Abstract
This study was designed to assess the health impacts related to noninvasive carbon monoxide saturation (SPCO %) in the blood of respondents. For this purpose, 150 respondents from the labour community of Hattar Industrial Estate (testing site) and 100 respondents from Sultan Pur (control site) were selected. To achieve this objective, a Rad-57 Pulse CO-Oximeter was used for noninvasive carboxyhemoglobin measurement. Carbon monoxide saturation (SPCO%) in the blood of respondents from Hattar Industrial Estate, Haripur, Pakistan has been compared with the WHO’s standard concentration of SPCO% (5%). High saturation of carbon monoxide (carboxyhemoglobin SPCO) in the blood of respondents and disease association have been interpreted in graphs formed on the basis of statistical analysis in terms of frequencies, using statistical software (SPSS), based on demographic entries as well as exposure time of the employees in the processing, food and steel industries. The highest SPCO% measured was 17% in the steel industry and the lowest measured level was 4.2%. Frequencies and percentages of respiratory inflammation, dermatosis, asthma, breathing issues and eye inflammation among respondents were 29%, 35%, 16.7%, 23.5% and 9%, respectively. Prevalence of disease in three different groups of respondents (from three testing sites) was also analyzed on the basis of exposure time (hrs.) to carbon monoxide emissions. Prevalence of disease among the exposed and non-exposed groups was analyzed and showed comparatively lower disease prevalence in the group of respondents who were not exposed to high carbon monoxide emissions. The data of the current study was also subjected to statistical modelling to find the health risk of air pollutants (carbon monoxide) on population health by calculating attributable risk (AR) or attributable proportion (AP). Results indicated that attributable risk of carbon monoxide exposure for respiratory diseases, dermatosis and eye inflammation were 61.12%, 65.77% and 24.95% respectively. Findings of statistical modelling indicated that dermatosis and respiratory diseases were more prevalent in laborers of industrial units than those at control site.
1. Introduction
Air pollution from the influence of anthropogenic factors in the modern world is becoming a global environmental problem, the consequences of which clearly negatively affect the health of people and the environment. These problems are also relevant today for the industrial city of Haripur, Hattar, where the mining, metallurgical and chemical industries are developing intensively [1]. Air pollution, mainly carbon monoxide, ozone and particulate matter emitted from industrial smoke may cause pulmonary diseases in humans, as reported in Pakistan [2]. Carbon monoxide (CO) is a toxic, colorless gas that results from the incomplete combustion of coal and other petroleum-derived materials on a large scale in the industrial sector. Among anthropogenic sources of carbon monoxide emissions, air pollution from car emissions is a major source of carbon monoxide pollution present in the atmosphere. Inhalation of this gas is considered to be potentially toxic to the body, resulting in a hemoglobin variant with reduced oxygen transport capacity, carboxyhaemoglobin (COHb). As the endogenous concentration of COHb in a healthy adult varies from 0.1% to 1.0%, higher values can lead to respiratory problems, impairment in visual perception, headache and nausea [3]. Carbon monoxide (CO) exposure occurs in- and outdoors, in occupational or accidental (e.g., fire) settings, or through smoking [4]. In some fire accidents, victims may inhale smoke that may contain toxic gases such as carbon monoxide (CO). Laborers exposed for a longer time were adversely affected by carbon monoxide as it reversibly combines with hemoglobin, leading to hypoxemia and carbon monoxide poisoning [5].
Exposure to carbon monoxide raises levels of circulating carboxyhemoglobin (SPCO) in the blood [6]. Exposure to carbon monoxide for a long duration may lead to exacerbation of asthma, chronic bronchitis (also called chronic obstructive pulmonary disease) and increased susceptibility to respiratory diseases [7]. The most common symptoms of CO poisoning are headache, dizziness, weakness, nausea, vomiting, chest pain and confusion. People who are sleeping or who have been drinking alcohol can die from CO poisoning before ever having symptoms [8].
People who are addicted to smoking are exposed to considerable CO concentrations, leading to a COHb of about 3–8% [9]. Carbon monoxide combines with hemoglobin to form carboxyhemoglobin at any or all of the oxygen-binding sites of hemoglobin, and also acts to increase the stability of the bond between hemoglobin and oxygen, reducing the ability of the hemoglobin molecule to release oxygen bound to other oxygen-binding sites. Consequently, carbon monoxide will bind hemoglobin preferentially over oxygen when both are present in the lungs. Even small amounts of carbon monoxide can dramatically reduce the ability of hemoglobin to transport oxygen [10]. Tissue damage results from local hypoxia. Organs with a high oxygen requirement, such as the heart and the brain, are especially sensitive to this effect [11].
There are about 50,000 Emergency Department visits for carbon monoxide poisoning per year in the United States. The Rad-57 pulse CO-oximeter is a new device that allows for a rapid noninvasive determination of the percentage of carboxyheamoglobin (COHb) in blood. The Rad-57 employs eight wavelengths of light. Standard pulse oximeters are composed of two wavelengths and can only measure arterial oxyhemoglobin saturation (%SaO2). This pulse CO-oximeter allows for instantaneous detection of %SaO2, COHb and the percentage of metheamoglobin (MetHb) in blood [12]. The U.S. National Ambient Air Quality Standards for carbon monoxide in outdoor air are 9 ppm (40,000 micrograms per meter cubed) for 8 h and 35 ppm for 1 h [13]. The Health and Safety Executive recommended that CO above 30 ppm can produce high COHb levels and affect occupational health [14].
The most common sources of CO are industrial boilers, lack of proper ventilation, generators and incomplete combustion using catalytic convertors in motor vehicles. Equipment failure is the primary contributing factor to most CO incidents [15]. The precise number of individuals who have suffered from CO intoxication is not known. The health effects associated with exposure to CO range from more subtle cardiovascular and neurobehavioral effects at low concentrations to unconsciousness and death after acute or chronic exposure at higher concentrations of CO. The symptoms, signs and prognosis of acute CO poisoning correlate poorly with the level of carboxyhemoglobin (COHb) measured at the time of hospital admission; however, because CO poisoning is a frequently overlooked diagnosis, the importance of measuring COHb in suspicious settings cannot be overstated. The early symptoms (headache, dizziness, weakness, nausea, confusion, disorientation and visual disturbances) also have to be emphasized, especially if they recur with a regular periodicity or in the same environment. Complications occur frequently in CO poisoning. Immediate death is most likely cardiac in origin because myocardial tissues are the most sensitive to the hypoxic effects of CO. Pulmonary edema may occur. Carbon monoxide poisoning during pregnancy results in high risk for the mother by increasing the short-term complication rate and for the fetus by causing fetal death, developmental disorders and chronic cerebral lesions. Efforts in prevention and in public and medical education should be encouraged [16].
Hattar Industrial Estate, KPK has provided employment to at least 0.2 million peoples with poor lifestyles with low grade education, Due to high exposure to air emissions and use of unprotected measures and lack of awareness regarding carbon monoxide and air emissions poisoning caused by incomplete industrial combustion processes, laborer’s health is at stake, they suffered acute disease affects the working efficiency as a result industries bear high medical costs per month spent of on labor community. Exposure of labor to the high carbon monoxide concentration emitted from industrial units of Hattar industrial estate may be one major cause of notable symptoms such as breath shortness, respiratory tract congestion, asthma and unconsciousness, which were noticed during initial visits to Hattar industrial units and were confirmed through medical history.
Many cases of carbon monoxide poisoning have been reported in the current study area, but no effective efforts have ever been carried out so far to mitigate the ratio of such incidences. It is perhaps possible by educating industries about simple protection techniques like the use of ecological indicators, baghouses and fabric filters [17]. Awareness sessions among industrial management of the area about regular medical checkups along with regular noninvasive measurements of carbon monoxide saturation in hemoglobin (SPCO) for laborers that are exposed to carbon monoxide emissions from different industrial processes for many hours per day. As such, this research was planned to evaluate baseline carboxyhemoglobin concentrations (SPCO) of respondents working in the food, processing (vegetable, ghee) and steel industries. Another important aspect covered in this study was evaluation of population risk factors (AP = AR) to show the possible association between high carbon monoxide saturation in hemoglobin (SPCO) and disease prevalence among the labor community of the study area. This study could help in the policy implementation for carbon monoxide-related health risk and pollution control by setting local standards for indoor air quality, applying a job rotation strategy, periodical medical checks, good ventilation and conducting further studies concerning the long-term effect of a high concentration of CO on occupational health [18]. Besides this, there is further needed to address a zero emissions rate with the industrial sector because the target of zero emissions may set a new standard for industry and industrial policy. Industrial policy in the twenty-first century must aim to achieve zero emissions in the energy- and emission-intensive industries. Sectors such as steel, cement and chemicals have so far largely been sheltered from the effects of climate policy, but a major shift is needed from contemporary industrial policy that mainly protects industry to policy strategies that transform the industry [19].
2. Materials and Methods
2.1. The Study Area
The study was carried out in Hattar Industrial Estate located in Haripur Basin. Hattar Industrial Estate (Figure 1) is one of the largest industrial estates of the Province of Khyber Pakhtunkhwa (KPK), Pakistan. The total area of the estate is 1063 acres. As there are more than 250 industries of various kinds, including the textile, chemical, marble, heavy electrical engineering, ghee and cooking oil and food and beverage industries.
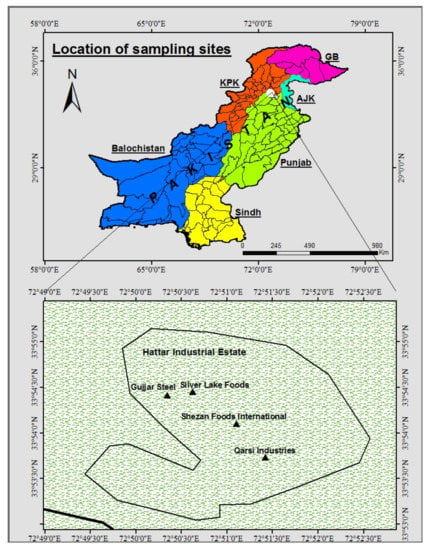
Figure 1.
Sampling points at industrial units (Hattar).
2.2. Sampling Sites
Sampling areas included food, steel and processing (vegetable oil and ghee) industries of Hattar industrial estate, Haripur Pakistan. Hattar Industrial Estate is one of the largest industrial estates of the Province of Khyber Pakhtunkhwa (KPK). The total area of the Estate is 1063 acres.
2.3. Control Sites
Control sampling was done at Sultan Pur, Havelian. It is a non-industrial area.
2.4. Carbon Monoxide Saturation in the Hemoglobin (SpCO) of Respondents
Symptoms of carbon monoxide (CO) poisoning are non-specific. Diagnosis requires suspicion of exposure, confirmed by measuring ambient CO levels or carboxyhemoglobin. The Masimo Rad-57 Pulse CO-Oximeter measures the saturation of carbon monoxide in hemoglobin (SpCO). It uses light waves (usually shone through the fingertips) to measure carbon monoxide saturation noninvasively, as shown in Figure 2.

Figure 2.
Masimo Rad-57 Pulse CO-Oximeter.
In this study, the Masimo Rad-57 Pulse CO-Oximeter was used for continuous and noninvasive measurement of carbon monoxide (SPCO) levels in the arterial blood of 150 respondents from Hattar Industrial Estate, Hattar, Pakistan. The Rad-57 is a noninvasive device that delivers readings in seconds. A sensor clips over the patient’s finger, as withmany standard pulse oximetry units. Proper sensor placement is especially important to ensure accurate measurements [20].
This FDA- (The Food and Drug Administration) approved pulse oximeter (Rad-57) can provide a continuous and noninvasive measurement of the carbon monoxide levels in arterial blood [21]. The interpretation of carboxyhemoglobin levels (SPCO%) devised by the FDA is shown in Table 1 [22].

Table 1.
Interpretation of carboxyhemoglobin (SPCO%) (FDA, 2017).
Noninvasive methods of body fluid chemical measurement have been expanding. New technologies are enabling the quantification of different compounds in the blood and interstitial tissues. One example of this is the pulse oximeter, which has facilitated the measurement of oxyhemoglobin rapidly and reliably without the requirement of blood-draws. The Masimo Rad-57 Pulse CO-Oximeter expanded the capabilities of pulse-oximetry to include measurements of carboxyhemoglobin (SPCO) and met hemoglobin (SPMet). This innovation is helpful in detection of patients with CO poisoning. Previously, clinicians relied on historical information and patient signs and symptoms pointing to the possibility of CO exposure or toxicity. Only then would a blood test be ordered to measure carboxyhemoglobin levels. Since the presentation of CO poisoning is nonspecific and overlaps with many other conditions, and since the presence of environmental CO is often unknown, the detection of this condition was only possible in cases where the presence of CO was obvious or where the symptoms were severe. We have now confirmed from studies conducted using the Rad-57, the only US FDA-approved device for noninvasive measurement of SPCO, that there are a significant number of patients who experience CO exposure but are non-symptomatic. The Rad-57 provides a clinical justification for screening in the healthcare setting to identify patients with significant CO exposure who would otherwise be undetected [23]. In previous studies, the Masimo Rad-57 Pulse CO-Oximeter has been used for noninvasive measurement of oxygen saturation from different staff grade employees at different occupational sites, but noninvasive saturation of carbon monoxide in hemoglobin (SPCO) has not been measured at Hattar Industrial Units, Khyber, Pakhtunkhwa (KPK) of Pakistan, where air emissions were not measured in Hazara Division including Abbottabad and Haripur by Environment protection A protection agency (EPA, Islamabad, Pakistan).
2.5. Comparision of Observed and Standard Concentration of Carbon Monoxide
Noninvasive measurement of carbon monoxide saturation (SPCO%) in the blood of respondents from Hattar Industrial Estate, Haripur, Pakistan has been compared with the WHO standard concentration of SPCO%, and greater-than-standard concentrations have been plotted in graphs.
2.6. Statistical Package for the Social Sciences (SPSS)
High saturation of carbon monoxide (carboxyhemoglobin, (SPCO) in the blood of respondents and disease association has also been interpreted in graphs formed on the basis of statistical analysis in terms of frequencies using statistical software (SPSS) [24].
2.7. Statistical Modelling Equation for Attributable Risk (AP)
A state-of-the-art review made a contribution to current knowledge about the impact of air pollution on population health by reflecting on the relevance of attributable risk to public health and also on the scientific and methodological problems of defining it, with the aim of contributing to future advances of research in this field [25]. The data of the current study were also subjected to statistical modelling to find the health risk of air pollutants (carbon monoxide) on population health by calculating attributable risk (AR) or attributable proportion (AP).
RR = Risk of exposed group of population/non-exposed group
The health risk of carbon monoxide has been statistically calculated by using a health risk assessment model equation as shown below. The attributable proportion (AP) can be calculated by the following equation:
RR is the relative risk value for a given air pollutant and health outcome, published by the WHO from epidemiological studies. RR in this equation was greater than 1, showing a high association of increased pollutant concentration with the disease prevalence among the labor community where P(c) is the population proportion in category “c” of exposure.
AP = Ʃ[{RR(c) − 1} × P(c)]/Ʃ[RR(c) × P(c)]
3. Results
3.1. Comparision of Observed and Standard Concentrations of Carbon Monoxide
3.1.1. Food Industry
The results obtained for noninvasive carbon monoxide saturation in the blood of respondents from the food industry from the Masimo Rad-57 Pulse CO-ximeter indicated that the maximum observed carbon monoxide concentration (SPCO%) was 14.1% and the minimum observed concentration was 10–12%, as shown in Figure 3. The minimum observed concentration was higher than the standard concentration of SPCO reading i.e., 5%. The high ratio indicates that there was less oxygen in the blood and that the patients may have needed to be treated with high-flow oxygen.
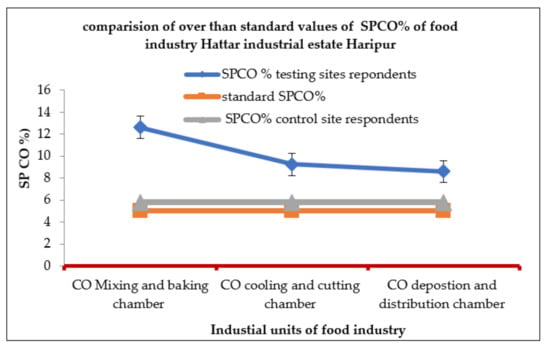
Figure 3.
Carbon monoxide saturation measured in respondents from the food industries of Hattar Industrial Estate.
3.1.2. Processing Industry
The measured percentage of carbon monoxide (SPCO%) ranged from 8–14 percent among the respondents from the processing industries of Hattar Industrial Estate, where the maximum observed carboxyhemoglobin was 14.9 percent and the minimum observed carboxyhemoglobin was 6–8%, as mentioned in Figure 4.

Figure 4.
Carbon monoxide saturation measured in respondents from processing industries of Hattar Industrial Estate.
3.1.3. Steel Industry
The SPCO percentage’s recorded maximum in the steel industries reached up to 17%, which is an alarmingly high concentration of carbon monoxide in the blood of respondents, as indicated in Figure 5.
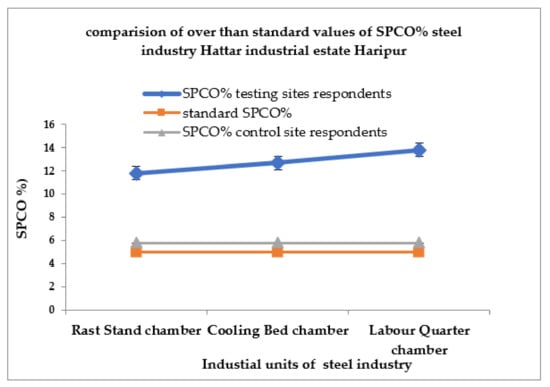
Figure 5.
Carbon monoxide saturation measured in respondents from the steel industries of Hattar Industrial Estate.
3.2. Comparision of SPCO% among Respondents from the Food, Processing and Steel Industries
The steel industries were more contaminated as compared to the food and processing industries. Greater-than-standard concentrations are plotted in the graph shown in Figure 6. An abrupt increase in SPCO% with increasing levels of air emissions particularly emitted from food, processing and steel industries have been noticed, with a significant value of R2 = 0.8669, a co-efficient of correlation indicating a strong positive relationship between two variables (xy) where variable x indicated the level of carbon monoxide emissions from different chambers of industrial units and variable y indicates the increasing percentage of perfusion index indirectly related to infusion of CO to blood of workers at different industrial units of Hattar Industrial Estate, Pakistan.

Figure 6.
Carbon monoxide saturation measured in respondents from food, processing and steel industries of Hattar Industrial Estate.
3.3. Statistical Package for the Social Sciences (SPSS)
The analysis of disease prevalence among the laborers of the food, processing and steel industries indicated various diseases such as respiratory diseases, hypertension, bronchitis, skin allergies, asthma, dermatosis, eye inflammation and gastrointestinal infection. The prevalence of disease was calculated by statistical analysis in terms of frequencies using statistical software (SPPS) based on demographic entries as well as exposure time of the employees in the processing, food and steel industries. The medical history of laborers/respondents was taken from the laboratories of Hattar Industries. Those who were exposed for 8 hrs per day in a high-temperature zone were more prone to respiratory and skin allergies. Among the respondents, 35% suffered from skin allergies, 25% from respiratory diseases, 35% from skin diseases, 16.7% from asthma and 9% from eye inflammation; 14% from hypertension and 4% from a gastrointestinal infection. Those who were exposed to carbon monoxide at a high concentration for 6 hrs. had a prevalence of 20% for respiratory diseases 30% for skin diseases 7% for eye inflammation, 14% for asthma, 12% for hypertension, and 3% for gastrointestinal infections. The respondents who were exposed for 5 hrs. showed the following disease prevalence pattern: 14% had respiratory diseases, 22% had skin diseases, 13% had asthma, 6% had eye inflammation, 10% had hypertension and 3% had a gastrointestinal infection, as shown in Figure 7. Among 150 testing site respondents, only 6.7% were smokers, while 93.3 percent were non-smokers. No strong association was found between smoking and disease prevalence in this study.

Figure 7.
Disease prevalence vs. CO exposure times (hrs.) among respondents Hattar industrial Estate (testing sites), Haripur, Pakistan.
The prevalence of disease among the labor community of testing sites which were exposed to high carbon monoxide emissions for longer hours, compared with the non-exposed group of the control site, was statistically analyzed by SPSS. Comparison of the two groups showed that those who were not exposed to such a high concentration of carbon monoxide emissions had a low percentage of diseases as compared to the exposed group. The prevalence of respiratory diseases was 8%, skin problems was 5%, eye inflammation was 2%, asthma was 2%, hypertension was 14% and gastrointestinal infections was 11%, as shown in Figure 8.

Figure 8.
Comparison of disease prevalence among the exposed and non-exposed group of respondents.
3.4. Statistical Model Validation of the Perfusion Index (%CO)
The response was validated from the statistical modeling equation by calculating the attributable risk or attributable proportion (AR = AP) to find out the prevalence of diseases caused by inhalation of carbon monoxide gas. The attributable risk calculated by the health risk assessment equation as shown in Table 2 depicted that prevalence of respiratory, skin and eye diseases, which were 61.12%, 65.77% and 24.95%, respectively.
where RR is the relative risk value for a given air pollutant and health outcome, published by the WHO from epidemiological studies, and P(c) is the population proportion in category “c” of exposure.
Table 2.
Attributable proportion for disease prevalence due to exposure to carbon monoxide for industrial units of Hattar, Haripur, Pakistan (AP%).
4. Discussion
The late onset of respiratory diseases in children and adults due to prenatal or perinatal exposure to air pollutants such as carbon monoxide ozone and sulfur dioxide is emerging as a critical concern in human health. Pregnancy and fetal development stages are highly susceptible to environmental exposure and tend to develop a long-term impact in later life. Epidemiological evidence is provided to show the association of prenatal or perinatal exposure to air pollutants with various adverse birth outcomes, such as preterm birth, lower birth weight and lung development defects, which are further, associated with respiratory diseases and reduced lung function in children and adults. Air pollutants impact various cellular and molecular targets in early life, which link to the pathogenesis and altered immune responses related to abnormal respiratory functions and lung diseases in later life [26].
Carbon monoxide (CO) poisoning is a common cause of death, leading to morbidity and mortality worldwide. Features of CO poisoning with low carboxyhemoglobin (COHb) levels remain to be characterized [27]. Hemoglobin comprises four globin chains, each containing a heme molecule which reversibly binds to oxygen. The binding of oxygen to heme alters oxygen affinity by inducing structural changes in the adjacent globin chains. Oxyhemoglobin is the normal, oxygen-carrying form of hemoglobin in which iron is in the reduced (ferrous) state. Methemoglobin is a nonfunctional form of hemoglobin in which ferrous iron is oxidized to ferric iron. Methemoglobin is nonfunctional because it cannot bind oxygen. In healthy animals, approximately 1% of oxyhemoglobin is converted to methemoglobin daily [28].
In the current study, results obtained from noninvasive carbon monoxide saturation measurements using the Masimo Rad-57 Pulse CO-Oximeter to assess the blood of respondents in the steel industry showed maximum SPCO% concentration of 17%. Many pieces of equipment used in the iron- and steel-making industries, such as coke ovens, sintering plants, blast furnaces, basic oxygen furnaces and thermal power plants, emit carbon monoxide. Many employees also work for longer hours in the raw materials production plant and were exposed to the highest mean concentration of carbon monoxide. The highest recorded exposure was found near the blast furnace, which causes a variety of toxic effects on human health, such as breathing issues, blurred vision, headache, nausea and skin issues due to less oxygen supply. Results have been presented according to the carbon monoxide inhalation rate and exposure time during job timings of respondents. At elevated exposure, carbon monoxide poisoning may lead to loss of consciousness and death. The results from the testing sites were compared with those from the control sites of Sultan Pur village, where noninvasive carbon monoxide saturation (SpCO %) was measured by the Masimo Rad-57 Pulse CO-Oximeter in the blood of 100 respondents. There was an inverse correlation found between respondents of understudy testing sites, was high in comparison less SPCO% concentration in the blood of respondents of control sites. This may be due to comparatively clean ambient air and no industries at the control site. Carbon monoxide saturation (SPCO%) was 14.9% in the blood of respondents from the processing (vegetable oil and ghee) industry, which is higher than the standard concentration of SPCO 5%. This high concentration might be due to the incomplete combustion of fuel types used in various processes at industries and the exposure of laborers for a long time, from 7.00 a.m. to 5.00 p.m., 6 days per week use of gas, oil, coal, wood and plastic tires in the time of energy crisis and COVID-pandemic. Another study supported this paradigm that carbon monoxide with COHb% poisoning is significantly associated with high temperatures and outdoor spaces, without considering any age group. Carbon monoxide saturation (SPCO%) was 14.1% in the blood of respondents from the food industry, which is also higher than the standard. This may be due to laborers’ long-time exposure to gas fires, boilers and central heating systems. Even 12% carbon monoxide saturation is a fatal concentration according to the CO level chart. CO gas inhalation may lead to unconsciousness and in some; high exposure may cause the death of individuals.
The Rad-57 Masimo Corporation (Irvine, CA, USA) allows noninvasive and instantaneous measurement of carboxyhemoglobin (COHb) and methemoglobin (MetHb) percentage level using a finger probe [29].
A previous study reported 307 CO poisoning cases from Shanghai Public Security Bureau, an official organization that handles the most complicated and life-threatening cases across Shanghai municipality in China, and regrouped these cases into three categories: group 1, 10% < COHb% < 30% (n = 58); group 2, 30% ≤ COHb% < 50% (n = 79); group 3, COHb% ≥ 50% (n = 170). Our results showed that assignment to groups two and three were mostly observed in younger victims (≤30 years), while assignment to group one was equally distributed among all age groups (p = 0.03). All the CO poisoning from groups two and three occurred in enclosed spaces, whereas cases from group one died in outdoor spaces (p = 0.01). in this case study some individuals, died due to fire, while only 45.57% of deaths from group two and 30.59% of deaths. From group three were fire-related (p = 0.00). Accordingly, This group was mostly associated with fire burns, while groups two or three were largely associated with gas leakage (p = 0.00). A combination with alcohol, but not other psychotropic drugs, was associated with significantly higher levels of blood COHb% in fire-unrelated (p = 0.021) but not fire-related cases (p = 0.23). Five extremely low COHb%- (<30%) related poisoning deaths were negative for any cardiopulmonary pathology or psychoactive substances. In conclusion, CO poisoning with low COHb% is significantly associated with fire circumstances and outdoor spaces and has no age preference [30].
Another study regarding the measurement of carboxyhemoglobin and methemoglobin using a noninvasive pulse CO-oximeter depicted that RAD-57 provides a reading that is between −6% and +4% of the true COHb value for 95% of all samples. Rad-57 appears to be a useful rapid and noninvasive method for initial screening of the patients arriving to the emergency department with suspected carbon monoxide intoxication. However, when the readings of SpCO are ≥15% with Rad-57, a second screening with blood drawing should be performed to ascertain carbon monoxide poisoning [31].
The acute CO poisoning was associated with the temperature in Taiwan, where an RR-0.0973 value is less than one, indicating less environmental impact [32]. In the current study, the calculated value of RR was 1.44 for CO poisoning as mentioned in Table 2, which could have severe effects on the health of respondents of steel industries at Hattar. Another study was conducted in Kuwait, where 63% of the deceased were males subjected to CO poisoning, and the disease percentage was 29 percent [33]. Long-term neurocognitive deficits occur in 15–40% of patients, whereas approximately one-third of moderate to severely poisoned patients exhibit cardiac dysfunction, including arrhythmia, left ventricular systolic dysfunction and myocardial infarction [34]. Patients with carbon monoxide poisoning (COP) commonly have long-term morbidities [35]. High-flow oxygen may be sufficient to treat patients with CO poisoning where hyperbaric oxygen is not available [36].
Findings from statistical modelling in the current study indicated that dermatosis and respiratory diseases were more prevalent with a frequency and percentage of 35 and 23.3% and 25 and 16.7%, respectively, and with statistical modelling—attributable proportions—of 65.77% and 61.12%, respectively, in laborers of the Hattar industrial units who were exposed for a longer time to high concentrations of carbon monoxide as compared to the control site. The attributable proportion or health risk factor (AR) is a statistical finding which assures the association of disease with the presence of specific pollutant [37,38].
5. Conclusions
Noninvasive carbon monoxide saturation (SPCO%) in 150 respondents of testing sites (steel, processing and food industries) was comparatively much higher than that of the respondents of the control site (Sultan pur) who were not exposed to such high carbon monoxide concentrations. Carbon monoxide saturation that was higher than the standard concentration showed that respondents of testing sites were exposed to high emissions of carbon monoxide on a daily basis for longer time duration. Regarding gender, 60% were male respondents and 40% were female. Respiratory and skin issues were more prevalent in respondents who were exposed for a longer time duration. In the steel industry, the maximum SpCO% was 17 percent, which is extremely high and indicated that individuals with potential disease risk are more vulnerable to current Pandemic due to high air emissions due to incomplete combustion and low quality fuels. Therefore, there is a need to mitigate health impacts due to high carbon monoxide concentrations being generated inside industrial units by modifying appliances and banning on plastic tire-burning as a source of alternative biofuels and technology based solutions to reduce the air pollution effects at the time of energy crisis in the study area. The burning of such materials (as an alternate source of energy), which deteriorates both ambient air quality and the health of industrial employees, needs to be banned. So, There is need of time to explore alternate ecofriendly energy sources, and permanent monitoring system to monitor the ambient air quality on regular basis by the Environmental Protection Agency (EPA) and community mobilization is necessary to mitigate the alarming levels of air emissions from industries as well country.
Author Contributions
Conceptualization, S.J. and S.N.; methodology, S.J.; software, S.N. validation, Q.M.; formal analysis, A.R.; writing—original draft preparation, S.J.; writing, S.N., review and editing, S.N.; visualization, S.S. and A.Z.; supervision, S.N.; project administration, COMSATS University Islamabad, Abbottabad Campus. All authors have read and agreed to the published version of the manuscript.
Funding
This research equipment’s, sampling, financial components were done through HEC_ NRPU, 9519, National Research Program for Universities awarded to Shamyla Nawazish and funded by the Higher Education Commission, Islamabad.
Institutional Review Board Statement
The ethical biosafety statement has been attached.
Informed Consent Statement
In this study, no animals were involved. Noninvasive blood sampling has been performed using the Masimo Rad-57 Pulse CO-Oximeter.
Data Availability Statement
These data have been obtained through intact digital CO Oximeter and did not involve extraction of blood from humans. The standard values were obtained from the World Health Organization and Environment Protection Agency as reference standard to check the permitted limit of CO generated through different industrial units. The supporting literature is under: https://doi.org/10.1016/j.resp.2012.05.010 (accessed on 4 February 2022); https://doi.org/10.3390/ijerph17124512 (accessed on 4 February 2022); https://www.researchgate.net/publication/325646432 (accessed on 4 February 2022).
Acknowledgments
We pay our sincere gratitude to the Higher Education Commission (HEC) Islamabad, Pakistan for the funding of NRPU research project, and thankful to Hattar Industrial Estate Association for facilitating these research activities and contributors/authors who have made a positive contribution to this research.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
| (ppm) | parts per million |
| The Food and Drug Administration | FDA- |
| Carboxyhemoglobin by pulse oximeter | (SPCO®) |
| Standard laboratory blood measurement | (COHb) |
| Cardiovascular disease | CV |
| Perfusion index ratio | (PI) |
| GIT | Gastrointestinal tract |
| Ppb | Parts per billion |
| CO | Carbon monoxide |
| PM | Particulate matter |
| O3 | Ozone |
| NO2 | Nitrogen dioxide |
| SO2 | Sulfur dioxide |
References
- Fidaev, D.T.; Khunarov, A.M.; Kuchkarova, N.X. Air pollution and its consequences for human health. J. Educ. Res. 2021, 2, 2. [Google Scholar]
- Bala, G.P.; Rajnoveanu, R.M.; Tudorache, E.; Motișan, R.; Oancea, C. Air pollution exposure—The (in) visible risk factor for respiratory diseases. Environ. Sci. Pollut. Res. 2019, 26, 12280–12287. [Google Scholar]
- Dias, C.; Marques, M.; Santos, V.; Tavares, A.S. Spectrophotometric determination of carboxyhaemoglobin in a sample of automobile mechanics occupationally exposed to carbon monoxide. Res. Netw. Health 2018, 1, 1–7. [Google Scholar]
- Oliverio, S.; Varlet, V.; Zeka, A.; Leonardi, G. PI-3-9 The burden of carbon monoxide exposure on public health: Evaluating the role of carboxyhaemoglobin (cohb) as a biomarker and exploring new approaches for quantification. Occup. Environ. Med. 2018, 75, 31–39. [Google Scholar]
- Hoy, R.F.; Glass, D.C.; Dimitriadis, C.; Hansen, J.; Hore-Lacy, F.; Sim, M.R. Identification of early-stage silicosis through health screening of stone benchtop industry workers in Victoria, Australia. Occup. Environ. Med. 2021, 78, 296–302. [Google Scholar] [CrossRef] [PubMed]
- Kantor, D.B.; Petty, C.R.; Phipatanakul, W.; Gaffin, J.M. Transcutaneous CO-oximetry differentiates asthma exacerbation and convalescence in children. J. Allergy Clin. Immunol. 2018, 142, 676–678. [Google Scholar] [CrossRef] [Green Version]
- Chen, L.; Li, J.; Pang, X.; Shi, K.; Chen, J.; Wang, J.; Xu, M. Impact of COVID-19 Lockdown on Air Pollutants in a Coastal area of the Yangtze River Delta: China. Measured by Low-Cost Sensor Package. Atmosphere 2021, 12, 345. [Google Scholar] [CrossRef]
- Acharya, S.P.; Purpura, A.; Kao, L.; House, D. RIncidence and risk factors for carbon monoxide poisoning in an emergency department in Nepal. Toxicol. Commun. 2022, 6, 13–19. [Google Scholar] [CrossRef]
- Martinasek, M.P.; Calvanese, A.V.; Lipski, B.K.A. Naturalistic Study of Carbon Monoxide, Heart Rate, Oxygen Saturation, and Perfusion Index in Hookah Lounge Patrons. Respir. Care 2021, 66, 269–274. [Google Scholar] [CrossRef]
- Bahng, Y.; Baek, K.; Park, J.T.; Choi, W.J.; Kwak, K. Carbon Monoxide Poisoning and Developing Ischemic Heart Disease: A Nationwide Population-Based Nested Case-Control Study. Toxics 2021, 9, 239. [Google Scholar] [CrossRef]
- Diaz-Canestro, C.; Pentz, B.; Sehgal, A.; Montero, D. Sex Differences in Orthostatic Tolerance Are Mainly Explained by Blood Volume and Oxygen Carrying Capacity. Crit. Care Explor. 2022, 9, 1. [Google Scholar] [CrossRef] [PubMed]
- Cloyd, T.; Davidson, C.; LoVecchio, F. Carbon Monoxide Exposure: Evaluation and Management. Emerg. Med. Rep. 2021, 42, 24. [Google Scholar]
- Zaouter, C.; Zavorsky, G.S. The measurement of carboxyhemoglobin and methemoglobin using a non-invasive pulse CO-oximeter. Respir. Physiol. Neurobiol. 2012, 182, 88–92. [Google Scholar] [CrossRef]
- World Health Organization. WHO Global Air Quality Guidelines: Particulate Matter (PM2.5 and PM10), Ozone, Nitrogen Dioxide, Sulfur Dioxide and Carbon Monoxide 2021; WHO: Geneva, Switzerland, 2021. [Google Scholar]
- Townsend, C.L.; Maynard, R.L. Effects on health of prolonged exposure to low Concentrations of carbon monoxide. Occup. Environ. Med. 2021, 59, 708–711. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mukhopadhyay, S.; Hirsch, A.; Etienne, S.; Melnikova, N.; Wu, J.; Sircar, K.; Orr, M. Surveillance of carbon monoxide-related incidents—Implications for prevention of related illnesses and injuries, 2005–2014. Am. J. Emerg. Med. 2018, 36, 1837–1844. [Google Scholar] [CrossRef] [PubMed]
- Raub, J.A.; Mathieu-Nolf, M.; Hampson, N.B.; Thom, S.R. Carbon monoxide poisoning—A public health perspective. J. Toxicol. 2000, 145, 1–14. [Google Scholar] [CrossRef]
- Quarmby, S.; Georgina, S.; Megan, M. Air Quality Strategies and Technologies: A Rapid Review of the International Evidence. Sustainability 2019, 11, 2757. [Google Scholar] [CrossRef] [Green Version]
- Bourdrel, T.; Annesi-Maesano, I.; Alahmad, B.; Maesano, C.N.; Bind, M.A. The impact of outdoor air pollution on COVID-19: A review of evidence from in vitro, animal, and human studies. Eur. Respir. Rev. 2021, 30, 200242. [Google Scholar] [CrossRef]
- Nilsson, L.J.; Bauer, F.; Åhman, M.; Andersson, F.N.; Bataille, C.; de la Rue du Can, S.; Vogl, V. An industrial policy framework for transforming energy and emissions intensive industries towards zero emissions. Clim. Policy 2021, 21, 1053–1065. [Google Scholar] [CrossRef]
- Andersson, K.; Busch Paulsson, E. Accuracy Validation of Pulse Oximeters Used at Hospitals: A Cross-Sectional Study performed in Stockholm; School of Technology and Health, Royal Institute of Technology: Stockholm, Sweden, 2017. [Google Scholar]
- Masimo Corp. Masimo SET Rad 57 Pulse CO-Oximeter. 510(k) Summary of the Safety and Efficacy. Available online: http://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfPMN/pmn.cfm (accessed on 10 August 2010).
- Verweij, B.G.F.; Rood, P.P.M.; Schuit, S.C.E.; Bouwhuis, M.G. Waterpipe smoking: Not as innocent as it may seem. Neth. J. Med. 2019, 77, 156–159. [Google Scholar]
- Yildiz, L.A.; Gultekingil, A.; Kesici, S.; Bayrakci, B.; Teksam, O. Predictors of severe clinical course in children with carbon monoxide poisoning. Pediatr. Emerg. Care 2021, 37, 308–311. [Google Scholar]
- Marvel, S.W.; House, J.S.; Wheeler, M.; Song, K.; Zhou, Y.H.; Wright, F.A.; Reif, D.M. The COVID-19 Pandemic Vulnerability Index (PVI) Dashboard: Monitoring county-level vulnerability using visualization, statistical modeling, and machine learning. Environ. Health Perspect. 2021, 129, 017701. [Google Scholar] [CrossRef] [PubMed]
- Okagbue, H.I.; Oguntunde, P.E.; Obasi, E.C.; Akhmetshin, E. MTrends and usage pattern of SPSS and Minitab Software in Scientific research. J. Phys. Conf. Ser. 2021, 1734, 012017. [Google Scholar] [CrossRef]
- Faustini, A.; Davoli, M. Attributable Risk to Assess the Health Impact of Air Pollution: Advances, Controversies, State of the Art and Future Needs. Int. J. Environ. Res. 2020, 17, 4512. [Google Scholar] [CrossRef]
- Kim, D.; Chen, Z.; Zhou, L.F.; Huang, S.X. Air pollutants and early origins of respiratory diseases. Chronic Dis. 2018, 4, 75–94. [Google Scholar] [CrossRef] [PubMed]
- Simonsen, C.; Magnusdottir, S.O.; Andreasen, J.J.; Wimmer, R.; Rasmussen Kjærgaard, B.S.B.; Maltesen, R.G. Metabolic changes during carbon monoxide poisoning, An experimental study. J. Cell. Mol. Med. 2021, 11, 5191–5201. [Google Scholar] [CrossRef] [PubMed]
- Gokhale, S.G.; Daggubati, V.S. Spectrometry of cord blood and maternal blood for Hb-F and Hb-A and novel technology for non-invasive measurement of hemoglobin in mother and baby. J. Matern. Fetal Neonatal. Med. 2021, 35, 1–4. [Google Scholar] [CrossRef]
- Maisel, W.H.; Lewis, R.J. Noninvasive measurement of carboxyhemoglobin: How accurate is accurate enough. Ann. Emerg. Med. 2010, 56, 389–391. [Google Scholar] [CrossRef]
- Liu, Z.; Meng, H.; Huang, J.; Kwangwari, P.; Ma, K.; Xiao, B.; Li, L. Acute carbon monoxide poisoning with low saturation of carboxyhaemoglobin: A forensic retrospective study in Shanghai, China. Sci. Rep. 2021, 11, 18554. [Google Scholar] [CrossRef]
- Rose, J.J.; Wang, L.; Xu, Q.; McTiernan, C.F.; Shiva, S.; Tejero, J.; Gladwin, M.T. Carbon monoxide poisoning: Pathogenesis, management, and future directions of therapy. Am. J. Respir. Crit. 2017, 195, 596–606. [Google Scholar] [CrossRef]
- Aoshima, K.; Yamaoka, H.; Nakamura, S.; Nojima, T.; Naito, H.; Nakao, A. Right hemiplegia following acute carbon monoxide poisoning. Cureus 2021, 7, 7759–16738. [Google Scholar] [CrossRef]
- Wang, H.; Hao, S.C.S.; Chang, K.C.; Hung, M.; Yang, C.C.; Liao, S.C. Quantifying the Effects of Climate Factors on Carbon Monoxide Poisoning: A Retrospective Study in Taiwan. Front. Public Health 2021, 14, 1537. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Lu, Q.; Jia, J.; Xiang, D.; Xi, Y. Multicenter retrospective analysis of the risk factors for delayed neurological sequelae after acute carbon monoxide poisoning. Am. J. Emerg. Med. 2021, 46, 165–169. [Google Scholar] [CrossRef] [PubMed]
- Carrol, R.; Prentice, C.R. Community vulnerability and mobility: What matters most in spatio-temporal modeling of the COVID-19 pandemic? Soc. Sci. Med. 2021, 287, 114395. [Google Scholar] [CrossRef] [PubMed]
- Yarragunta, Y.; Srivastava, S.; Mitra, D.; Chandola, H.C. Source apportionment of carbon monoxide over India: A quantitative analysis using mozart-4. Environ. Sci. Pollut. Res. 2021, 28, 8722–8742. [Google Scholar] [CrossRef] [PubMed]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).