
The Effect of Absorbable and Non-Absorbable Sutures on Nasal Width Following Cinch Sutures in Orthognathic Surgery

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
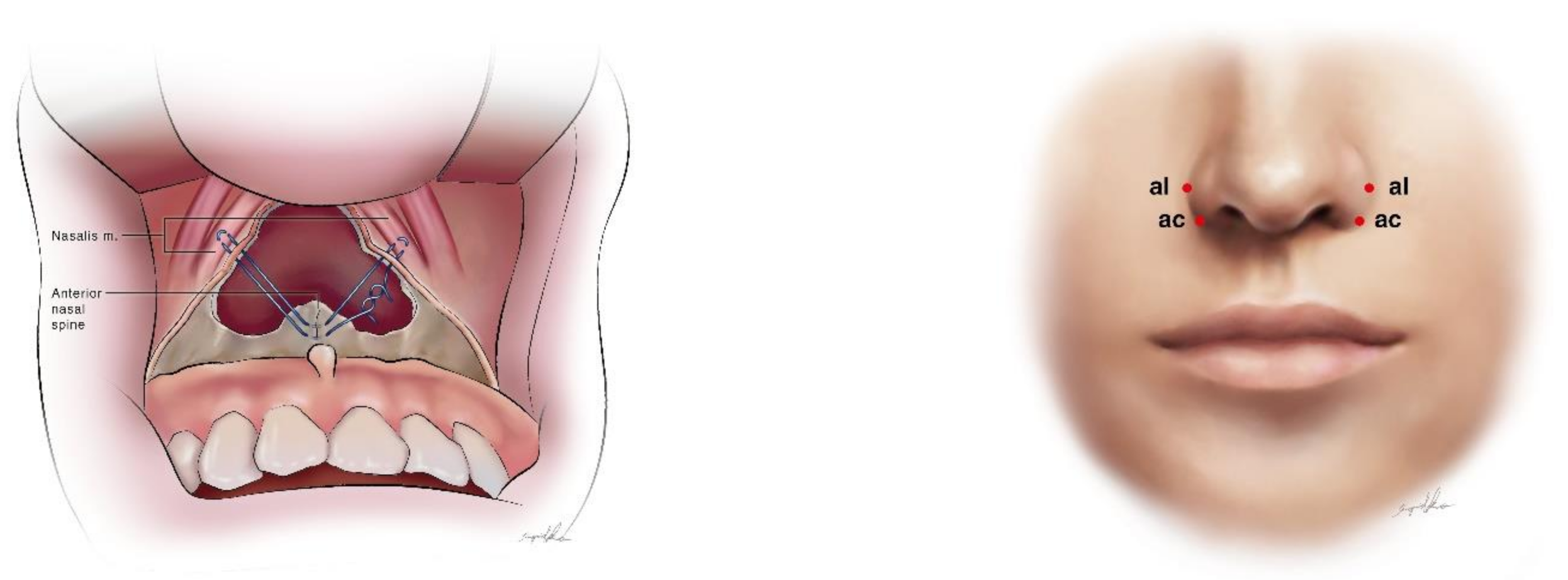
2.2. Surgical Method
2.3. Assessment of Nasal Soft Tissue Change
2.4. Statistics
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Steiner, C.C. Cephalometrics in clinical practice. Angle Orthod. 1959, 29, 8–29. [Google Scholar]
- Steiner, C.C. Cephalometrics for you and me. Am. J. Orthod. 1953, 39, 729–755. [Google Scholar] [CrossRef]
- Jakobsone, G.; Stenvik, A.; Sandvik, L.; Espeland, L. Three-year follow-up of bimaxillary surgery to correct skeletal Class III malocclusion: Stability and risk factors for relapse. Am. J. Orthod. Dentofac. Orthop. 2011, 139, 80–89. [Google Scholar] [CrossRef]
- Liao, Y.F.; Chen, Y.F.; Yao, C.F.; Chen, Y.A.; Chen, Y.R. Long-term outcomes of bimaxillary surgery for treatment of asymmetric skeletal class III deformity using surgery-first approach. Clin. Oral Investig. 2019, 23, 1685–1693. [Google Scholar] [CrossRef] [PubMed]
- Rosen, H.M. Lip-nasal aesthetics following Le Fort I osteotomy. Plast. Reconstr. Surg. 1988, 81, 171–182. [Google Scholar] [CrossRef]
- Sarver, D.M.; Weissman, S.M. Long-term soft tissue response to LeFort I maxillary superior repositioning. Angle Orthod. 1991, 61, 267–276. [Google Scholar] [CrossRef]
- Millard, D.R., Jr. The alar cinch in the flat, flaring nose. Plast. Reconstr. Surg. 1980, 65, 669–672. [Google Scholar] [CrossRef]
- Rauso, R.; Gherardini, G.; Santillo, V.; Biondi, P.; Santagata, M.; Tartaro, G. Comparison of two techniques of cinch suturing to avoid widening of the base of the nose after Le Fort I osteotomy. Br. J. Oral Maxillofac. Surg. 2010, 48, 356–359. [Google Scholar] [CrossRef]
- Ritto, F.G.; Medeiros, P.J.; de Moraes, M.; Ribeiro, D.P. Comparative analysis of two different alar base sutures after Le Fort I osteotomy: Randomized double-blind controlled trial. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2011, 111, 181–189. [Google Scholar] [CrossRef]
- Nirvikalpa, N.; Narayanan, V.; Wahab, A.; Ramadorai, A. Comparison between the classical and a modified trans-septal technique of alar cinching for Le Fort I osteotomies: A prospective randomized controlled trial. Int. J. Oral Maxillofac. Surg. 2013, 42, 49–54. [Google Scholar] [CrossRef] [PubMed]
- Stewart, A.; Edler, R.J. Efficacy and stability of the alar base cinch suture. Br. J. Oral Maxillofac. Surg. 2011, 49, 623–626. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.Y.; Lin, C.C.; Ko, E.W. Effects of two alar base suture techniques suture techniques on nasolabial changes after bimaxillary orthognathic surgery in Taiwanese patients with class III malocclusions. Int. J. Oral Maxillofac. Surg. 2015, 44, 816–822. [Google Scholar] [CrossRef]
- Raithatha, R.; Naini, F.B.; Patel, S.; Sherriff, M.; Witherow, H. Long-term stability of limiting nasal alar base width changes with a cinch suture following Le Fort I osteotomy with submental intubation. Int. J. Oral Maxillofac. Surg. 2017, 46, 1372–1379. [Google Scholar] [CrossRef]
- Jin, H.R.; Won, T.B. Rhinoplasty in the Asian Patient. Clin. Plast. Surg. 2016, 43, 265–279. [Google Scholar] [CrossRef]
- Vaca, E.E.; Alghoul, M.S. Upper Blepharoplasty with Endoscopically Assisted Brow Lift to Restore Harmonious Upper Lid Arc Curvatures. Plast. Reconstr. Surg. 2020, 146, 565e–568e. [Google Scholar] [CrossRef]
- Sajid, M.S.; Parampalli, U.; Baig, M.K.; McFall, M.R. A systematic review on the effectiveness of slowly-absorbable versus non-absorbable sutures for abdominal fascial closure following laparotomy. Int. J. Surg. 2011, 9, 615–625. [Google Scholar] [CrossRef] [Green Version]
- Chen, Y.A.; Ng, L.S.; Ko EW, C.; Chen, Y.R. Mandibular contouring during orthognathic surgery using the modified hunsuck technique. J. Craniofacial Surg. 2017, 28, 239–240. [Google Scholar] [CrossRef]
- Chou, P.Y.; Denadai, R.; Yao, C.F.; Chen, Y.A.; Chang, C.S.; Lin CC, H.; Chen, Y.R. History and evolution of orthognathic surgery at Chang Gung Craniofacial Center: Lessons learned from 35-year experience. Ann. Plast. Surg. 2020, 84, S60–S68. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.Y.; Denadai, R.; Chou, P.Y.; Yao, C.F.; Chen, Y.A.; Wang, P.F.; Chen, Y.R. Impact of the Different Types of Le Fort I Maxillary Surgical Movement on Nasal Width Changes: A Photogrammetric Analysis. Ann. Plast. Surg. 2021, 86, S64–S69. [Google Scholar] [CrossRef] [PubMed]
- Maal, T.J.; van Loon, B.; Plooij, J.M.; Rangel, F.; Ettema, A.M.; Borstlap, W.A.; Berge, S.J. Registration of 3-dimensional facial photographs for clinical use. J. Oral Maxillofac. Surg. 2010, 68, 2391–2401. [Google Scholar] [CrossRef] [PubMed]
- Farkas, L.G. Anthropometry of the Head and Neck, 2nd ed.; Raven Press: New York, NY, USA, 1994. [Google Scholar] [CrossRef]
- Kahkhaie, K.R.; Keikhaie, K.R.; Vahed, A.S.; Shirazi, M.; Amjadi, N. Randomized comparison of nylon versus absorbing polyglactin 910 for fascial closure in caesarean section. Iran. Red Crescent Med, J. 2014, 16, e12580. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Durmaz, A.; Kilic, A.; Gumral, R.; Yildizoglu, U.; Polat, B. The effects of different suture materials in the nasal cavity. J. Laryngol. Otol. 2016, 130, 352–356. [Google Scholar] [CrossRef]
- Betts, N.J.; Vig, K.W.; Vig, P.; Spalding, P.; Fonseca, R.J. Changes in the nasal and labial soft tissues after surgical repositioning of the maxilla. Int. J. Adult Orthodon. Orthognath. Surg. 1993, 8, 7–23. [Google Scholar] [CrossRef]
- Mitchell, C.; Oeltjen, J.; Panthaki, Z.; Thaller, S.R. Nasolabial aesthetics. J. Craniofac. Surg. 2007, 18, 756–765. [Google Scholar] [CrossRef]
- Ryckman, M.S.; Harrison, S.; Oliver, D.; Sander, C.; Boryor, A.A.; Hohmann, A.A.; Kilic, F.; Kim, K.B. Soft-tissue changes after maxillomandibular advancement surgery assessed with cone-beam computed tomography. Am. J. Orthod. Dentofacial. Orthop. 2010, 137, S86–S93. [Google Scholar] [CrossRef]
- Denadai, R.; Chou, P.Y.; Lin, Y.Y.; Yao, C.F.; Chen, Y.A.; Huang, C.S.; Chen, Y.R. Type of maxillary segment mobilization affects three-dimensional nasal morphology. J. Plast. Reconstr. Aesthetic Surg. 2021, 74, 592–604. [Google Scholar] [CrossRef]
- Denadai, R.; Chou, P.Y.; Yao, C.F.; Chen, Y.A.; Lin, Y.Y.; Huang, C.S.; Chen, Y.R. Effect of Le Fort I Maxillary Repositioning on Three-Dimensional Nasal Tip Rotation: A Comparative Study with Implication for the Asian Nose. Plast. Reconstr. Surg. 2021, 147, 903–914. [Google Scholar] [CrossRef]
- Howley, C.; Ali, N.; Lee, R.; Cox, S. Use of the alar base cinch suture in Le Fort I osteotomy: Is it effective? Br. J. Oral Maxillofac. Surg. 2011, 49, 127–130. [Google Scholar] [CrossRef]
- Shoji, T.; Muto, T.; Takahashi, M.; Akizuki, K.; Tsuchida, Y. The stability of an alar cinch suture after Le Fort I and mandibular osteotomies in Japanese patients with Class III malocclusions. Br. J. Oral Maxillofac. Surg. 2012, 50, 361–364. [Google Scholar] [CrossRef]
- Liu, X.; Zhu, S.; Hu, J. Modified versus classic alar base sutures after LeFort I osteotomy: A systematic review. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2014, 117, 37–44. [Google Scholar] [CrossRef] [PubMed]
- Dindaroğlu, F.; Kutlu, P.; Duran, G.S.; Görgülü, S.; Aslan, E. Accuracy and reliability of 3D stereophotogrammetry: A comparison to direct anthropometry and 2D photogrammetry. Angle Orthod. 2016, 86, 487–494. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Denadai, R.; Chou, P.Y.; Seo, H.J.; Lonic, D.; Lin, H.H.; Pai, B.C.; Lo, L.J. Patient-and 3D morphometry-based nose outcomes after skeletofacial reconstruction. Sci. Rep. 2020, 10, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Chou, P.Y.; Hallac, R.R.; Ajiwe, T.; Xie, X.J.; Liao, Y.F.; Kane, A.A.; Park, Y.J. The role of Nasoalveolar molding: A 3D Prospective analysis. Sci. Rep. 2017, 7, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Adams, B.; Levy, R.; Rademaker, A.E.; Goldberg, L.H.; Alam, M. Frequency of use of suturing and repair techniques preferred by dermatologic surgeons. Dermatol. Surg. 2006, 32, 682–689. [Google Scholar] [CrossRef]
- Gupta, D.; Sharma, U.; Chauhan, S.; Sahu, S.A. Improved outcomes of scar revision with the use of polydioxanone suture in comparison to polyglactin 910: A randomized controlled trial. J. Plast. Reconstr. Aesthet. Surg. 2018, 71, 1159–1163. [Google Scholar] [CrossRef] [PubMed]
- Sakamoto, A.; Kiyokawa, K.; Rikimaru, H.; Watanabe, K.; Nishi, Y. An investigation of the fixation materials for cartilage frames in microtia. J. Plast. Reconstr. Aesthetic Surg. 2012, 65, 584–589. [Google Scholar] [CrossRef] [PubMed]
- Hennessey, D.B.; Carey, E.; Simms, C.K.; Hanly, A.; Winter, D.C. Torsion of monofilament and polyfilament sutures under tension decreases suture strength and increases risk of suture fracture. J. Mech. Behav. Biomed. Mater. 2012, 12, 168–173. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Nylon | PDS | p-Value | |
|---|---|---|---|
| Number of patients (n = 57) | 29 | 28 | |
| Mean age (years) | 25.9 ± 3.6 | 25.6 ± 5.9 | 0.844 |
| Male (M) | 11 | 10 | |
| Female (F) | 18 | 18 | |
| Sex ratio: M/F | 11/18 | 10/18 | |
| Le Fort I mean advancement 1 | 2.37 ± 1.13 | 2.38 ± 1.59 | 0.977 |
| Le Fort I impaction 1 | 0.52 ± 1.20 | 0.16 ± 0.69 | 0.207 |
| MMC CCW 2 | 24/29 | 21/28 | 0.371 |
| Pre-op Al-Al width | 37.65 ± 3.32 | 38.57 ± 2.42 | 0.238 |
| Pre-op Ac-Ac width | 33.68 ±3.25 | 33.98 ± 2.93 | 0.717 |
| T2-T1 | Nylon | PDS | p-Value |
|---|---|---|---|
| Alar width change (Al-Al) | 1.861 ± 1.66 | 1.115 ± 0.92 | 0.056 |
| Alar base change (Ac-Ac) | 1.999 ± 1.40 | 1.484 ± 0.97 | 0.112 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, P.-F.; Pascasio, D.C.; Kwon, S.H.; Chen, S.-H.; Chou, P.-Y.; Yao, C.-F.; Chen, Y.-A.; Lin, C.-H.; Chen, Y.-R. The Effect of Absorbable and Non-Absorbable Sutures on Nasal Width Following Cinch Sutures in Orthognathic Surgery. Symmetry 2021, 13, 1495. https://doi.org/10.3390/sym13081495
Wang P-F, Pascasio DC, Kwon SH, Chen S-H, Chou P-Y, Yao C-F, Chen Y-A, Lin C-H, Chen Y-R. The Effect of Absorbable and Non-Absorbable Sutures on Nasal Width Following Cinch Sutures in Orthognathic Surgery. Symmetry. 2021; 13(8):1495. https://doi.org/10.3390/sym13081495
Chicago/Turabian StyleWang, Po-Fang, Dax Carlo Pascasio, Soo Ha Kwon, Shih-Hsien Chen, Pang-Yun Chou, Chuan-Fong Yao, Ying-An Chen, Cheng-Hui Lin, and Yu-Ray Chen. 2021. "The Effect of Absorbable and Non-Absorbable Sutures on Nasal Width Following Cinch Sutures in Orthognathic Surgery" Symmetry 13, no. 8: 1495. https://doi.org/10.3390/sym13081495
APA StyleWang, P.-F., Pascasio, D. C., Kwon, S. H., Chen, S.-H., Chou, P.-Y., Yao, C.-F., Chen, Y.-A., Lin, C.-H., & Chen, Y.-R. (2021). The Effect of Absorbable and Non-Absorbable Sutures on Nasal Width Following Cinch Sutures in Orthognathic Surgery. Symmetry, 13(8), 1495. https://doi.org/10.3390/sym13081495