

Case Series: Efficacy of Polyclonal Intravenous Immunoglobulin for Refractory Clostridioides difficile Infection

 , and
, and
Abstract
1. Introduction
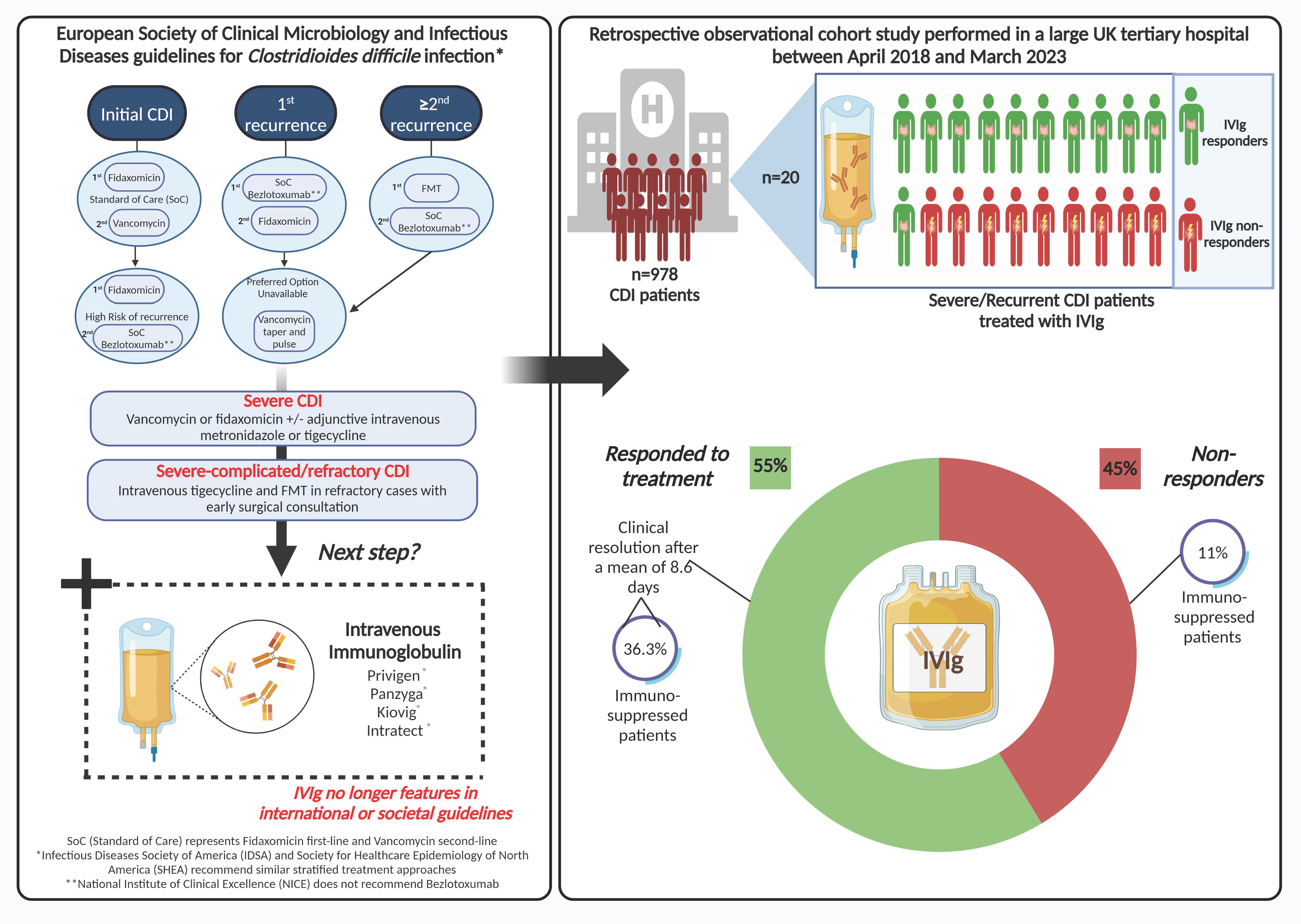
2. Materials and Methods
2.1. Data Source and Study Population
2.2. Exposure and Study Outcomes
2.3. Statistical Analysis
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bishop, E.J.; Tiruvoipati, R. Management of Clostridioides difficile infection in adults and challenges in clinical practice: Review and comparison of current IDSA/SHEA, ESCMID and ASID guidelines. J. Antimicrob. Chemother. 2022, 78, 21–30. [Google Scholar] [CrossRef] [PubMed]
- Balsells, E.; Shi, T.; Leese, C.; Lyell, I.; Burrows, J.; Wiuff, C.; Campbell, H.; Kyaw, M.H.; Nair, H. Global burden of Clostridium difficile infections: A systematic review and meta-analysis. J. Glob. Health 2019, 9, 010407. [Google Scholar] [CrossRef]
- Liu, C.; Monaghan, T.; Yadegar, A.; Louie, T.; Kao, D. Insights into the Evolving Epidemiology of Clostridioides difficile Infection and Treatment: A Global Perspective. Antibiotics 2023, 12, 1141. [Google Scholar] [CrossRef]
- Freeman, J.; Bauer, M.P.; Baines, S.D.; Corver, J.; Fawley, W.N.; Goorhuis, B.; Kuijper, E.J.; Wilcox, M.H. The changing epidemiology of Clostridium difficile infections. Clin. Microbiol. Rev. 2010, 23, 529–549. [Google Scholar] [CrossRef] [PubMed]
- Martin, J.S.; Monaghan, T.M.; Wilcox, M.H. Clostridium difficile infection: Epidemiology, diagnosis and understanding transmission. Nat. Rev. Gastroenterol. Hepatol. 2016, 13, 206–216. [Google Scholar] [CrossRef] [PubMed]
- van Prehn, J.; Reigadas, E.; Vogelzang, E.H.; Bouza, E.; Hristea, A.; Guery, B.; Krutova, M.; Norén, T.; Allerberger, F.; Coia, J.E.; et al. European Society of Clinical Microbiology and Infectious Diseases: 2021 update on the treatment guidance document for Clostridioides difficile infection in adults. Clin. Microbiol. Infect. 2021, 27, S1–S21. [Google Scholar] [CrossRef]
- Olsen, M.; Yan, Y.; Reske, K.; Zilberberg, M.; Dubberke, E. Recurrent Clostridium difficile infection is associated with increased mortality. Clin. Microbiol. Infect. 2015, 21, 164–170. [Google Scholar] [CrossRef]
- Lurienne, L.; Bandinelli, P.-A.; Galvain, T.; Coursel, C.-A.; Oneto, C.; Feuerstadt, P. Perception of quality of life in people experiencing or having experienced a Clostridioides difficile infection: A US population survey. J. Patient-Rep. Outcomes 2020, 4, 14. [Google Scholar] [CrossRef]
- Tresman, R.; Goldenberg, S.D. Healthcare resource use and attributable cost of Clostridium difficile infection: A micro-costing analysis comparing first and recurrent episodes. J. Antimicrob. Chemother. 2018, 73, 2851–2855. [Google Scholar] [CrossRef] [PubMed]
- Johnson, S.; Lavergne, V.; Skinner, A.M.; Gonzales-Luna, A.J.; Garey, K.W.; Kelly, C.P.; Wilcox, M.H. Clinical Practice Guideline by the Infectious Diseases Society of America (IDSA) and Society for Healthcare Epidemiology of America (SHEA): 2021 Focused Update Guidelines on Management of Clostridioides difficile Infection in Adults. Clin. Infect. Dis. 2021, 73, e1029–e1044. [Google Scholar] [CrossRef]
- National Institute for Health and Care Excellence. Clostridioides difficile Infection: Antimicrobial Prescribing NICE Guidance. 2021. Available online: https://www.nice.org.uk/guidance/ng199/chapter/Recommendations (accessed on 5 March 2024).
- Swart, N.; Sinha, A.M.; Bentley, A.; Smethurst, H.; Spencer, G.; Ceder, S.; Wilcox, M.H. A cost-utility analysis of two Clostridioides difficile infection guideline treatment pathways. Clin. Microbiol. Infect. 2023, 29, 1291–1297. [Google Scholar] [CrossRef]
- Abougergi, M.S.; Kwon, J.H. Intravenous immunoglobulin for the treatment of Clostridium difficile infection: A review. Dig. Dis. Sci. 2011, 56, 19–26. [Google Scholar] [CrossRef] [PubMed]
- Vani, J.; Elluru, S.; Negi, V.S.; Lacroix-Desmazes, S.; Kazatchkine, M.D.; Bayry, J.; Kaveri, S.V. Role of natural antibodies in immune homeostasis: IVIg perspective. Autoimmun. Rev. 2008, 7, 440–444. [Google Scholar] [CrossRef] [PubMed]
- Negm, O.H.; MacKenzie, B.; Hamed, M.R.; Ahmad, O.A.J.; Shone, C.C.; Humphreys, D.P.; Ravi Acharya, K.; Loscher, C.E.; Marszalowska, I.; Lynch, M.; et al. Protective antibodies against Clostridium difficile are present in intravenous immunoglobulin and are retained in humans following its administration. Clin. Exp. Immunol. 2017, 188, 437–443. [Google Scholar] [CrossRef]
- Bayry, J.; Misra, N.; Latry, V.; Prost, F.; Delignat, S.; Lacroix-Desmazes, S.; Kazatchkine, M.D.; Kaveri, S.V. Mechanisms of action of intravenous immunoglobulin in autoimmune and inflammatory diseases. Transfus. Clin. Biol. 2003, 10, 165–169. [Google Scholar] [CrossRef]
- Nibbering, B.; Gerding, D.N.; Kuijper, E.J.; Zwittink, R.D.; Smits, W.K. Host Immune Responses to Clostridioides difficile: Toxins and Beyond. Front. Microbiol. 2021, 12, 804949. [Google Scholar] [CrossRef] [PubMed]
- Hassoun, A.; Ibrahim, F. Use of intravenous immunoglobulin for the treatment of severe Clostridium difficile colitis. Am. J. Geriatr. Pharmacother. 2007, 5, 48–51. [Google Scholar] [CrossRef]
- Murphy, C.; Vernon, M.; Cullen, M. Intravenous immunoglobulin for resistant Clostridium difficile infection. Age Ageing 2005, 35, 85–86. [Google Scholar] [CrossRef]
- Coffman, K.; Chen, X.J.; Okamura, C.; Louie, E. IVIG—A cure to severe refractory NAP-1 Clostridium difficile colitis? A case of successful treatment of severe infection, which failed standard therapy including fecal microbiota transplants and fidaxomicin. IDCases 2017, 8, 27–28. [Google Scholar] [CrossRef]
- O’Horo, J.; Safdar, N. The role of immunoglobulin for the treatment of Clostridium difficile infection: A systematic review. Int. J. Infect. Dis. 2009, 13, 663–667. [Google Scholar] [CrossRef]
- Leung, D.Y.; Kelly, C.P.; Boguniewicz, M.; Pothoulakis, C.; LaMont, J.T.; Flores, A. Treatment with intravenously administered gamma globulin of chronic relapsing colitis induced by Clostridium difficile toxin. J. Pediatr. 1991, 118, 633–637. [Google Scholar] [CrossRef]
- Wilcox, M.H. Descriptive study of intravenous immunoglobulin for the treatment of recurrent Clostridium difficile diarrhoea. J. Antimicrob. Chemother. 2004, 53, 882–884. [Google Scholar] [CrossRef] [PubMed]
- Hassett, J.; Meyers, S.; Mcfarland, L.V.; Mulligan, M.E. Recurrent Clostridium difficile infection in a patient with selective IgG1 deficiency treated with intravenous immune globulin and Saccharomyces boulardii. Clin. Infect. Dis. 1995, 20 (Suppl. S2), S266–S268. [Google Scholar] [CrossRef] [PubMed]
- Beales, I.L. Intravenous immunoglobulin for recurrent Clostridium difficile diarrhoea. Gut 2002, 51, 456. [Google Scholar] [CrossRef]
- McPherson, S.; Rees, C.J.; Ellis, R.; Soo, S.; Panter, S.J. Intravenous immunoglobulin for the treatment of severe, refractory, and recurrent Clostridium difficile diarrhea. Dis. Colon. Rectum 2006, 49, 640–645. [Google Scholar] [CrossRef]
- Abougergi, M.S.; Broor, A.; Cui, W.; Jaar, B.G. Intravenous immunoglobulin for the treatment of severe Clostridium difficile colitis: An observational study and review of the literature. J. Hosp. Med. 2010, 5, E1–E9. [Google Scholar] [CrossRef]
- Public Health England. Clostridium difficile Infection Surveillance Updates 2017. Available online: https://assets.publishing.service.gov.uk/media/5a81bf29e5274a2e87dbf429/CDI_mandatory_surveillance_update_April_2017.pdf (accessed on 5 March 2024).
- Centers for Disease Control and Prevention. Altered Immunocompetence: General Best Practice Guidelines for Immunization. Available online: https://www.cdc.gov/vaccines/hcp/acip-recs/general-recs/immunocompetence.pdf (accessed on 5 March 2024).
- Fettucciari, K.; Fruganti, A.; Marchegiani, A.; Brancorsini, S.; Marconi, P.; Bassotti, G. Proinflammatory Cytokines: Possible Accomplices for the Systemic Effects of Clostridioides difficile Toxin B. J. Inflamm. Res. 2021, 14, 57–62. [Google Scholar] [CrossRef]
- Solomon, K.; Martin, A.J.; O’Donoghue, C.; Chen, X.; Fenelon, L.; Fanning, S.; Kelly, C.P.; Kyne, L. Mortality in patients with Clostridium difficile infection correlates with host pro-inflammatory and humoral immune responses. J. Med. Microbiol. 2013, 62, 1453–1460. [Google Scholar] [CrossRef]
- Yu, H.; Chen, K.; Sun, Y.; Carter, M.; Garey, K.W.; Savidge, T.C.; Devaraj, S.; Tessier, M.E.; von Rosenvinge, E.C.; Kelly, C.P.; et al. Cytokines Are Markers of the Clostridium difficile-Induced Inflammatory Response and Predict Disease Severity. Clin. Vaccine Immunol. 2017, 24, e00037-17. [Google Scholar] [CrossRef]
- Czepiel, J.; Biesiada, G.; Brzozowski, T.; Ptak-Belowska, A.; Perucki, W.; Birczynska, M.; Jurczyszyn, A.; Strzalka, M.; Targosz, A.; Garlicki, A. The role of local and systemic cytokines in patients infected with Clostridium difficile. J. Physiol. Pharmacol. 2014, 65, 695–703. [Google Scholar] [PubMed]
- Arumugham, V.B.; Rayi, A. Intravenous Immunoglobulin (IVIG); Updated 2023 Jul 3; StatPearls. Available online: https://www.ncbi.nlm.nih.gov/books/NBK554446/ (accessed on 15 March 2024).
- Juang, P.; Skledar, S.J.; Zgheib, N.K.; Paterson, D.L.; Vergis, E.N.; Shannon, W.D.; Ansani, N.T.; Branch, R.A. Clinical outcomes of intravenous immune globulin in severe Clostridium difficile-associated diarrhea. Am. J. Infect. Control 2007, 35, 131–137. [Google Scholar] [CrossRef] [PubMed]
- Herbert, R.; Hatcher, J.; Jauneikaite, E.; Gharbi, M.; d’Arc, S.; Obaray, N.; Rickards, T.; Rebec, M.; Blandy, O.; Hope, R.; et al. Two-year analysis of Clostridium difficile ribotypes associated with increased severity. J. Hosp. Infect. 2019, 103, 388–394. [Google Scholar] [CrossRef]
- Walker, A.S.; Eyre, D.W.; Wyllie, D.H.; Dingle, K.E.; Griffiths, D.; Shine, B.; Oakley, S.; O’Connor, L.; Finney, J.; Vaughan, A.; et al. Relationship between bacterial strain type, host biomarkers, and mortality in Clostridium difficile infection. Clin. Infect. Dis. 2013, 56, 1589–1600. [Google Scholar] [CrossRef]
- Thabit, A.K.; Nicolau, D.P. An exploratory study to evaluate Clostridium difficile polymerase chain reaction ribotypes and infection outcomes. Infect. Drug Resist. 2016, 9, 143–148. [Google Scholar] [CrossRef]
- Negm, O.H.; Hamed, M.; Monaghan, T.M. A Protein Microarray Assay for Serological Determination of Antigen-specific Antibody Responses Following Clostridium difficile Infection. J. Vis. Exp. 2018, 136, e57399. [Google Scholar] [CrossRef]
- Negm, O.H.; Hamed, M.R.; Dilnot, E.M.; Shone, C.C.; Marszalowska, I.; Lynch, M.; Loscher, C.E.; Edwards, L.J.; Tighe, P.J.; Wilcox, M.H.; et al. Profiling Humoral Immune Responses to Clostridium difficile-Specific Antigens by Protein Microarray Analysis. Clin. Vaccine Immunol. 2015, 22, 1033–1039. [Google Scholar] [CrossRef] [PubMed]
- Zhang, A.; Stacey, H.D.; D’Agostino, M.R.; Tugg, Y.; Marzok, A.; Miller, M.S. Beyond neutralization: Fc-dependent antibody effector functions in SARS-CoV-2 infection. Nat. Rev. Immunol. 2023, 23, 381–396. [Google Scholar] [CrossRef] [PubMed]
- Cobb, B.A. The history of IgG glycosylation and where we are now. Glycobiology 2020, 30, 202–213. [Google Scholar] [CrossRef]
- Karbiener, M.; Farcet, M.R.; Schwaiger, J.; Powers, N.; Lenart, J.; Stewart, J.M.; Tallman, H.; Kreil, T.R. Highly Potent SARS-CoV-2 Neutralization by Intravenous Immunoglobulins manufactured from Post-COVID-19 and COVID-19-Vaccinated Plasma Donations. J. Infect. Dis. 2021, 224, 1707–1711. [Google Scholar] [CrossRef]
- Zahra, F.T.; Bellusci, L.; Grubbs, G.; Golding, H.; Khurana, S. Neutralisation of circulating SARS-CoV-2 delta and omicron variants by convalescent plasma and SARS-CoV-2 hyperimmune intravenous human immunoglobulins for treatment of COVID-19. Ann. Rheum. Dis. 2022, 81, 1044–1045. [Google Scholar] [CrossRef]
- Huygens, S.; Hofsink, Q.; Nijhof, I.S.; Goorhuis, A.; Kater, A.P.; Te Boekhorst, P.A.W.; Swaneveld, F.; Novotný, V.M.J.; Bogers, S.; Welkers, M.R.A.; et al. Hyperimmune Globulin for Severely Immunocompromised Patients Hospitalized with Coronavirus Disease 2019: A Randomized, Controlled Trial. J. Infect. Dis. 2023, 227, 206–210. [Google Scholar] [CrossRef] [PubMed]
- Rahmel, T.; Kraft, F.; Haberl, H.; Achtzehn, U.; Brandenburger, T.; Neb, H.; Jarczak, D.; Dietrich, M.; Magunia, H.; Zimmer, F.; et al. Intravenous IgM-enriched immunoglobulins in critical COVID-19: A multicentre propensity-weighted cohort study. Crit. Care 2022, 26, 204. [Google Scholar] [CrossRef] [PubMed]
- Tascini, C.; Cotrufo, M.; Sozio, E.; Fanin, M.; Dellai, F.; Zanus Forte, A.; Cesselli, D.; Stefanis, P.; Ripoli, A.; Sbrana, F.; et al. Potential role of IgM-enriched immunoglobulin as adjuvant treatment in severe SARS-CoV-2 infection. Minerva Anestesiol. 2023, 89, 884–894. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Whole Cohort (n = 20) | IVIg Responders (n = 11) | p Value | |
|---|---|---|---|
| Age (years), mean (SD) | 65.8 (24.2) | 68.9 (20.0) | 0.55 |
| BMI (kg/m2), mean (SD) | 24.3 (5.9) | 25.4 (5.1) | 0.39 |
| Female gender, n (%) | 11 (55.0%) | 5 (45.4%) | 0.65 |
| Ethnicity: White British, n (%) | 20 (100%) | 11 (100%) | |
| Own home, n (%) | 20 (100%) | 11 (100%) | |
| Indication: recurrent or relapsing, n (%) | 4 (20.0%) | 3 (27.3%) | 0.37 |
| Indication: Severe, n (%) | 16 (80.0%) | 8 (72.7%) | 0.37 |
| Total IVIg dose (g), mean (SD) | 33.2 (15.5) | 33.2 (15.5) | 0.63 |
| Days to disease resolution, mean (SD) | 8.6 (10.7) | ||
| Charlson Comorbidity Index, mean (SD) | 5.9 (2.9) | 6.3 (3.2) | 0.52 |
| Immunosuppression, n (%) | 5 (25.0%) | 4 (36.3%) | 0.15 |
| Number of other drugs on admission, mean (SD) | 7.4 (4.2) | 7.1 (4.6) | 0.78 |
| PPI on admission, n (%) | 7 (35.0%) | 4 (20.0%) | 0.88 |
| Hospital-onset CDI, n (%) | 12 (60.0%) | 7 (63.6%) | 0.73 |
| Community-onset CDI, n (%) | 8 (40.0%) | 4 (36.4%) | 0.71 |
| Recent antibiotics, n (%) | 13 (65.0%) | 8 (72.7%) | 0.73 |
| Peak WCC (×109/L), mean (SD) | 27.8 (15.8) | 27.4 (15.4) | 0.92 |
| Peak CRP (mg/L), mean (SD) | 267.8 (101.5) | 265.8 (89.8) | 0.93 |
| Lowest albumin (g/L), mean (SD) | 18.2 (4.0) | 18.4 (3.0) | 0.85 |
| Radiological evidence of CDI, n (%) | |||
| Toxic megacolon | 1 (5.0%) | ||
| Pancolitis | 12 (60.0%) | ||
| Localized colitis | 5 (25.0%) | ||
| Chronic colitis | 1 (5.0%) | ||
| Normal | 1 (5.0%) | ||
| Days from diagnosis of CDI to IVIg request, mean (SD) | 5.5 (3.3) | 6.36 (4.0) | 0.19 |
| Days from onset of symptoms to IVIg administration, mean (SD) | 10.3 (5.1) | 9.9 (5.5) | 0.72 |
| Days from diagnosis of CDI to IVIg administration, mean (SD) | 6.2 (4.9) | 6.36 (4.10) | 0.88 |
| Second infusion required, n (%) | 6 (30.0%) | ||
| Surgical intervention, n (%) | 3 (15%) | ||
| Length of hospital stay, mean (SD) | 30.4 (15.2) | 30.5 (14.3) | 0.47 |
| Recurrence following IVIg, n (%) | 2 (10%) | 1 (9.0%) | 0.89 |
| 30-day mortality, n (%) | 6 (30%) | ||
| Mortality attributable to CDI (if 30-day mortality), n (%) | 3 (50%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ragan, S.A.; Doyle, C.; Datta, N.; Abdic, H.; Wilcox, M.H.; Montgomery, R.; Crusz, S.A.; Mahida, Y.R.; Monaghan, T.M. Case Series: Efficacy of Polyclonal Intravenous Immunoglobulin for Refractory Clostridioides difficile Infection. Antibodies 2024, 13, 26. https://doi.org/10.3390/antib13020026
Ragan SA, Doyle C, Datta N, Abdic H, Wilcox MH, Montgomery R, Crusz SA, Mahida YR, Monaghan TM. Case Series: Efficacy of Polyclonal Intravenous Immunoglobulin for Refractory Clostridioides difficile Infection. Antibodies. 2024; 13(2):26. https://doi.org/10.3390/antib13020026
Chicago/Turabian StyleRagan, Sophie A., Caitlin Doyle, Neha Datta, Heather Abdic, Mark H. Wilcox, Ros Montgomery, Shanika A. Crusz, Yashwant R. Mahida, and Tanya M. Monaghan. 2024. "Case Series: Efficacy of Polyclonal Intravenous Immunoglobulin for Refractory Clostridioides difficile Infection" Antibodies 13, no. 2: 26. https://doi.org/10.3390/antib13020026
APA StyleRagan, S. A., Doyle, C., Datta, N., Abdic, H., Wilcox, M. H., Montgomery, R., Crusz, S. A., Mahida, Y. R., & Monaghan, T. M. (2024). Case Series: Efficacy of Polyclonal Intravenous Immunoglobulin for Refractory Clostridioides difficile Infection. Antibodies, 13(2), 26. https://doi.org/10.3390/antib13020026