
Exploring Risk Perception and Behaviours at the Intersection of Flood Events and Private Groundwater Supplies: A Qualitative Focus Group Study


 ,
,  ,
,  and
and
Abstract
:1. Introduction
2. Methods
2.1. Participant Recruitment and Data Collection
- (i).
- water quality perception;
- (ii).
- flood vulnerability and severity;
- (iii).
- public awareness and health-protection resources.
2.2. Data Analysis
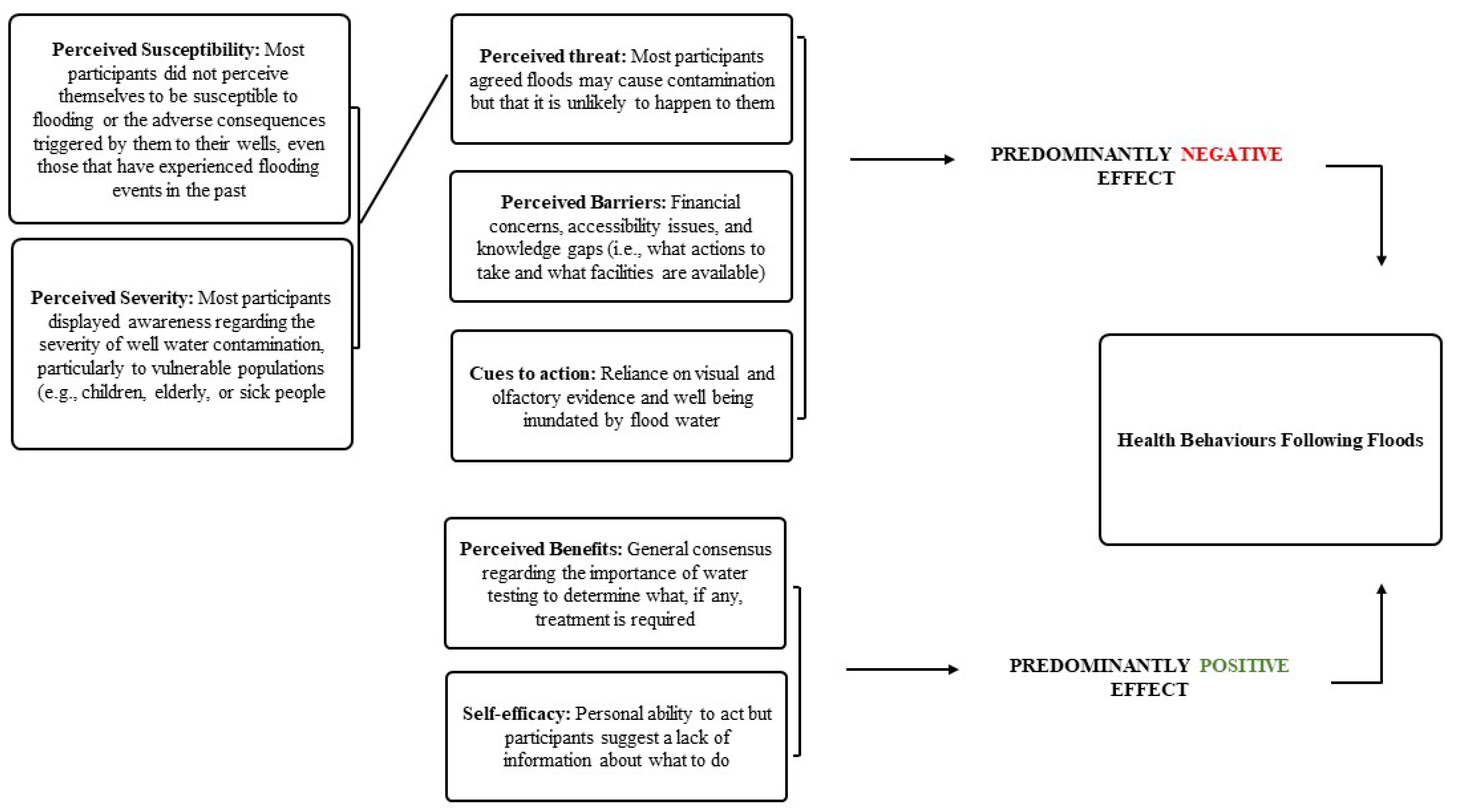
2.3. Health Belief Model
3. Results
3.1. Focus Group Characteristics
3.2. General Thoughts on Well Water Quality
FG5: “My son had gastroenteritis a couple of weeks ago, not that, like I think it’s probably nothing to do with the [well], just something but it’s just in the back of my mind”
FG1: “[It would be] far cheaper [less expensive]”
FG3: “I’d say the public water is way safer”
FG5: “I have to get it (my well) serviced twice a year. It would be cheaper for me to pay water charges”
FG7: “I might as a second… just to have as a backup”
FG1: “One doesn’t know exactly what chemicals are being put in, I know they’re probably ok, but you don’t know that”,
FG1: “I suppose the main thing is that you’d like to know what is in your water”,
FG7: “I can taste the chlorine in town water, even when it’s boiled I can still taste it”
FG8: “I like the idea, I think, of the well, I do think like it’s fresh, it has no additives and things like that”.
3.3. Flooding Experience and Perceived Threat
FG1: “Mine couldn’t, I’m on a hill”
FG2: “No, I’m high up”
FG7: “I would say (other participant’s name) if you or I flood, the rest of the country will be under six feet of water”
FG5: “Sort of, I wouldn’t call it flooding, just it came around like and just took a while to [dissipate]”
FG8: “I think once we might have had sort of a heavy flood, actually the water was ok, it’s a good few years ago now”
FG3: “If it wasn’t very close, if it was a hundred metres away, I don’t think I’d think of it”.
FG1: “Now every other well could be contaminated in that field, mine can’t. Because mine is higher than theirs”
FG5: “Mine certainly would be [less likely to become contaminated], no matter what because I’m there 45 years so it never happened, and it would be very unlikely to happen, that’s just my own personal experience”.
FG5: “Personally my own well compared to other wells in the area, I would classify as low risk”.
FG7: “And you have your own land around so nobody can be doing anything. Perfect circumstances”.
FG3: “At least with a septic tank you can control it yourself, you know”.
3.4. Cues to Action
FG8: “After the snow, our pipes froze and then when we got it all back working. And after that then for a good while there was a lot of dirt coming out in the water. I stopped using it. I stopped using it for a while, but we let it run and then after a while, then considered getting it tested and then after a while it seemed fine”.
3.5. Perceived Benefits and Barriers
FG2: “You need to see whether you need treatment”
FG2: “Just to see is it contaminated and that, you know?”
FG5: “Unless you know what’s in the water you can’t deal with it”.
FG2: “It was quite dear; I remember at the time being a lone parent. I thought: ‘Gee €150 or something’. I do remember it being very dear [expensive], and I thought ‘Not this week, maybe next week. Not next week, maybe the week after…”
FG5: “It kind of slipped down the list of priorities”.
FG3: “No, I wouldn’t go near them, not in a million years”.
3.6. Self Efficacy
FG2 “Q: If your well flooded would you know what to do? Or where to find the information out?
A: Wouldn’t have a clue”.
FG 5 “(I would be) prepared to do it if I knew what I had to do…”
3.7. Health Behaviours following Floods
FG5: “The highest risk to all wells is lack of information and lack of knowledge. People not even understanding how, where the water comes from, let alone what to do with it. If people understand the risk of flooding, 90% of them would get a remedy fairly quick, it’s just that they’re not aware of the risks”.
FG1: “The man who owns the well”
FG1: “The way I look at it if it’s my well it’s my job”
FG3: “I would see it as our own responsibility, but I’d like to get a bit more help from council as regards testing, you know, if you’re supposed to get it tested but if they had the facilities to test it, which they probably do because they’re testing their own water all the time”.
FG7: “You bored your well, it’s up to you to keep it”
FG8: “The owners first”.
FG1: “They should yeah, but they don’t”
FG7: “It’s a pity the local authority hasn’t a board of some kind there that you can run in to a place and say ‘could I get that tested please’ and [get] a charge, a small charge, now not astronomical money, but I’m sure fifty euro would cover a water test, it would be a great service, but it’ll never happen…”
FG8: “I wouldn’t expect someone knocking on the door saying did your well flood, it would be nice to have somebody to contact if it did”.
4. Discussion
4.1. Overview
4.2. Implications & Future Research
4.3. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| 1 | What is your gender: | ||||
| □ Male | □ Female | ||||
| 2 | How old are you? | ||||
| □ 18–24 | □ 25–34 | □ 35–49 | □ 50–65 | □ 65+ | |
| 3 | How long have you lived in your current home? | ||||
| □ 0–1 years | □ 2–5 years | □ 6–10 years | □ Over 10 years | ||
| 4 | Do you own it or rent your current home? | ||||
| □ Own | □ Rent | □ Other | |||
| 5 | Please provide your eircode so we can identify your well’s hydrogeological information: ________________ | ||||
| 6 | How many people that currently live in your household (including yourself) fall under each of the following age groups? Leaving blank space equals 0 (zero) persons in that age group | ||||
| Less than 1 year old: ___ | 11–17 years old: ___ | ||||
| 1–5 years old: ___ | 18–65 years old: ___ | ||||
| 6–10 years old: ___ | Over 65 years old: ___ | ||||
| 7 | Which of the following is a source of drinking water in your household? | ||||
| □ Private household well | □ Private group (ground)water scheme | ||||
| 8 | What type of well do you have? | ||||
| □ Hand-dug | □ Borehole | □ Don’t know | |||
| 9 | How deep is your well? | ||||
| □ Under 15 ft (Under 5 m) | □ 31 to 65 ft (11 to 20 m) | □ Over 100 ft (Over 30 m) | |||
| □ 15 to 30 ft (5 to 10 m) | □ 66 to 100 ft (21 to 30 m) | □ Don’t know | |||
| 10 | Do you apply any of the following to your well water before consuming it? Mark as many options as are applicable | ||||
| □ Chlorination | □ UV treatment | □ I boil my water before drinking | |||
| □ Jug Filters | □ Water softener | □ None of the ones mentioned | |||
| □ Cartridge filters | □ Reverse osmosis | □ Don’t know | |||
| 11 | Do you drink the water from your well? | ||||
| □ Yes | □ No | ||||
| 12 | Have you ever had your well water tested for contamination by a laboratory (before today)? | ||||
| □ Yes—and didn’t find contamination | □ No | ||||
| □ Yes—and found contamination | □ Don’t know | ||||
| 13 | Has flooding (as shown in the pictures below) ever occurred within 100 m of your well? | ||||
 | |||||
| □ Yes—every year | □ No—but it has happened to people I know | ||||
| □ Yes—a few of times in the past | □ No—and it has not happened to anyone I know | ||||
| □ Yes—once before | □ Don’t know | ||||
References
- Barredo, J.I. Major flood disasters in Europe: 1950–2005. Nat. Hazards 2007, 42, 125–148. [Google Scholar] [CrossRef]
- Owrangi, A.M.; Lannigan, R.; Simonovic, S.P. Interaction between land-use change, flooding and human health in Metro Vancouver, Canada. Nat. Hazards 2014, 72, 1219–1230. [Google Scholar] [CrossRef]
- EEA. Climate Change Adaptation and Disaster Risk Reduction in Europe. Enhancing Coherence of the Knowledge Base, Policies and Practices. Report No. 15/217; EEA: Luxembourg, 2017. [Google Scholar]
- Pall, P.; Aina, T.; Stone, D.A.; Stott, P.; Nozawa, T.; Hilberts, A.G.J.; Lohmann, D.; Allen, M.R. Anthropogenic greenhouse gas contribution to flood risk in England and Wales in autumn 2000. Nat. Cell Biol. 2011, 470, 382–385. [Google Scholar] [CrossRef] [PubMed]
- Arnell, N.W.; Gosling, S. The impacts of climate change on river flood risk at the global scale. Clim. Chang. 2016, 134, 387–401. [Google Scholar] [CrossRef] [Green Version]
- Hosseinzadehtalaei, P.; Tabari, H.; Willems, P. Satellite-based data driven quantification of pluvial floods over Europe under future climatic and socioeconomic changes. Sci. Total Environ. 2020, 721, 137688. [Google Scholar] [CrossRef]
- Bubeck, P.; Botzen, W.; Aerts, J.C.J.H. A Review of Risk Perceptions and Other Factors that Influence Flood Mitigation Behavior. Risk Anal. 2012, 32, 1481–1495. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Neill, E. Expanding the horizons of integrated flood risk management: A critical analysis from an Irish perspective. Int. J. River Basin Manag. 2017, 16, 71–77. [Google Scholar] [CrossRef]
- O’Neill, E. Neighbourhood design considerations in flood risk management. Plan Theory Pract. 2013, 14, 129–134. [Google Scholar]
- Kellens, W.; Terpstra, T.; De Maeyer, P. Perception and Communication of Flood Risks: A Systematic Review of Empirical Research. Risk Anal. 2013, 33, 24–49. [Google Scholar] [CrossRef] [Green Version]
- Escobar-Tello, M.P.; DeMeritt, D. Flooding and the framing of risk in British broadsheets, 1985–2010. Public Underst. Sci. 2014, 23, 454–471. [Google Scholar] [CrossRef] [Green Version]
- Devitt, C.; O’Neill, E. The framing of two major flood episodes in the Irish print news media: Implications for societal adaptation to living with flood risk. Public Underst. Sci. 2016, 26, 872–888. [Google Scholar] [CrossRef] [PubMed]
- Semenza, J.C.; Höser, C.; Herbst, S.; Rechenburg, A.; Suk, J.E.; Frechen, T.; Kistemann, T. Knowledge Mapping for Climate Change and Food- and Waterborne Diseases. Crit. Rev. Environ. Sci. Technol. 2012, 42, 378–411. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muirhead, R.; Davies-Colley, R.; Donnison, A.; Nagels, J. Faecal bacteria yields in artificial flood events: Quantifying in-stream stores. Water Res. 2004, 38, 1215–1224. [Google Scholar] [CrossRef] [PubMed]
- Weber, C.; Schager, E.; Peter, A. Habitat diversity and fish assemblage structure in local river widenings: A case study on a swiss river. River Res. Appl. 2009, 25, 687–701. [Google Scholar] [CrossRef]
- Andrade, L.; O’Dwyer, J.; O’Neill, E.; Hynds, P. Surface water flooding, groundwater contamination, and enteric disease in developed countries: A scoping review of connections and consequences. Environ. Pollut. 2018, 236, 540–549. [Google Scholar] [CrossRef]
- Murphy, H.M.; Prioleau, M.D.; Borchardt, M.A.; Hynds, P.D. Review: Epidemiological evidence of groundwater contribution to global enteric disease, 1948–2015. Hydrogeol. J. 2017, 25, 981–1001. [Google Scholar] [CrossRef]
- Konikow, L.F.; Kendy, E. Groundwater depletion: A global problem. Hydrogeol. J. 2005, 13, 317–320. [Google Scholar] [CrossRef]
- Charrois, J.W. Private drinking water supplies: Challenges for public health. Can. Med. Assoc. J. 2010, 182, 1061–1064. [Google Scholar] [CrossRef] [Green Version]
- Murphy, H.M.; Thomas, M.K.; Schmidt, P.J.; Medeiros, D.T.; McFadyen, S.; Pintar, K.D.M. Estimating the burden of acute gastrointestinal illness due to Giardia, Cryptosporidium, Campylobacter, E. coliO157 and norovirus associated with private wells and small water systems in Canada. Epidemiol. Infect. 2016, 144, 1355–1370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Flanagan, S.V.; Gleason, J.A.; Spayd, S.E.; Procopio, N.A.; Rockafellow-Baldoni, M.; Braman, S.; Chillrud, S.N.; Zheng, Y. Health protective behavior following required arsenic testing under the New Jersey Private Well Testing Act. Int. J. Hyg. Environ. Health 2018, 221, 929–940. [Google Scholar] [CrossRef]
- Kreutzwiser, R.; de Loë, R.; Imgrund, K.; Conboy, M.J.; Simpson, H.; Plummer, R. Understanding stewardship behaviour: Factors facilitating and constraining private water well stewardship. J. Environ. Manag. 2011, 92, 1104–1114. [Google Scholar] [CrossRef]
- Hynds, P.D.; Misstear, B.D.; Gill, L.W. Unregulated private wells in the Republic of Ireland: Consumer awareness, source susceptibility and protective actions. J. Environ. Manag. 2013, 127, 278–288. [Google Scholar] [CrossRef]
- Flanagan, S.V.; Marvinney, R.G.; Zheng, Y. Influences on domestic well water testing behavior in a Central Maine area with frequent groundwater arsenic occurrence. Sci. Total Environ. 2015, 505, 1274–1281. [Google Scholar] [CrossRef] [Green Version]
- Malecki, K.M.; Schultz, A.A.; Severtson, D.J.; Anderson, H.A.; VanDerslice, J. Private-well stewardship among a general population based sample of private well-owners. Sci. Total. Environ. 2017, 601–602, 1533–1543. [Google Scholar] [CrossRef]
- HSE Health Protection Surveillance Centre. VTEC Infection in Ireland, 2017; HSE HPSC: Dublin, Ireland, 2019. [Google Scholar]
- Óhaiseadha, C.; Hynds, P.D.; Fallon, U.B.; O’Dwyer, J. A geostatistical investigation of agricultural and infrastructural risk factors associated with primary verotoxigenicE. coli(VTEC) infection in the Republic of Ireland, 2008–2013. Epidemiol. Infect. 2017, 145, 95–105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hynds, P.D.; Misstear, B.D.; Gill, L.W. Development of a microbial contamination susceptibility model for private domestic groundwater sources. Water Resour. Res. 2012, 48. [Google Scholar] [CrossRef]
- Hynds, P.; Misstear, B.D.; Gill, L.W.; Murphy, H.M. Groundwater source contamination mechanisms: Physicochemical profile clustering, risk factor analysis and multivariate modelling. J. Contam. Hydrol. 2014, 159, 47–56. [Google Scholar] [CrossRef] [PubMed]
- O’Dwyer, J.; Hynds, P.D.; Byrne, K.A.; Ryan, M.P.; Adley, C.C. Development of a hierarchical model for predicting microbiological contamination of private groundwater supplies in a geologically heterogeneous region. Environ. Pollut. 2018, 237, 329–338. [Google Scholar] [CrossRef]
- Andrade, L.; O’Malley, K.; Hynds, P.; O’Neill, E.; O’Dwyer, J. Assessment of two behavioural models (HBM and RANAS) for predicting health behaviours in response to environmental threats: Surface water flooding as a source of groundwater contamination and subsequent waterborne infection in the Republic of Ireland. Sci. Total Environ. 2019, 685, 1019–1029. [Google Scholar] [CrossRef]
- McDowell, C.P.; Andrade, L.; O’Neill, E.; O’Malley, K.; O’Dwyer, J.; Hynds, P.D. Gender-Related Differences in Flood Risk Perception and Behaviours among Private Groundwater Users in the Republic of Ireland. Int. J. Environ. Res. Public Health 2020, 17, 2072. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Musacchio, A.; Andrade, L.; O’Neill, E.; Re, V.; O’Dwyer, J.; Hynds, P.D. Planning for the health impacts of climate change: Flooding, private groundwater contamination and waterborne infection—A cross-sectional study of risk perception, experience and behaviours in the Republic of Ireland. Environ. Res. 2021, 194, 110707. [Google Scholar] [CrossRef] [PubMed]
- Hooks, T.; Schuitema, G.; McDermott, F. Risk Perceptions Toward Drinking Water Quality Among Private Well Owners in Ireland: The Illusion of Control. Risk Anal. 2019, 39, 1741–1754. [Google Scholar] [CrossRef] [PubMed]
- Xu, L.; Gober, P.; Wheater, H.S.; Kajikawa, Y. Reframing socio-hydrological research to include a social science perspective. J. Hydrol. 2018, 563, 76–83. [Google Scholar] [CrossRef]
- Boudou, M.; Óhaiseadha, C.; Garvey, P.; O’Dwyer, J.; Hynds, P. Flood hydrometeorology and gastroenteric infection: The Winter 2015–2016 flood event in the Republic of Ireland. J. Hydrol. 2021, 599, 126376. [Google Scholar] [CrossRef]
- Hynds, P.; Regan, S.; Andrade, L.; Mooney, S.; O’Malley, K.; DiPelino, S.; O’Dwyer, J. Muddy Waters: Refining the Way Forward for the “Sustainability Science” of Socio-Hydrogeology. Water 2018, 10, 1111. [Google Scholar] [CrossRef] [Green Version]
- Re, V. Incorporating the social dimension into hydrogeochemical investigations for rural development: The Bir Al-Nas approach for socio-hydrogeology. Hydrogeol. J. 2015, 23, 1293–1304. [Google Scholar] [CrossRef] [Green Version]
- Sim, J. Collecting and analysing qualitative data: Issues raised by the focus group. J. Adv. Nurs. 1998, 28, 345–352. [Google Scholar] [CrossRef]
- Krueger, R.A. Focus Groups: A Practical Guide for Applied Research, 3rd ed.; Sage: Newcastle upon Tyne, UK, 2000. [Google Scholar]
- Brod, M.; Tesler, L.E.; Christensen, T.L. Qualitative research and content validity: Developing best practices based on science and experience. Qual. Life Res. 2009, 18, 1263–1278. [Google Scholar] [CrossRef] [PubMed]
- Fox-Rogers, L.; Devitt, C.; O’Neill, E.; Brereton, F.; Clinch, J.P. Is there really “nothing you can do”? Pathways to enhanced flood-risk preparedness. J. Hydrol. 2016, 543, 330–343. [Google Scholar] [CrossRef] [Green Version]
- Devitt, C.; O’Neill, E.; Waldron, R. Drivers and barriers among householders to managing domestic wastewater treatment systems in the Republic of Ireland; implications for risk prevention behaviour. J. Hydrol. 2016, 535, 534–546. [Google Scholar] [CrossRef]
- McLafferty, I. Focus group interviews as a data collecting strategy. J. Adv. Nurs. 2004, 48, 187–194. [Google Scholar] [CrossRef] [PubMed]
- Morse, J.M.; Barrett, M.; Mayan, M.; Olson, K.; Spiers, J. Verification Strategies for Establishing Reliability and Validity in Qualitative Research. Int. J. Qual. Methods 2002, 1, 13–22. [Google Scholar] [CrossRef]
- Nyamathi, A.; Shuler, P. Focus group interview: A research technique for informed nursing practice. J. Adv. Nurs. 1990, 15, 1281–1288. [Google Scholar] [CrossRef]
- Rosenstock, I.M. Historical Origins of the Health Belief Model. Health Educ. Monogr. 1974, 2, 328–335. [Google Scholar] [CrossRef]
- Perreault, J.W.D. Controlling Order-Effect Bias. Public Opin. Q. 1975, 39, 544. [Google Scholar] [CrossRef]
- Colaizzi, P.F. Psychological research as the phenomenologist views it. In Existential-Phenomenological Alternatives for Psychology; Valle, R., King, M., Eds.; Oxford University Press: Oxford, UK, 1978; pp. 48–71. [Google Scholar]
- Nicholls, D. Qualitative research: Part three: Methods. Int. J. Ther. Rehabil. 2017, 24, 114–121. [Google Scholar] [CrossRef]
- Straub, C.L.; Leahy, J.E. Application of a Modified Health Belief Model to the Pro-Environmental Behavior of Private Well Water Testing. JAWRA J. Am. Water Resour. Assoc. 2014, 50, 1515–1526. [Google Scholar] [CrossRef]
- Munene, A.; Lockyer, J.; Checkley, S.; Hall, D.C. Exploring Well Water Testing Behaviour Through the Health Belief Model. Environ. Health Insights 2020, 14, 1–10. [Google Scholar] [CrossRef]
- Akompab, D.A.; Bi, P.; Williams, S.; Grant, J.; Walker, I.A.; Augoustinos, M. Heat Waves and Climate Change: Applying the Health Belief Model to Identify Predictors of Risk Perception and Adaptive Behaviours in Adelaide, Australia. Int. J. Environ. Res. Public Health 2013, 10, 2164–2184. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rainey, R.C.; Harding, A.K. Acceptability of solar disinfection of drinking water treatment in Kathmandu Valley, Nepal. Int. J. Environ. Health Res. 2005, 15, 361–372. [Google Scholar] [CrossRef]
- Janz, N.K.; Becker, M.H. The Health Belief Model: A Decade Later. Health Educ. Q. 1984, 11, 1–47. [Google Scholar] [CrossRef] [Green Version]
- Conner, M. Cognitive Determinants of Health Behavior. Handb. Behav. Med. 2010, 2011, 19–30. [Google Scholar] [CrossRef]
- Orji, R.; Vassileva, J.; Mandryk, R. Towards an Effective Health Interventions Design: An Extension of the Health Belief Model. Online, J. Public Health Inform. 2012, 4, ojphi.v4i3.4321. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davis, R.; Campbell, R.; Hildon, Z.; Hobbs, L.; Michie, S. Theories of behaviour and behaviour change across the social and behavioural sciences: A scoping review. Health Psychol. Rev. 2015, 9, 323–344. [Google Scholar] [CrossRef]
- O’Neill, E.; Brereton, F.; Shahumyan, H.; Clinch, J.P. The Impact of Perceived Flood Exposure on Flood-Risk Perception: The Role of Distance. Risk Anal. 2016, 36, 2158–2186. [Google Scholar] [CrossRef] [PubMed]
- Kelly-Quinn, M.; Blacklocke, S.; Bruen, M.; Earle, R.; O’Neill, E.; O’Sullivan, J.; Purcell, P. Dublin Ireland: A city addressing challenging water supply, management, and governance issues. Ecol. Soc. 2014, 19. [Google Scholar] [CrossRef] [Green Version]
- O’Neill, E.; Devitt, C.; Lennon, M.; Duvall, P.; Astori, L.; Ford, R.; Hughes, C. The Dynamics of Justification in Policy Reform: Insights from Water Policy Debates in Ireland. Environ. Commun. 2018, 12, 451–461. [Google Scholar] [CrossRef]
- Van Vugt, M.; Griskevicius, V.; Schultz, P.W. Naturally Green: Harnessing Stone Age Psychological Biases to Foster Environmental Behavior. Soc. Issues Policy Rev. 2014, 8, 1–32. [Google Scholar] [CrossRef] [Green Version]
- Kollmuss, A.; Agyeman, J. Mind the Gap: Why do people act environmentally and what are the barriers to pro-environmental behaviour? Environ. Educ. Res. 2002, 8, 239–260. [Google Scholar] [CrossRef] [Green Version]
- Jones, A.Q.; Dewey, C.E.; Doré, K.; Majowicz, S.E.; McEwen, S.A.; Waltner-Toews, D.; Henson, S.J.; Mathews, E. Public perception of drinking water from private water supplies: Focus group analyses. BMC Public Health 2005, 5, 129. [Google Scholar] [CrossRef]
- O’Sullivan, J.J.; Bradford, R.A.; Bonaiuto, M.; De Dominicis, S.; Rotko, P.; Aaltonen, J.; Waylen, K.; Langan, S. Enhancing flood resilience through improved risk communications. Nat. Hazards Earth Syst. Sci. 2012, 12, 2271–2282. [Google Scholar] [CrossRef]
- O’Neill, E.; Brennan, M.; Brereton, F.; Shahumyan, H. Exploring a spatial statistical approach to quantify flood risk perception using cognitive maps. Nat. Hazards 2015, 76, 1573–1601. [Google Scholar] [CrossRef]
- Chyzheuskaya, A.; Cormican, M.; Srivinas, R.; O’Donovan, D.; Prendergast, M.; O’Donoghue, C.; Morris, D. Economic Assessment of Waterborne Outbreak of Cryptosporidiosis. Emerg. Infect. Dis. 2017, 23, 1650–1656. [Google Scholar] [CrossRef]
- Aakko, E. Risk communication, risk perception, and public health. WMJ Off. Publ. State Med. Soc. Wis. 2004, 103, 25–28. [Google Scholar]
- Yousaf, O.; Gobet, F. The hypocrisy paradigm. In The Sage Encyclopedia of Political Behavior; Moghaddam, F.M., Ed.; Sage Publications: Newcastle upon Tyne, UK, 2017. [Google Scholar]
- Dickerson, C.A.; Thibodeau, R.; Aronson, E.; Miller, D. Using Cognitive Dissonance to Encourage Water Conservation1. J. Appl. Soc. Psychol. 1992, 22, 841–854. [Google Scholar] [CrossRef]
- Taylor, M.R.; Lamm, A.; Lundy, L.K. Using Cognitive Dissonance to Communicate with Hypocrites About Water Conservation and Climate Change. J. Appl. Commun. 2017, 101, 5. [Google Scholar] [CrossRef] [Green Version]
- Kelleher, L.; Henchion, M.; O’Neill, E. Policy Coherence and the Transition to a Bioeconomy: The Case of Ireland. Sustainability 2019, 11, 7247. [Google Scholar] [CrossRef] [Green Version]
- Hynds, P.; Naughton, O.; O’Neill, E.; Mooney, S. Efficacy of a national hydrological risk communication strategy: Domestic wastewater treatment systems in the Republic of Ireland. J. Hydrol. 2018, 558, 205–213. [Google Scholar] [CrossRef] [Green Version]
- Henwood, K.L.; Pidgeon, N.F. Qualitative research and psychological theorizing. Br. J. Psychol. 1992, 83, 97–111. [Google Scholar] [CrossRef]
- Flyvbjerg, B. Case Study. In The Sage Handbook of Qualitative Research, 4th ed.; Sage: Newcastle upon Tyne, UK, 2011; Chapter 17; pp. 301–316. [Google Scholar]
| County | Host Venue | Coordinates & Elevation | District Flood History | Hydrology, Geology and Topography | Primary Land Use |
|---|---|---|---|---|---|
| Wicklow | Moneystown Community Centre | 53°00’08.1” N 6°11’55.5” W Elevation: 220 m | Small-scale localised flooding | Foothills of Wicklow Mountains. District within Avonmore and Vartry catchments. Principal bedrock: slates and shales, granites GW Vulnerability: High | Forestry and Agriculture |
| Westmeath | Kilcleagh National School | 53°22’27.8” N 7°48’29.1” W Elevation: 50 m | Recurring localised flooding from River Boar in Upper Shannon catchment and at low lying adjacent land (South) after heavy rainfall | Located in low lying terrain of Upper Shannon catchment Principal bedrock: limestones, sandstones, mudstones GW Vulnerability: Variable (Medium, High) | Bogland and Agriculture |
| Dublin | Larch Hill Scout Centre | 53°15’14.0” N 6°17’03.6” W Elevation: 225 m | Recurring fluvial flooding from stream Incidences of small-scale localised flooding | Foothills of Dublin Mountains and primarily within River Dodder. Principal bedrock: granites GW Vulnerability: High | Forestry and Agriculture |
| Clare | Clonlara GAA Club | 52°43’13.2” N 8°33’31.4” W Elevation: 19 m | Extensive & recurring fluvial flooding in Lower Shannon. | Located in low lying terrain in Lower Shannon catchment Principal bedrock: limestones GW Vulnerability: Variable (Medium, High, Extreme (Karst)) | Agriculture |
| Themes | Thematic Descriptor |
|---|---|
| General Thoughts on Well Water Quality | Participants’ perceptions regarding their own well water quality and factors influencing their relative confidence in their well water |
| Flooding Experience and Perceived Threat | Participants’ past flood experience and their perception of the level of flood risk that their well is exposed |
| Cues to Action | Factors that mobilise participants to take action to protect themselves from waterborne health risks |
| Perceived Benefits and Barriers | Benefits that participants perceive from protecting themselves against waterborne health risk from well-contaminants; and the barriers they report hindering them in protecting themselves against those risks |
| Self Efficacy | Participants’ confidence in their ability to test their well water and/or install water treatments |
| Health Behaviours Following Floods | Participants’ intentions and responses after flood water inundation of their well |
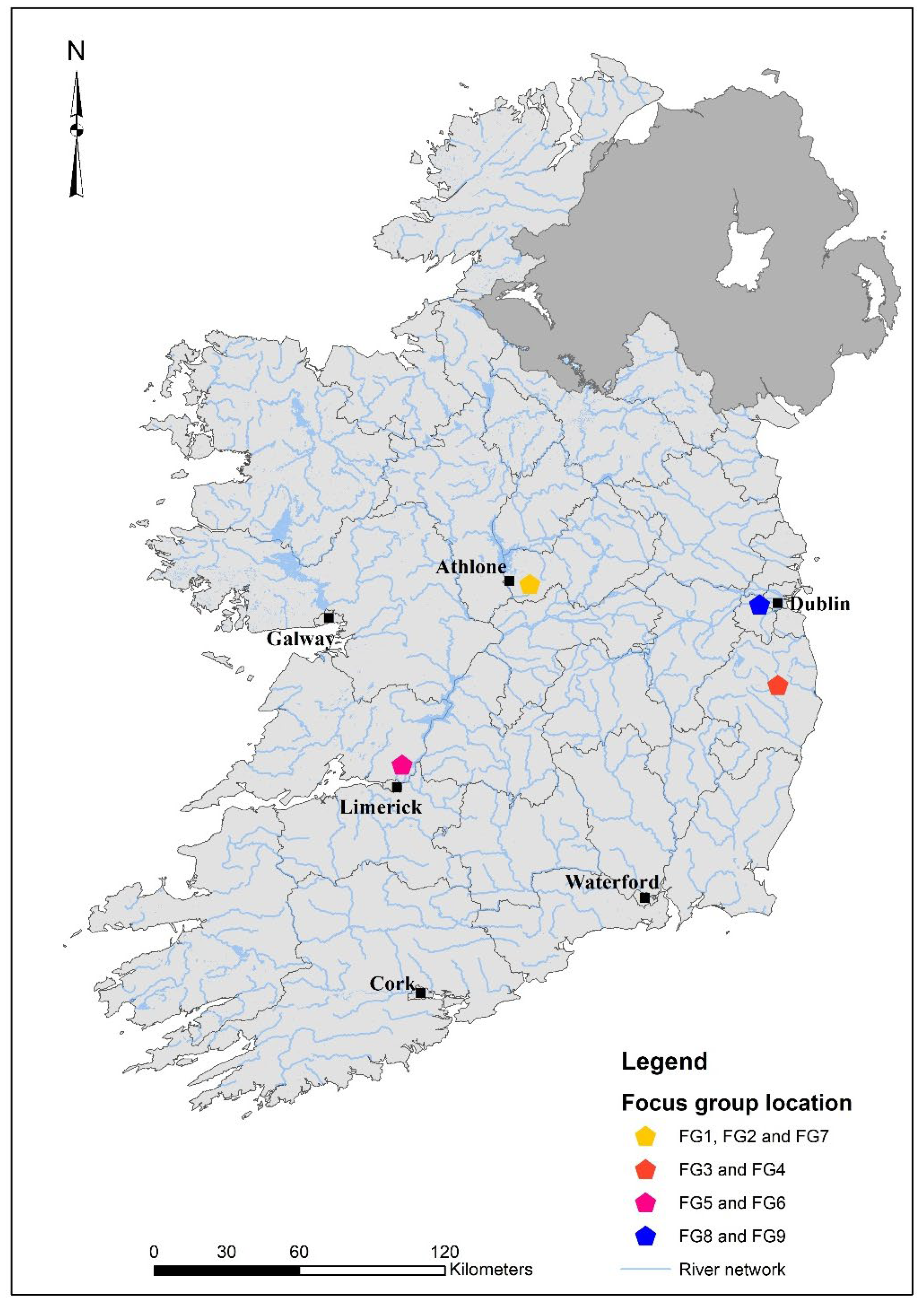
| Focus Group | Date (2018) | Location (See Figure 2) | Recruitment Strategy | n (Targeted Households) | n (Participants) | Session Length (mm:ss) |
|---|---|---|---|---|---|---|
| FG1 | 28/04 | Westmeath | Letters | 100 | 9 | 71:25 |
| FG2 | 28/04 | Westmeath | Letters | 100 | 2 | 24:07 |
| FG3 | 05/05 | Clare | Letters | 100 | 6 | 62:25 |
| Clare | Letters | 100 | - | - | ||
| FG5 | 07/06 | Wicklow | Local recruiter | - | 6 | 64:27 |
| Wicklow | Local recruiter | - | - | - | ||
| FG7 | 23/06 | Westmeath | Local recruiter | - | 4 | 73:47 |
| FG8 | 18/07 | Dublin | Letters | 60 | 8 | 44:23 |
| Dublin | Letters | 60 | - | - |
| Focus Group | n (Male/ Female) | Own the Property They Live on | Children <10 Years in Household | Drink Well Water | Well Water Treatment Installed | Experienced Floods near Their Wells in the Past | Total |
|---|---|---|---|---|---|---|---|
| FG1 | 6/3 | 9 | 0 | 9 | 0 | 3 | 9 |
| FG2 | 0/2 | 2 | 0 | 2 | 0 | 0 | 2 |
| FG3 | 3/3 | 6 | 2 | 5 | 2 | 0 | 6 |
| FG5 | 3/3 | 6 | 3 | 6 | 2 | 4 | 6 |
| FG7 | 3/1 | 4 | 0 | 2 | 1 | 0 | 4 |
| FG8 | 4/4 | 7 | 1 | 8 | 0 | 1 | 8 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
McDowell, C.P.; Andrade, L.; Re, V.; O’Dwyer, J.; Hynds, P.D.; O’Neill, E. Exploring Risk Perception and Behaviours at the Intersection of Flood Events and Private Groundwater Supplies: A Qualitative Focus Group Study. Water 2021, 13, 3467. https://doi.org/10.3390/w13233467
McDowell CP, Andrade L, Re V, O’Dwyer J, Hynds PD, O’Neill E. Exploring Risk Perception and Behaviours at the Intersection of Flood Events and Private Groundwater Supplies: A Qualitative Focus Group Study. Water. 2021; 13(23):3467. https://doi.org/10.3390/w13233467
Chicago/Turabian StyleMcDowell, Cillian P., Luisa Andrade, Viviana Re, Jean O’Dwyer, Paul D. Hynds, and Eoin O’Neill. 2021. "Exploring Risk Perception and Behaviours at the Intersection of Flood Events and Private Groundwater Supplies: A Qualitative Focus Group Study" Water 13, no. 23: 3467. https://doi.org/10.3390/w13233467