1. Introduction
The prevalence of allergic diseases has increased worldwide over the past few decades. In the 1990s, the ECRHS (the European Community Respiratory Health Survey) surveyed the prevalence of asthma in 22 European countries and found that with the development of urbanization, the prevalence of asthma was increasing year by year [
1]. In Chinese Taipei, Hsieh and Tsai [
2] examined the prevalence of allergic diseases in school children aged 7 to 15 years and found that the prevalence of childhood asthma increased from 1.3% in 1974 to 5.1% in 1985 and 5.8% in 1991. In Guangzhou, China, a survey among school-aged children found that the prevalence of asthma has doubled over the past 15 years [
3]. In the process of exploring the rising incidence of allergic diseases, indoor environmental exposure has received extensive attention. Endotoxins are ubiquitous in indoor environments and serve as important components of active ingredients in indoor dust. Endotoxins are the lipopolysaccharide components of the outer membrane of Gram-negative bacteria and have strong immunostimulatory and pro-inflammatory properties [
4]. It is of great significance to explore endotoxin exposure and its health effects.
Endotoxin concentrations in household dust have been investigated in some studies and geographical variations have been observed. The International Study of Asthma and Allergy in Children (ISAAC II) reported a fivefold difference in the endotoxin concentration in house dust between Rome, Italy and Linkoping, Sweden [
5]. A multi-center study conducted across 22 study centers from 10 European countries found that the median endotoxin concentration in mattress dust ranged from 772 EU/g in Reykjavik, Iceland, to 4806 EU/g in Turin, Italy [
6]. In China, previous research on household endotoxins has primarily focused on southern regions such as Guangzhou and Hong Kong [
7,
8]. However, to our knowledge, endotoxin concentrations in household dust in northern China have not been reported previously.
Aiming to enhance the comprehension of endotoxins, numerous studies have been conducted to investigate the determinants of endotoxins in household dust. These studies have indicated various factors, including the dwelling type, dwelling location, occupant density, household cleaning frequency, use of air conditioners, environmental tobacco smoking and pet ownership [
6,
7,
9,
10,
11,
12,
13,
14,
15,
16]. It has been demonstrated by Giovannangelo et al. [
12] that the determinants of endotoxins vary across countries. Our understanding in this area is limited in China, as only one study conducted in Hong Kong has reported the determinants of household endotoxins [
7].
Exposure to endotoxins might induce an inflammatory response, leading to the development of allergy-related diseases [
17]. However, previous observational studies that have examined the associations of endotoxin concentrations with asthma and allergic symptoms in children did not provide a consistent picture, with reports of a protective role of endotoxin exposure [
10,
18,
19], a higher risk and severity of disease in those who were exposed at elevated levels [
20,
21,
22] and no influence of exposure on disease [
14,
23].
Considering the limited information on endotoxins in Chinese households and inconsistent findings regarding its impact on asthma and allergies in children, the present study aims to describe the concentrations and determinants of endotoxins in household dust in northern China, as well as investigate their associations with asthma, rhinitis and eczema among children.
2. Methods
This study was part of the project “CCHH (China, Children, Health, Home)” in Tianjin region. Tianjin is located approximately 130 km away from Beijing and covers an area of 11,966.45 square kilometers with a resident population of 13.64 million [
24]. The average outdoor air temperatures for spring, summer, autumn and winter are 13.4 °C, 25.7 °C, 13.6 °C and −1.7 °C in Tianjin [
25]. The outdoor average relative humidities range from 52% in spring to 72% in summer [
26]. The CCHH study consisted of two phases. The first phase (May 2013–December 2014) was a cross-sectional questionnaire survey, which collected information on children’s and family background, building characteristics, dampness problems, personnel activities as well as the health status of children. In the second phase (September 2013–January 2016), home inspections were conducted to collect dust samples and to measure indoor environmental parameters such as indoor temperature, relative humidity and ventilation. This paper focuses on 324 inspected homes in urban Tianjin.
2.1. Dust Collection and Endotoxin Analysis
Dust samples were collected from children’s bedroom floors using filter socks mounted on a mouthpiece connected to a household vacuum cleaner. A minimum of 100 mg dust was collected for each sample. The filter sock was then detached and wrapped in aluminum foil. The samples were transported to the laboratory and stored in a freezer at −20 °C until analysis.
For endotoxin analysis, dust was extracted in pyrogen-free water with 0.05% Tween for 40 min centrifuged and the supernatant was removed and assayed. Endotoxins were analyzed by Limulus Amebocyte Lysate (LAL) assay according to the manufacturer’s protocol (GenScript, Inc., Piscataway, NJ, USA). All endotoxin levels were within the limits of detection of the assay. The resulting endotoxin unit (EU) per mL values were converted into EU/g dust.
2.2. Building Characteristics, Environmental Parameters and Personnel Activities in Homes
Information on building characteristics, self-reported indoor environmental parameters and personnel activities were collected in the first phase through questionnaires. The questionnaire details have been previously published [
27]. The measurement of indoor environmental parameters was conducted during home inspection. Portable CO
2 monitors (AZ
® 7798, Taiwan, China) were placed in the living room and bedrooms to continuously monitor indoor temperature, relative humidity and CO
2 concentration for at least 24 h with sampling interval of one minute. We used CO
2 produced by the occupants during sleep as a tracer gas to calculate ventilation rate at night. The detailed method has been described previously [
28]. Absolute humidity (
AH, g/m
3) was calculated as a function of relative humidity (
RH, %) and temperature (
T, °C) using the following empirical equation [
29]:
2.3. Asthma and Allergy of Investigated Children
Asthma and allergic symptoms among children were self-reported by parents through the questionnaire survey. These questions were identical to those used in the ISAAC study [
30]. We used the diagnosis of disease and the related symptoms in the last 12 months to categorize current asthma, current rhinitis and current eczema, while children without any allergic symptoms were defined as controls, as shown below,
Current asthma: “child has been diagnosed with asthma by a doctor” and “child has had wheezing or whistling in the chest in the last 12 months”.
Current rhinitis: “child has been diagnosed with hay fever or allergic rhinitis by a doctor” and “child has had a problem with sneezing, or a runny, or a blocked nose in the last 12 months when he/she has not had a cold or the flu”.
Current eczema: “child has been diagnosed with eczema by a doctor” and “child has had eczema symptoms in the last 12 months”.
This study was approved by the research office at Tianjin University. Guardian of participants provided written informed consent to participate in this study.
2.4. Statistical Analysis
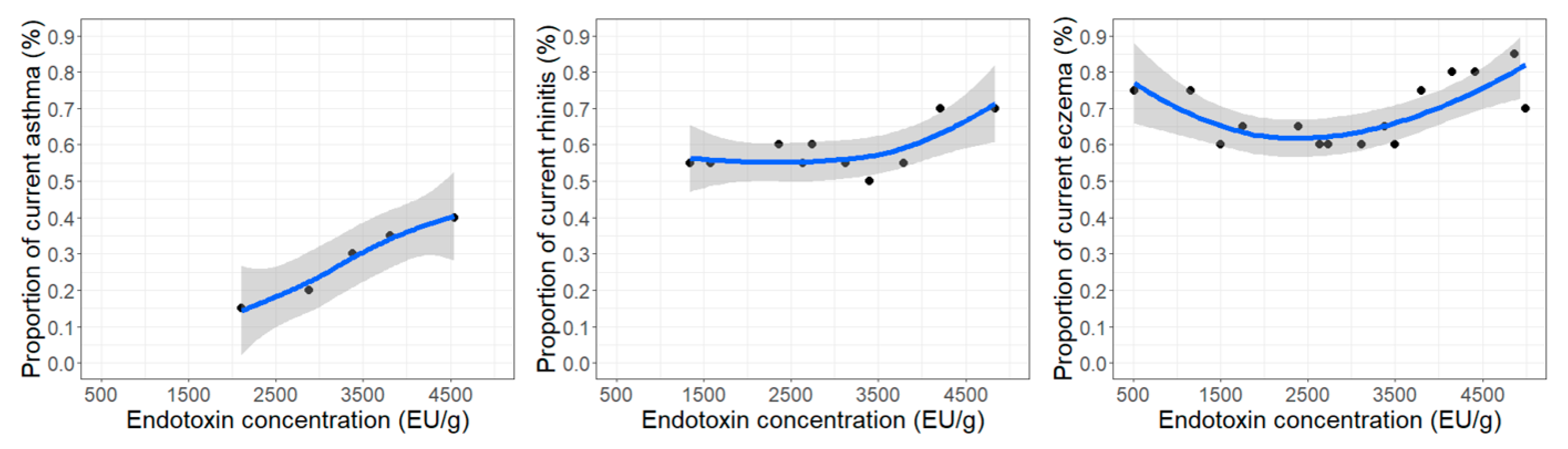
Endotoxin concentrations were normally distributed and expressed as mean and standard deviation (SD). The associations between endotoxin concentrations in household dust and determinants were investigated using linear regression analysis. The mutual effect of determinants that showed marginal significant associations (p < 0.1) with endotoxin concentrations were further explored in multivariate linear regression model. Locally weighted regression smoothing plots were used to exhibit the variation of proportion of asthma and allergies among investigated children with endotoxin concentrations. Logistic regression models were performed to estimate odds ratios (ORs) of endotoxin for health outcomes in children with adjustment for gender, age and family allergic history. Endotoxin concentration was treated as a dichotomized variable (below vs. above median). p-values less than 0.05 were accepted as significant. Statistical analysis was performed with SPSS 26.
4. Discussion
In this study, we found a positive association between endotoxin concentrations and children’s current asthma. Endotoxin concentrations in bedroom floor dust were associated with the age of the house, cleaning frequency and ventilation system.
In 324 inspected homes in urban Tianjin, we observed a wide range of endotoxin concentrations in dust samples collected from children’s bedrooms, ranging from 94 to 11,625 EU/g, with a mean concentration of 3638 EU/g. Comparing the endotoxin concentrations between our study and other Chinese studies was challenging due to limited household studies in China and variations in the units used for measuring endotoxin, with EU/m
2 [
8] and ng/mg dust [
31] being employed while we utilized EU/g. Given the strong pro-inflammatory and immunostimulatory properties of endotoxins, further investigations employing a standardized approach are warranted to characterize endotoxins in Chinese households. The endotoxin concentrations in bedroom floor dust in our study were lower than those reported by previous studies conducted in other countries, with geometric means of 7300 EU/g in Germany [
32], 35,300 EU/g in the USA [
33], 9244 EU/g in New Zealand [
20], 5700 EU/g in Sweden [
14] and 31,100 EU/g in Denmark [
13].
In this study, we found a clear positive trend between endotoxin concentrations and the proportion of current asthma in children. Additionally, we observed a significant association between high endotoxin concentrations and an increased risk of current asthma in children (AOR: 9.68, 95% CI: 1.01–92.45). Our results indicate that endotoxins in household dust may be a risk factor for current asthma in children, which is consistent with some of the previous studies [
20,
21,
22]. One potential mechanism is that alveolar macrophages in the airways produce a wide variety of cytokines and express functional CD14 and Toll-like receptors, which recognize endotoxins and can induce inflammatory responses [
34].
The determinants of endotoxin concentrations in household dust were explored to identify effective control measures. Both one-determinant regression and mutual effect models revealed a positive association between the age of the house and the endotoxin concentration, consistent with Gehring et al.’s [
10] findings of higher endotoxin levels in “old” houses. One possible explanation is that endotoxins accumulate over time [
10]. Another possibility could be that older houses serve as an indicator of poor housing quality, as we have previously reported a significant association between older houses and dampness indicators [
35]. Dampness indicators were positively related to endotoxin exposure (See
Table 5, self-reported dampness). Additionally, exhaust fans were less frequently installed in older houses (>20 years: 77.3% vs. <10 years: 47.4%). Significantly lower endotoxin concentrations were observed in those houses equipped with exhaust fans in the present study. Therefore, older houses require maintenance to control endotoxins, such as reducing dampness problems and installing exhaust fans to improve ventilation.
We found that homes equipped with exhaust fans and frequently opened windows had significantly lower concentration of endotoxins. The same patterns were also observed in the mutual effect analysis. A study conducted in Nanjing, China, found that both airborne endotoxins and endotoxins in dust were lower in the outdoor environment than those in the home environment [
31]. An outdoor to indoor airflow might dilute the endotoxins in the home environment. This influence of ventilation on the indoor endotoxin concentration was also observed by Bischof et al. [
9], who reported a significant negative association between ventilation and endotoxin concentrations in living room floor dust. Therefore, ventilation may serve as an effective strategy for controlling endotoxins indoors.
We observed a significant increase in endotoxin levels in bedrooms with frequent cleaning. The association between endotoxin concentrations and cleaning frequency were contradictory in previous studies. Bischof et al. [
9] observed an association between elevated endotoxin concentrations and infrequent vacuum cleaning, whereas Moniruzzaman et al. [
14] identified an association between frequent vacuum cleaning and higher endotoxin concentrations. These two studies primarily focused on the frequency of vacuum cleaning, while wet mopping emerged as the most predominant cleaning method employed in children’s bedroom (86%) in our study. Smedje and Norback [
36] reported that the wet mopping of floors increased the airborne concentrations of viable bacteria. We speculate that frequent wet mopping facilitates bacteria growth and increases endotoxin concentrations in dust. The influence of cleaning frequency and endotoxins, considering the cleaning method, requires further investigation.
We noticed a significant inverse association between the absolute humidity and endotoxin levels. In the mutual effect model, although not statistically significant, there was still a negative trend between the absolute humidity and endotoxins. A previous study reported a significant association between a low relative humidity and high endotoxin concentrations [
16]. The authors argued that measuring the relative humidity on a single day may be a poor measure of the usual indoor conditions, leading to potential misclassification. Some studies have not found an association between the air’s relative humidity and the endotoxin concentration [
9,
14,
37]. However, a study conducted in New Zealand revealed a significant positive association between the carpet-based relative humidity and endotoxin concentrations in living room floor dust [
38]. The association between endotoxins and air relative humidity as well as surface relative humidity requires further investigation through extended-duration measurements.


 and
and 

{kind=link}