
Potential Health Risk of Dust from Stone Mill Industries



Abstract
1. Introduction
2. Materials and Methods
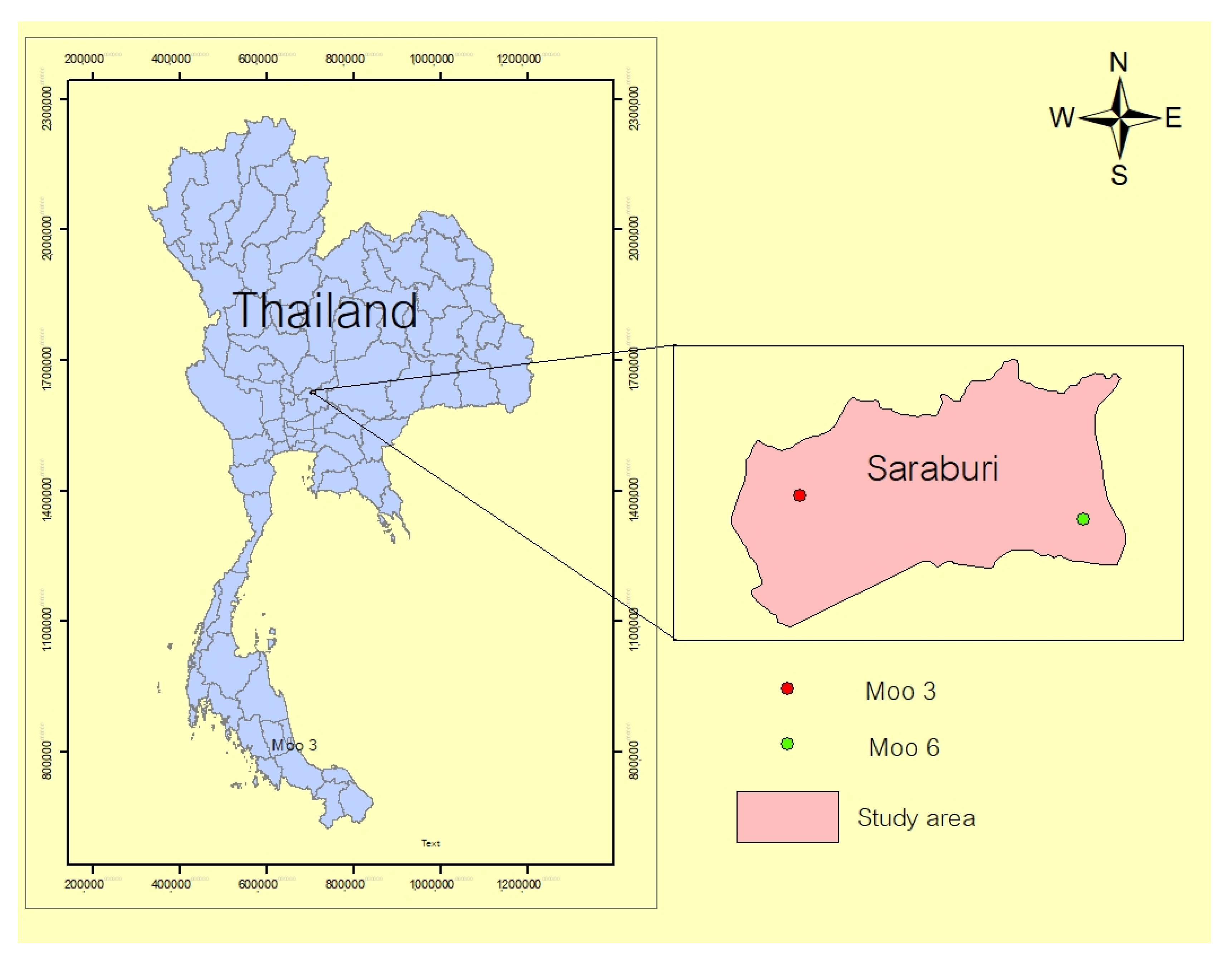
2.1. Study Area and Population Frame
2.2. Questionnaire
2.3. Air Quality Data
2.4. Health Risk Assessment
2.5. Statistical Analysis
3. Results
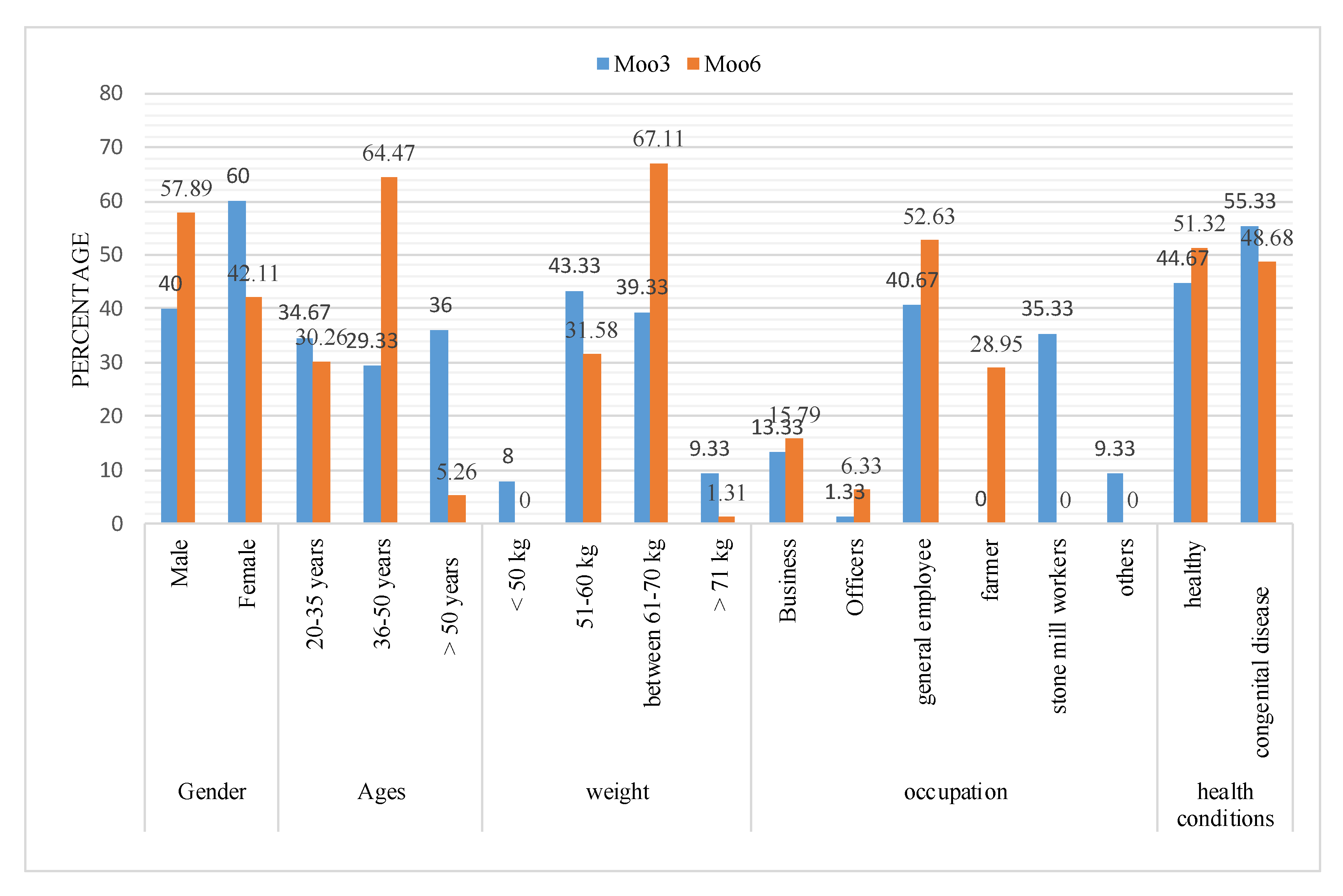
3.1. Population Conditions in the Study Areas
3.2. Environment and Personal Behavior Related to Underlying Disease
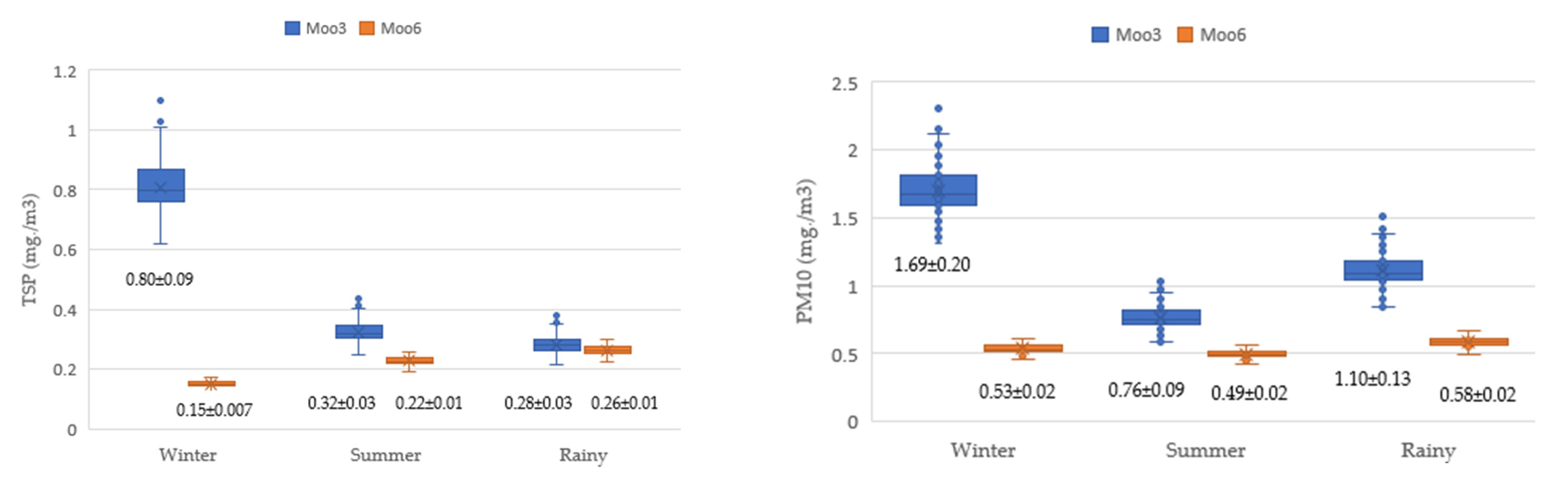
3.3. Air Quality
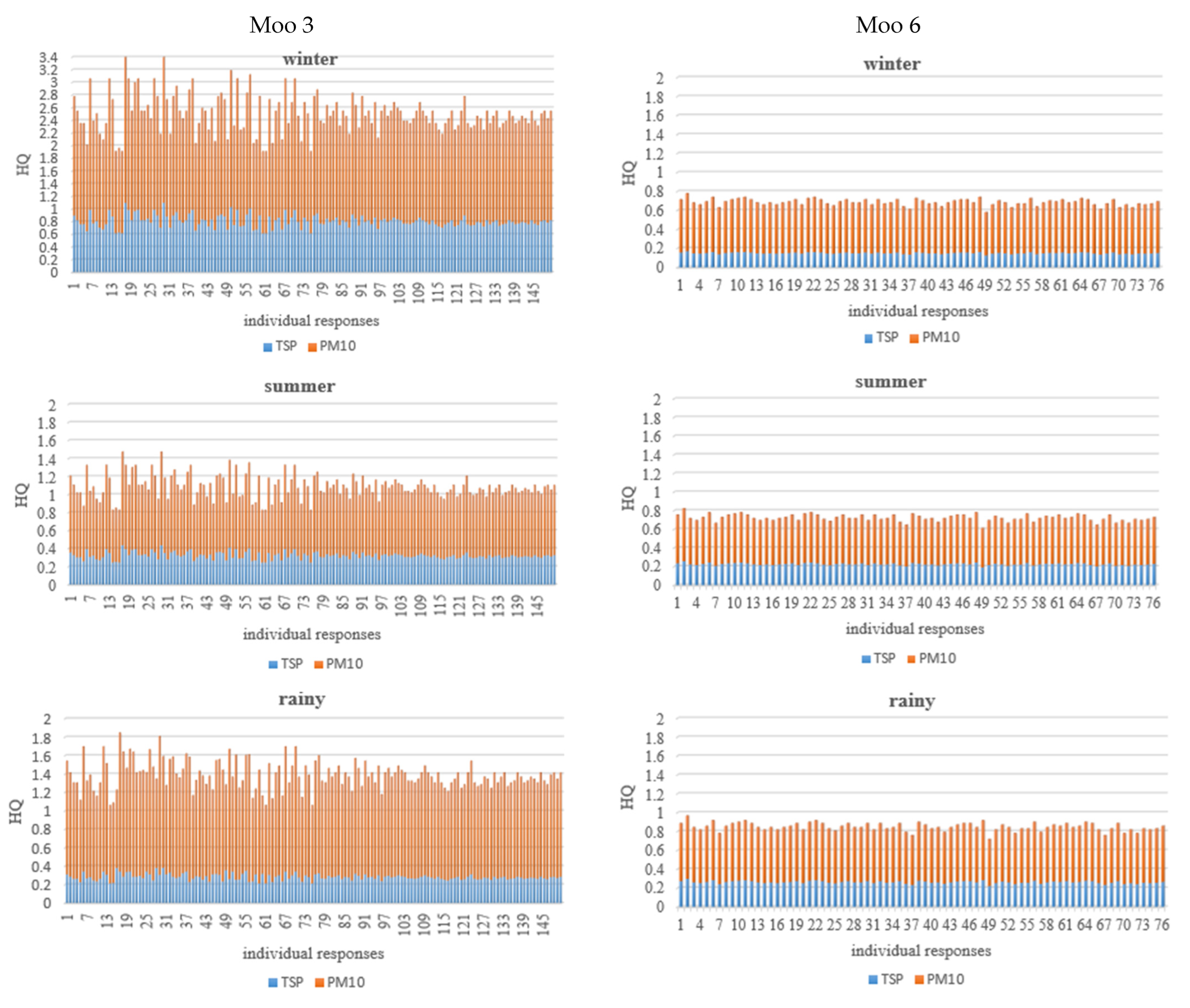
3.4. Health Risk Assessment
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| PM | Particulate matter |
| TSP | Total suspended particulate |
| HQ | Hazard quotient |
| Rfc | Reference concentration |
| EIA | Environmental impact assessment |
| EIS | Environmental impact statement |
| WHO | World Health Organization |
| DPIM | Department of Primary Industries and Mines |
| ONEP | Office of Natural Resources and Environmental Policy and Planning |
References
- Nawaz, M.O.; Henze, D.K.; Anenberg, S.C.; Ahn, D.Y.; Goldberg, D.L.; Tessum, C.W.; Chafe, Z.A. Sources of air pollution-related health impacts and benefits of radially applied transportation policies in 14 US cities. Front. Sustain. Cities 2023, 5, 1102493. [Google Scholar] [CrossRef]
- Patterson, G. The environmental impact of grain processing technologies. Environ. Sci. Ind. Rev. 2018, 22, 200–215. [Google Scholar]
- Silva, L.S.; Amario, M.; Stolz, C.M.; Figueiredo, K.V.; Haddad, A.N. A comprehensive review of stone dust in concrete: Mechanical behavior, durability, and environmental performance. Buildings 2023, 13, 1856. [Google Scholar] [CrossRef]
- Leuenberger, A.; Winkler, M.S.; Cambaco, O.; Cossa, H.; Kihwele, F.; Lyatuu, I.; Zabré, H.R.; Farnham, A.; Macete, E.; Munguambe, K. Health impacts of industrial mining on surrounding communities: Local perspectives from three sub-Saharan African countries. PLoS ONE 2021, 16, e025433. [Google Scholar] [CrossRef] [PubMed]
- Jenwitheesuk, K.; Peansukwech, U. Construction of polluted aerosol in accumulation that affects the incidence of lung cancer. Heliyon 2020, 6, e03337. [Google Scholar] [CrossRef]
- Foocharoen, C.; Peansukwech, U.; Pongkulkiat, P. Aerosol components associated with hospital mortality in systemic sclerosis: An analysis from a nationwide Thailand healthcare database. Sci. Rep. 2021, 11, 7983. [Google Scholar] [CrossRef]
- Smallwood, J.M. Implementation International Environmental Law and Policy: An Interactive Approach to Environmental Regulation; Routledge: London, UK, 2024; p. 232. [Google Scholar]
- Dantrakula, A.; Swangjang, K.; Pumakjanchana, O. Study of particulate in the stone mill industry; case study Tambol Na Phra Lan, Saraburi. In Proceedings of the in Management in Disruptive Technologies National Conference of Rachamongkol Technology University, Online, Thailand, 27 May 2022; pp. 656–662. [Google Scholar]
- Department of Primary Industries and Mines. In Thai. Available online: https://www.dpim.go.th (accessed on 15 July 2024).
- Office of Natural Resources and Environmental Policy and Planning. Government Gazette: Project types and sizes required Environmental Impact Assessment. Number 136 Section 3 on 4 January 2562. Bangkok Thailand (In Thai). Available online: https://www.onep.go.th (accessed on 15 July 2024).
- Thailand Mineral Act, BE 2560. 2017. Available online: https://www.dpim.go.th/en/media/002_2560.pdf (accessed on 15 December 2024).
- Nikam, J.; Archer, D.; Nopsert, C. Regulating Air Quality in Thailand: A Review Policies. SEI Policy Brief. Stockholm Environmental Institute. 2021. Available online: https://www.sei.org/publications/regulating-air-quality-in-thailand-a-review-of-policies/ (accessed on 9 November 2024).
- Rughooputh, S.P.; Rughooputh, M.S.; Guo, Y.; Rong, Y.; Chen, W. Occupational exposure to silica dust and risk of lung cancer: An updated meta-analysis of epidemiological studies. BMC Public Health 2016, 16, 1137. [Google Scholar] [CrossRef]
- Samana, K.; Ketsakorn, A. Health risk assessment of inhalation exposure to respirable dust among workers in stone mill, Saraburi Province. Dis. Control. J. 2023, 49, 167–178. [Google Scholar] [CrossRef]
- Jaber, H.M.; Mohamed, M.S.; El-Safty, A.M.; El-Salamoni, O.K.; Ibrahim, H.M.; El-Din, W.S. Pulmonary Problems among stone cutting workers in West Bank-Palestine. Med. J. Cairo Univ. 2015, 83, 1. Available online: www.medicaljournalofcairouniversity.net (accessed on 20 March 2023).
- Krejcie, R.V.; Morgan, D.W. Determining sample size for research activities. Educ. Psychol. Meas. 1970, 30, 607–610. [Google Scholar] [CrossRef]
- Thai Meteorological Department. In Thai. Available online: https://www.tmd.go.th (accessed on 6 February 2025).
- United States Environmental Protection Agency. United States Environmental Protection Agency, EPA Human Health Risk Assessment Guidance; United States Environmental Protection Agency: Washington, DC, USA, 1991.
- World Health Organization. Ambient Outdoor Air Pollution. Available online: https://www.who.int./news-room/fact-sheets/detail/ambient-(outdoor)-air-quality-and-health (accessed on 20 March 2023).
- United States Environmental Protection Agency. The Risk Assessment Guidelines of 1986; USEPA EPA/600/8-87/045; United States Environmental Protection Agency: Washington, DC, USA, 1987.
- Zheng, H.; Csemezová, J.; Loomans, M.; Walker, S.; Gauvin, F.; Zeiler, W. Species profile of volatile organic compounds emission and health risk assessment from typical indoor events in daycare centers. Sci. Total Environ. 2024, 918, 170734. [Google Scholar] [CrossRef] [PubMed]
- Saraburi Town & Country Planning. In Thai. Available online: https://ratchakitcha.soc.go.th/documents/1912656.pdf (accessed on 15 January 2024).
- Zhang, H.; Hu, J.; Ying, Q.; Hu, X.M. Relationships between meteorological parameters and criteria air pollutants in three megacities in China. Environ. Res. 2015, 140, 242–254. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Ji, Z.; Kang, S.; Zhang, Q.; Chen, X. Spatiotemporal variations of air pollutants in western China and their relationship to meteorological factors and emission sources. Environ. Pollut. 2019, 254 Pt A, 112952. [Google Scholar] [CrossRef]
- Hu, M.; Wang, Y.; Wang, S.; Jiao, M.; Huang, G. Spatial-temporal heterogeneity of air pollution and its relationship with meteorological factors in the Pearl River Delta, China. Atmos. Environ. 2021, 254, 118415. [Google Scholar] [CrossRef]
- Aladag, E. The influence of meteorological factors on air quality in the province of Van, Turkey. Water Air Soil Pollut. 2023, 234, 259. [Google Scholar] [CrossRef]
- Çelik, M.B.; Kadı, İ. The relation between meteorological factors and pollutants concentrations in Karabük city. Gazi Univ. J. Sci. 2007, 20, 87–95. [Google Scholar]
- Danek, T.; Weglinska, E.; Zareba, M. The influence of meteorological factors and terrain on air pollution concentration and migration: A geostatistical case study from Krakow, Poland. Sci. Rep. 2022, 12, 11050. [Google Scholar] [CrossRef]
- Tian, Y.; Yao, X.A.; Mu, L.; Fan, Q. Integrating meteorological factors for better understanding of the urban form-air quality relationship. Landsc. Ecol. 2020, 35, 2357–2373. [Google Scholar] [CrossRef]
- Li, R.; Wang, Z.; Cui, L.; Fu, H.; Zhang, L. Air pollution characteristics in China during 2015–2016: Spatiotemporal variations and key meteorological factors. Sci. Total Environ. 2019, 648, 902–915. [Google Scholar] [CrossRef]
- Chen, C.H.; Tsai, P.J.; Chang, W.W.; Chen, C.Y.; Chen, C.Y.; Yates, D.; Guo, Y.L. Dose-response relationship between lung function and chest imaging response to silica exposures in artificial stone manufacturing workers. Environ. Health 2024, 23, 25. [Google Scholar] [CrossRef]
- Choudhary, A.; Kumar, P.; Pradhan, C.; Sahu, S.K.; Chaudhary, S.; Joshi, P.K.; Pandey, D.N.; Prakash, D.; Mohanty, A. Environmental and health impacts of air pollution: A review. Front. Environ. Sci. 2023, 11, 1132159. [Google Scholar] [CrossRef]
- Swangjang, K.; Cumkett, S. Mitigation Hierarchy; An Effectiveness of Project Control Mechanism. In Handbook of Advanced Approaches Towards Pollution Prevention and Control; Rahman, R.O.A., Hussain, C.M., Eds.; Elsevier: New York, NY, USA, 2021; Volume 1, pp. 235–240. [Google Scholar]
- Swangjang, K. Comparative review of EIA in the Association of Southeast AsianNations. Environ. Impact Assess. Rev. 2018, 78, 33–42. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Stone Mills | Number of Monitoring Station | Monitoring Frequencies (per Year) ** |
|---|---|---|
| 1 | 4 | 2 |
| 2 | 7 | 2,1 |
| 3 | 5 * | 2 |
| 4 | 5 | 2 |
| 5 | 5 | 2 |
| 6 | 6 | 2 |
| 7 | 3 | 2 |
| Factors | Units | Sources |
|---|---|---|
| Concentration of TSP and PM10 (C) | mg·m−3 | Monitoring reports of stone mill industries |
| Inhalation rate (IR) | 0.83 m3·h−1 for adults 0.208 m3·h−1 for children | US EPA (1987) [20] |
| Exposure time (ET) | h·day−1 | Questionnaire |
| Exposure frequency (EF) | day·year−1 | Questionnaire |
| Exposure duration (ED) | Year | Questionnaire |
| Body weight of the exposed individual (BW) | kg | Questionnaire |
| Time period over which the dose was averaged (AT) | Day | Questionnaire |
| Environment and Personal Behavior | Underlying Disease (N: Percentage) | Non-Underlying Disease (N: Percentage) | χ2 | p-Value |
|---|---|---|---|---|
| Smoking | 09: 13.4 | 59: 26.6 | 60.162 | <0.00 ** |
| Pollution prevention | ||||
| -Mask use | 13: 06.7 | 06: 33.3 | 28.223 | <0.00 ** |
| -Staying indoors | 30: 30.6 | 03: 09.4 | ||
| Distance from stone mill | ||||
| 1–300 m | 02: 47.2 | 07: 52.8 | 30.711 | <0.00 ** |
| 301–500 m | 31: 30.9 | 03: 09.1 | ||
| More than 500 m | 22: 34.4 | 43: 05.6 | ||
| Distance from road | ||||
| 1–100 m | 13: 52.1 | 07: 47.9 | 2.682 | 0.262 |
| 101–300 m | 08: 10.0 | 03: 30.0 | ||
| More than 300 m | 34: 44.7 | 42: 55.3 | ||
| House characteristics | ||||
| Single floor | 37: 46.4 | 112: 100 | 18.06 | <0.00 ** |
| More than one floor | 17: 53.6 |
| Factors | Moo 3 (N: Percentage) | Moo 6 (N: Percentage) | p-Value |
|---|---|---|---|
| Underlying diseases | 83: 55.33% | 37: 48.68% | 0.344 |
| Smoking | 40: 26.67% | 27: 35.53% | 0.1683 |
| Pollution-prevention awareness | 35: 23.33% | 15: 19.74% | 0.5383 |
| Housing distance from stone mills | |||
| 1–300 m | 129: 86% | 0 | 0.001 ** |
| 301–500 m | 21: 14% | 12: 15.79% | |
| More than 500 m | 0 | 64: 84.21% | |
| Housing distance from road | |||
| 1–100 m | 140: 93.33% | 72: 94.74% | 0.6792 |
| 101–300 m | 10: 6.67% | 4: 5.26% | |
| House characteristics | |||
| Single floor | 146: 97.33% | 62: 81.58% | 0.001 ** |
| More than one floor | 4: 2.67% | 14: 18.42% |
| Hazard Risk | Areas | Winter | Summer | Rainy | |||
|---|---|---|---|---|---|---|---|
| HQ (Mean ± SD) | t-Test | HQ (Mean ± SD) | t-Test | HQ (Mean ± SD) | t-Test | ||
| TSP | Moo 3 | 0.808 ± 0.097 | 82.940 ** | 0.322 ± 0.038 | 28.026 ** | 0.281 ± 0.033 | 5.538 ** |
| Moo 6 | 0.150 ± 0.008 | 0.227 ± 0.115 | 0.263 ± 0.014 | ||||
| PM10 | Moo 3 | 1.696 ± 0.202 | 69.033 ** | 0.763 ± 0.091 | 33.397 ** | 1.108 ± 0.132 | 46.149 ** |
| Moo 6 | 0.535 ± 0.027 | 0.497 ± 0.025 | 0.585 ± 0.030 | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Swangjang, K.; Dantrakul, A.; Panishkan, K. Potential Health Risk of Dust from Stone Mill Industries. Atmosphere 2025, 16, 230. https://doi.org/10.3390/atmos16020230
Swangjang K, Dantrakul A, Panishkan K. Potential Health Risk of Dust from Stone Mill Industries. Atmosphere. 2025; 16(2):230. https://doi.org/10.3390/atmos16020230
Chicago/Turabian StyleSwangjang, Kanokporn, Arnol Dantrakul, and Kamolchanok Panishkan. 2025. "Potential Health Risk of Dust from Stone Mill Industries" Atmosphere 16, no. 2: 230. https://doi.org/10.3390/atmos16020230
APA StyleSwangjang, K., Dantrakul, A., & Panishkan, K. (2025). Potential Health Risk of Dust from Stone Mill Industries. Atmosphere, 16(2), 230. https://doi.org/10.3390/atmos16020230