
The Impact of Urban Built Environments on Elderly People’s Sense of Safety and Adaptation to Aging: A Case Study of Three Major Urban Agglomerations in China



Abstract
1. Introduction
2. Literature Review
2.1. Sense of Safety
2.2. Urban Environment, Social Environment, Individual Characteristics, and Sense of Safety among the Elderly
2.3. Research on the Elderly
3. Materials and Methodology
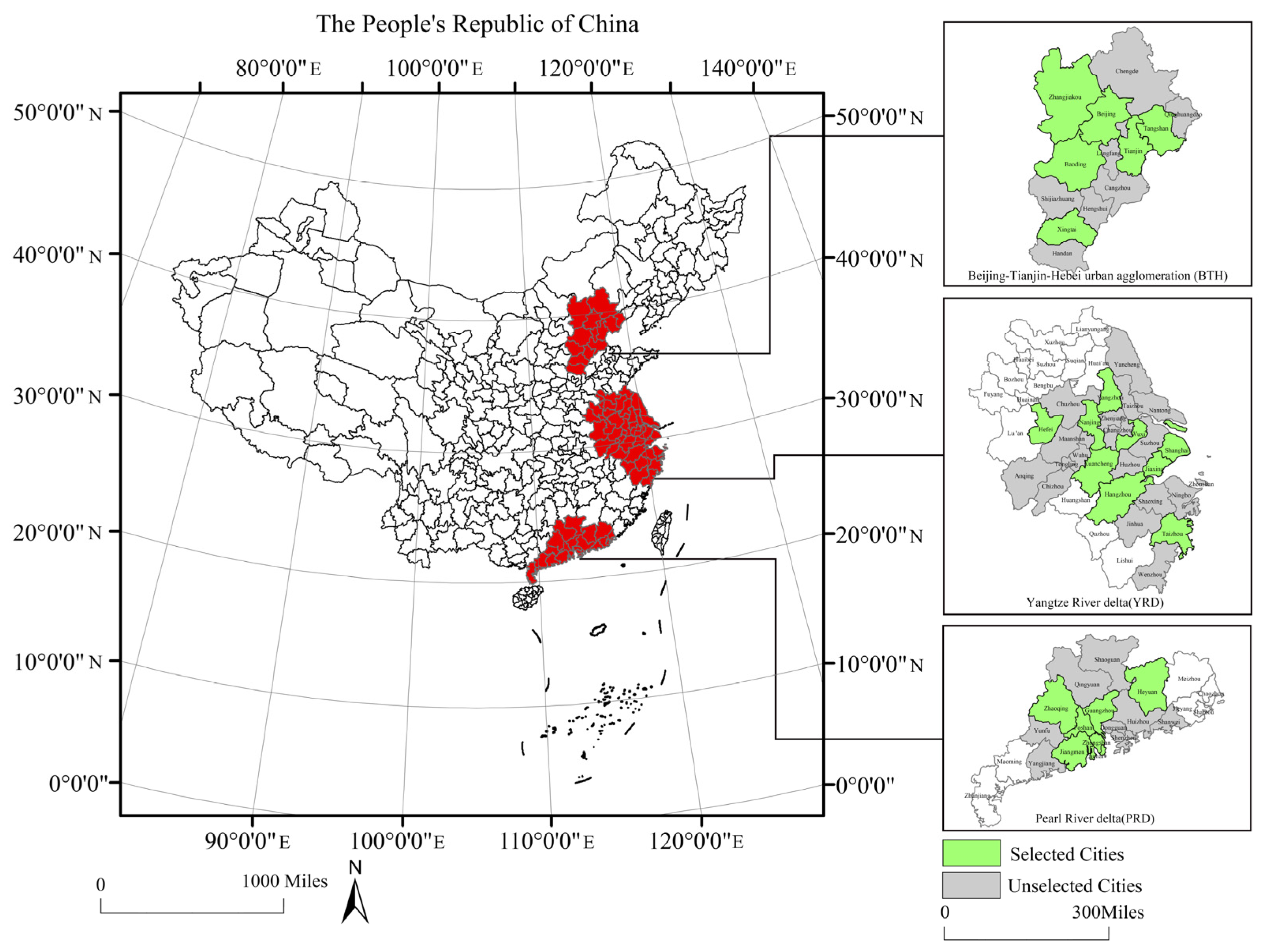
3.1. Case Study
3.2. Data Sources
3.3. Research Methods
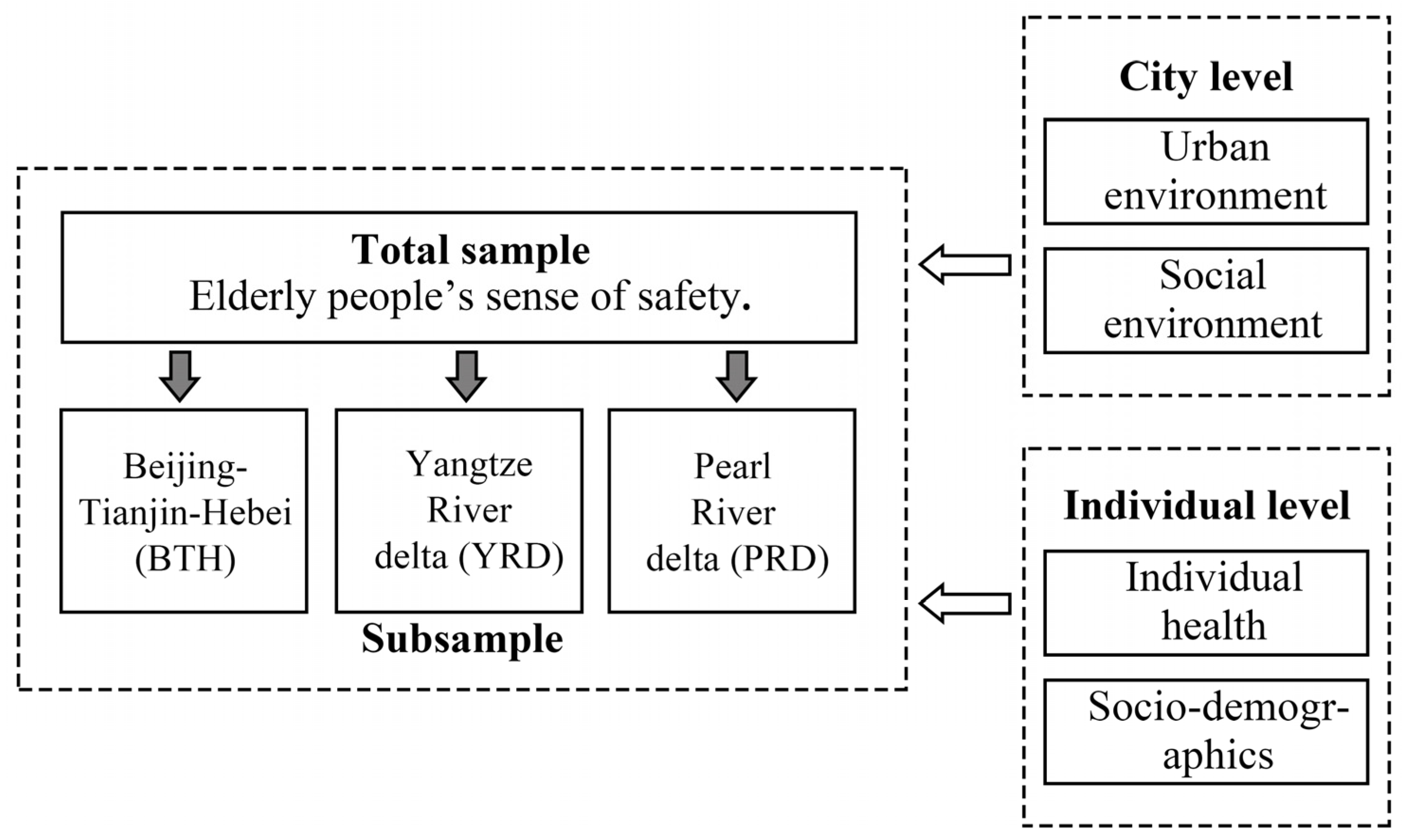
3.3.1. The Research Framework
3.3.2. Linear Regression Model
3.4. Variables and Measures
3.4.1. Sense of Safety
3.4.2. Social Environment Characteristics
3.4.3. Urban Environmental Characteristics
3.4.4. Individual Health Characteristics
4. Results and Analysis
4.1. Analysis of Total Sample Results
4.2. Comparative Analysis of Three Major Urban Agglomerations
5. Discussion
6. Conclusions and Recommendations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Han, H.; Yang, K.; Yang, C.; Yang, G.; Xu, L. Influence and Mechanism of a Multi-Scale Built Environment on the Leisure Activities of the Elderly: Evidence from Hefei City in China. Int. J. Environ. Res. Public Health 2022, 19, 9237. [Google Scholar] [CrossRef]
- Zhang, F.; Loo, B.P.; Wang, B. Aging in place: From the neighborhood environment, sense of community, to life satisfaction. Ann. Am. Assoc. Geogr. 2022, 112, 1484–1499. [Google Scholar] [CrossRef]
- van Hoof, J.; Marston, H.R.; Kazak, J.K.; Buffel, T. Ten questions concerning age-friendly cities and communities and the built environment. Build. Environ. 2021, 199, 107922. [Google Scholar] [CrossRef]
- Song, S.; Yap, W.; Hou, Y.; Yuen, B. Neighbourhood built Environment, physical activity, and physical health among older adults in Singapore: A simultaneous equations approach. Transp. Health 2020, 18, 100881. [Google Scholar] [CrossRef]
- Xin, Y.; An, J.; Xu, J. Continuous voluntary community care services for older people in China: Evidence from Wuhu. Front. Public Health 2022, 10, 1063156. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Age-Friendly Cities: A Guide; World Health Organization: Geneva, Switzerland, 2007.
- Xi, J.P. File Assembly of Chinese Communist Party Twentieth National Congress; People’s Publishing House: Beijing, China, 2022. [Google Scholar]
- Lee, S.; Yoon, J.; Woo, A. Does elderly safety matter? Associations between built environments and pedestrian crashes in Seoul, Korea. Accid. Anal. Prev. 2020, 144, 105621. [Google Scholar] [CrossRef]
- Loukaitou-Sideris, A. Is it safe to walk? 1 neighborhood safety and security considerations and their effects on walking. J. Plan Lit. 2006, 20, 219–232. [Google Scholar] [CrossRef]
- Baba, Y.; Austin, D.M. Neighborhood environmental satisfaction, victimization, and social participation as determinants of perceived neighborhood safety. Environ. Behav. 1989, 21, 763–780. [Google Scholar] [CrossRef]
- Li, J.; Tian, L.; Ouyang, W. Exploring the relationship between neighborhood-built environment and elderly health: A research based on heterogeneity of age and gender groups in Beijing. Front. Public Health 2022, 10, 882361. [Google Scholar] [CrossRef]
- Hong, J.; Chen, C. The role of the built environment on perceived safety from crime and walking: Examining direct and indirect impacts. Transportation 2014, 41, 1171–1185. [Google Scholar] [CrossRef]
- Funk, L.M.; Allan, D.E.; Chappell, N.L. Testing the relationship between involvement and perceived neighborhood safety: A multinomial logit approach. Environ. Behav. 2007, 39, 332–351. [Google Scholar] [CrossRef]
- Van Hoof, J.; Dikken, J.; van Staalduinen, W.H.; van der Pas, S.; van den Hoven, R.F.; Hulsebosch-Janssen, L.M. Towards a better understanding of the sense of safety and security of community-dwelling older adults. the case of the age-friendly city of The Hague. Int. J. Environ. Res. Public Health 2022, 19, 3960. [Google Scholar] [CrossRef]
- Zeng, E.; Dong, Y.; Yan, L.; Lin, A. Perceived Safety in the Neighborhood: Exploring the Role of Built Environment, Social Factors, Physical Activity and Multiple Pathways of Influence. Buildings 2022, 13, 2. [Google Scholar] [CrossRef]
- Roe, J.; Mondschein, A.; Neale, C.; Barnes, L.; Boukhechba, M.; Lopez, S. The urban built environment, walking and mental health outcomes among older adults: A pilot study. Front. Public Health 2020, 8, 528. [Google Scholar] [CrossRef]
- Aliyas, Z. Does social environment mediate the association between perceived safety and physical activity among adults living in low socioeconomic neighborhoods? J. Transp. Health 2019, 14, 100578. [Google Scholar] [CrossRef]
- Bracy, N.L.; Millstein, R.A.; Carlson, J.A.; Conway, T.L.; Sallis, J.F.; Saelens, B.E.; Kerr, J.; Cain, K.L.; Frank, L.D.; King, A.C. Is the relationship between the built environment and physical activity moderated by perceptions of crime and safety? Int. J. Behav. Nutr. Phys. Act. 2014, 11, 24. [Google Scholar] [CrossRef]
- Wu, H.; Chen, Y.; Zhang, Z.; Jiao, J. The impact of street characteristics on older pedestrians’ perceived safety in Shanghai, China. J. Transp. Land Use 2020, 13, 469–490. [Google Scholar] [CrossRef]
- He, H.; Li, T.; Yu, Y.; Lin, X. Associations between built environment characteristics and walking in older adults in a high-density city: A study from a Chinese megacity. Front. Public Health 2020, 8, 577140. [Google Scholar] [CrossRef]
- Wood, L.; Shannon, T.; Bulsara, M.; Pikora, T.; McCormack, G.; Giles-Corti, B. The anatomy of the safe and social suburb: An exploratory study of the built environment, social capital and residents’ perceptions of safety. Health Place 2008, 14, 15–31. [Google Scholar] [CrossRef] [PubMed]
- Yung, E.H.; Conejos, S.; Chan, E.H. Social needs of the elderly and active aging in public open spaces in urban renewal. Cities 2016, 52, 114–122. [Google Scholar] [CrossRef]
- Cai, H. China Labor Force Dynamics Survey (CLDS); China Social Science Survey Platform: Guangzhou, China, 2016. [Google Scholar]
- Maslow, A.H.; Hirsh, E.; Stein, M.; Honigmann, I. A clinically derived test for measuring psychological security-insecurity. J. Gen. Psychol. 1945, 33, 21–41. [Google Scholar] [CrossRef]
- Schichel, M.C.; Veenstra, M.Y.; Kempen, G.I.; de Vugt, M.E.; van der Zanden, B.A.; Verhey, F.R. Senior friendly communities: Designing an approach for cross-border exchange of public health policy. Health Policy 2020, 124, 1129–1136. [Google Scholar] [CrossRef]
- Zhang, Y.; Qin, B.; Tang, J. The impact of urban built environment on residential security—Based on the empirical analysis of 278 urban communities across the country. Geogr. Sci. 2017, 37, 1318–1325. [Google Scholar]
- Yue, Y.; Yang, D.; Owen, N.; Van Dyck, D. The built environment and mental health among older adults in Dalian: The mediating role of perceived environmental attributes. Soc. Sci. Med. 2022, 311, 115333. [Google Scholar] [CrossRef] [PubMed]
- Cervero, R.; Kockelman, K. Travel demand and the 3Ds: Density, diversity, and design. Transp. Res. Part D Transp. Environ. 1997, 2, 199–219. [Google Scholar] [CrossRef]
- Ewing, R.; Cervero, R. Travel and the built environment: A meta-analysis. J. Am. Plan. Assoc. 2010, 76, 265–294. [Google Scholar] [CrossRef]
- Chen, S.; Bao, Z.; Chen, J.; Yang, L.; Lou, V. Sustainable built environment for facilitating public health of older adults: Evidence from Hong Kong. Sustain. Dev. 2022, 30, 1086–1098. [Google Scholar] [CrossRef]
- Morenoff, J.D. Neighborhood mechanisms and the spatial dynamics of birth weight. Am. J. Soc. 2003, 108, 976–1017. [Google Scholar] [CrossRef]
- Wang, D.; Lin, T. Built environments, social environments, and activity-travel behavior: A case study of Hong Kong. J. Transp. Geogr. 2013, 31, 286–295. [Google Scholar] [CrossRef]
- Lin, T.; Wang, D. Tradeoffs between in-and out-of-residential neighborhood locations for discretionary activities and time use: Do social contexts matter? J. Transp. Geogr. 2015, 47, 119–127. [Google Scholar] [CrossRef]
- Lin, T.; Wang, D.; Zhou, M. Residential relocation and changes in travel behavior: What is the role of social context change? Transp. Res. Part A Policy Pract. 2018, 111, 360–374. [Google Scholar] [CrossRef]
- McDonald, N.C. Travel and the social environment: Evidence from Alameda County, California. Transp. Res. Part D Transp. Environ. 2007, 12, 53–63. [Google Scholar] [CrossRef]
- Zhang, R.; Yao, E.; Liu, Z. School travel mode choice in Beijing, China. J. Transp. Geogr. 2017, 62, 98–110. [Google Scholar] [CrossRef]
- Marquet, O.; Miralles-Guasch, C. Neighbourhood vitality and physical activity among the elderly: The role of walkable environments on active ageing in Barcelona, Spain. Soc. Sci. Med. 2015, 135, 24–30. [Google Scholar] [CrossRef] [PubMed]
- Wilson, D.K.; Kirtland, K.A.; Ainsworth, B.E.; Addy, C.L. Socioeconomic status and perceptions of access and safety for physical activity. Ann. Behav. Med. 2004, 28, 20–28. [Google Scholar] [CrossRef]
- Tucker-Seeley, R.D.; Subramanian, S.V.; Li, Y.; Sorensen, G. Neighborhood safety, socioeconomic status, and physical activity in older adults. Am. J. Prev. Med. 2009, 37, 207–213. [Google Scholar] [CrossRef] [PubMed]
- Foster, S.; Giles-Corti, B.; Knuiman, M. Neighbourhood design and fear of crime: A social-ecological examination of the correlates of residents’ fear in new suburban housing developments. Health Place 2010, 16, 1156–1165. [Google Scholar] [CrossRef]
- Kim, D. The transportation safety of elderly pedestrians: Modeling contributing factors to elderly pedestrian collisions. Accid. Anal. Prev. 2019, 131, 268–274. [Google Scholar] [CrossRef]
- Mori, Y.; Tsuji, T.; Watanabe, R.; Hanazato, M.; Miyazawa, T.; Kondo, K. Built environments and frailty in older adults: A three-year longitudinal JAGES study. Arch. Gerontol. Geriat. 2022, 103, 104773. [Google Scholar] [CrossRef]
- Li, F. Physical activity and health in the presence of China’s economic growth: Meeting the public health challenges of the aging population. J. Sport Health Sci. 2016, 5, 258–269. [Google Scholar] [CrossRef]
- Liu, Y.; Sangthong, R.; Ingviya, T.; Wan, C. Nothing like living with a family: A qualitative study of subjective well-being and its determinants among migrant and local elderly in Dongguan, China. Int. J. Environ. Res. Public Health 2019, 16, 4874. [Google Scholar] [CrossRef] [PubMed]
- National Bureau of Statistics of China. The Seventh National Census; China Statistics Press: Beijing, China, 2021. [Google Scholar]
- National Bureau of Statistics of China. China Statistical Yearbook; China Statistics Press: Beijing, China, 2017. [Google Scholar]
- Liu, J.; Liu, M.; Deng, X.; Zhuang, D.; Zhang, Z.; Luo, D. The land use and land cover change database and its relative studies in China. J. Geogr. Sci. 2002, 12, 275–282. [Google Scholar]
- Lowenkamp, C.T.; Cullen, F.T.; Pratt, T.C. Replicating Sampson and Groves’s test of social disorganization theory: Revisiting a criminological classic. J. Res. Crime Delinq. 2003, 40, 351–373. [Google Scholar] [CrossRef]
- Abdullah, A.; Hedayati Marzbali, M.; Woolley, H.; Bahauddin, A.; Maliki, N.Z. Testing for individual factors for the fear of crime using a multiple indicator-multiple cause model. Eur. J. Crim. Policy Res. 2014, 20, 1–22. [Google Scholar] [CrossRef]
- Chinese Academy of Sciences. China Meteorological Data. Available online: http://www.resdc.cn (accessed on 15 June 2016).
- Qiu, Y.; Chen, H.; Li, Z.; Wang, R.; Liu, Y.; Qin, X. Exploring Neighborhood Environmental Effects on Mental Health: A Case Study in Guangzhou. Prog. Geogr. 2019, 38, 283–295. [Google Scholar]
- Lichtenberg, P.A.; Sugarman, M.A.; Paulson, D.; Ficker, L.J.; Rahman-Filipiak, A. Psychological and functional vulnerability predicts fraud cases in older adults: Results of a longitudinal study. Clin. Gerontol. 2016, 39, 48–63. [Google Scholar] [CrossRef]
- Burnes, D.; Henderson Jr, C.R.; Sheppard, C.; Zhao, R.; Pillemer, K.; Lachs, M.S. Prevalence of financial fraud and scams among older adults in the United States: A systematic review and meta-analysis. Am. J. Public Health 2017, 107, e13–e21. [Google Scholar] [CrossRef]
- Ross, M.; Grossmann, I.; Schryer, E. Contrary to psychological and popular opinion, there is no compelling evidence that older adults are disproportionately victimized by consumer fraud. Perspect. Psychol. Sci. 2014, 9, 427–442. [Google Scholar] [CrossRef] [PubMed]
- Kircanski, K.; Notthoff, N.; DeLiema, M.; Samanez-Larkin, G.R.; Shadel, D.; Mottola, G.; Carstensen, L.L.; Gotlib, I.H. Emotional arousal may increase susceptibility to fraud in older and younger adults. Psychol. Aging 2018, 33, 325. [Google Scholar] [CrossRef]
- Button, M.; Lewis, C.; Tapley, J. Not a victimless crime: The impact of fraud on individual victims and their families. Secur. J. 2014, 27, 36–54. [Google Scholar] [CrossRef]
- Lin, Y.; Wang, T.; Zhu, T. Do migration characteristics influence the utilization of basic public health services in internal elderly migrants in China? Front. Public Health 2021, 9, 514687. [Google Scholar] [CrossRef] [PubMed]
- Jiang, B.; Mak, C.N.S.; Zhong, H.; Larsen, L.; Webster, C.J. From broken windows to perceived routine activities: Examining impacts of environmental interventions on perceived safety of urban alleys. Front. Psychol. 2018, 9, 2450. [Google Scholar] [CrossRef]
- Bauman, A.E. Updating the evidence that physical activity is good for health: An epidemiological review 2000–2003. J. Sci. Med. Sport 2004, 7, 6–19. [Google Scholar] [CrossRef]
- Firdaus, G. Built environment and health outcomes: Identification of contextual risk factors for mental well-being of older adults. Ageing Int. 2017, 42, 62–77. [Google Scholar] [CrossRef]
- Wu, D.; Tie, X.; Li, C.; Ying, Z.; Lau, A.K.H.; Huang, J.; Deng, X.; Bi, X. An extremely low visibility event over the Guangzhou region: A case study. Atmos. Environ. 2005, 39, 6568–6577. [Google Scholar] [CrossRef]
- Wang, T.J.; Lam, K.S.; Xie, M.; Wang, X.M.; Carmichael, G.; Li, Y.S. Integrated studies of a photochemical smog episode in Hong Kong and regional transport in the Pearl River Delta of China. Tellus B Chem. Phys. Meteorol. 2006, 58, 31–40. [Google Scholar] [CrossRef]
- Tao, Y.; Zhong, L.; Huang, X.; Lu, S.E.; Li, Y.; Dai, L.; Zhang, Y.; Zhu, T.; Huang, W. Acute mortality effects of carbon monoxide in the Pearl River Delta of China. Sci. Total Environ. 2011, 410, 34–40. [Google Scholar] [CrossRef]
- Feng, J. The influence of built environment on travel behavior of the elderly in urban China. Transp. Res. Part D Transp. Environ. 2017, 52, 619–633. [Google Scholar] [CrossRef]
- Wang, A.N.; Jing, J.L.; Luo, F.L.; Liang, L.S. Analysis of aqi change characteristics and correlation with PM2.5 and PM10 in Beijing-Tianjin-Hebei region. Int. Arch. Photogramm. 2020, 42, 1041–1048. [Google Scholar] [CrossRef]
- Zhang, Y.; Yao, E. Exploring elderly people’s daily time-use patterns in the living environment of Beijing, China. Cities 2022, 129, 103838. [Google Scholar] [CrossRef]
- Fernandes, A.; Van Lenthe, F.J.; Vallée, J.; Sueur, C.; Chaix, B. Linking physical and social environments with mental health in old age: A multisensor approach for continuous real-life ecological and emotional assessment. J. Epidemiol. Commun. Health 2021, 75, 477–483. [Google Scholar] [CrossRef] [PubMed]
- Biswas, R.K.; Kabir, E. Influence of distance between residence and health facilities on non-communicable diseases: An assessment over hypertension and diabetes in Bangladesh. PLoS ONE 2017, 12, e0177027. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Wang, R.; Xiao, Y.; Huang, B.; Chen, H.; Li, Z. Exploring the linkage between greenness exposure and depression among Chinese people: Mediating roles of physical activity, stress and social cohesion and moderating role of urbanicity. Health Place 2019, 58, 102168. [Google Scholar] [CrossRef] [PubMed]
- Pouso, S.; Borja, Á.; Fleming, L.E.; Gómez-Baggethun, E.; White, M.P.; Uyarra, M.C. Contact with blue-green spaces during the COVID-19 pandemic lockdown beneficial for mental health. Sci. Total Environ. 2021, 756, 143984. [Google Scholar] [CrossRef] [PubMed]
- Brown, B.B.; Werner, C.M.; Smith, K.R.; Tribby, C.P.; Miller, H.J. Physical activity mediates the relationship between perceived crime safety and obesity. Prev. Med. 2014, 66, 140–144. [Google Scholar] [CrossRef] [PubMed]
- Collia, D.V.; Sharp, J.; Giesbrecht, L. The 2001 national household travel survey: A look into the travel patterns of older Americans. J. Saf. Res. 2003, 34, 461–470. [Google Scholar] [CrossRef] [PubMed]
- Gómez, L.F.; Parra, D.C.; Buchner, D.; Brownson, R.C.; Sarmiento, O.L.; Pinzón, J.D.; Ardila, M.; Moreno, J.; Serrato, M.; Lobelo, F. Built environment attributes and walking patterns among the elderly population in Bogotá. Am. J. Prev. Med. 2010, 38, 592–599. [Google Scholar] [CrossRef]
- Fishback, P.V.; Haines, M.R.; Kantor, S. Births, deaths, and New Deal relief during the Great Depression. Rev. Econ. Stat. 2007, 89, 1–14. [Google Scholar] [CrossRef]
- Chen, Y.L.; Shih, Y.H.; Tseng, C.H.; Kang, S.Y.; Wang, H.C. Economic and health benefits of the co-reduction of air pollutants and greenhouse gases. Mitig. Adapt. Strateg. Glob. Chang. 2013, 18, 1125–1139. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | Total | PRD | YRD | BTH |
|---|---|---|---|---|
| Number of samples | 1212 | 477 | 368 | 367 |
| Age (years) | ||||
| Mean value | 62.31 | 63.17 | 62.50 | 61.01 |
| Gender (%) | ||||
| Male | 39.69 | 43.4 | 41.85 | 32.70 |
| Female | 60.31 | 56.6 | 58.15 | 67.30 |
| Marital status (%) | ||||
| Married | 92.07 | 89.10 | 89.95 | 90.71 |
| Unmarried/divorced/ widowed/separated | 7.93 | 10.90 | 10.05 | 9.29 |
| Political Affiliation (%) | ||||
| Member of the Communist Party | 7.8 | 6.0 | 12.8 | 5.5 |
| Non-Communist Party member | 92.2 | 94.0 | 86.9 | 94.5 |
| Hukou status (%) | ||||
| Local | 94.6 | 96.5 | 90.7 | 96.2 |
| Nonlocal | 5.4 | 3.5 | 9.3 | 3.8 |
| Education (%) | ||||
| Primary school and below | 56.4 | 66.6 | 35.1 | 65.0 |
| Middle and high school | 40.0 | 29.6 | 57.5 | 34.6 |
| College and above | 3.6 | 3.8 | 7.4 | 0.4 |
| Variable | Cronbach’s α | Cronbach’s α Based on Standardized Terms | Explanation |
|---|---|---|---|
| Sense of safety | 0.645 | 0.722 | 1. Unemployment |
| 2. Crimes | |||
| 3. Terrorist attacks | |||
| 4. Consuming counterfeit drugs or substandard food | |||
| 5. Being infected with a certain infectious disease |
| Variable | Cronbach’s α | Cronbach’s α Based on Standardized Terms | Explanation |
|---|---|---|---|
| Frequency of dining out | 0.926 | 0.926 | 1. Dining out on weekdays |
| 2. Dining out on rest days | |||
| 3. Inviting people to dine out | |||
| 4. Being invited to dine out | |||
| 5. Dining out with friends |
| Variables | Explanation | Measurement Method |
|---|---|---|
| Population density | Population per unit land area (persons/km2) | Number of permanent urban residents/total urban area |
| Urbanization rate | The proportion of urban permanent population to the total permanent population | Urban permanent population/total permanent population |
| Number of hospitals | Number of hospitals in each case city | — |
| Greening rate | The proportion of green land to total land area | Green land/total land area |
| Air quality (PM10) | The average concentration of dust or drifting dust (particulate matter) with diameters of 10 μm or less (PM10) in the ambient air | — |
| Variable | Cronbach’s α | Cronbach’s α Based on Standardized Terms | Explanation |
|---|---|---|---|
| Mental health | 0.929 | 0.936 | 1. Worried about some small things. |
| 2. Don’t want to eat, I have a bad appetite. | |||
| 3. Even with the help of family and friends, I still can’t get rid of my depression. | |||
| 4. Feeling inferior to others. | |||
| 5. Unable to concentrate when doing things. | |||
| 6. Feeling down. | |||
| 7. Feeling that doing anything takes a lot of effort. | |||
| 8. Feeling hopeless about the future. | |||
| 9. Feeling like my life is a failure. | |||
| 10. Feeling scared. | |||
| 11. Poor sleep. | |||
| 12. Feeling unhappy. | |||
| 13. Speaking less than usual. | |||
| 14. Feeling lonely. | |||
| 15. Feeling that people are not very friendly to me. | |||
| 16. Feeling that life is meaningless. | |||
| 17. Crying. | |||
| 18. Feeling nervous. | |||
| 19. Feeling that people don’t like me. | |||
| 20. Feeling that life cannot continue. |
| Variables | Model 1 (Total Sample) | ||
|---|---|---|---|
| Coefficient | Standard Error | T-Value | |
| Urban environment | |||
| Urbanization rate | −0.033 *** | 0.011 | −3.100 |
| Greening rate | −0.020 *** | 0.007 | −2.970 |
| Number of hospitals | 0.002 ** | 0.001 | 2.050 |
| Population density | −0.000 * | 0.000 | −1.740 |
| Air quality (PM10) | −0.013 * | 0.007 | −1.920 |
| Social environment | |||
| Social support | −0.006 | 0.006 | −1.050 |
| Community trust | −0.014 | 0.113 | −0.130 |
| Frequency of dining out | −0.059 ** | 0.028 | −2.120 |
| Individual health | |||
| Mental health | 0.041 *** | 0.012 | 3.550 |
| Exercise status | 0.366 * | 0.212 | 1.730 |
| Smoking history | −0.272 | 0.275 | −0.990 |
| Drinking history | 0.066 | 0.272 | 0.240 |
| Hospitalization status | −0.469 | 0.318 | −1.470 |
| Sociodemographic characteristics | |||
| Age | 0.004 | 0.022 | 0.180 |
| Gender (Reference group: Female) | |||
| Male | −0.335 | 0.271 | −1.240 |
| Marital status (Reference group: Unmarried/divorced/widowed/separated) | |||
| Married | 0.037 | 0.339 | 0.110 |
| Political affiliation (Reference group: Non-Communist Party member) | |||
| Members of Communist Party | 0.181 ** | 0.353 | 0.510 |
| Hukou status (Reference group: Nonlocal) | |||
| Local | −0.879 | 0.432 | −2.040 |
| Education (Reference group: Primary school and below) | |||
| Middle and high school | 0.142 | 0.212 | 0.670 |
| College and above | −0.420 | 0.590 | −0.710 |
| Constant | 25.177 *** | 2.103 | 11.970 |
| Variables | Model 2 (YRD) | Model 3 (BTH) | Model 4 (PRD) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Coefficient | Standard Error | T-Value | Coefficient | Standard Error | T-Value | Coefficient | Standard Error | T-Value | |
| Urban environment | |||||||||
| Urbanization rate | 0.042 | 0.037 | 1.150 | −0.002 | 0.044 | −0.030 | 0.000 | 0.054 | −0.000 |
| Greening rate | −0.023 * | 0.012 | −1.880 | −0.051 | 0.033 | −1.570 | −0.002 | 0.050 | −0.030 |
| Number of hospitals | 0.002 | 0.004 | 0.620 | 0.000 | 0.002 | 0.100 | 0.010 | 0.006 | 1.610 |
| Population density | −0.001 ** | 0.000 | −2.370 | −0.001 | 0.001 | −1.310 | −0.002 ** | 0.001 | −2.140 |
| Air quality (PM10) | −0.016 | 0.029 | −0.550 | −0.04 ** | 0.018 | −2.180 | −0.094 ** | 0.044 | −2.140 |
| Social environment | |||||||||
| Social support | −0.019 | 0.013 | −1.450 | 0.007 | 0.014 | 0.470 | −0.005 | 0.007 | −0.760 |
| Community trust | −0.081 | 0.239 | −0.340 | −0.240 | 0.207 | −1.160 | 0.192 | 0.173 | 1.110 |
| Frequency of dining out | −0.027 | 0.056 | −0.490 | −0.066 | 0.056 | −1.170 | −0.051 | 0.046 | −1.120 |
| Individual health | |||||||||
| Mental health | 0.068 *** | 0.022 | 3.090 | 0.050 ** | 0.021 | 2.340 | 0.028 | 0.019 | 1.450 |
| Exercise status | 1.210 *** | 0.408 | 2.960 | −0.147 | 0.375 | −0.390 | 0.331 | 0.379 | 0.870 |
| Smoking history | −0.794 | 0.513 | −1.550 | −0.615 | 0.495 | −1.240 | 0.180 | 0.472 | 0.380 |
| Drinking history | 0.465 | 0.493 | 0.940 | 0.081 | 0.536 | 0.150 | −0.004 | 0.442 | −0.010 |
| Hospitalization status | −1.285 * | 0.675 | −1.900 | −0.288 | 0.625 | −0.460 | 0.015 | 0.462 | 0.030 |
| Sociodemographic characteristics | |||||||||
| Age | 0.010 | 0.037 | 0.280 | −0.073 | 0.068 | −1.080 | 0.004 | 0.032 | 0.140 |
| Gender (Reference group: Female) | |||||||||
| Male | −0.205 | 0.457 | −0.450 | −0.912 * | 0.547 | −1.670 | 0.137 | 0.464 | 0.300 |
| Marital status (Reference group: Unmarried/divorced/widowed/separated) | |||||||||
| Married | −0.163 | 0.649 | −0.250 | 0.442 | 0.713 | 0.620 | −0.139 | 0.503 | −0.280 |
| Political affiliation (Reference group: Non-Communist Party member) | |||||||||
| Members of Communist Party | −0.797 | 0.712 | −1.120 | 1.326 ** | 0.564 | 2.350 | −0.556 | 0.638 | −0.870 |
| Hukou status (Reference group: Nonlocal) | |||||||||
| Local | −1.137 | 0.916 | −1.240 | −0.802 | 0.723 | −1.110 | −0.960 | 0.821 | −1.170 |
| Education (Reference group: Primary school and below) | |||||||||
| Middle and high school | 0.226 | 0.458 | 0.490 | −0.135 | 0.423 | −0.320 | 0.085 | 0.339 | 0.250 |
| College and above | −1.175 | 1.045 | −1.120 | −0.925 | 0.886 | −1.040 | 1.484 | 2.111 | 0.700 |
| Constant | 19.447 *** | 4.388 | 4.430 | 32.627 *** | 5.035 | 6.480 | 24.642 *** | 6.138 | 4.010 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lu, J.; Dai, M.; Li, F.; Qin, L.; Cheng, B.; Li, Z.; Yao, Z.; Wu, R. The Impact of Urban Built Environments on Elderly People’s Sense of Safety and Adaptation to Aging: A Case Study of Three Major Urban Agglomerations in China. Land 2023, 12, 1486. https://doi.org/10.3390/land12081486
Lu J, Dai M, Li F, Qin L, Cheng B, Li Z, Yao Z, Wu R. The Impact of Urban Built Environments on Elderly People’s Sense of Safety and Adaptation to Aging: A Case Study of Three Major Urban Agglomerations in China. Land. 2023; 12(8):1486. https://doi.org/10.3390/land12081486
Chicago/Turabian StyleLu, Junyu, Meilin Dai, Fuhan Li, Ludan Qin, Bin Cheng, Zhuoyan Li, Zikun Yao, and Rong Wu. 2023. "The Impact of Urban Built Environments on Elderly People’s Sense of Safety and Adaptation to Aging: A Case Study of Three Major Urban Agglomerations in China" Land 12, no. 8: 1486. https://doi.org/10.3390/land12081486
APA StyleLu, J., Dai, M., Li, F., Qin, L., Cheng, B., Li, Z., Yao, Z., & Wu, R. (2023). The Impact of Urban Built Environments on Elderly People’s Sense of Safety and Adaptation to Aging: A Case Study of Three Major Urban Agglomerations in China. Land, 12(8), 1486. https://doi.org/10.3390/land12081486