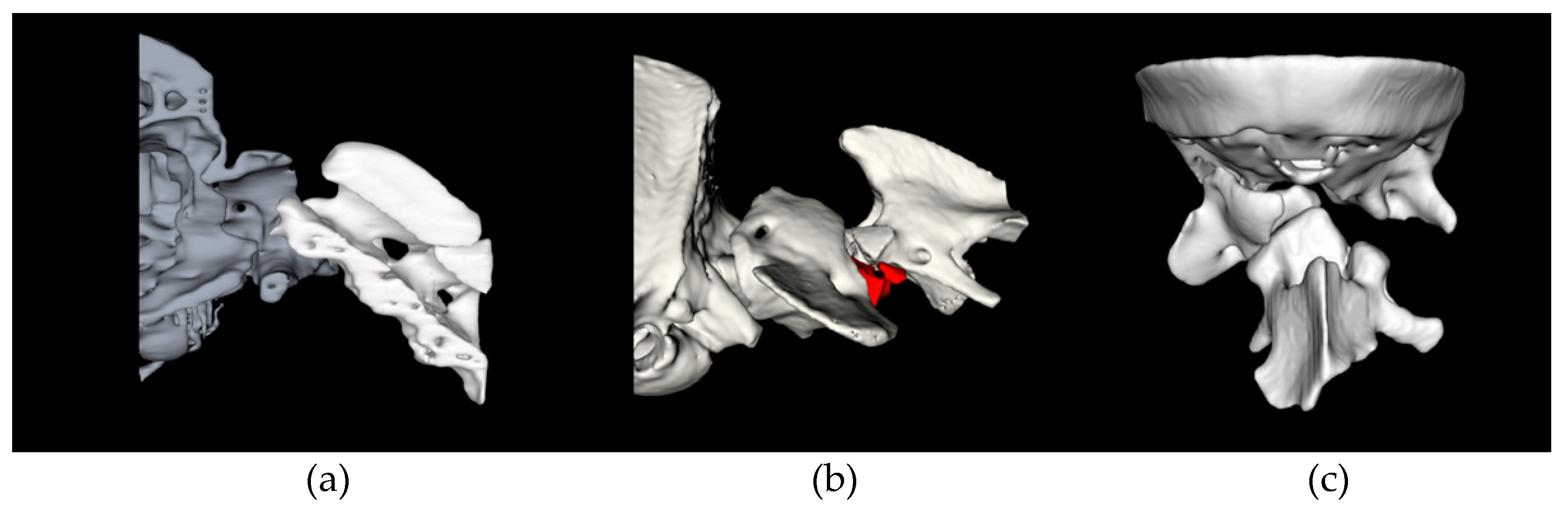
2.2. Advanced Imaging
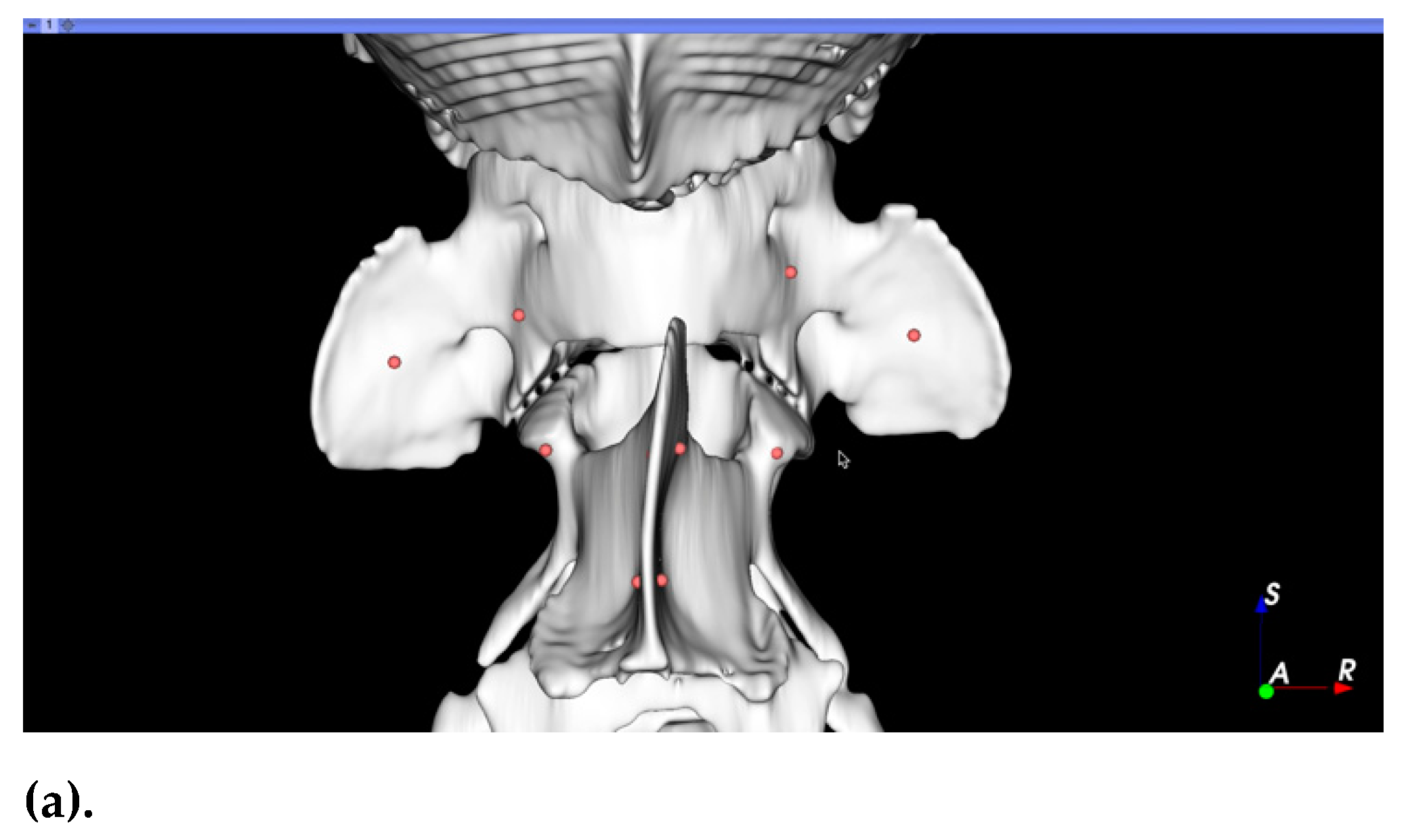
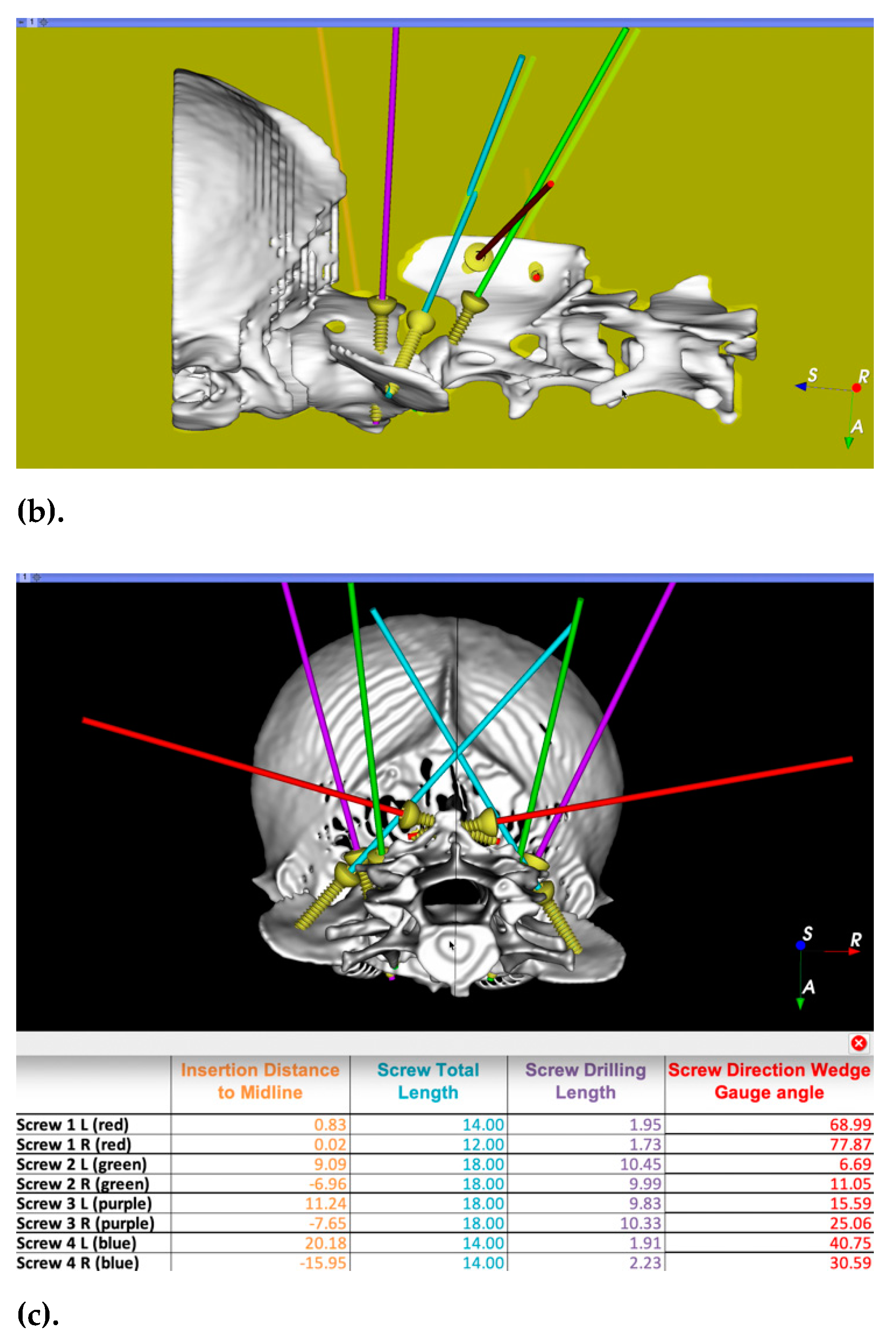
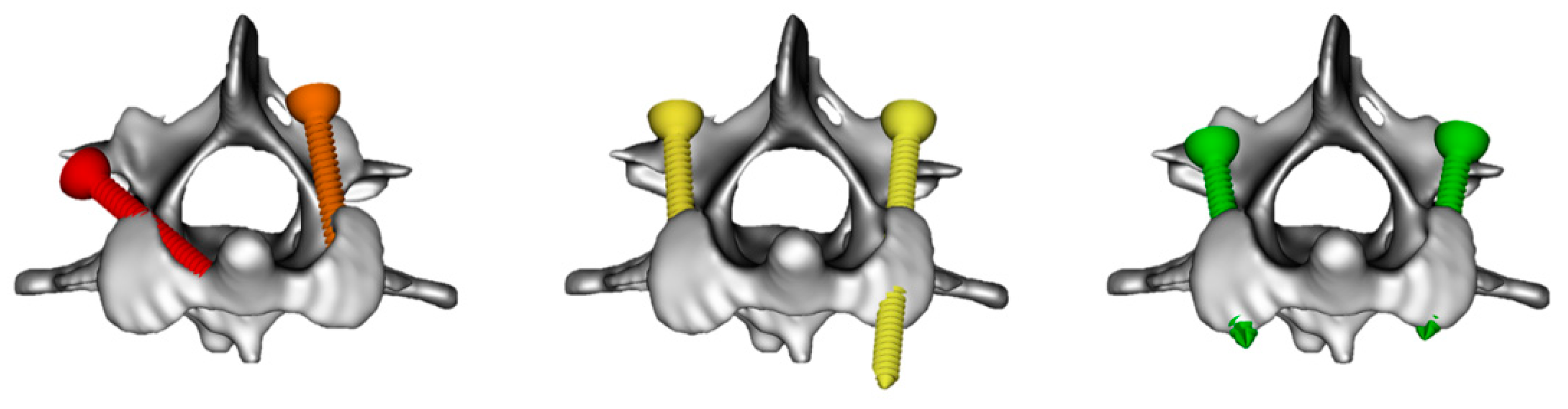
2.3. Surgical Planning
2.4. Surgical Technique
2.5. Immediate Postoperative Care
2.6. Follow-Up
2.7. Implant Accuracy, Bone Fusion, and Implant Failure
3. Results
3.1. Signalment and Clinical Presentation
3.2. Preoperative Imaging Interpretation and Surgical Planning
3.3. Immediate Surgical Outcome
3.4. Perioperative Outcome
3.5. Short-Term Clinical Outcome
3.6. Long-Term Clinical Outcome
3.7. Bone Fusion and Implant Failure
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Downey, R.S. An unusual cause of tetraplegia in a dog. Can. Vet. J. La Rev. Vet. Can. 1967, 8, 216–217. [Google Scholar]
- Geary, J.C.; Oliver, J.E.; Hoerlein, B.F. Atlanto axial subluxation in the canine. J. Small Anim. Pract. 1967, 8, 577–582. [Google Scholar] [CrossRef]
- Stalin, C.; Gutierrez-Quintana, R.; Faller, K.; Guevar, J.; Yeamans, C.; Penderis, J. A review of canine atlantoaxial joint subluxation. Vet. Comp. Orthop. Traumatol. 2015, 28, 1–8. [Google Scholar] [CrossRef]
- Plessas, I.; Volk, H. Signalment, clinical signs and treatment of atlantoaxial subluxation in dogs: A systematic review of 336 published cases from 1967 to 2013. J. Vet. Intern. Med. 2014, 28, 948. [Google Scholar]
- McCarthy, R.J.; Lewis, D.D.; Hosgood, G. Atlantoaxial subluxation in dogs. Comp. Contin. Educ. Pract. Vet. 1995, 17, 215–227. [Google Scholar]
- Slanina, M.C. Atlantoaxial Instability. Vet. Clin. N. Am. Small Anim. Pract. 2016, 46, 265–275. [Google Scholar] [CrossRef] [PubMed]
- Warren-Smith, C.M.; Kneissl, S.; Benigni, L.; Kenny, P.J.; Lamb, C.R. Incomplete ossification of the atlas in dogs with cervical signs. Vet. Radiol. Ultrasound 2009, 50, 635–638. [Google Scholar] [CrossRef]
- Takahashi, F.; Hakozaki, T.; Kouno, S.; Suzuki, S.; Sato, A.; Kanno, N.; Harada, Y.; Yamaguchi, S.; Hara, Y. Epidemiological and morphological characteristics of incomplete ossification of the dorsal neural arch of the atlas in dogs with atlantoaxial instability. Am. J. Vet. Res. 2018, 79, 1079–1086. [Google Scholar] [CrossRef] [PubMed]
- Waschk, M.A.; Vidondo, B.; Carrera, I.; Hernandez-Guerra, A.M.; Moissonnier, P.; Plessas, I.N.; Schmidt, M.J.; Schnötzinger, D.; Forterre, F.; Precht, C. Craniovertebral junction anomalies in small breed dogs with atlantoaxial instability: A multicentre case–control study. Vet. Comp. Orthop. Traumatol. 2019, 32, 033–040. [Google Scholar] [CrossRef]
- Cerda-Gonzalez, S.; Dewey, C.W. Congenital diseases of the craniocervical junction in the dog. Vet. Clin. N. Am. Small Anim. Pract. 2010, 40, 121–141. [Google Scholar] [CrossRef]
- Dewey, C.; Marino, D.; Loughin, C. Craniocervical junction abnormalities in dogs. N. Z. Vet. J. 2013, 61, 202–211. [Google Scholar] [CrossRef] [PubMed]
- Galban, E.M.; Gilley, R.S.; Long, S.N. Surgical stabilization of an occipitoatlantoaxial malformation in an adult dog. Vet. Surg. 2010, 39, 1001–1004. [Google Scholar] [CrossRef] [PubMed]
- Petite, A.; McConnell, F.; De Stefani, A.; McKee, M.; Dennis, R. Abstracts from the annual conference of the european association of veterinary diagnostic imaging. Congenital occipito-atlanto-axial malformation in five dogs. Vet. Radiol. Ultrasound 2009, 50, 118. [Google Scholar] [CrossRef]
- Watson, A.G.; de Lahunta, A.; Evans, H.E. Morphology and embryological interpretation of a congenital occipito-atlanto-axial malformation in a dog. Teratology 1988, 38, 451–459. [Google Scholar] [CrossRef]
- Dolera, M.; Malfassi, L.; Pavesi, S.; Finesso, S.; Mazza, G.; Marcarini, S.; Sala, M.; Carrara, N.; Bianchi, C.; Gambino, J.M. Computed tomography, magnetic resonance imaging and a novel surgical approach of atlanto-axial instability with incongruence in dogs. J. Vet. Med. Sci. 2017. [Google Scholar] [CrossRef]
- Read, R.; Brett, S.; Cahill, J. Surgical treatment of occipito-atlanto-axial malformation in the dog. Aust. Vet. Pract. 1987, 17, 184–189. [Google Scholar]
- Havig, M.E.; Cornell, K.K.; Hawthorne, J.C.; McDonnell, J.J.; Selcer, B.A. Evaluation of nonsurgical treatment of atlantoaxial subluxation in dogs: 19 cases (1992–2001). J. Am. Vet. Med. Assoc. 2005, 227, 257–262. [Google Scholar] [CrossRef]
- Denny, H.R.; Gibbs, C.; Waterman, A. Atlanto-axial subluxation in the dog—a review of 30 cases and an evaluation of treatment by lag screw fixation. J. Small Anim. Pract. 1988, 29, 37–47. [Google Scholar] [CrossRef]
- Jeffery, N.D. Dorsal cross pinning of the atlantoaxial joint: New surgical technique for atlantoaxial subluxation. J. Small Anim. Pract. 1996, 37, 26–29. [Google Scholar] [CrossRef]
- LeCouteur, R.A.; McKeown, D.; Johnson, J.; Eger, C.E. Stabilization of atlantoaxial subluxation in the dog, using the nuchal ligament. J. Am. Vet. Med. Assoc. 1980, 177, 1011–1017. [Google Scholar] [PubMed]
- Pujol, E.; Bouvy, B.; Omana, M.; Fortuny, M.; Riera, L.; Pujol, P. Use of the Kishigami atlantoaxial tension band in eight toy breed dogs with atlantoaxial subluxation. Vet. Surg. 2010, 39, 35–42. [Google Scholar] [CrossRef]
- Aikawa, T.; Shibata, M.; Fujita, H. Modified ventral stabilization using positively threaded profile pins and polymethylmethacrylate for atlantoaxial instability in 49 dogs. Vet. Surg. 2013, 42, 683–692. [Google Scholar] [CrossRef]
- Thomas, W.B.; Sorjonen, D.C.; Simpson, S.T. Surgical management of atlantoaxial subluxation in 23 dogs. Vet. Surg. 1991, 20, 409–412. [Google Scholar] [CrossRef] [PubMed]
- Beaver, D.P.; Ellison, G.W.; Lewis, D.D.; Goring, R.L.; Kubilis, P.S.; Barchard, C. Risk factors affecting the outcome of surgery for atlantoaxial subluxation in dogs: 46 cases (1978–1998). J. Am. Vet. Med. Assoc. 2000, 216, 1104–1109. [Google Scholar] [CrossRef] [PubMed]
- Schulz, K.S.; Waldron, D.R.; Fahie, M. Application of ventral pins and polymethylmethacrylate for the management of atlantoaxial instability: Results in nine dogs. Vet. Surg. 1997, 26, 317–325. [Google Scholar] [CrossRef]
- Platt, S.R.; Chambers, J.N.; Cross, A. A modified ventral fixation for surgical management of atlantoaxial subluxation in 19 dogs. Vet. Surg. 2004, 33, 349–354. [Google Scholar] [CrossRef]
- Sanders, S.G.; Bagley, R.S.; Silver, G.M.; Moore, M.; Tucker, R.L. Outcomes and complications associated with ventral screws, pins, and polymethyl methacrylate for atlantoaxial instability in 12 dogs. J. Am. Anim. Hosp. Assoc. 2004, 40, 204–210. [Google Scholar] [CrossRef] [PubMed]
- Toni, C.; Oxley, B.; Behr, S. Atlanto-axial ventral stabilisation using 3D-printed patient-specific drill guides for placement of bicortical screws in dogs. J. Small Anim. Pract. 2020, 61, 609–616. [Google Scholar] [CrossRef] [PubMed]
- Kamishina, H.; Sugawara, T.; Nakata, K.; Nishida, H.; Yada, N.; Fujioka, T.; Nagata, Y.; Doi, A.; Konno, N.; Uchida, F.; et al. Clinical application of 3D printing technology to the surgical treatment of atlantoaxial subluxation in small breed dogs. PLoS ONE 2019, 14, e0216445. [Google Scholar] [CrossRef]
- Leblond, G.; Barnard, L.; Gutierrez-Quintana, R. Proceedings 31st Symposium ESVN-ECVN. Evaluation of a preoperative implant placement planning method for canine atlantoaxial stabilisation. J. Vet. Intern. Med. 2020, 34. [Google Scholar] [CrossRef]
- Sanchez-Masian, D.; Lujan-Feliu-Pascual, A.; Font, C.; Mascort, J. Dorsal stabilization of atlantoaxial subluxation using non-absorbable sutures in toy breed dogs. Vet. Comp. Orthop. Traumatol. 2014, 27, 62–67. [Google Scholar] [CrossRef] [PubMed]
- Leblond, G.; Gaitero, L.; Moens, N.M.; Zur Linden, A.; James, F.M.; Monteith, G.; Runciman, J. Computed tomography analysis of ventral atlantoaxial optimal safe implantation corridors in 27 dogs. Vet. Comp. Orthop. Traumatol. 2017, 30, 413–423. [Google Scholar] [PubMed]
- Wang, X.; Chou, D.; Jian, F. Influence of postoperative O-C2 angle on the development of dysphagia after occipitocervical fusion surgery: Results from a retrospective analysis and prospective validation. World Neurosurg. 2018, 116, e595–e601. [Google Scholar] [CrossRef] [PubMed]
- Cerda-Gonzalez, S.; Dewey, C.W.; Scrivani, P.V.; Kline, K.L. Imaging features of atlanto-occipital overlapping in dogs. Vet. Radiol. Ultrasound Off. J. Am. Coll. Vet. Radiol. Int. Vet. Radiol. Assoc. 2009, 50, 264–268. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, F.; Hakozaki, T.; Kouno, S.; Suzuki, S.; Sato, A.; Kanno, N.; Harada, Y.; Yamaguchi, S.; Hara, Y. Atlantooccipital overlapping and its effect on outcomes after ventral fixation in dogs with atlantoaxial instability. J. Vet. Med. Sci. 2018, 80, 526–531. [Google Scholar] [CrossRef]
- Fujita, A.; Nishimura, R. Surgical stabilization of the atlanto-occipital overlap with atlanto-axial instability in a dog. Jpn. J. Vet. Res. 2016, 64, 141–145. [Google Scholar]
- Rylander, H.; Robles, J.C. Diagnosis and treatment of a chronic atlanto-occipital subluxation in a dog. J. Am. Anim. Hosp. Assoc. 2007, 43, 173–178. [Google Scholar] [CrossRef] [PubMed]
- Evans, H.E.; de Lahunta, A. Miller’s anatomy of the dog, 4th ed.; Elsevier/Saunders: St. Louis, MO, USA, 2012. [Google Scholar]
- Leblond, G. Canine Atlantoaxial Ventral Stabilization: Computed Tomography Analysis of Optimal Safe Implantation Corridors and Comparison of the Technical Outcome and Biomechanical Properties of 3 Surgical Techniques. Ph.D. Thesis, University of Guelph, Guelph, ON, Canada, 2015. Available online: http://hdl.handle.net/10214/9354 (accessed on 27 September 2021).








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Case | Signalment (Breed, Age in Months, Gender, Weight) | Onset/Clinical Progression | Additional Anomalies | Surgical Time (Sx), Hospitalisation (H) and Complications (C) | Neurological Score 1 | Final Outcome (Time in Months) | |
|---|---|---|---|---|---|---|---|
| Initial | Follow-Up | ||||||
| 1 | Dachshund, 4 m, ME, 3.3 kg | Chronic and progressive | Dens hypoplasia, C1–C2 incongruence | Sx: 260 min H: 2 days C: none | Ad: 3 Dis: 3 | ST: 3 LT: 2 | 19 m: improved gait, unable to jump |
| 2 | Maltese, 17 m, ME, 1.5 kg | Paroxysmal episodes pain | None | Sx: 155 min H: 2 days C: regurgitation (short lived) | Ad: 1 Dis: 2 | ST: 2 LT: 0 | 20 m: much-improved gait; rare episodes of mild pain, occasional cough when drinking |
| 3 | Chihuahua, 10 m, FE, 2 kg | Chronic progressive with peracute deterioration | Dens hypoplasia, atlanto-occipital overlap | Sx: 300 min H: 4 days C: subtle torticollis. | Ad: 4 Dis: 4 | ST: 3 LT: 2 | 11 m: improved gait; rare episodes of 2–3 seconds thoracic limb collapse and limb paddling. |
| 4 | Labrador Retriever cross, 3 m, FE, 9 kg | Trauma C1 and C2 fracture | Incomplete fusion of C1 ventral arch | Sx: 215 min H: 3 days C: none | Ad: 4* Dis: 3 | ST: 0 LT: 0 | 12 m: normal gait; subtle stiffness of the neck. |
| 5 | Chihuahua cross, 23 m, FN, 2.2 kg | Chronicprogressive | Dens aplasia, C1–C2 incongruence | Sx: 165 min H: 4 days C: none | Ad: 3 Dis: 3 | ST: X LT: 0 | 16 m: normal gait |
| 6 | German Shorthaired Pointer, 6 m, ME, 25 kg | Trauma C2 fracture | None | Sx: 175 min H: 10 days C: none | Ad: 4* Dis: 2 | ST: 0 LT: 0 | 16 m: normal gait |
| 7 | Chihuahua, 11 m, MN, 2.2 kg | Single acute episode of pain, collapse, and ataxia | C1 incomplete dorsal arch fusion, caudal occipital malformation, | Sx: 220 min H: 2 days C: none | Ad: 2 Dis: 2 | ST: 2 LT: 0 | 10 m: improved gait; 3 further paroxysmal episodes of syncope vs. seizures. Reverse sneezing and occasional dysphagia. Frequent neck scratching responding to gabapentin |
| 8 | Yorkshire Terrier, 4 m, FE, 1.7 kg | Subacute | Dens agenesis, atlanto-occipital overlap (suspect instability) | Sx: 160 min H: 2 days C: none | Ad: 5 Dis: 4 | ST: 2 LT: 2 | 8 m: improved gait; mild ataxia in all four limbs (suspected occipito-atlantal instability 5 m postsurgery due to acute deterioration) |
| 9 | Cockapoo, 4 m, FE, 3.8 kg | Acute after collision with another dog | Complex OAAM, partial occipito-atlantal fusion, C1–C2 incongruence | Sx: 220 min H: 4 days C: none | Ad: 4 Dis: 2 | ST: 0 LT: 0 | 6 m: improved gait; subtle low head carriage.Rare paroxysmal vestibular episodes (improving with diet adjustment/gabapentin) |
| 10 | Chihuahua, 34 m, MN, 2.1 kg | Paroxysmal episodes of pain and lateral recumbency | C1–C2 incongruence | Sx: 165 min H: 2 days C: none | Ad: 1 Dis: 2 | ST: 0 LT: 0 | 6 m: return to normal (phone communication only) |
| 11 | Dachshund, 75 m, FN, 4.7 kg | Paroxysmal vestibular episodes 2 | C2–3 block vertebrae | Sx: 245 min H: 3 days C: none | Ad: 0 Dis: 0 | ST: 0 LT: 0 | 6 m: normal gait. No episodes since surgery |
| 12 | Lagotto Romagnolo, 4 m, FE, 8.5 kg | Acute and progressive | Complex OAAM, partial occipito-atlantal fusion | Sx: 200 min H: 2 days C: subcutaneous seroma and subtle torticollis | Ad: 3 Dis: 3 | ST: 1 LT: 0 | 6 m: improved gait; mild over-reaching of all four limbs. Slight resistance to cervical ventroflexion |
| Case | Screw Sites (n) | Screws Grading Score 1 | Bone Graft | C1–C2 Fusion (Location) | Construct Failure | CT Time Postsurgery (Months) | ||
|---|---|---|---|---|---|---|---|---|
| C1 | C2 | n | Sites | |||||
| 1 | LM: 2 Wi: 0 | AS: 2 SP: 1 | Score 0: 4 Score 1: 1 Score 2: 0 | LM, AS, SP LM | Yes | Yes (C1 dorsal arch and C1–C2 articular surfaces) | No | 19 |
| 2 | LM: 2 Wi: 0 | AS: 2 SP: 1 | Score 0: 4 Score 1: 1 Score 2: 0 | LM, AS, SP LM | Yes | No | No | 20 |
| 3 | LM: 2 Wi: 0 | AS: 2 SP: 1 | Score 0: 3 Score 1: 2 Score 2: 0 | LM, AS, SP LM, AS | No | No | Yes | 11 |
| 4 | LM: 2 Wi: 0 | AS: 2 SP: 1 | Score 0: 2 Score 1: 1 Score 2: 2 | AS, SP LM LM, AS | No | Yes (C1 dorsal arch) | No | 12 |
| 5 | LM: 2 Wi: 0 | AS: 2 SP: 1 | Score 0: 4 Score 1: 1 Score 2: 0 | LM, AS, SP AS | No | No | No | 16 |
| 6 | LM: 2 Wi: 0 | AS: 2 SP: 1 | Score 0: 3 Score 1: 2 Score 2: 0 | LM, AS, SP LM, AS | No | Partial bone remodelling (C1 dorsal arch and C1–C2 articular surfaces) | No | 16 |
| 7 | LM: 2 Wi: 0 | AS: 2 SP: 2 | Score 0: 4 Score 1: 1 Score 2: 1 | AS, SP LM LM | No | No | No | 10 |
| 8 | LM: 2 Wi: 0 | AS: 1 SP: 1 | Score 0: 3 Score 1: 1 Score 2: 0 | LM, AS, SP AS | No | No | No | 5 |
| 9 2 | LM: 2 Wi: 2 | AS: 2 SP: 2 | Score 0: 6 Score 1: 2 Score 2: 0 | LM, Wi, AS, SP LM, AS | No | Partial bone remodelling (C1 ventral arch) | No | 6 |
| 10 | LM: 2 Wi: 2 | AS: 2 SP: 2 | Score 0: 6 Score 1: 2 Score 2: 0 | LM, Wi, AS, SP AS, Wi | No | n/a | n/a | n/a |
| 11 | LM: 2 Wi: 2 | AS: 2 SP: 2 | Score 0: 5 Score 1: 2 Score 2: 1 | LM, AS, SP LM, AS AS | Yes | No | No | 6 |
| 12 | LM: 2 Wi: 2 | AS: 2 SP: 2 | Score 0: 7 Score 1: 1 Score 2: 0 | LM, Wi, AS, SP LM | Yes | Partial bone remodelling (C1–C2 right articular surface) | No | 6 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tabanez, J.; Gutierrez-Quintana, R.; Kaczmarska, A.; José-López, R.; Nadal, V.G.; Rotter, C.; Leblond, G. Evaluation of a Novel Dorsal-Cemented Technique for Atlantoaxial Stabilisation in 12 Dogs. Life 2021, 11, 1039. https://doi.org/10.3390/life11101039
Tabanez J, Gutierrez-Quintana R, Kaczmarska A, José-López R, Nadal VG, Rotter C, Leblond G. Evaluation of a Novel Dorsal-Cemented Technique for Atlantoaxial Stabilisation in 12 Dogs. Life. 2021; 11(10):1039. https://doi.org/10.3390/life11101039
Chicago/Turabian StyleTabanez, Joana, Rodrigo Gutierrez-Quintana, Adriana Kaczmarska, Roberto José-López, Veronica Gonzalo Nadal, Carina Rotter, and Guillaume Leblond. 2021. "Evaluation of a Novel Dorsal-Cemented Technique for Atlantoaxial Stabilisation in 12 Dogs" Life 11, no. 10: 1039. https://doi.org/10.3390/life11101039
APA StyleTabanez, J., Gutierrez-Quintana, R., Kaczmarska, A., José-López, R., Nadal, V. G., Rotter, C., & Leblond, G. (2021). Evaluation of a Novel Dorsal-Cemented Technique for Atlantoaxial Stabilisation in 12 Dogs. Life, 11(10), 1039. https://doi.org/10.3390/life11101039