
Spatial Inequalities in Access to Safe Drinking Water in an Upper-Middle-Income Country: A Multi-Scale Analysis of Brazil


Abstract
1. Introduction
2. Materials and Methods
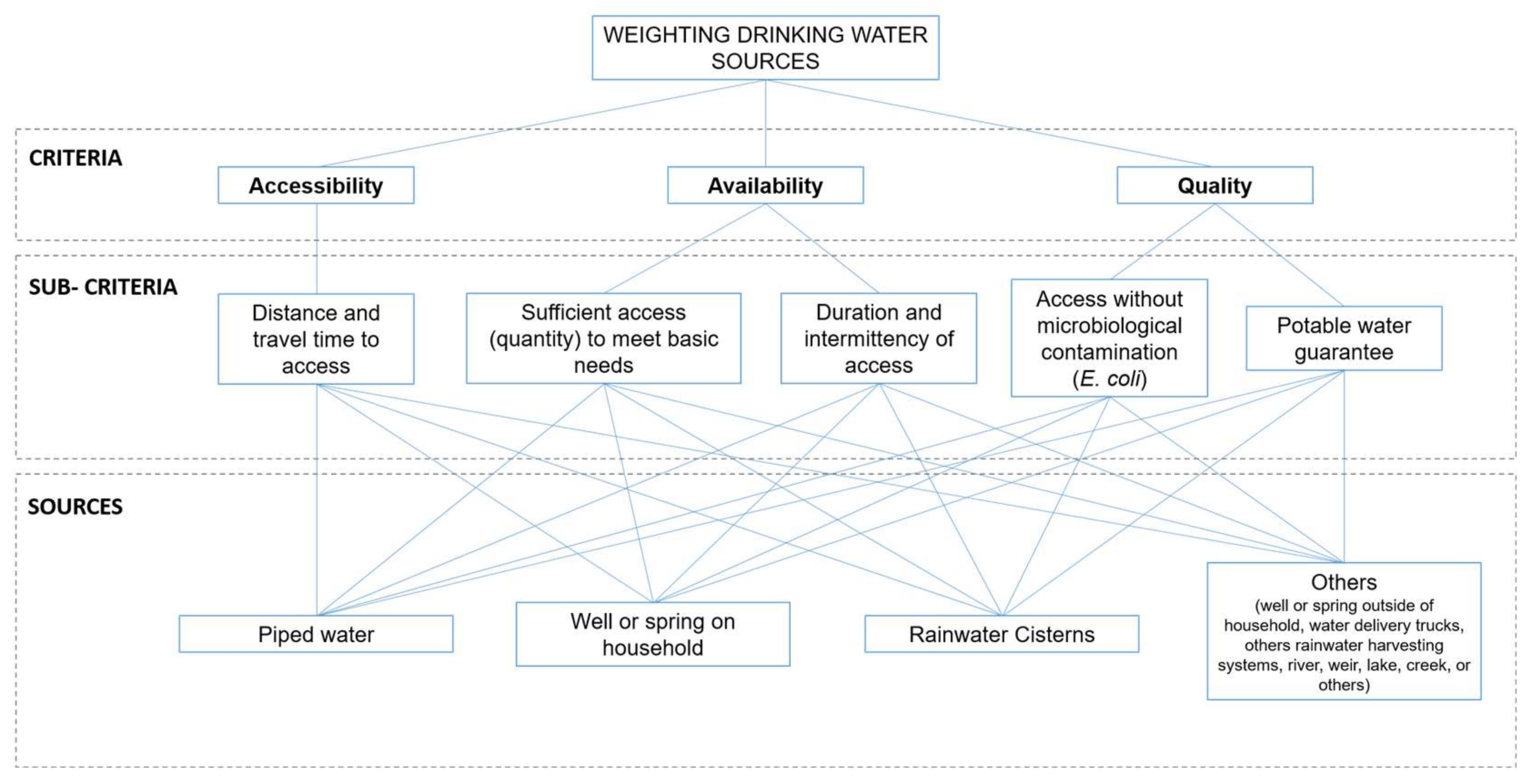
2.1. Process Analytical Hierarchy (AHP) Method
2.2. Safe Drinking Water Access Index (SDWA)
2.3. Inequalities Index for Safe Drinking Water Access
3. Results
3.1. Process Analytical Hierarchy (AHP) Method
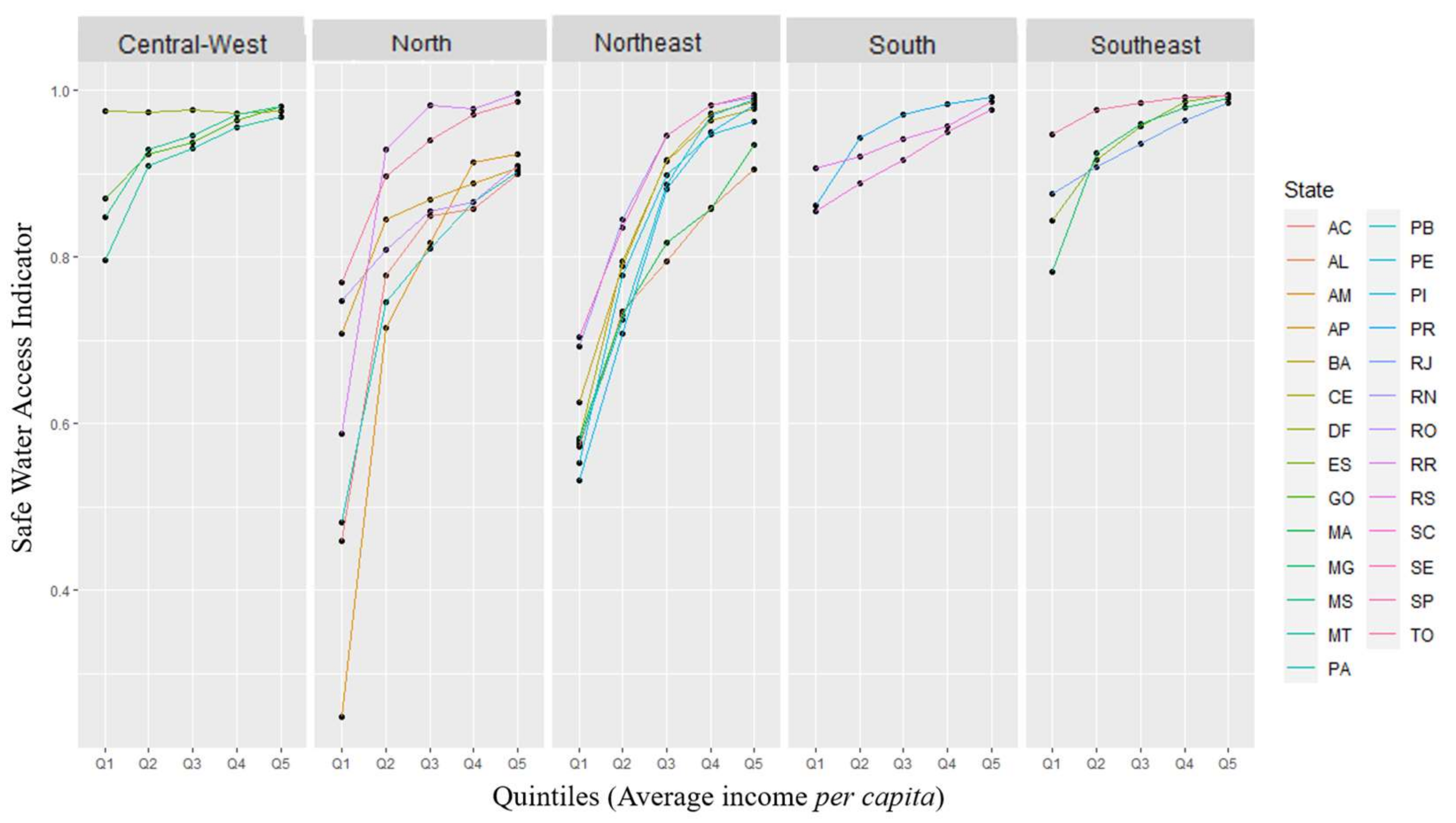
3.2. Safe Drinking Water Access Index (SDWA)
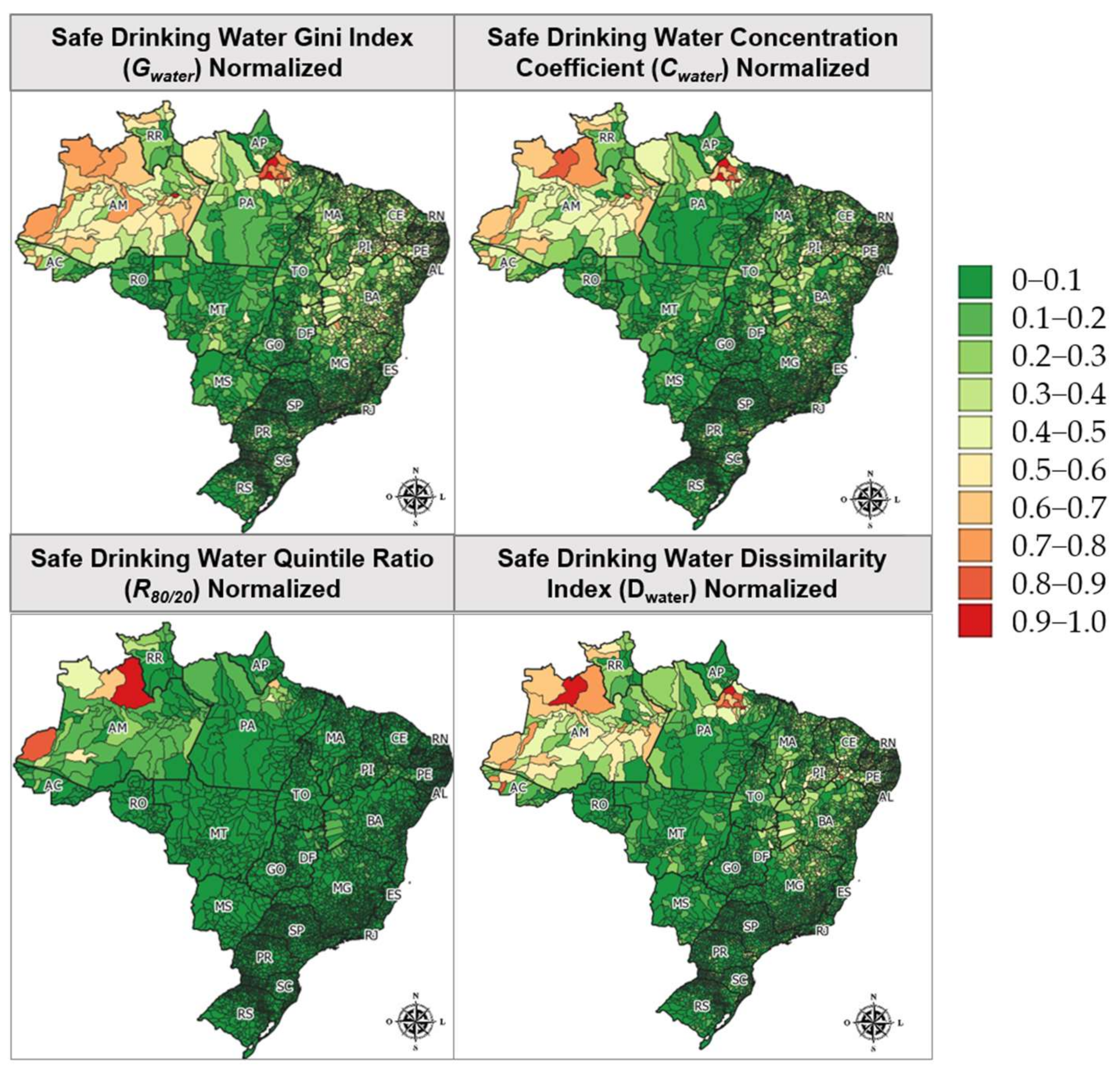
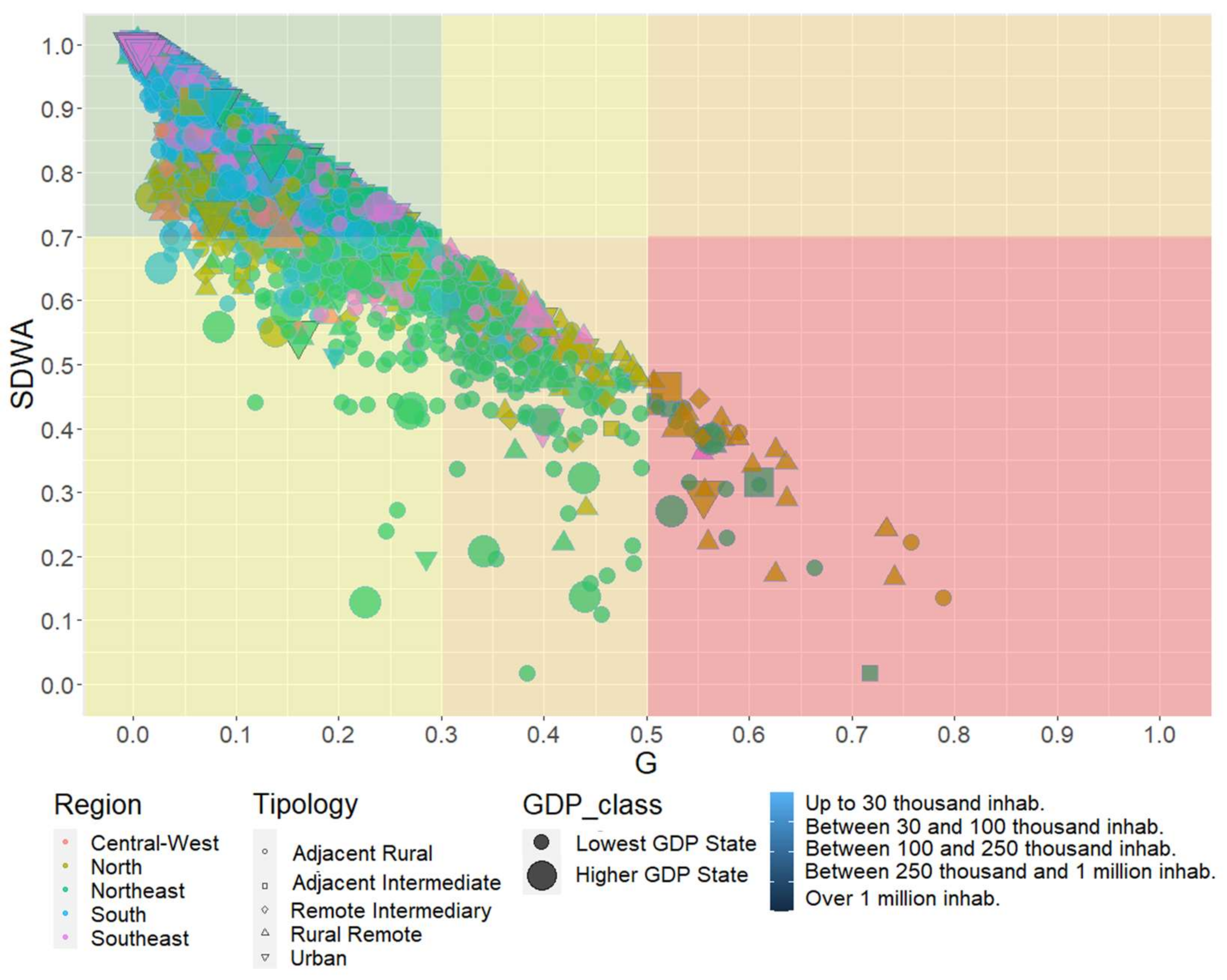
3.3. Inequalities Index
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
Abbreviations
| AHP | Process Analytical Hierarchy |
| Cwater | Safe Drinking Water Concentration Coefficient |
| Dwater | Safe Drinking Water Dissimilarity Index |
| GDP | Gross Domestic Product |
| Gwater | Safe Drinking Water Gini Index |
| IBGE | Brazilian Institute of Geography and Statistics |
| JMP | Joint Monitoring Program for Water Supply, Sanitation and Hygiene |
| MDGs | Millennium Development Goals |
| PLANSAB | National Plan of Basic Sanitation |
| PNAD | National Household Sampling Survey |
| R80/20 | Ratios between Upper and Lower Quintiles |
| SDGs | Sustainable Development Goals |
| SDWA | Safe Drinking Water Access Index |
| SNIS | National Sanitation Information |
| UF | Federal Units |
| UNICEF | United Nations International Children’s Emergency Fund |
| WHO | World Health Organization |
References
- United Nations General Assembly. Resolution A/RES/64/292. The Human Right to Water and Sanitation. 2010. Available online: https://documents-dds-ny.un.org/doc/UNDOC/GEN/N09/479/35/PDF/N0947935.pdf?OpenElement (accessed on 30 January 2023).
- United Nations. The Human Right to Water and Sanitation Milestones. Available online: https://www.un.org/waterforlifedecade/pdf/human_right_to_water_and_sanitation_milestones.pdf (accessed on 30 January 2023).
- United Nations General Assembly. Resolution A/RES/70/1. Transforming Our World: The 2030 Agenda for Sustainable Development. 2015. Available online: https://documents-dds-ny.un.org/doc/UNDOC/GEN/N15/291/89/PDF/N1529189.pdf?OpenElement (accessed on 30 January 2023).
- United Nations (UN). The Millennium Development Goals Report 2015; United Nations: New York, NY, USA, 2015. [Google Scholar]
- World Health Organization (WHO). United Nations Children’s Fund (UNICEF) Progress on Household Drinking Water, Sanitation and Hygiene 2000–2020: Five Years into the SDGs 2021; WHO: Geneva, Switzerland, 2021. [Google Scholar]
- Ministério do Desenvolvimento Regional. Secretaria Nacional de Saneamento (SNS) Plano Nacional de Saneamento Básico 2019; MDR/SNS: Brasilia, Brazil, 2019; p. 239.
- Morales-Novelo, J.A.; Rodríguez-Tapia, L.; Revollo-Fernández, D.A. Inequality in Access to Drinkingwater and Subsidies between Low and High Income Households in Mexico City. Water 2018, 10, 1023. [Google Scholar] [CrossRef]
- Cetrulo, T.B.; Marques, R.C.; Malheiros, T.F.; Cetrulo, N.M. Monitoring Inequality in Water Access: Challenges for the 2030 Agenda for Sustainable Development. Sci. Total Environ. 2020, 727, 138746. [Google Scholar] [CrossRef]
- Queiroz, V.C.; de Carvalho, R.C.; Heller, L. New Approaches to Monitor Inequalities in Access to Water and Sanitation: The SDGs in Latin America and the Caribbean. Water 2020, 12, 931. [Google Scholar] [CrossRef]
- Cowell, F. Measuring Inequality, 3rd ed.; Oxford University Press: Oxford, UK, 2011; ISBN 9780199594030. [Google Scholar]
- World Health Organization (WHO); United Nations Children’s Fund (UNICEF). Inequalities in Sanitation and Drinking Water in Latin America and the Caribbean; WHO: Geneva, Switzerland, 2016. [Google Scholar]
- Berthe, A. Mesurer Les Inégalités d’accès à l’eau et à l’assainissement Dans Le Nord et Le Nordeste Du Brésil: Quels Enseignements En Matière de Justice Sociale? Cah. du GREThA 2016, 7, 22. [Google Scholar]
- Cole, M.J.; Bailey, R.M.; Cullis, J.D.S.; New, M.G. Spatial Inequality in Water Access and Water Use in South Africa. Water Policy 2018, 20, 37–52. [Google Scholar] [CrossRef]
- Cha, S.; Jin, Y.; Elhag, M.S.; Kim, Y.; Ahmed Ismail, H.A.H. Unequal Geographic Distribution of Water and Sanitation at the Household and School Level in Sudan. PLoS ONE 2021, 16, e0258418. [Google Scholar] [CrossRef]
- Chaudhuri, S.; Roy, M. Rural-Urban Spatial Inequality in Water and Sanitation Facilities in India: A Cross-Sectional Study from Household to National Level. Appl. Geogr. 2017, 85, 27–38. [Google Scholar] [CrossRef]
- Guragai, B.; Takizawa, S.; Hashimoto, T.; Oguma, K. Effects of Inequality of Supply Hours on Consumers’ Coping Strategies and Perceptions of Intermittent Water Supply in Kathmandu Valley, Nepal. Sci. Total Environ. 2017, 599, 431–441. [Google Scholar] [CrossRef]
- Malakar, K.; Mishra, T. Application of Gini, Theil and Concentration Indices for Assessing Water Use Inequality. Int. J. Soc. Econ. 2017, 44, 1335–1347. [Google Scholar] [CrossRef]
- Roche, R.; Bain, R.; Cumming, O. A Long Way to Go—Estimates of Combined Water, Sanitation and Hygiene Coverage for 25 Sub-Saharan African Countries. PLoS ONE 2017, 12, e0171783. [Google Scholar] [CrossRef]
- Malakar, K.; Mishra, T.; Patwardhan, A. Inequality in Water Supply in India: An Assessment Using the Gini and Theil Indices. Environ. Dev. Sustain. 2018, 20, 841–864. [Google Scholar] [CrossRef]
- He, W.J.; Lai, Y.S.; Karmacharya, B.M.; Dai, B.F.; Hao, Y.T.; Xu, D.R. Geographical Heterogeneity and Inequality of Access to Improved Drinking Water Supply and Sanitation in Nepal. Int. J. Equity Health 2018, 17, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Fuller, M.; Dwivedi, P. Assessing Changes in Inequality for Millennium Development Goals among Countries: Lessons for the Sustainable Development Goals. Soc. Sci. 2019, 8, 207. [Google Scholar] [CrossRef]
- Babuna, P.; Yang, X.; Bian, D. Water Use Inequality and Efficiency Assessments in the Yangtze River Economic Delta of China. Water 2020, 12, 1709. [Google Scholar] [CrossRef]
- Bayu, T.; Kim, H.; Oki, T. Water Governance Contribution to Water and Sanitation Access Equality in Developing Countries. Water Resour. Res. 2020, 56, 1–13. [Google Scholar] [CrossRef]
- Indra, I.; Nazara, S.; Hartono, D.; Sumarto, S. Inequality of Opportunity among Indonesian School Children: Education, Electricity and Clean Water. Int. J. Dev. Issues 2020, 19, 119–144. [Google Scholar] [CrossRef]
- Hernández-Vasquéz, A.; Rojas-Roque, C.; Marques Sales, D.; Santero, M.; Bendezu-Quispe, G.; Barrientos-Gutiérrez, T.; Miranda, J.J. Inequalities in Access to Safe Drinking Water in Peruvian Households According to City Size: An Analysis from 2008 to 2018. Int. J. Equity Health 2021, 20, 1–11. [Google Scholar] [CrossRef]
- Oskam, M.J.; Pavlova, M.; Hongoro, C.; Groot, W. Socio-Economic Inequalities in Access to Drinking Water among Inhabitants of Informal Settlements in South Africa. Int. J. Environ. Res. Public Health 2021, 18, 10528. [Google Scholar] [CrossRef]
- Tasbasi, A. A Threefold Empirical Analysis of the Relationship between Regional Income Inequality and Water Equity Using Tapio Decoupling Model, WPAT Equation, and the Local Dissimilarity Index: Evidence from Bulgaria. Environ. Sci. Pollut. Res. 2021, 28, 4352–4365. [Google Scholar] [CrossRef]
- Yu, W.; Bain, R.E.S.; Yu, J.; Alegana, V.; Dotse-Gborgbortsi, W.; Lin, Y.; Wright, J.A. Mapping Access to Basic Hygiene Services in Low- and Middle-Income Countries: A Cross-Sectional Case Study of Geospatial Disparities. Appl. Geogr. 2021, 135, 102549. [Google Scholar] [CrossRef]
- Alfonso, S.M.; Kazama, S.; Takizawa, S. Inequalities in Access to and Consumption of Safely Managed Water Due to Socio-Economic Factors: Evidence from Quezon City, Philippines. Curr. Res. Environ. Sustain. 2022, 4, 100117. [Google Scholar] [CrossRef]
- Babuna, P.; Yang, X.; Tulcan, R.X.S.; Dehui, B.; Takase, M.; Guba, B.Y.; Han, C.; Awudi, D.A.; Li, M. Modeling Water Inequality and Water Security: The Role of Water Governance. J. Environ. Manag. 2023, 326, 116815. [Google Scholar] [CrossRef]
- Wang, X.J.; Zhang, J.Y.; Shahid, S.; El Mahdi, A.; He, R.M.; Wang, X.G.; Ali, M. Gini Coefficient to Assess Equity in Domestic Water Supply in the Yellow River. Mitig. Adapt. Strateg. Glob. Chang. 2012, 17, 65–75. [Google Scholar] [CrossRef]
- Yang, H.; Bain, R.; Bartram, J.; Gundry, S.; Pedley, S.; Wright, J. Water Safety and Inequality in Access to Drinking-Water between Rich and Poor Households. Environ. Sci. Technol. 2013, 47, 1222–1230. [Google Scholar] [CrossRef]
- Pullan, R.L.; Freeman, M.C.; Gething, P.W.; Brooker, S.J. Geographical Inequalities in Use of Improved Drinking Water Supply and Sanitation across Sub-Saharan Africa: Mapping and Spatial Analysis of Cross-Sectional Survey Data. PLoS Med. 2014, 11, e1001626. [Google Scholar] [CrossRef]
- Yu, W.; Bain, R.E.S.; Mansour, S.; Wright, J.A. A Cross-Sectional Ecological Study of Spatial Scale and Geographic Inequality in Access to Drinking-Water and Sanitation. Int. J. Equity Health 2014, 13, 113. [Google Scholar] [CrossRef]
- Instituto Brasileiro de Geografia e Estatística (IBGE). Cidades e Estados. Available online: https://www.ibge.gov.br/cidades-e-estados (accessed on 24 January 2023).
- World Bank. World Bank Open Data. Available online: https://data.worldbank.org/ (accessed on 24 January 2023).
- Sistema Nacional de Informações sobre Saneamento (SNIS). Diagnóstico Temático Serviços de Água e Esgoto: Gestão Técnica de Água—Ano de Referência 2020. 2022. Available online: https://arquivos-snis.mdr.gov.br/DIAGNOSTICO_TEMATICO_GESTAO_TECNICA_DE_AGUA_AE_SNIS_2022.pdf (accessed on 30 January 2023).
- Instituto Brasileiro de Geografia e Estatística (IBGE). Classificação e Caracterização Dos Espaços Rurais e Urbanos Do Brasil: Uma Primeira a Proximação; IBGE: Rio de Janeiro, Brazil, 2017; ISBN 978-85-240-4421-2.
- Saaty, R.W. The Analytic Hierarchy Process-What It Is and How It Is Used. Math. Model. 1987, 9, 161–176. [Google Scholar] [CrossRef]
- Goepel, K. Implementation of an Online Software Tool for the Analytic Hierarchy Process (AHP-OS). Int. J. Anal. Hierarchy Process 2018, 10, 469–487. [Google Scholar] [CrossRef]
- Haughton, J.; Khandker, S.R. Chapter 6: Inequality Measures. In Handbook on Poverty and Inequality; World Bank: Washington, DC, USA, 2009; Volume 3, pp. 101–120. [Google Scholar]
- Sitthiyot, T.; Holasut, K. A Simple Method for Measuring Inequality. Palgrave Commun. 2020, 6, 1–9. [Google Scholar] [CrossRef]
- United Nations (UN). Development Issues No. 2: Inequality Measurement. Available online: https://www.un.org/development/desa/dpad/wp-content/uploads/sites/45/publication/dsp_policy_02.pdf (accessed on 30 January 2023).
- Comissão Econômica e Social para a Ásia e o Pacífico (ESCAP). Measuring Inequality of Access: What Is the D-Index? ESCAP: Bangkok, Thailand, 2019. [Google Scholar]
- Instituto Trata Brasil. Acesso à Água Nas Regiões Norte e Nordeste Do Brasil: Desafios e Perspectivas; Instituto Trata Brasil: Sao Paulo, Brazil, 2018. [Google Scholar]
- World Health Organization (WHO). Handbook on Health Inequality Monitoring: With a Special Focus on Low- and Middle-Income Countries; WHO: Geneva, Switzerland, 2013; p. 105. [Google Scholar]
- World Health Organization (WHO); United Nations Children’s Fund (UNICEF). Safely Managed Drinking Water; WHO: Geneva, Switzerland, 2017. [Google Scholar]
- Every Woman Every Child Latin America and Caribbean (EWEC-LAC). Step-by-Step Guide for Measuring Social Inequalities in Health; EWEC-LAC: Ciudad del Saber, Panamá, 2020. [Google Scholar]
- Agência Nacional de Águas (ANA). Atlas Esgotos—Despoluição de Bacias Hidrográficas; ANA: Brasília, Brazil, 2017.











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Region | UF |
|---|---|
| North | Acre (AC)/Amapá (AP)/Amazonas (AM)/Pará (PA)/Rondônia (RO)/Roraima (RR)/Tocantins (TO) |
| Northeast | Alagoas (AL)/Bahia (BA)/Ceará (CE)/Maranhão (MA)/Paraíba (PB)/Pernambuco (PE)/Piauí (PI)/Rio Grande do Norte (RN)/Sergipe (SE) |
| Southeast | Espírito Santo (ES)/Minas Gerais (MG)/Rio de Janeiro (RJ)/São Paulo (SP) |
| South | Paraná (PR)/Rio Grande do Sul (RS)/Santa Catarina (SC) |
| Central-West | Distrito Federal (DF)/Goiás (GO)/Mato Grosso (MT)/Mato Grosso do Sul (MS) |
| Value Range | Inequality Class |
|---|---|
| <0.3 | Equality |
| ≥0.3 and <0.4 | Warning limit |
| ≥0.4 and <0.5 | Inequality |
| ≥0.5 | High inequality |
| SDWA < 40% | 40% ≤ SDWA < 60% | 60% ≤ SDWA < 80% | SDWA ≥ 80% | ||
|---|---|---|---|---|---|
| Gwater | Average | 0.51 | 0.35 | 0.20 | 0.07 |
| Max | 0.79 | 0.57 | 0.38 | 0.19 | |
| Min | 0.23 | 0.08 | 0.02 | 0.00 | |
| Cwater | Average | 0.35 | 0.27 | 0.15 | 0.05 |
| Max | 0.74 | 0.56 | 0.38 | 0.21 | |
| Min | 0.00 | 0.02 | 0.00 | 0.00 | |
| R80/20 | Average | 2.12 | 1.57 | 1.22 | 1.06 |
| Max | 9.37 | 11.39 | 2.66 | 1.50 | |
| Min | 0.46 | 0.71 | 0.59 | 0.87 | |
| Dwater | Average | 0.32 | 0.22 | 0.11 | 0.04 |
| Max | 0.61 | 0.49 | 0.35 | 0.49 | |
| Min | 0.08 | 0.00 | 0.00 | 0.00 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jesus, F.S.M.d.; Monteiro, A.M.V.; Tomasella, J. Spatial Inequalities in Access to Safe Drinking Water in an Upper-Middle-Income Country: A Multi-Scale Analysis of Brazil. Water 2023, 15, 1620. https://doi.org/10.3390/w15081620
Jesus FSMd, Monteiro AMV, Tomasella J. Spatial Inequalities in Access to Safe Drinking Water in an Upper-Middle-Income Country: A Multi-Scale Analysis of Brazil. Water. 2023; 15(8):1620. https://doi.org/10.3390/w15081620
Chicago/Turabian StyleJesus, Fernanda Santos Mota de, Antonio Miguel Vieira Monteiro, and Javier Tomasella. 2023. "Spatial Inequalities in Access to Safe Drinking Water in an Upper-Middle-Income Country: A Multi-Scale Analysis of Brazil" Water 15, no. 8: 1620. https://doi.org/10.3390/w15081620
APA StyleJesus, F. S. M. d., Monteiro, A. M. V., & Tomasella, J. (2023). Spatial Inequalities in Access to Safe Drinking Water in an Upper-Middle-Income Country: A Multi-Scale Analysis of Brazil. Water, 15(8), 1620. https://doi.org/10.3390/w15081620