
Study on the Health Effect of Temperature on Cardiovascular and Cerebrovascular Diseases in Haikou City

Abstract
1. Introduction
2. Materials and Methods
2.1. Data Sources
2.2. Research Methods
2.2.1. Descriptive Analysis
2.2.2. Distributed-Lag Nonlinear Model (DLNM)
2.2.3. Subgroup Analysis
3. Results
3.1. Basic Information
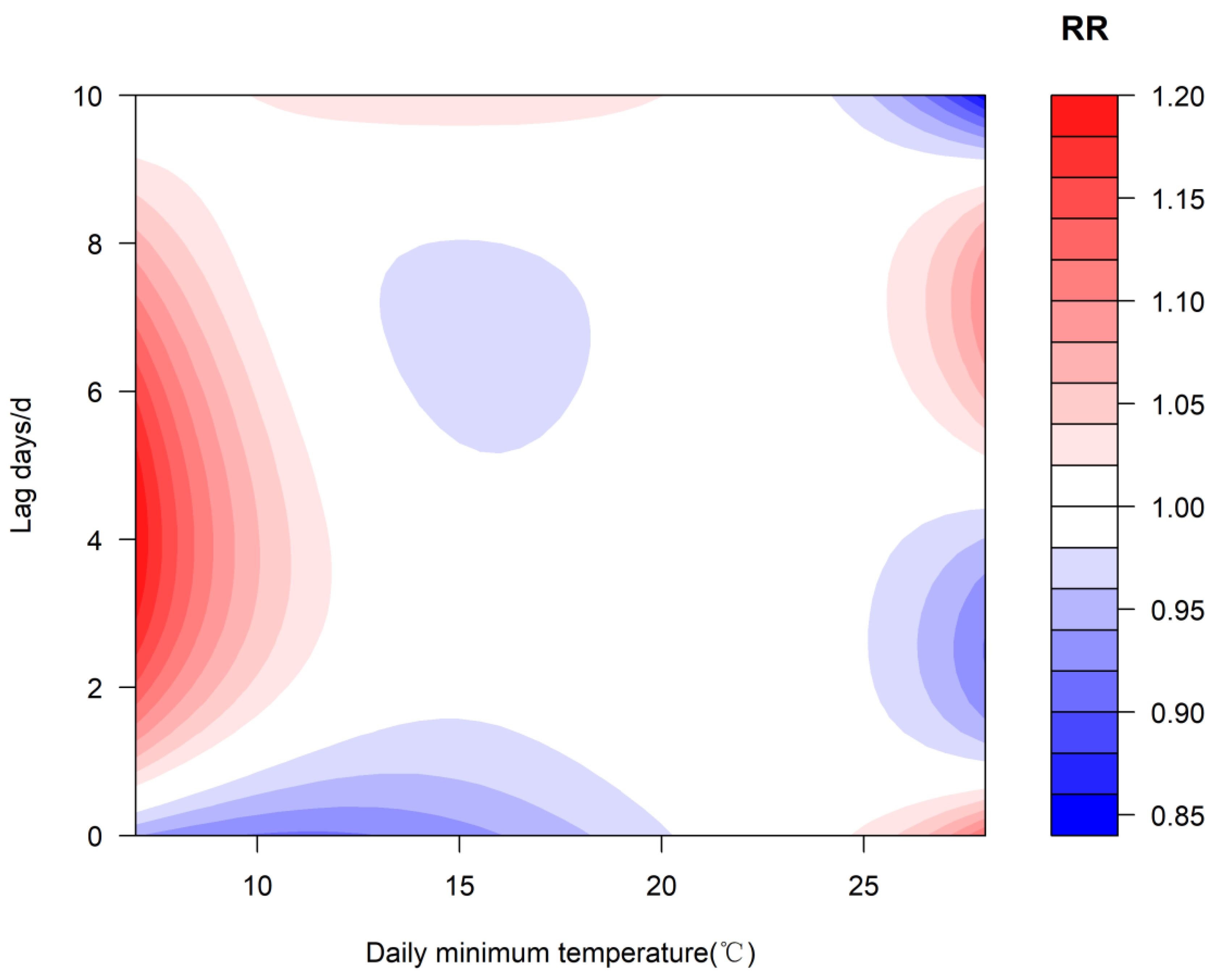
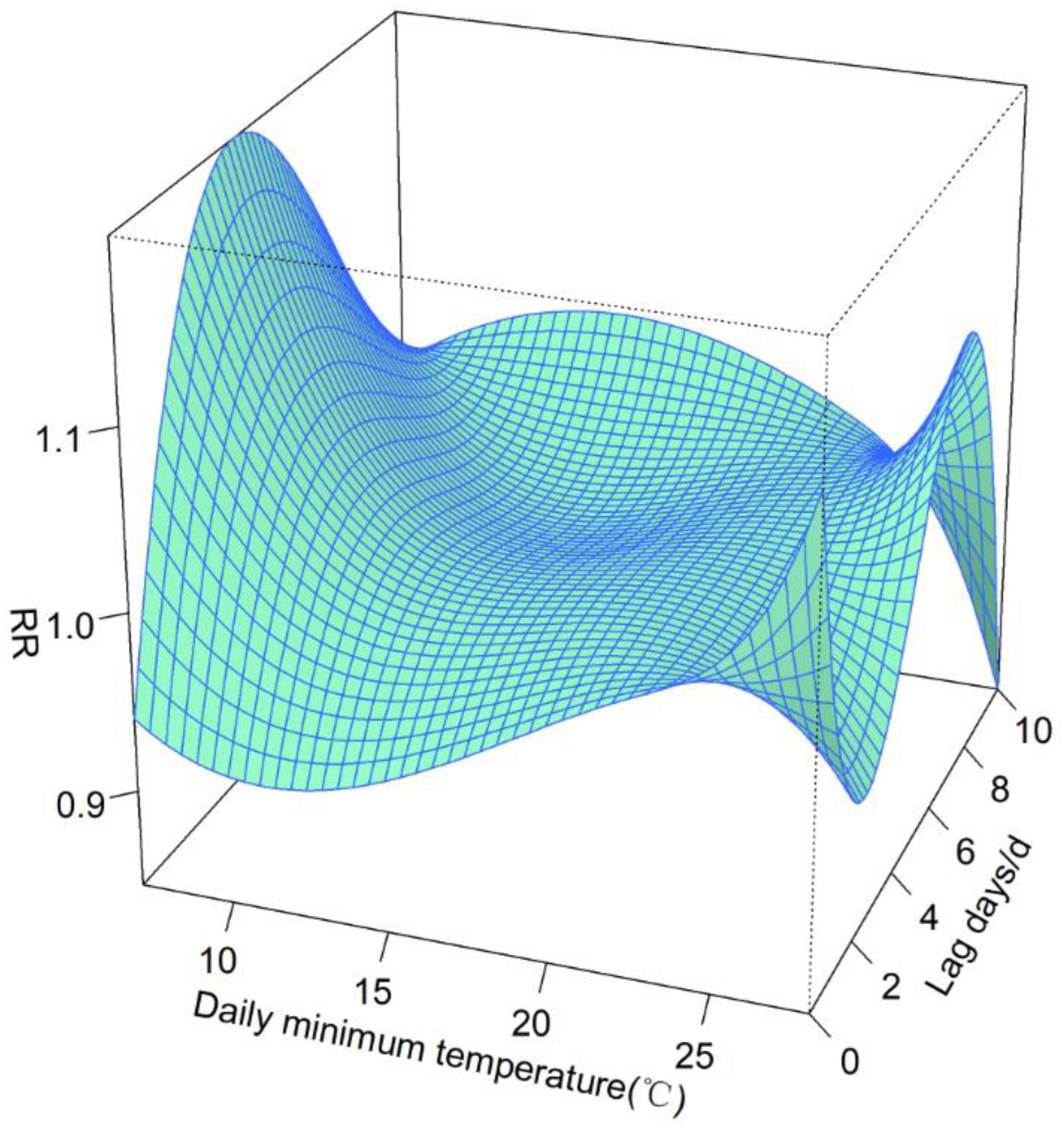
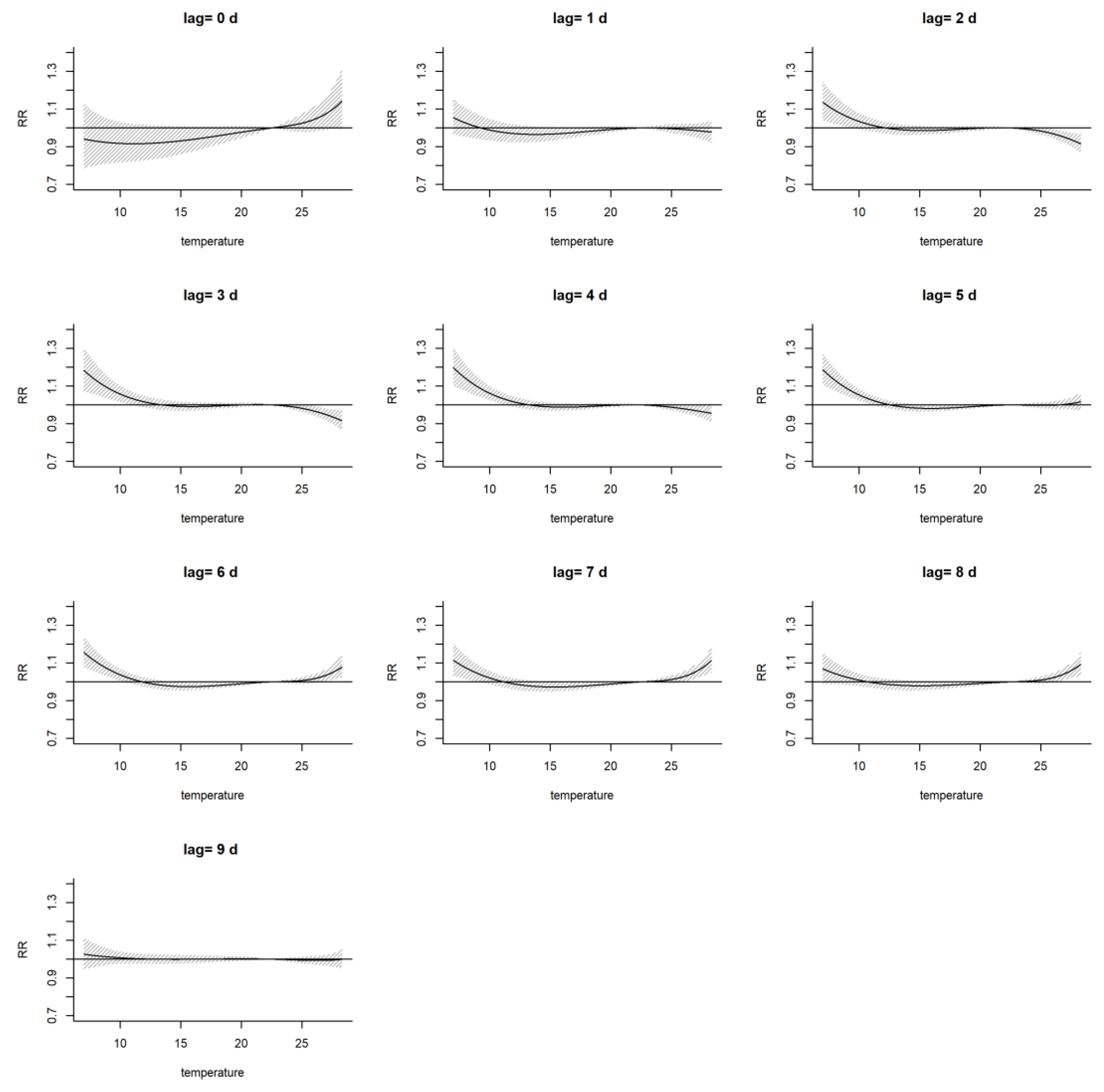
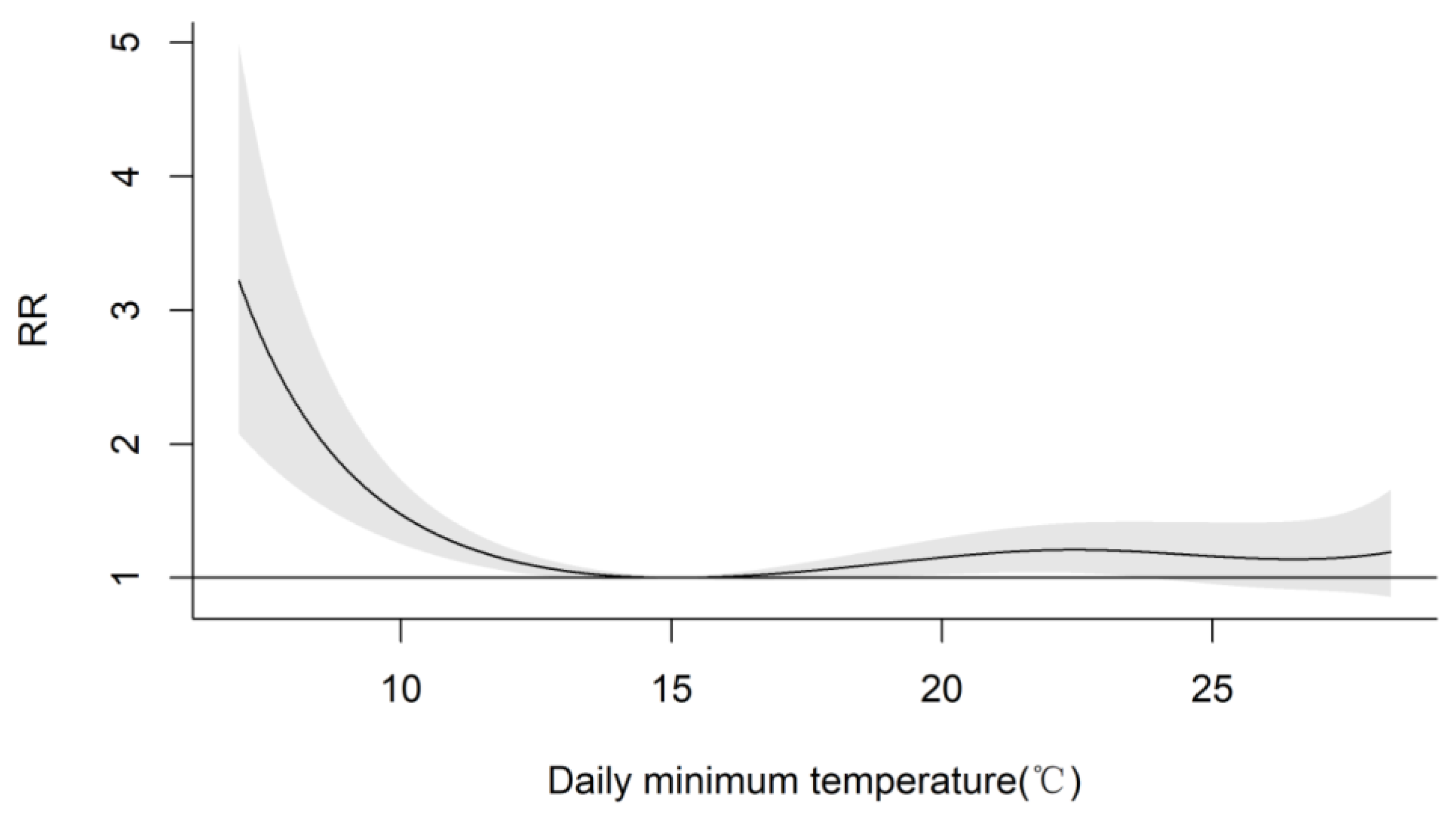
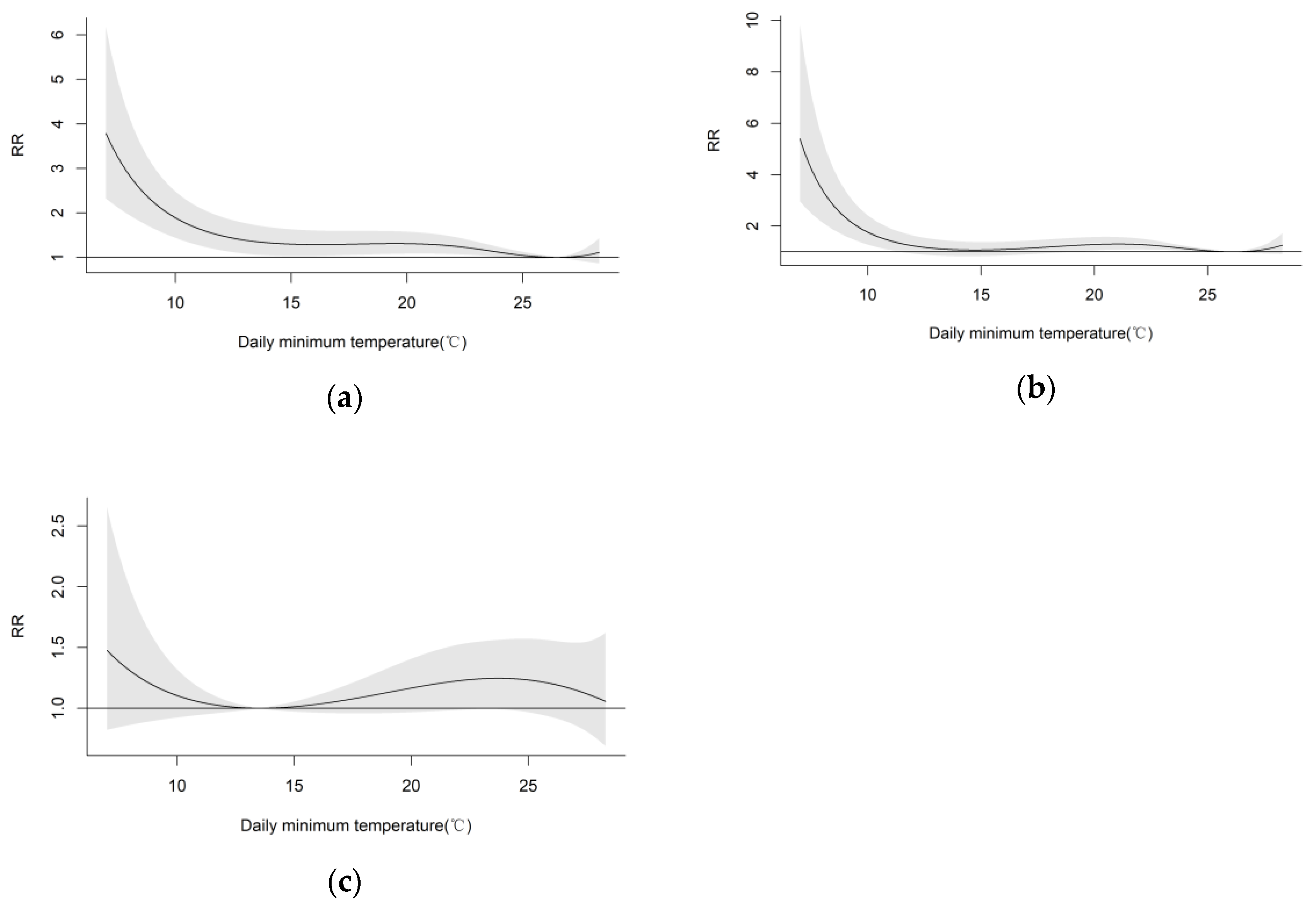
3.2. Exposure–Response Relationship between Temperature and the Total Number of Individuals with CVD and CeVD
3.3. Exposure–Response Relationship between Temperature and the Number of Visits for Different CVD and CeVD Subtypes
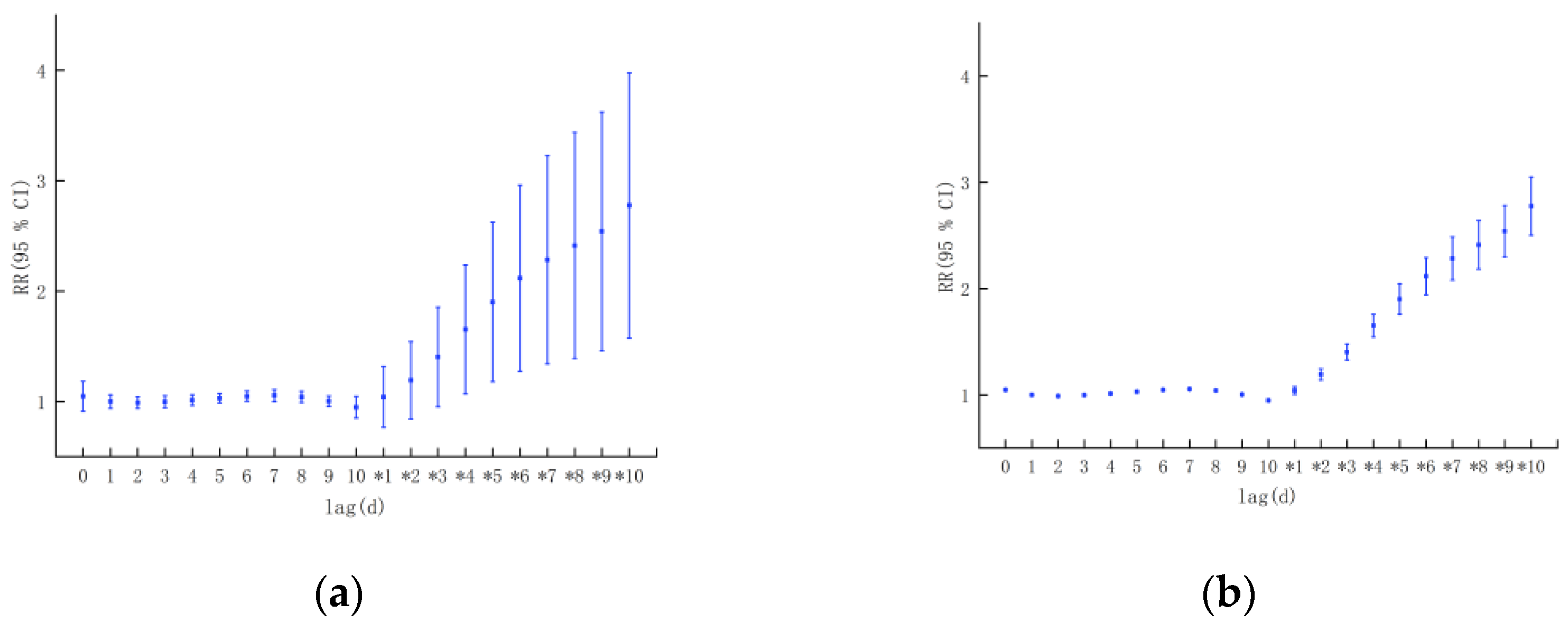
3.3.1. Different Sexes
3.3.2. Different Ages
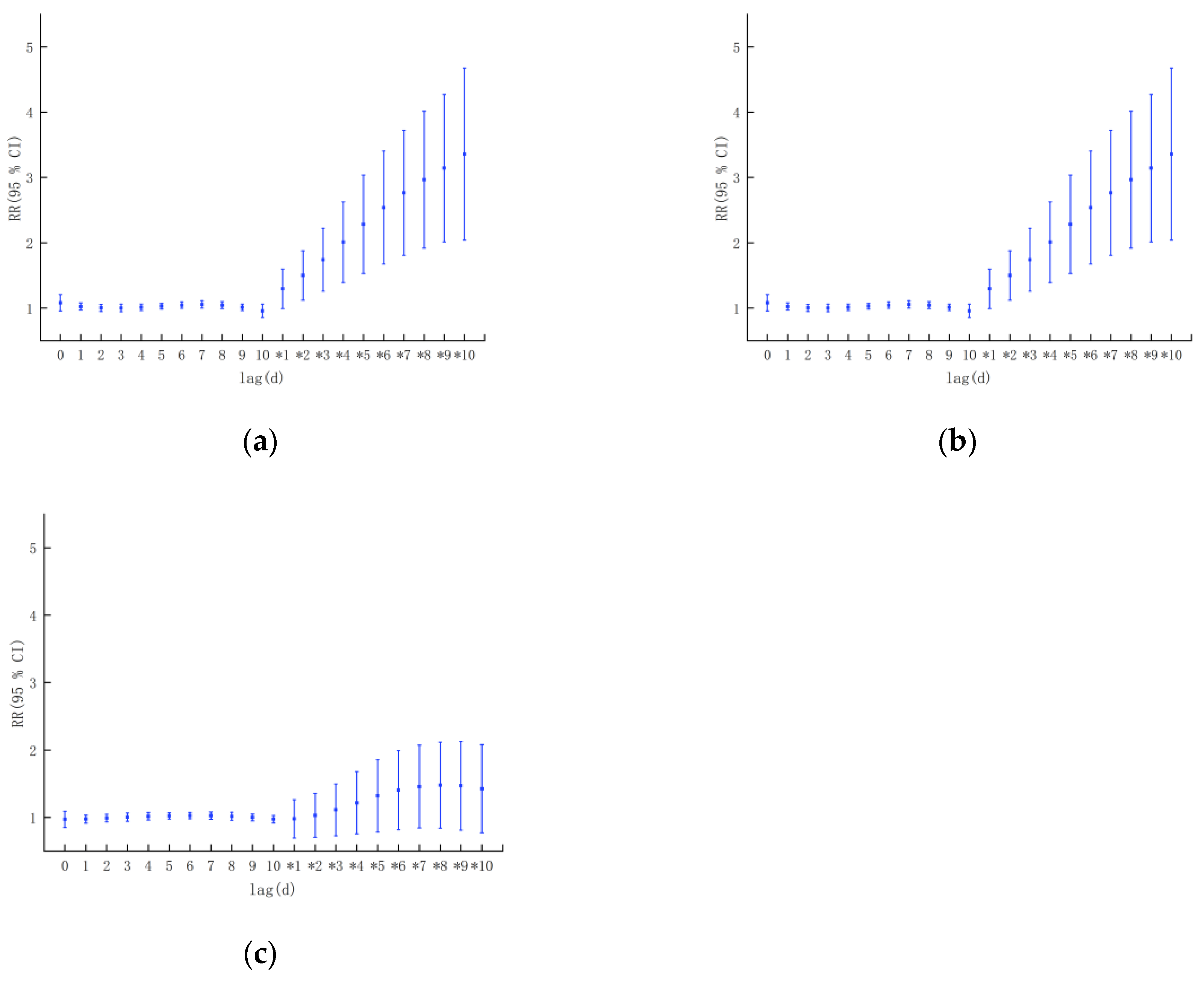
3.3.3. Different CVD and CeVD Subtypes
4. Discussion
- (1)
- The influence of temperature on the risk of CVD and CeVD development in Haikou city was dominated by the cold effect, and the health risk of the cold effect was greater than that of the heat effect, and this was consistent with the findings of Park S et al. [3] that an elevation in blood pressure during the colder seasons could potentially result in increased cardiovascular risk, and the findings of Mascarenhas MS et al. [13] that associations between suboptimal air temperatures and increased risk of death from CVD were observed in all of Brazil’s five regions. Meanwhile, the health risk of the cold effect had an obvious lag effect, and the risk of temperature exposure was greater among male working-age individuals, which was consistent with the findings of Zheng Shan [8] that the highest number of male and under 65 year old cardiovascular system diseases are seen in Beijing and Lanzhou during the winter and spring seasons. This study also found that high temperatures had a higher impact on women than men and exhibited acute effects, which was consistent with the findings of Achebak H et al. [29] that between 1980 and 2016 in Spain, 4,576,600 cardiovascular deaths were recorded. For warm temperatures, the increase in relative risk (RR) of death from cardiovascular diseases was higher for women than men, whereas for cold temperatures, RRs were higher for men than women. But Misailidou M et al. [7] found the cold effect was more prominent in the elderly, and no difference was detected according to sex. On the other hand, previous studies have shown that low temperature has an immediate effect on the incidence of circulatory diseases in Zunyi, China [25], which is different from the findings of the present study, which revealed a lagging effect of low temperatures and an immediate effect of high temperatures; changes in temperature have an effect on the incidence of CVD and CeVD [28,30], for example, Liu Bo et al. [9] found that 24-h temperature fluctuations in Beijing had the greatest impact on stroke and coronary heart disease that in spring and autumn, when the 24-h negative temperature below the threshold decreases by 1 ℃, the risk of onset increases by 18.1–34.5%, which was 2–10 times that of other meteorological changes causing an increase in risk and Rahman MM [30] found that a 1 °C increase in temperature variability (TV) was associated with a 1.00% (95% CI: 0.05%, 1.96%) increase in CVD visits at lag 0–1 days (TV0–1) in Dhaka, Bangladesh. But correlation analyses in the present study showed that the magnitude of the change in temperature had no correlation with the number of visits to the clinic for CVD and CeVD in Haikou city. These differences may be related to the different climatic conditions caused by the different study areas and the different selections of medical data.
- (2)
- The research results indicate that attention should be given to this topic and that efforts should be made to strengthen CVD and CeVD-related prevention, risk prediction, and early warning in tropical areas with climate conditions similar to those in Haikou, especially the acute effects of high temperatures and the cumulative effects of low temperatures. Collaboration between work and research groups should be established among multiple departments, such as those related to meteorology and medical health, emphasizing the health protection of special populations and formulating effective prevention and control strategies to reduce the health and economic burdens related to CVD and CeVD.
- (3)
- During the research process, we also analyzed the effects of the daily average temperature, water vapor pressure, air quality, and other factors on the number of CVD and CeVD patients. The effect of water vapor pressure on the increase in the number of CVD patients was not significant, but polluted weather conditions had an impact on the increase in the number of hypertension patients. Although the correlation between NO2 and the number of CVD and CeVD patients was statistically significant, according to the “Environmental Air Quality Standards” [GB/T 3095-2012] [31], NO2 in Haikou city did not reach the pollution threshold, which may be related to the excellent air quality caused by the regulation and purification of air by the island climate, environment, and vegetation conditions in Haikou city. Therefore, NO2 was not selected as an influencing factor, but the AQI, which characterizes air quality, was chosen as a model covariate.
- (4)
- In addition, previous studies have shown that air pollution has a significant impact on CVD and CeVD incidence and mortality. For example, Xiao Ye et al. [32] found that ischemic heart disease and stroke mortality were associated with exposure concentrations of PM10 and O3, and there was a significant lag; Britney Gaines et al. [33] found that PM2.5 exposure was associated with a higher ischemic stroke risk, with larger effect estimates at higher exposure levels with all stroke cases across Israel in 2014–2018. Therefore, it is necessary to conduct an analysis of the synergistic effects of air quality, meteorological factors, and air quality factors on the increase in the number of CVD and CeVD patients and different CVD and CeVD subtypes based on the collection of disease case data with longer time series.
5. Conclusions
- (1)
- From September 2016 to April 2018, the temperature in Haikou city showed an inverted J-shaped distribution with the number of CVD and CeVD patients, indicating that the impact of temperature on the risk of CVD and CeVD was mainly due to the cold effect. Regarding time lags, the cold effect began to appear and lasted much longer than the heat effect. A longer lag time led to a greater health risk from the accumulation of cold effects. High temperature manifested as an acute effect, which had a strong impact on the increase in the number of CVD and CeVD patients on the day of high temperature and then rapidly decreased. This could be summarized as an immediate high-temperature effect and a lagging low-temperature effect.
- (2)
- Regarding sex differences, the impact of low temperatures on women was weaker than that on men and lagged behind that on men, making women more susceptible to the effects of high temperatures. From the perspective of age classification, the lag period of the impact of low temperatures on the working-age group was longer than that on the elderly group, and the working-age group was more affected. A high temperature only had an impact on the risk of CVD and CeVD in the working-age group and reached its maximum on the day that the high temperature occurred. This may be related to the lifestyle habits of different groups of people. For example, in low-temperature weather, women and elderly people pay more attention to keeping warm and reducing outdoor activities. In high-temperature weather, elderly people perform fewer outdoor activities, while the working-age group still needs to go out to work. This indicated that attention should be given to the health risks of low-temperature weather conditions for men as well as the health risks of high temperatures for the working-age group. In addition, when comparing the impact of different CVD and CeVD subtypes on the risk of hypertension, it was found that the lag effect of low temperature on the risk of hypertension was the largest, with the longest lag period; the impact of low temperature on the three CVD and CeVD was significantly greater than that of high temperature; from the cumulative effect perspective, the impact of temperature on the risk of hypertension and CHD was greater than that of stroke.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Correction Statement
References
- Available online: https://www.who.int/health-topics/cardiovascular-diseases#tab=tab_1 (accessed on 22 March 2024).
- The Writing Committee of the Report on Cardiovascular Health and Diseases in China. Summary of China Cardiovascular Health and Disease Report 2022. Chin. Circ. J. 2023, 38, 583–612. [Google Scholar]
- Park, S.; Kario, K.; Chia, Y.C.; Turana, Y.; Chen, C.H.; Buranakitjaroen, P.; Nailes, J.; Hoshide, S.; Siddique, S.; Sison, J. The influence of the ambient temperature on blood pressure and how it will affect the epidemiology of hypertension in Asia. J. Clin. Hypertens. 2020, 22, 438–444. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.; Yang, Z. Correlation between air temperature, air pollutants, and the incidence of coronary heart disease in Liaoning Province, China: A retrospective, observational analysis. Ann. Palliat. Med. 2021, 10, 12412–12419. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Wan, J.; Peng, S.; Wang, R.; Dai, Z.; Liu, C.; Feng, Y.; Xiang, H. Associations between cold spells of different time types and coronary heart disease severity. Environ. Pollut. 2024, 343, 123100. [Google Scholar] [CrossRef] [PubMed]
- Tian, Z.; Li, S.; Zhang, J.; Guo, Y. The characteristic of heat wave effects on coronary heart disease mortality in Beijing, China: A time series study. PLoS ONE 2013, 8, e77321. [Google Scholar] [CrossRef] [PubMed]
- Misailidou, M.; Pitsavos, C.; Panagiotakos, D.B.; Chrysohoou, C.; Stefanadis, C. Short-term effects of atmospheric temperature and humidity on morbidity from acute coronary syndromes in free of air pollution rural Greece. Eur. J. Cardiovasc. Prev. Rehabil. 2006, 13, 846–848. [Google Scholar] [CrossRef] [PubMed]
- San, Z. A Study on the Impact of Weather Changes on Cardiovascular System Diseases. Ph.D. Thesis, Lanzhou University, Lanzhou, China, 2013. [Google Scholar]
- Liu, B. A Study on the Response of Stroke and Coronary to Weather Change and the Prediction Model. Master’s Thesis, Lanzhou University, Lanzhou, China, 2014. [Google Scholar]
- Yu, Y. To Assess Effect of Temperature on Cardiovascular Diseases Out-Patient Visits in Shanghai Residents with Medical Insurance. Master’s Thesis, Fudan University, Shanghai, China, 2011. [Google Scholar]
- Lu, W.; Gu, S.; Sun, S.; Zhang, C.; Zhu, X. Quantitative lagged effects of extreme temperature on stroke deaths in a coastal city. Acta Meteorol. Sin. 2022, 80, 449–459. [Google Scholar] [CrossRef]
- Wang, Q. The Impact of Temperature and Air Pollution on Stroke and Acute Coronary Syndrome in Ningxia. Ph.D. Thesis, Ningxia Medical University, Yinchuan, China, 2022. [Google Scholar] [CrossRef]
- Mascarenhas, M.S.; Silva, D.D.D.; Nogueira, M.C.; Farias, W.C.M.; Ferreira, C.C.M.; Ferreira, L.C.M. The effect of air temperature on mortality from cerebrovascular diseases in Brazil between 1996 and 2017. Cien. Saude Colet. 2022, 27, 3295–3306. (In Portuguese) [Google Scholar] [CrossRef]
- Chen, H.; Zhang, X. Influences of temperature and humidity on cardiovascular disease among adults 65 years and older in China. Front. Public Health 2023, 10, 1079722. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.J.; Ma, W.P.; Zhao, N.Q.; Wang, X.L. Time series analysis of the association between ambient temperature and cerebrovascular morbidity in the elderly in Shanghai, China. Sci. Rep. 2016, 6, 19052. [Google Scholar] [CrossRef] [PubMed]
- Bai, L.; Li, Q.; Wang, J.; Lavigne, E.; Gasparrini, A.; Copes, R.; Yagouti, A.; Burnett, R.T.; Goldberg, M.S.; Cakmak, S.; et al. Increased coronary heart disease and stroke hospitalisations from ambient temperatures in Ontario. Heart 2018, 104, 673–679. [Google Scholar] [CrossRef] [PubMed]
- Pan, W.H.; Li, L.A.; Tsai, M.J. Temperature extremes and mortality from coronary heart disease and cerebral infarction in elderly Chinese. Lancet 1995, 345, 353–355. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Xin, J.; Ma, P.; Feng, X.; Zhang, X.; Wang, S.; Zhang, J.; Feng, H.; Zheng, C. Interaction effects between ambient temperature and PM2.5 and O3 on mortality in Chengdu. China Environ. Sci. 2021, 41, 3887–3895. [Google Scholar] [CrossRef]
- Wang, D.Z.; Jiang, G.H.; Zhang, H.; Song, G.D.; Zhang, Y. Effect of air pollution on coronary heart disease mortality in Tianjin, 2001–2009: A time-series study. Zhonghua Liu Xing Bing Xue Za Zhi 2013, 34, 478–483. [Google Scholar] [PubMed]
- Fu, G.; Cheng, H.; Lu, Q.; Liu, H.; Zhang, X.; Zhang, X. The synergistic effect of high temperature and ozone on the number of deaths from circulatory system diseases in Shijiazhuang, China. Front. Public Health 2023, 11, 1266643. [Google Scholar] [CrossRef] [PubMed]
- Tan, Y. The Impact and Prediction of Meteorological Elements on Cardiovascular and Cerebrovascular Diseases in Different Regions of East and West China. Master’s Thesis, Chengdu University of Information Technology, Chengdu, China, 2019. [Google Scholar] [CrossRef]
- Dastoorpoor, M.; Khodadadi, N.; Khanjani, N.; Borsi, S.H. Physiological Equivalent Temperature (PET) index and cardiovascular hospital admissions in Ahvaz, southwest of Iran. Arch. Environ. Occup. Health 2022, 77, 653–661. [Google Scholar] [CrossRef] [PubMed]
- Cheng, B.J.; Li, H.; Meng, K.; Li, T.L.; Meng, X.C.; Wang, J.; Wang, C.; Jiang, N.; Sun, M.J.; Yang, L.S.; et al. Short-term effects of heatwaves on clinical and subclinical cardiovascular indicators in Chinese adults: A distributed lag analysis. Environ. Int. 2024, 183, 108358. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Wang, S.G.; Zhang, J.; Feng, X.Y.; Zhang, X.L.; Hu, W.D.; Jia, X.W. Attributable risk assessment of the effects of different temperature on death of respiratory and cardiovascular diseases in Chengdu. Chin. Health Stat. 2019, 36, 818–823+828. [Google Scholar]
- Zhao, W. Research on the Response and Prediction Application of Circulating System Diseases to Weather and Climate Change in Zunyi Area. Master’s Thesis, Chengdu University of Information Technology, Chengdu, China, 2019. [Google Scholar]
- Wang, J.; Shi, Y.; Lu, S.; Feng, X.; Wang, S.; Zhang, Y. A Study on the Change Characteristics of Major Weather Sensitive Diseases and Their Medical Expenses in the County of Eastern and Western China. Desert Oasis Meteorol. 2019, 13, 133–140. [Google Scholar]
- Gasparrini, A. Modeling exposure-lag-response associations with distributed lag non-linear models. Stat. Med. 2014, 33, 881–899. [Google Scholar] [CrossRef] [PubMed]
- Tan, Y.; Yin, L.; Wang, S.; Chen, L.; Tan, Y.W.; Kang, Y.Z. Comparative research of the effects of temperature change on ischemic cardio-cere-brovascular diseases in different regions. J. Meteorol. Environ. 2019, 35, 94–99. [Google Scholar]
- Achebak, H.; Devolder, D.; Ballester, J. Trends in temperature-related age-specific and sex-specific mortality from cardiovascular diseases in Spain: A national time-series analysis. Lancet Planet. Health 2019, 3, e297–e306. [Google Scholar] [CrossRef] [PubMed]
- Rahman, M.M.; Garcia, E.; Lim, C.C.; Ghazipura, M.; Alam, N.; Palinkas, L.A.; McConnell, R.; Thurston, G. Temperature variability associations with cardiovascular and respiratory emergency department visits in Dhaka, Bangladesh. Environ. Int. 2022, 164, 107267. [Google Scholar] [CrossRef] [PubMed]
- GB/T 3095-2012; National Standards of the People’s Republic of China: Environmental Air Quality Standards. Standards Press of China: Beijing, China, 2012.
- Xiao, Y. Association of PM10 and O3 Exposure with Risk of Death from Specific Cardiovascular and Cerebrovascular Disease. Master’s Thesis, Chengdu Medical College, Chengdu, China, 2023. [Google Scholar]
- Gaines, B.; Kloog, I.; Zucker, I.; Ifergane, G.; Novack, V.; Libruder, C.; Hershkovitz, Y.; Sheffield, P.E.; Yitshak-Sade, M. Particulate Air Pollution Exposure and Stroke among Adults in Israel. Int. J. Environ. Res. Public Health 2023, 20, 1482. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Meteorological Elements | Average Air Pressure | Maximum Air Pressure | Lowest Air Pressure | Average Temperature | Maximum Temperature | Minimum Temperature | Vapor Pressure | Relative Humidity | Precipitation | Average Wind Speed | Temperature Change Range |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Number of visits | 0.07 | 0.08 | 0.06 | −0.09 * | −0.08 * | −0.11 ** | −0.11 ** | −0.04 | −0.05 | 0.02 | −0.02 |
| Air quality indicators | AQI | PM2.5 | PM10 | SO2 | NO2 | CO | O3 | ||||
| Number of doctors | 0.05 * | 0.06 | 0.08 | 0.00 | 0.09 * | 0.07 | 0.01 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, M.; Lin, S.; Zhang, Y.; Zhang, J. Study on the Health Effect of Temperature on Cardiovascular and Cerebrovascular Diseases in Haikou City. Atmosphere 2024, 15, 725. https://doi.org/10.3390/atmos15060725
Zhang M, Lin S, Zhang Y, Zhang J. Study on the Health Effect of Temperature on Cardiovascular and Cerebrovascular Diseases in Haikou City. Atmosphere. 2024; 15(6):725. https://doi.org/10.3390/atmos15060725
Chicago/Turabian StyleZhang, Mingjie, Shaowu Lin, Yajie Zhang, and Jinghong Zhang. 2024. "Study on the Health Effect of Temperature on Cardiovascular and Cerebrovascular Diseases in Haikou City" Atmosphere 15, no. 6: 725. https://doi.org/10.3390/atmos15060725
APA StyleZhang, M., Lin, S., Zhang, Y., & Zhang, J. (2024). Study on the Health Effect of Temperature on Cardiovascular and Cerebrovascular Diseases in Haikou City. Atmosphere, 15(6), 725. https://doi.org/10.3390/atmos15060725