The Roles of Autoimmunity and Biotoxicosis in Sick Building Syndrome as a “Starting Point” for Irreversible Dampness and Mold Hypersensitivity Syndrome

{kind=link}
{kind=link}
Abstract
Highlights
- Sick Building Syndrome (SBS) is an imprecise terminology that may comprise a variety of environmental hazards;
- The term SBS does not reflect the effect of indoor air dampness microbiota that may have a devastating pathophysiological impact on human health;
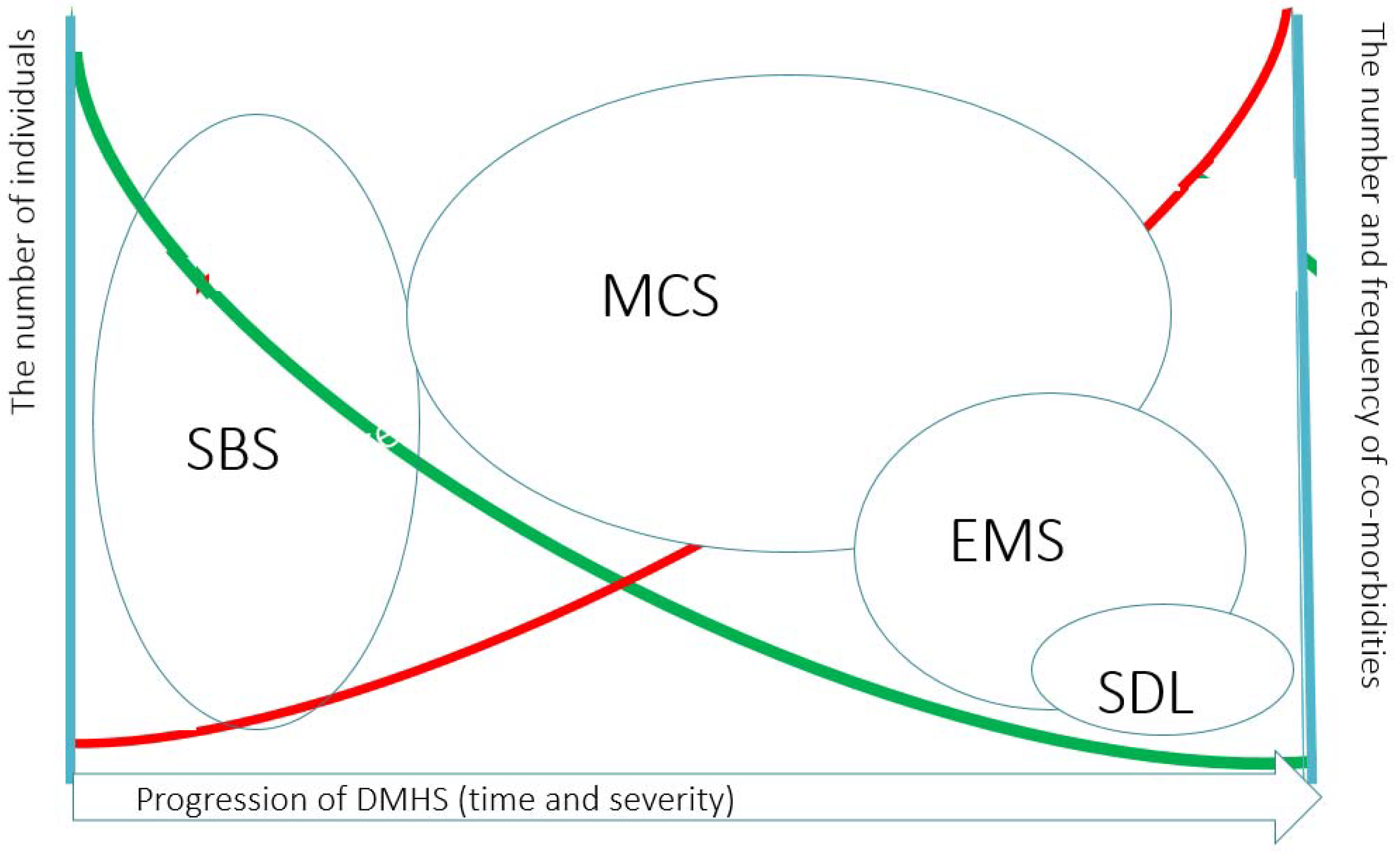
- When left untreated, reversible SBS may proceed into irreversible dampness and mold hypersensitivity syndrome (DMHS) that may affect many organs;
- Autoimmunity may be linked to postural tachycardia syndrome (POTS) and myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS), the conditions associated with DMHS;
- Chip-based affordable technology to detect autoantibodies in patients with symptoms of peripheral nervous system is of a big clinical demand;
- New techniques to study indoor air toxicity should be implemented;
- Psychologization of SBS/DMHS should be discouraged because this approach undermines patients’ trust towards the medical community.
1. What is a Sick Building Syndrome?
2. How Sick Building Syndrome is Related to the Dampness and Mold Hypersensitivity Syndrome (DMHS)?
3. Sick Building Syndrome/Dampness and Mold Hypersensitivity Syndrome are Related to other Chronic Illnesses and Autoimmunity in Particular
4. Postural Tachycardia Syndrome (POTS), Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS) and Autoantibodies: How They are Linked?
5. Is the Detection of Mold-Specific Antibodies Useful in Diagnostics?
6. Why the Problems Due to the Exposure to Moisture-Damaged Buildings Persist?
7. Conclusions
Funding
Acknowledgments
Conflicts of Interest
References and Notes
- Sundell, J. Reflections on the history of indoor air science, focusing on the last 50 years. Indoor Air 2017, 27, 708–724. [Google Scholar] [CrossRef] [PubMed]
- Skov, P. The sick building syndrome. Ann. N.Y. Acad. Sci. 1992, 641, 17–20. [Google Scholar] [CrossRef] [PubMed]
- Riesenberg, D.E.; Arehart-Treichel, J. Sick building” syndrome plagues workers, dwellers. JAMA 1986, 255, 3063. [Google Scholar] [CrossRef]
- Robertson, A. Sick building syndrome. Practitioner 1989, 233, 1250–1252. [Google Scholar]
- Lyles, W.B.; Greve, K.W.; Bauer, R.M.; Ware, M.R.; Schramke, C.J.; Crouch, J.; Hicks, A. Sick building syndrome. South Med. J. 1991, 84, 65–71. [Google Scholar] [CrossRef]
- Ishibashi, M.; Tonori, H.; Miki, T.; Miyajima, E.; Kudo, Y.; Tsunoda, M.; Sakabe, K.; Aizawa, Y. Classification of patients complaining of sick house syndrome and/or multiple chemical sensitivity. Tohoku J. Exp. Med. 2007, 211, 223–233. [Google Scholar] [CrossRef]
- Hicks, J.B. Tight building syndrome: When work makes you sick. Occup. Health Saf. 1984, 51–56. [Google Scholar]
- Welch, L.S. Severity of health effects associated with building-related illness. Environ. Health Perspect. 1991, 95, 67–69. [Google Scholar] [CrossRef] [PubMed]
- Welch, L.S.; Sokas, R. Development of multiple chemical sensitivity after an outbreak of sick-building syndrome. Toxicol. Ind. Health 1992, 8, 47–50. [Google Scholar] [CrossRef]
- Thörn, A.; Lewné, M.; Belin, L. Allergic alveolitis in a school environment. Scand. J. Work Environ. Health 1996, 22, 311–314. [Google Scholar] [CrossRef]
- Carey, J.; Hager, M.; King, P. Beware ‘sick-building syndrome’. The deadliest pollutants of all may be the ones you breathe at home or at work. Neewsweek 1985, 105, 58–60. [Google Scholar]
- Barsky, A.J.; Borus, J.F. Functional somatic syndromes. Ann. Intern. Med. 1999, 130, 910–921. [Google Scholar] [CrossRef] [PubMed]
- Bardana, E.J., Jr. Sick building syndrome—A wolf in sheep’s clothing. Ann. Allergy Asthma Immunol. 1997, 79, 283–293. [Google Scholar] [CrossRef]
- Straus, D.C. Molds, mycotoxins, and sick building syndrome. Toxicol. Ind. Health 2009, 25, 617–635. [Google Scholar] [CrossRef]
- Straus, D.C. The possible role of fungal contamination in sick building syndrome. Front. Biosci. (Elite Ed.) 2011, 3, 562–580. [Google Scholar] [CrossRef] [PubMed]
- Piecková, E. Adverse health effects of indoor moulds. Arh. Hig. Rada Toxicol. 2012, 63, 545–549. [Google Scholar] [CrossRef]
- Newman, A. Do microbes contribute to sick building syndrome? Environ. Sci. Technol. 1995, 29, 450A. [Google Scholar] [CrossRef]
- Williams, D.L. Overview of (1→3)-beta-D-glucan immunobiology. Mediat. Inflamm. 1997, 6, 247–250. [Google Scholar] [CrossRef]
- Valtonen, V. Clinical Diagnosis of the Dampness and Mold Hypersensitivity Syndrome: Review of the Literature and Suggested Diagnostic Criteria. Front. Immunol. 2017, 8, 951. [Google Scholar] [CrossRef]
- Chester, A.C.; Levine, P.H. Concurrent sick building syndrome and chronic fatigue syndrome: Epidemic neuromyasthenia revisited. Clin. Infect. Dis. 1994, 18 (Suppl. 1), S43–S48. [Google Scholar] [CrossRef]
- Tuuminen, T.; Antila, E. Multiple Chemical Sensitivity. The Disease Is Tangible–The Reactivity Is Physiological; Lambert Academic Publishing: Saarbrücken, Germany, 2018; ISBN 978-613-7-34824-6. [Google Scholar]
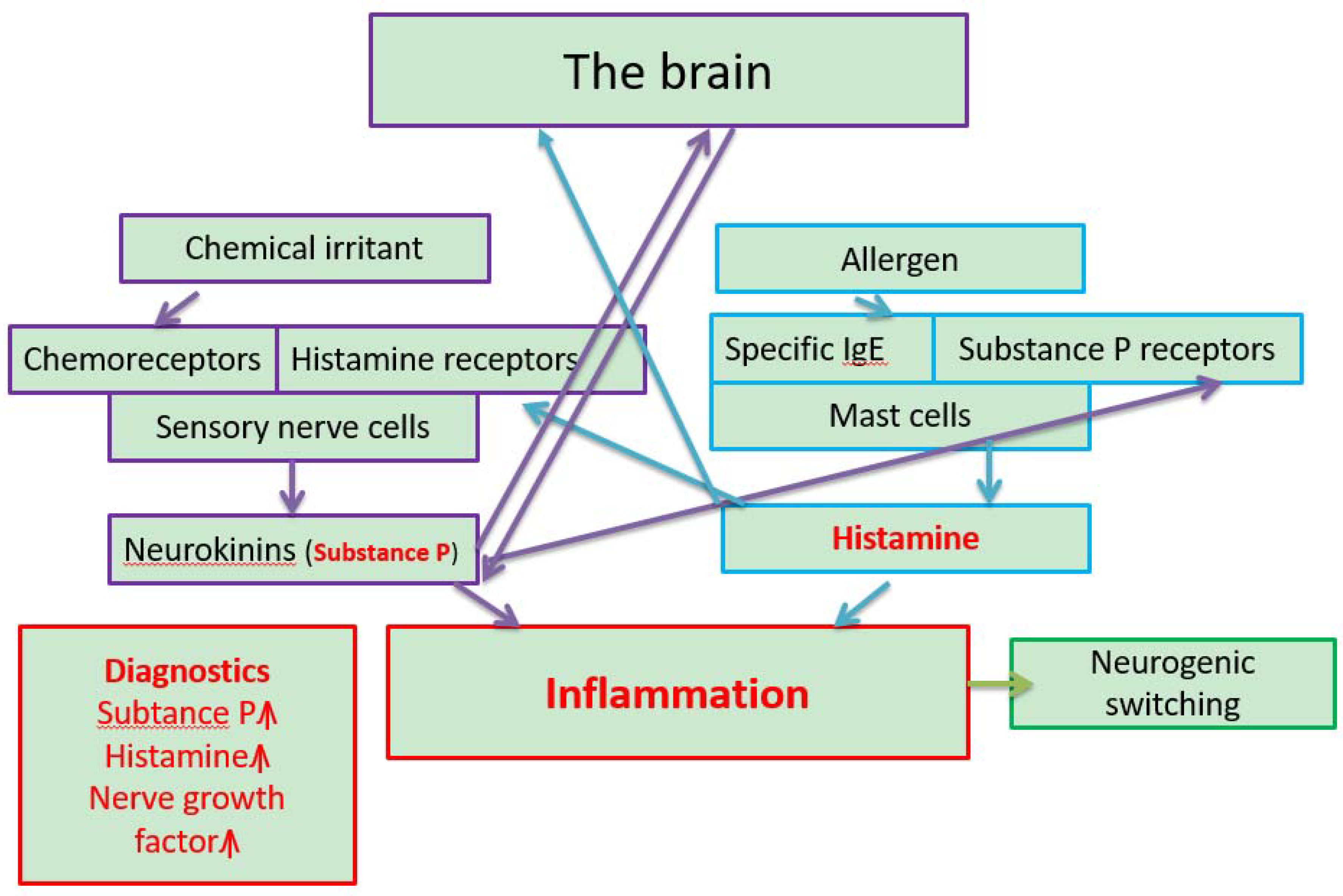
- Meggs, W.J. Neurogenic inflammation and sensitivity to environmental chemicals. Environ. Health Perspect. 1993, 101, 234–238. [Google Scholar] [CrossRef] [PubMed]
- Meggs, W.J. Neurogenic switching: A hypothesis for a mechanism for shifting the site of inflammation in allergy and chemical sensitivity. Environ. Heath Perspect. 1995, 103, 54–56. [Google Scholar] [CrossRef] [PubMed]
- Meggs, W.J. Hypothesis for induction and propagation of chemical sensitivity based on biopsy studies. Environ. Health Perspect. 1997, 105 (Suppl. 2), 473–478. [Google Scholar] [PubMed]
- Usuda, H.; Endo, T.; Shimouchi, A.; Saito, A.; Tominaga, M.; Yamashita, H.; Nagai, H.; Inagaki, N.; Tanaka, H. Transient receptor potential vanilloid 1-a polymodal nociceptive receptor-plays a crucial role in formaldehyde-induced skin inflammation in mice. J. Pharm. Sci. 2012, 118, 266–274. [Google Scholar] [CrossRef]
- Levine, T. Small fiber neuropathy: Disease classification beyond pain and burning. J. Cent. Nerv. Syst. Dis. 2018, 10. [Google Scholar] [CrossRef]
- Tuuminen, T.; Lohi, J. Immunological and toxicological effects of bad indoor air to cause Dampness and Mold Hypersensitivity Syndrome. Aims Allergy Immunol. 2018, 2, 190–203. [Google Scholar] [CrossRef]
- Tuuminen, T.; Lohi, J. Revising the criteria for occupational mold-related disease: Arguments, misconceptions and facts. EMJ Allergy Immunol. 2018, 1, 128–135. [Google Scholar]
- Tuuminen, T.; Lohi, J. Dampness and Mold Hypersensitivity Syndrome is a biotoxicosis that should be diagnosed promptly. Editorial. Adv. Clin. Toxicol. 2019, 4, 1–4. [Google Scholar]
- Tuuminen, T.; Vaali, K.; Valtonen, V. Dampness and Mold Hypersensitivity Syndrome as an Umbrella for Many Chronic Diseases—The Clinician’s Point of View. In Encyclopedia of Environmental Health; Nriagu, J., Ed.; Elsevier: Amsterdam, The Netherlands, 2019; Volume 2, pp. 1–9. ISBN 9780444639516. [Google Scholar] [CrossRef]
- Hyvönen, S.; Tuuminen, T.; Lohi, J. Case Report Occupants in Moisture-Damaged Buildings May be at Risk for Various Symptoms and Inflammatory Reactions: A Case Series Report and Literature Review. Arch. Clin. Med. Case Rep. 2019, 3, 692–701. [Google Scholar] [CrossRef]
- Kumar, S.N.; Telang, A.G.; Singh, K.P.; Jain, A.K.; Afroz, M.; Patil, R.D. Experimentally Induced Toxicity of Ochratoxin A and Endosulfan in Male Wistar Rats: A Hormonal Disorder. J. Anim. Vet. Adv. 2011, 10, 1750–1755. [Google Scholar] [CrossRef]
- Hassan, A.A.; Rashid, M.A.; Koratum, K.M. Effect of Aflatoxin B1, Zearalenone And Ochratoxin A On Some Hormones Related To Fertility In Male Rats. Life Sci. J. 2010, 7, 64–72. [Google Scholar]
- Reddy, K.E.; Young Jeong, J.; Lee, Y.; Lee, H.J.; Kim, M.S.; Kim, D.W.; Jung, H.J.; Choe, C.; Oh, Y.K.; Lee, S.D. Deoxynivalenol- and zearalenone-contaminated feeds alter gene expression profiles in the livers of piglets. Asian-Australas. J. Anim. Sci. 2018, 31, 595–606. [Google Scholar] [CrossRef] [PubMed]
- Somppi, T.L. Non-Thyroidal Illness Syndrome in Patients Exposed to Indoor Air Dampness Microbiota Treated Successfully with Triiodothyronine. Front. Immunol. 2017, 8, 919. [Google Scholar] [CrossRef] [PubMed]
- Dennis, D.; Robertson, D.; Curtis, L.; Black, J. Fungal exposure endocrinopathy in sinusitis with growth hormone deficiency: Dennis-Robertson syndrome. Toxicol. Ind. Health 2009, 25, 669–680. [Google Scholar] [CrossRef] [PubMed]
- Campbell, A.W.; Thrasher, J.D.; Madison, R.A.; Vojdani, A.; Gray, M.R.; Johnson, A. Neural autoantibodies and neurophysiologic abnormalities in patients exposed to molds in water-damaged buildings. Arch. Environ. Health 2003, 58, 464–474. [Google Scholar] [CrossRef] [PubMed]
- Gray, M.R.; Thrasher, J.D.; Crago, R.; Madison, R.A.; Arnold, L.; Campbell, A.W.; Vojdani, A. Mixed mold mycotoxicosis: Immunological changes in humans following exposure in water-damaged buildings. Arch. Environ. Health 2003, 58, 410–420. [Google Scholar] [CrossRef]
- Abou-Donia, M.B.; Lieberman, A.; Curtis, L. Neural autoantibodies in patients with neurological symptoms and histories of chemical/mold exposures. Toxicol. Ind. Health 2018, 34, 44–53. [Google Scholar] [CrossRef]
- Empting, L.D. Neurologic and neuropsychiatric syndrome features of mold and mycotoxin exposure. Toxicol. Ind. Health 2009, 25, 577–581. [Google Scholar] [CrossRef]
- Heuser, G.; Heuser, S.A. Functional brain MRI in patients complaining of electrohypersensitivity after long term exposure to electromagnetic fields. Rev. Environ. Health 2017, 32, 291–299. [Google Scholar]
- Vezzani, A.; Baram, T.Z. New roles for interleukin-1 Beta in the mechanisms of epilepsy. Epilepsy Curr. 2007, 7, 45–50. [Google Scholar] [CrossRef]
- Balosso, S.; Maroso, M.; Sanchez-Alavez, M.; Ravizza, T.; Frasca, A.; Bartfai, T.; Vezzani, A. A novel non-transcriptional pathway mediates the proconvulsive effects of interleukin-1beta. Brain 2008, 131, 3256–3265. [Google Scholar] [CrossRef] [PubMed]
- Sanchez-Alavez, M.; Tabarean, I.V.; Behrens, M.M.; Bartfai, T. Ceramide mediates the rapid phase of febrile response to IL-1beta. Proc. Natl. Acad. Sci. USA 2006, 103, 2904–2908. [Google Scholar] [CrossRef] [PubMed]
- Ryabkova, V.A.; Churilov, L.P.; Shoenfeld, Y. Neuroimmunology: What Role for Autoimmunity, Neuroinflammation, and Small Fiber Neuropathy in Fibromyalgia, Chronic Fatigue Syndrome, and Adverse Events after Human Papillomavirus Vaccination? Int. J. Mol. Sci. 2019, 20, 5164. [Google Scholar] [CrossRef]
- Tuuminen, T.; Jääskeläinen, T.; Vaali, K.; Polo, O. Dampness and mold hypersensitivity syndrome and vaccination as risk factors for chronic fatigue syndrome. Autoimmune Rev. 2019, 18, 107–108. [Google Scholar] [CrossRef]
- Farhad, K. Current Diagnosis and Treatment of Painful Small Fiber Neuropathy. Curr. Neurol. Neurosci. Rep. 2019, 19, 103. [Google Scholar] [CrossRef]
- Baronio, M.; Sadia, H.; Paolacci, S.; Prestamburgo, D.; Miotti, D.; Guardamagna, V.A.; Natalini, G.; Sullivan, S.G.B.; Bertelli, M. Molecular Aspects of Regional Pain Syndrome. Pain Res. Manag. 2020, 2020, 7697214. [Google Scholar] [CrossRef] [PubMed]
- Ruzieh, M.; Batizy, L.; Dasa, O.; Oostra, C.; Grubb, B. The role of autoantibodies in the syndromes of orthostatic intolerance: A systematic review. Scand. Cardiovasc. J. 2017, 51, 243–247. [Google Scholar] [CrossRef]
- Gunning, W.T.; Kvale, H.; Kramer, P.M.; Karabin, B.L.; Grubb, B.P. Postural Orthostatic Tachycardia Syndrome is associated with elevated G-Protein coupled receptor autoantibodies. J. Am. Health Assoc. 2019, 8, e013602. [Google Scholar] [CrossRef]
- Wirth, K.; Scheibenbogen, C. A Unifying Hypothesis of the Pathophysiology of Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS): Recognitions from the finding of autoantibodies against ß2-adrenergic receptors. Autoimm. Rev. 2020, 1, 102527. [Google Scholar] [CrossRef]
- Shoenfeld, Y.; Ryabkova, V.A.; Scheibenbogen, C.; Brinth, L.; Martinez-Lavin, M.; Ikeda, S.; Heidecke, H.; Watad, A.; Bragazzi, N.L.; Chapman, J.L.; et al. Complex syndromes of chronic pain, fatigue and cognitive impairment linked to autoimmune dysautonomia and small fiber neuropathy. Clin. Immunol. 2020, 214, 108384. [Google Scholar] [CrossRef]
- Fedorowski, A.; Li, H.; Yu, X.; Koelsch, K.A.; Harris, V.M.; Liles, C.; Murphy, T.A.; Quadri, S.M.S.; Scofield, R.H.; Sutton, R.; et al. Antiadrenergic autoimmunity in postural tachycardia syndrome. Eurospace 2017, 19, 1211–1219. [Google Scholar] [CrossRef] [PubMed]
- Neuman, R.; Danser, A.H.J. Autoantibodies against angiotensin and adrenergic receptors: More than a biomarker? Clin. Sci. (Lond) 2018, 132, 127–130. [Google Scholar] [CrossRef] [PubMed]
- Hyvönen, S.; Lohi, J.; Tuuminen, T. Moist and Mold Exposure is Associated with High Prevalence of Neurological Symptoms and MCS in a Finnish Hospital Workers Cohort. Saf. Health Work 2020. [Google Scholar] [CrossRef]
- Edmondson, D.A.; Barrios, C.S.; Brasel, T.L.; Straus, D.C.; Kurup, V.P.; Fink, J.N. Immune response among patients exposed to molds. Int. J. Mol. Sci. 2009, 10, 5471–5484. [Google Scholar] [CrossRef]
- Schütze, N.; Lehmann, I.; Bönisch, U.; Simon, J.C.; Polte, T. Exposure to mycotoxins increases the allergic immune response in a murine asthma model. Am. J. Respir. Crit. Care Med. 2010, 181, 1188–1199. [Google Scholar] [CrossRef] [PubMed]
- Bhan, U.; Newstead, M.J.; Zeng, X.; Ballinger, M.N.; Standiford, L.R.; Standiford, T.J. Stachybotrys chartarum-induced hypersensitivity pneumonitis is TLR9 dependent. Am. J. Pathol. 2011, 179, 2779–2787. [Google Scholar]
- Rasimus-Sahari, S.; Teplova, V.V.; Andersson, M.A.; Mikkola, R.; Kankkunen, P.; Matikainen, S.; Gahmberg, C.G.; Andersson, L.C.; Salkinoja-Salonen, M. The peptide toxin amylosin of Bacillus amyloliquefaciens from moisture-damaged buildings is immunotoxic, induces potassium efflux from mammalian cells, and has antimicrobial activity. Appl. Environ. Microbiol. 2015, 81, 2939–2949. [Google Scholar] [CrossRef]
- Van de Veerdonk, F.L.; Gresnigt, M.S.; Romani, L.; Netea, M.G.; Latgé, J.P. Aspergillus fumigatus morphology and dynamic host interactions. Nat. Rev. Microbiol. 2017, 15, 661–674. [Google Scholar] [CrossRef]
- Vincent, M.; Percier, P.; De Prins, S.; Huygen, K.; Potemberg, G.; Muraille, E.; Romano, M.; Michel, O.; Denis, O. Investigation of inflammatory and allergic responses to common mold species: Result from in vitro experiments, from a mouse model of asthma, and from a group of asthmatic patients. Indoor Air 2017, 27, 933–945. [Google Scholar] [CrossRef]
- Taskinen, T. Moisture and Mould Problem in School Children. Ph.D. Thesis, National Public Health Institute (KTL), Kuopio, Finland, 2001. [Google Scholar]
- Flamant-Hulin, M.; Anniesi-Maesano, I.; Caillaud, D. Relationships between molds and asthma suggesting non-allergic mechanisms. A rural-urban comparison. Pediatr. Allergy Immunol. 2013, 24, 345–352. [Google Scholar] [CrossRef]
- Weinmayr, G.; Gehring, U.; Genuneit, J.; Büchele, G.; Kleiner, A.; Siebers, R.; Wickens, K.; Crane, J.; Brunekreef, B.; Strachan, D.P.; et al. Dampness and moulds in relation to respiratory and allergic symptoms in children: A result from Phase two of the international study of asthma and allergies in childhood (ISAAC phase two). Clin. Exp. Allergy 2013, 43, 762–774. [Google Scholar] [CrossRef]
- Huttunen, K.; Wlodarczyk, A.J.; Tirkkonen, J.; Mikkonen, S.; Täubel, M.; Krop, E.; Jacobs, J.; Pekkanen, J.; Heederik, D.; Zock, J.P.; et al. Oxidative capacity and hemolytic activity of settled dust from moisture-damaged schools. Indoor Air 2019, 29, 299–307. [Google Scholar] [CrossRef] [PubMed]
- Gareis, M. Gottschalk. Stachybotrys spp. and the guttation phenomenon. Mycotoxin Res. 2014, 30, 151–159. [Google Scholar] [CrossRef] [PubMed]
- Castagnoli, E.; Marik, T.; Mikkola, R.; Kredics, L.; Andersson, M.A.; Salonen, H.; Kurnitski, J. Indoor Trichoderma strains emitting peptaibols in guttation droplets. J. Appl. Microbiol. 2018, 25, 1408–1422. [Google Scholar] [CrossRef] [PubMed]
- Mannerstöm, M.; Ahoniemi, J.; Aattela, E.; Heinonen, T. Solutoksisuuden testaus sisäilmasta kerätyistä huurrevesinäytteistä. Sisäilmaseminaari. (Testing of cytotoxicity from the indoor air condensed water samples Presentation on indoor air seminar). Poster 2019.
- Tuuminen, T.; Andersson, A.; Hyvönen, S.; Lohi, J.; Vaali, K. Indoor air nontoxicity should be proven with special techniques prior claiming that it may cause a variety of mental disorders. J. Hyg. Environ. Health 2020. [Google Scholar] [CrossRef]
- Salin, J.T.; Salkinoja-Salonen, M.; Salin, P.J.; Nelo, K.; Holma, T.; Ohtonen, P.; Syrjälä, H. Building related symptoms are linked to the in vitro toxicity of indoor dust and airborne microbial propagules in schools: A cross-sectional study. Environ. Res. 2017, 154, 234–239. [Google Scholar] [CrossRef] [PubMed]
- Hyvönen, S.; Poussa, T.L.; Tuuminen, T. High prevalence of neurological sequelae and multiple chemical sensitivity among occupants of a Finnish police station damaged by dampness microbiota. Arch. Environ. Occup. Health 2020. [Google Scholar] [CrossRef] [PubMed]


© 2020 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tuuminen, T. The Roles of Autoimmunity and Biotoxicosis in Sick Building Syndrome as a “Starting Point” for Irreversible Dampness and Mold Hypersensitivity Syndrome. Antibodies 2020, 9, 26. https://doi.org/10.3390/antib9020026
Tuuminen T. The Roles of Autoimmunity and Biotoxicosis in Sick Building Syndrome as a “Starting Point” for Irreversible Dampness and Mold Hypersensitivity Syndrome. Antibodies. 2020; 9(2):26. https://doi.org/10.3390/antib9020026
Chicago/Turabian StyleTuuminen, Tamara. 2020. "The Roles of Autoimmunity and Biotoxicosis in Sick Building Syndrome as a “Starting Point” for Irreversible Dampness and Mold Hypersensitivity Syndrome" Antibodies 9, no. 2: 26. https://doi.org/10.3390/antib9020026
APA StyleTuuminen, T. (2020). The Roles of Autoimmunity and Biotoxicosis in Sick Building Syndrome as a “Starting Point” for Irreversible Dampness and Mold Hypersensitivity Syndrome. Antibodies, 9(2), 26. https://doi.org/10.3390/antib9020026