
SARS-CoV-2 Infection Enhances Humoral Immune Response in Vaccinated Liver Transplant Recipients

 , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Sample Acquisition
2.2. Assessment of Humoral Immunity
2.3. Statistics
3. Results
3.1. Patient Characteristics
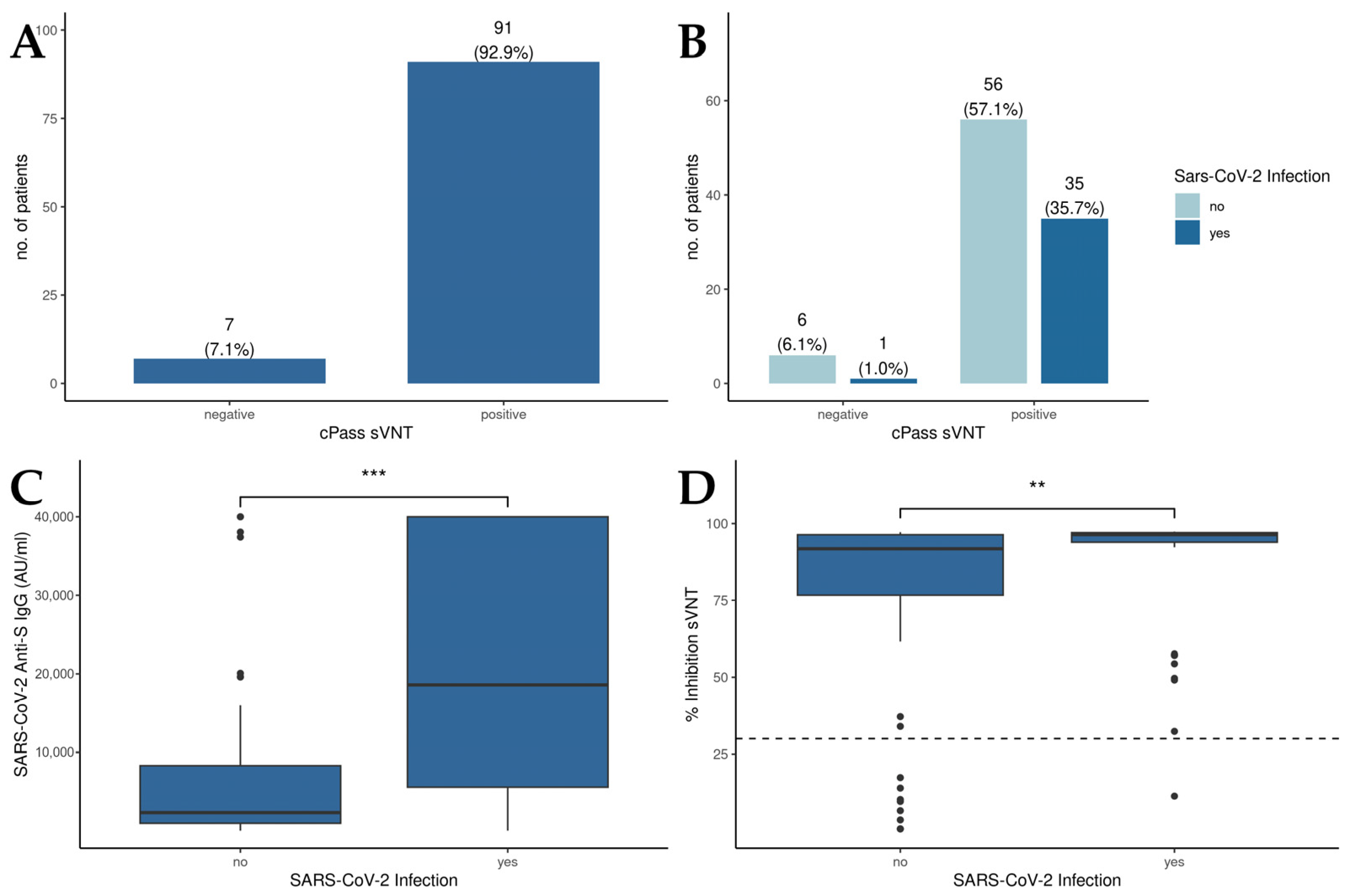
3.2. SARS-CoV-2 Infection Augments the Humoral Immune Response in Vaccinated Liver Transplant Recipients
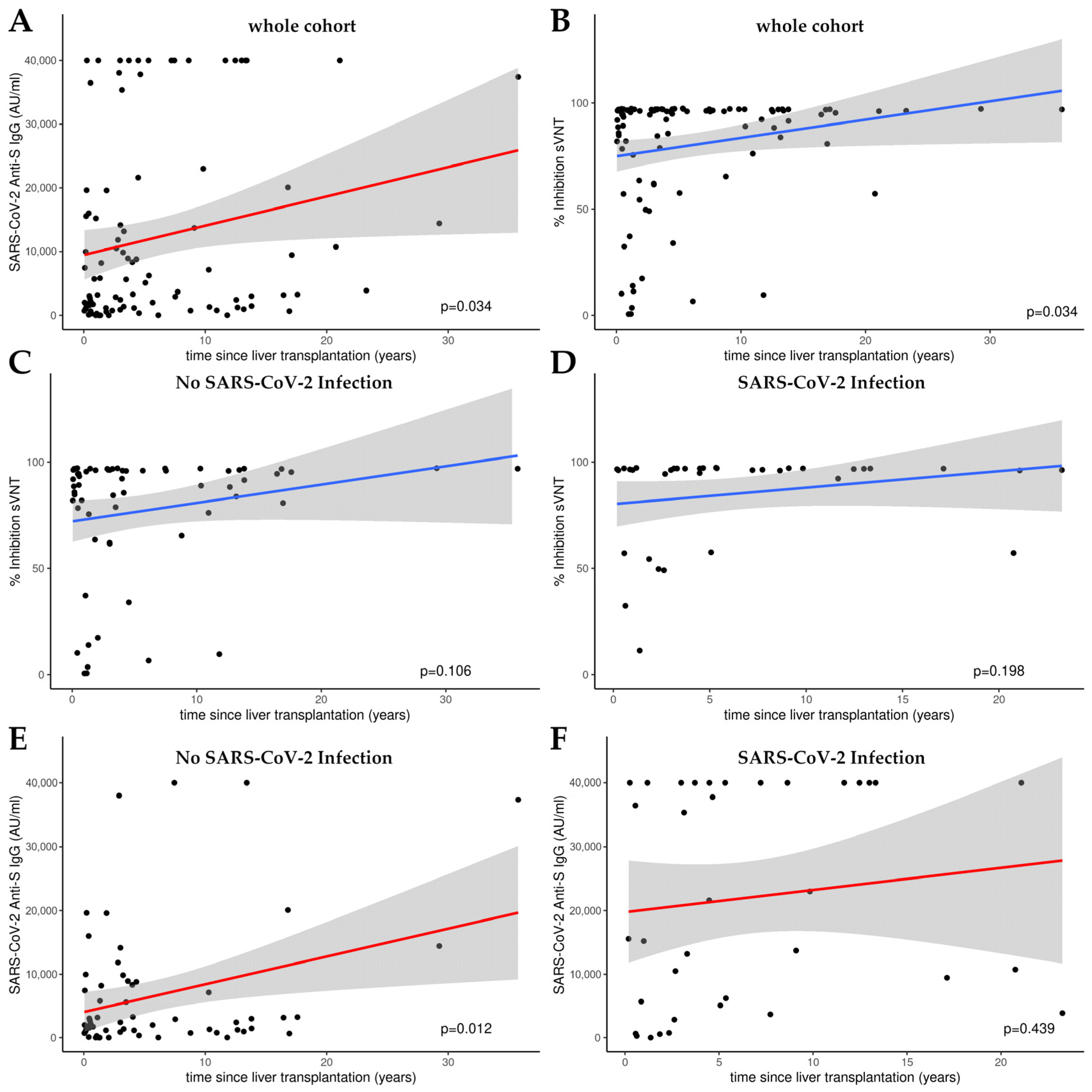
3.3. Time-Dependent Amplification of Humoral Immune Response in Liver Transplant Recipients: A Linear Model Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
List of Abbreviations
| Abbreviation | Definition |
| AU | arbitrary units |
| BAU | binding antibody units |
| CMIA | chemiluminescence microparticle assay |
| ELISA | enzyme-linked immunosorbent assay |
| hACE2 | human angiotensin-converting enzyme 2 |
| RBD | receptor-binding domain |
| sVNT | surrogate virus neutralization test |
References
- Wu, J.T.; Leung, K.; Leung, G.M. Nowcasting and forecasting the potential domestic and international spread of the 2019-nCoV outbreak originating in Wuhan, China: A modelling study. Lancet 2020, 395, 689–697. [Google Scholar] [CrossRef]
- Wu, Z.; McGoogan, J.M. Characteristics of and Important Lessons from the Coronavirus Disease 2019 (COVID-19) Outbreak in China: Summary of a Report of 72 314 Cases from the Chinese Center for Disease Control and Prevention. JAMA 2020, 323, 1239–1242. [Google Scholar] [CrossRef]
- Imam, A.; Abukhalaf, S.A.; Merhav, H.; Abu-Gazala, S.; Cohen-Arazi, O.; Pikarsky, A.J.; Safadi, R.; Khalaileh, A. Prognosis and Treatment of Liver Transplant Recipients in the COVID-19 Era: A Literature Review. Ann. Transplant. 2020, 25, e926196. [Google Scholar] [CrossRef]
- Thuluvath, P.J.; Robarts, P.; Chauhan, M. Analysis of antibody responses after COVID-19 vaccination in liver transplant recipients and those with chronic liver diseases. J. Hepatol. 2021, 75, 1434–1439. [Google Scholar] [CrossRef]
- Ruether, D.F.; Schaub, G.M.; Duengelhoef, P.M.; Haag, F.; Brehm, T.T.; Fathi, A.; Wehmeyer, M.; Jahnke-Triankowski, J.; Mayer, L.; Hoffmann, A.; et al. SARS-CoV2-specific Humoral and T-cell Immune Response After Second Vaccination in Liver Cirrhosis and Transplant Patients. Clin. Gastroenterol. Hepatol. 2022, 20, 162–172.e9. [Google Scholar] [CrossRef]
- Harberts, A.; Schaub, G.M.; Ruether, D.F.; Duengelhoef, P.M.; Brehm, T.T.; Karsten, H.; Fathi, A.; Jahnke-Triankowski, J.; Fischer, L.; Addo, M.M.; et al. Humoral and Cellular Immune Response After Third and Fourth SARS-CoV-2 mRNA Vaccination in Liver Transplant Recipients. Clin. Gastroenterol. Hepatol. 2022, 20, 2558–2566.e5. [Google Scholar] [CrossRef]
- Herrera, S.; Colmenero, J.; Pascal, M.; Escobedo, M.; Castel, M.A.; Sole-González, E.; Palou, E.; Egri, N.; Ruiz, P.; Mosquera, M.; et al. Cellular and humoral immune response after mRNA-1273 SARS-CoV-2 vaccine in liver and heart transplant recipients. Am. J. Transplant. 2021, 21, 3971–3979. [Google Scholar] [CrossRef]
- Hall, V.; Foulkes, S.; Insalata, F.; Kirwan, P.; Saei, A.; Atti, A.; Wellington, E.; Khawam, J.; Munro, K.; Cole, M.; et al. Protection against SARS-CoV-2 after COVID-19 Vaccination and Previous Infection. N. Engl. J. Med. 2022, 386, 1207–1220. [Google Scholar] [CrossRef]
- Bobrovitz, N.; Ware, H.; Ma, X.; Li, Z.; Hosseini, R.; Cao, C.; Selemon, A.; Whelan, M.; Premji, Z.; Issa, H.; et al. Protective effectiveness of previous SARS-CoV-2 infection and hybrid immunity against the omicron variant and severe disease: A systematic review and meta-regression. Lancet Infect. Dis. 2023, 23, 556–567. [Google Scholar] [CrossRef]
- Vollenberg, R.; Tepasse, P.-R.; Kühn, J.E.; Hennies, M.; Strauss, M.; Rennebaum, F.; Schomacher, T.; Boeckel, G.; Lorentzen, E.; Bokemeyer, A.; et al. Humoral Immune Response in IBD Patients Three and Six Months after Vaccination with the SARS-CoV-2 mRNA Vaccines mRNA-1273 and BNT162b2. Biomedicines 2022, 10, 171. [Google Scholar] [CrossRef]
- Vollenberg, R.; Tepasse, P.-R.; Lorentzen, E.; Nowacki, T.M. Impaired Humoral Immunity with Concomitant Preserved T Cell Reactivity in IBD Patients on Treatment with Infliximab 6 Month after Vaccination with the SARS-CoV-2 mRNA Vaccine BNT162b2: A Pilot Study. J. Pers. Med. 2022, 12, 694. [Google Scholar] [CrossRef] [PubMed]
- Schoefbaenker, M.; Neddermeyer, R.; Guenther, T.; Mueller, M.M.; Romberg, M.-L.; Classen, N.; Hennies, M.T.; Hrincius, E.R.; Ludwig, S.; Kuehn, J.E.; et al. Surrogate Virus Neutralisation Test Based on Nanoluciferase-Tagged Antigens to Quantify Inhibitory Antibodies against SARS-CoV-2 and Characterise Omicron-Specific Reactivity in a Vaccination Cohort. Vaccines 2023, 11, 1832. [Google Scholar] [CrossRef] [PubMed]
- Tan, C.W.; Chia, W.N.; Qin, X.; Liu, P.; Chen, M.I.-C.; Tiu, C.; Hu, Z.; Chen, V.C.-W.; Young, B.E.; Sia, W.R.; et al. A SARS-CoV-2 surrogate virus neutralization test based on antibody-mediated blockage of ACE2-spike protein-protein interaction. Nat. Biotechnol. 2020, 38, 1073–1078. [Google Scholar] [CrossRef] [PubMed]
- Taylor, S.C.; Hurst, B.; Charlton, C.L.; Bailey, A.; Kanji, J.N.; McCarthy, M.K.; Morrison, T.E.; Huey, L.; Annen, K.; DomBourian, M.G.; et al. A New SARS-CoV-2 Dual-Purpose Serology Test: Highly Accurate Infection Tracing and Neutralizing Antibody Response Detection. J. Clin. Microbiol. 2021, 59, e02438-20. [Google Scholar] [CrossRef] [PubMed]
- Fiolet, T.; Kherabi, Y.; MacDonald, C.-J.; Ghosn, J.; Peiffer-Smadja, N. Comparing COVID-19 vaccines for their characteristics, efficacy and effectiveness against SARS-CoV-2 and variants of concern: A narrative review. Clin. Microbiol. Infect. 2022, 28, 202–221. [Google Scholar] [CrossRef]
- Haas, E.J.; Angulo, F.J.; McLaughlin, J.M.; Anis, E.; Singer, S.R.; Khan, F.; Brooks, N.; Smaja, M.; Mircus, G.; Pan, K.; et al. Impact and effectiveness of mRNA BNT162b2 vaccine against SARS-CoV-2 infections and COVID-19 cases, hospitalisations, and deaths following a nationwide vaccination campaign in Israel: An observational study using national surveillance data. Lancet 2021, 397, 1819–1829. [Google Scholar] [CrossRef]
- Naaber, P.; Tserel, L.; Kangro, K.; Sepp, E.; Jürjenson, V.; Adamson, A.; Haljasmägi, L.; Rumm, A.P.; Maruste, R.; Kärner, J.; et al. Dynamics of antibody response to BNT162b2 vaccine after six months: A longitudinal prospective study. Lancet Reg. Health Eur. 2021, 10, 100208. [Google Scholar] [CrossRef]
- Andrews, N.; Stowe, J.; Kirsebom, F.; Toffa, S.; Sachdeva, R.; Gower, C.; Ramsay, M.; Lopez Bernal, J. Effectiveness of COVID-19 booster vaccines against COVID-19-related symptoms, hospitalization and death in England. Nat. Med. 2022, 28, 831–837. [Google Scholar] [CrossRef]
- Ayala-Borges, B.; Escobedo, M.; Egri, N.; Herrera, S.; Crespo, M.; Mirabet, S.; Arias-Cabrales, C.; Vilella, A.; Palou, E.; Mosquera, M.M.; et al. Impact of SARS-CoV-2 Infection on Humoral and Cellular Immunity in a Cohort of Vaccinated Solid Organ Transplant Recipients. Vaccines 2023, 11, 1845. [Google Scholar] [CrossRef]
- Kirchner, T.; Heinrich, S.; Bonifacius, A.; Engel, B.; Ruhl, L.; Pink, I.; Thomas, N.; Martens, J.; Hoeper, M.M.; Blasczyk, R.; et al. Reduced humoral but stable cellular SARS-CoV-2-specific immunity in liver transplant recipients in the first year after COVID-19. PLoS ONE 2022, 17, e0276929. [Google Scholar] [CrossRef]
- Caballero-Marcos, A.; Salcedo, M.; Alonso-Fernández, R.; Rodríguez-Perálvarez, M.; Olmedo, M.; Graus Morales, J.; Cuervas-Mons, V.; Cachero, A.; Loinaz-Segurola, C.; Iñarrairaegui, M.; et al. Changes in humoral immune response after SARS-CoV-2 infection in liver transplant recipients compared to immunocompetent patients. Am. J. Transplant. 2021, 21, 2876–2884. [Google Scholar] [CrossRef] [PubMed]
- van Thiel, D.H.; el-Ashmawy, L.; Love, K.; Gavaler, J.S.; Starzl, T.E. Response to hepatitis B vaccination by liver transplant candidates. Dig. Dis. Sci. 1992, 37, 1245–1249. [Google Scholar] [CrossRef] [PubMed]
- Loinaz, C.; de Juanes, J.R.; Gonzalez, E.M.; López, A.; Lumbreras, C.; Gómez, R.; Gonzalez-Pinto, I.; Jiménez, C.; Garcia, I.; Fuertes, A. Hepatitis B vaccination results in 140 liver transplant recipients. Hepatogastroenterology 1997, 44, 235–238. [Google Scholar] [PubMed]

{kind=link}
{kind=link}
| No SARS-CoV-2 Infection (n = 62) | SARS-CoV-2 Infection (n = 36) | p-Value | ||
|---|---|---|---|---|
| Patient characteristics | Age, years median (IQR) | 62.5 (17.8) | 60.5 (15.5) | 0.563 |
| Sex, male, total | 35 (35.7%) | 20 (20.4%) | 0.931 | |
| Months after transplantation, median (IQR) | 36.7 (111) | 54.6 (92) | 0.218 | |
| Retransplantation | 7 (7.1%) | 6 (6.1%) | 0.449 | |
| Pre-existing conditions | Diabetes mellitus | 14 (14.2%) | 8 (8.2%) | 0.140 |
| Kidney insufficiency | 24 (24.5%) | 10 (10.2%) | 0.273 | |
| Inflammatory disease | 16 (16.3%) | 12 (12.2%) | 0.427 | |
| Medication | Tacrolimus | 50 (51%) | 30 (30.6%) | 0.740 |
| Everolimus | 19 (19.4%) | 12 (12.2%) | 0.783 | |
| Mycophenolatmofetil | 36 (36.7%) | 18 (18.4%) | 0.439 | |
| Ciclosporin | 3 (3.1%) | 2 (2%) | 0.876 | |
| Prednisolon | 17 (17.3%) | 9 (9.2%) | 0.794 | |
| Sirolimus | 2 (2%) | 2 (2%) | 0.574 | |
| Immunosuppressive therapy | 0.957 1 | |||
| Immunosuppressive monotherapy | 11 (11.2%) | 6 (6.1%) | 0.892 | |
| Immunosuppressive dual therapy | 36 (36.7%) | 22 (22.4%) | 0.767 | |
| Immunosuppressive triple therapy | 15 (15.3%) | 8 (8.2%) | 0.824 | |
| Indication for liver transplantation | 0.993 1 | |||
| Hepatocellular carcinoma | 7 (7.1%) | 10 (10.2%) | 0.676 | |
| Primary sclerosing cholangitis | 6 (6.1%) | 6 (6.1%) | 1 | |
| Secondary sclerosing cholangitis | 1 (1%) | 2 (2%) | 0.901 | |
| Autoimmune hepatitis | 2 (2%) | 4 (4.1%) | 0.858 | |
| Ethanol related | 4 (4.1%) | 9 (9.2%) | 0.632 | |
| Drug induced liver injury | 2 (2%) | 3 (3.1%) | 0.876 | |
| Viral hepatitis | 3 (3.1%) | 4 (4.1%) | 0.727 | |
| Budd Chiari | 1 (1%) | 1 (1%) | 1 | |
| Non-alcoholic steatohepatitis | 1 (1%) | 4 (4.1%) | 0.426 | |
| Cryptogene | 6 (6.1%) | 10 (10.2%) | 0.945 | |
| Other | 3 (3.1%) | 9 (9.2%) | 0.544 | |
| No SARS-CoV-2 Infection (n = 62) | SARS-CoV-2 Infection (n = 36) | p-Value | ||
|---|---|---|---|---|
| Manufacturer of first vaccine | 0.727 | |||
| mRNA (BNT162b2 and mRNA-1273) | 58 (93.5%) | 33 (91.7%) | n.d. | |
| vector-based (ChAdOx1-S and Ad26.COV2.S) | 4 (6.5%) | 3 (8.3%) | n.d. | |
| no vaccination | 0 | 0 | n.d. | |
| Manufacturer of second vaccine | 0.070 | |||
| mRNA (BNT162b2 and mRNA-1273) | 62 (100%) | 33 (91.7%) | 0.021 | |
| vector-based (ChAdOx1-S and Ad26.COV2.S) | 0 (0%) | 2 (5.6%) | 0.061 | |
| no vaccination | 0 (0%) | 1 (2.8%) | 0.187 | |
| Manufacturer of third vaccine | 0.049 | |||
| mRNA (BNT162b2 and mRNA-1273) | 58 (93.5%) | 29 (80.6%) | n.d. | |
| vector-based (ChAdOx1-S and Ad26.COV2.S) | 0 | 0 | n.d. | |
| no vaccination | 4 (6.5%) | 7 (19.4%) | n.d. | |
| Manufacturer of fourth vaccine | 0.040 | |||
| mRNA (BNT162b2 and mRNA-1273) | 34 (54.8%) | 12 (33.3%) | n.d. | |
| vector-based (ChAdOx1-S and Ad26.COV2.S) | 0 | 0 | n.d. | |
| no vaccination | 28 (45.2%) | 24 (66.7%) | n.d. | |
| Manufacturer of fifth vaccine | 0.901 | |||
| mRNA (BNT162b2 and mRNA-1273) | 2 (3.2%) | 1 (2.8%) | n.d. | |
| vector-based (ChAdOx1-S and Ad26.COV2.S) | 0 | 0 | n.d. | |
| no vaccination | 60 (96.8%) | 35 (97.2%) | n.d. | |
| Vaccination History | vaccinations | 0.101 | ||
| 1 vaccination | 0 (0%) | 1 (2.8%) | 0.187 | |
| 2 vaccinations | 3 (4.8%) | 6 (16.7%) | 0.051 | |
| 3 vaccinations | 25 (40.3%) | 17 (47.2%) | 0.506 | |
| 4 vaccinations | 32 (51.6%) | 11 (30.6%) | 0.043 | |
| 5 vaccinations | 2 (3.2%) | 1 (2.8%) | 0.901 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Adiprasito, J.B.; Nowacki, T.; Vollenberg, R.; Meier, J.A.; Rennebaum, F.; Schomacher, T.; Trebicka, J.; Fischer, J.; Lorentzen, E.U.; Tepasse, P.-R. SARS-CoV-2 Infection Enhances Humoral Immune Response in Vaccinated Liver Transplant Recipients. Antibodies 2024, 13, 78. https://doi.org/10.3390/antib13030078
Adiprasito JB, Nowacki T, Vollenberg R, Meier JA, Rennebaum F, Schomacher T, Trebicka J, Fischer J, Lorentzen EU, Tepasse P-R. SARS-CoV-2 Infection Enhances Humoral Immune Response in Vaccinated Liver Transplant Recipients. Antibodies. 2024; 13(3):78. https://doi.org/10.3390/antib13030078
Chicago/Turabian StyleAdiprasito, Jan Basri, Tobias Nowacki, Richard Vollenberg, Jörn Arne Meier, Florian Rennebaum, Tina Schomacher, Jonel Trebicka, Julia Fischer, Eva U. Lorentzen, and Phil-Robin Tepasse. 2024. "SARS-CoV-2 Infection Enhances Humoral Immune Response in Vaccinated Liver Transplant Recipients" Antibodies 13, no. 3: 78. https://doi.org/10.3390/antib13030078
APA StyleAdiprasito, J. B., Nowacki, T., Vollenberg, R., Meier, J. A., Rennebaum, F., Schomacher, T., Trebicka, J., Fischer, J., Lorentzen, E. U., & Tepasse, P.-R. (2024). SARS-CoV-2 Infection Enhances Humoral Immune Response in Vaccinated Liver Transplant Recipients. Antibodies, 13(3), 78. https://doi.org/10.3390/antib13030078