Air Quality Levels and Health Risk Assessment of Particulate Matters in Abuja Municipal Area, Nigeria



Abstract
1. Introduction
2. Methodology
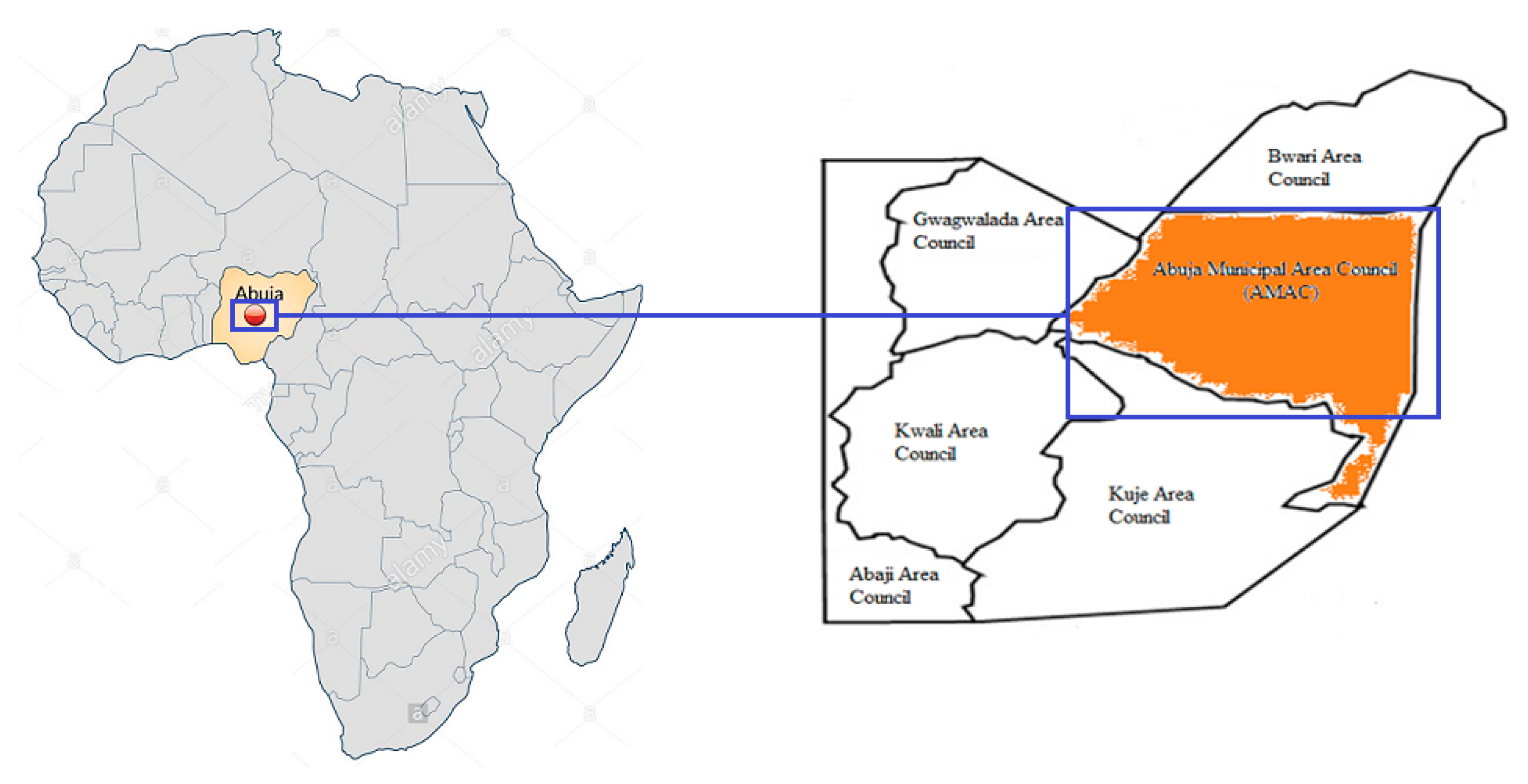
2.1. Research Area
2.2. Sampling
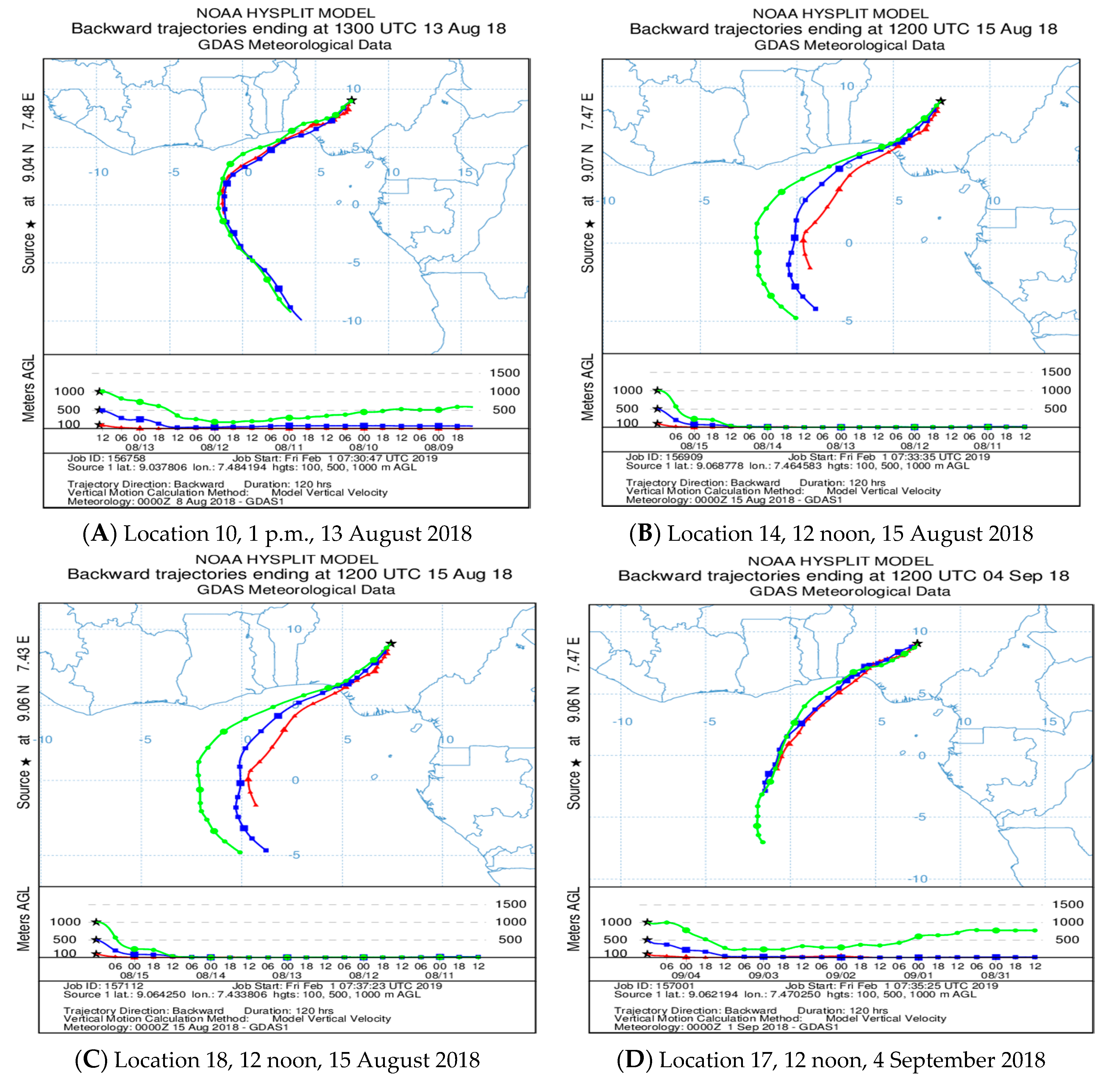
2.3. Hybrid Single Particle Lagrangian Integrated Trajectory (HYSPLIT) Model
2.4. Risk Assessment
3. Results
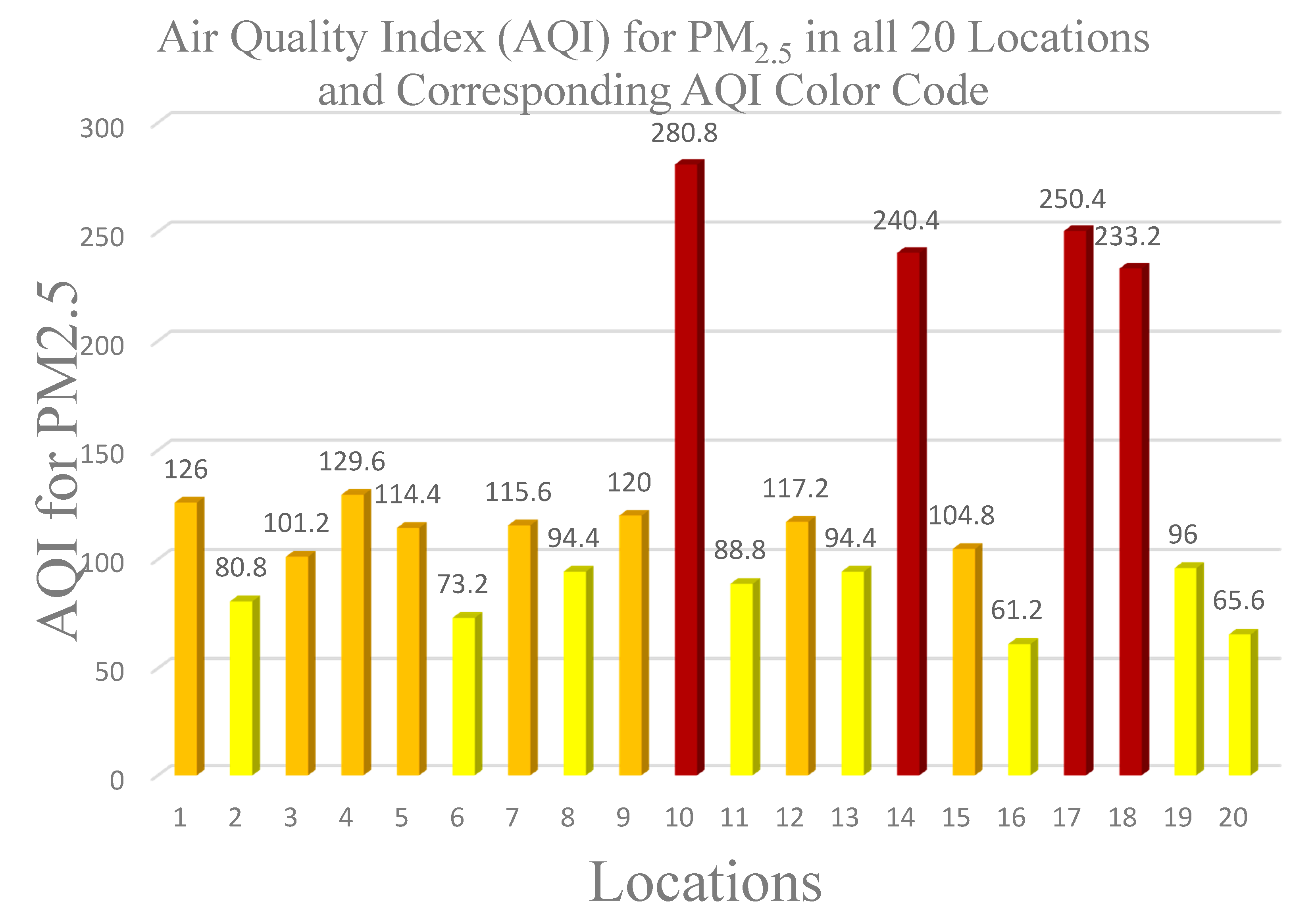
3.1. Particulate Matters (PM) Concentrations
3.2. Spatial Variation
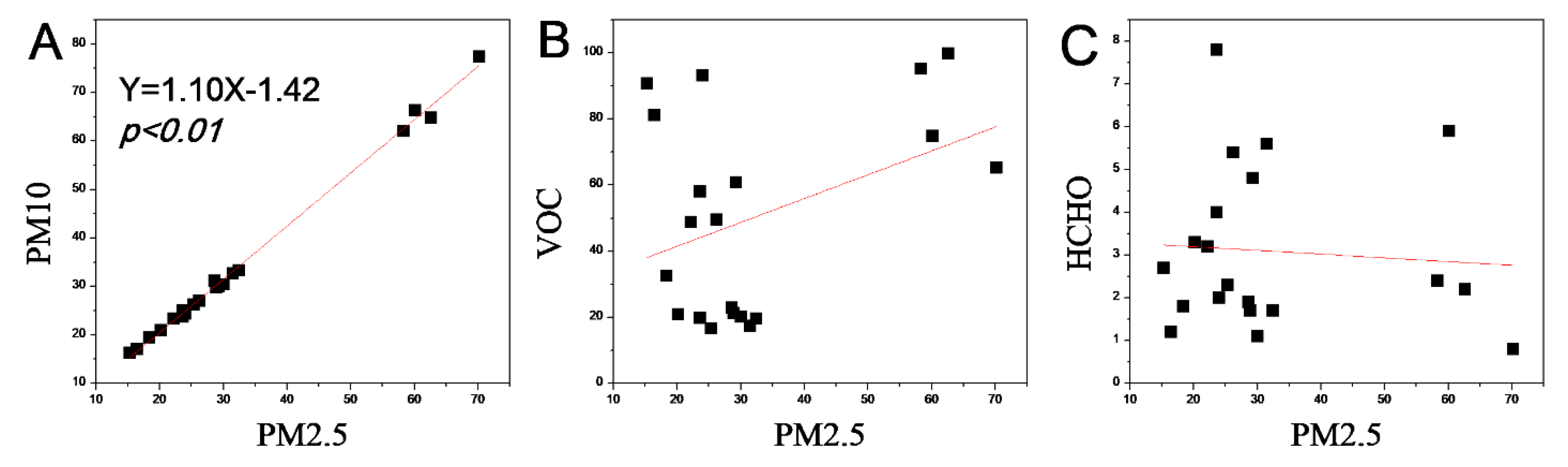
3.3. PM2.5 Relationship with PM10, VOCs and HCHO
3.4. Source Appointment—Backward Air Flow Trajectory
- PM2.5 has the lowest mean value of 15.30 µg/m3 and 70.20 µg/m3 as the highest value. However, going by the WHO standard of 25 µg/m3 24 h mean, 12 of the 20 location had a mean value higher than the standard with 8 having values lower than the standard;
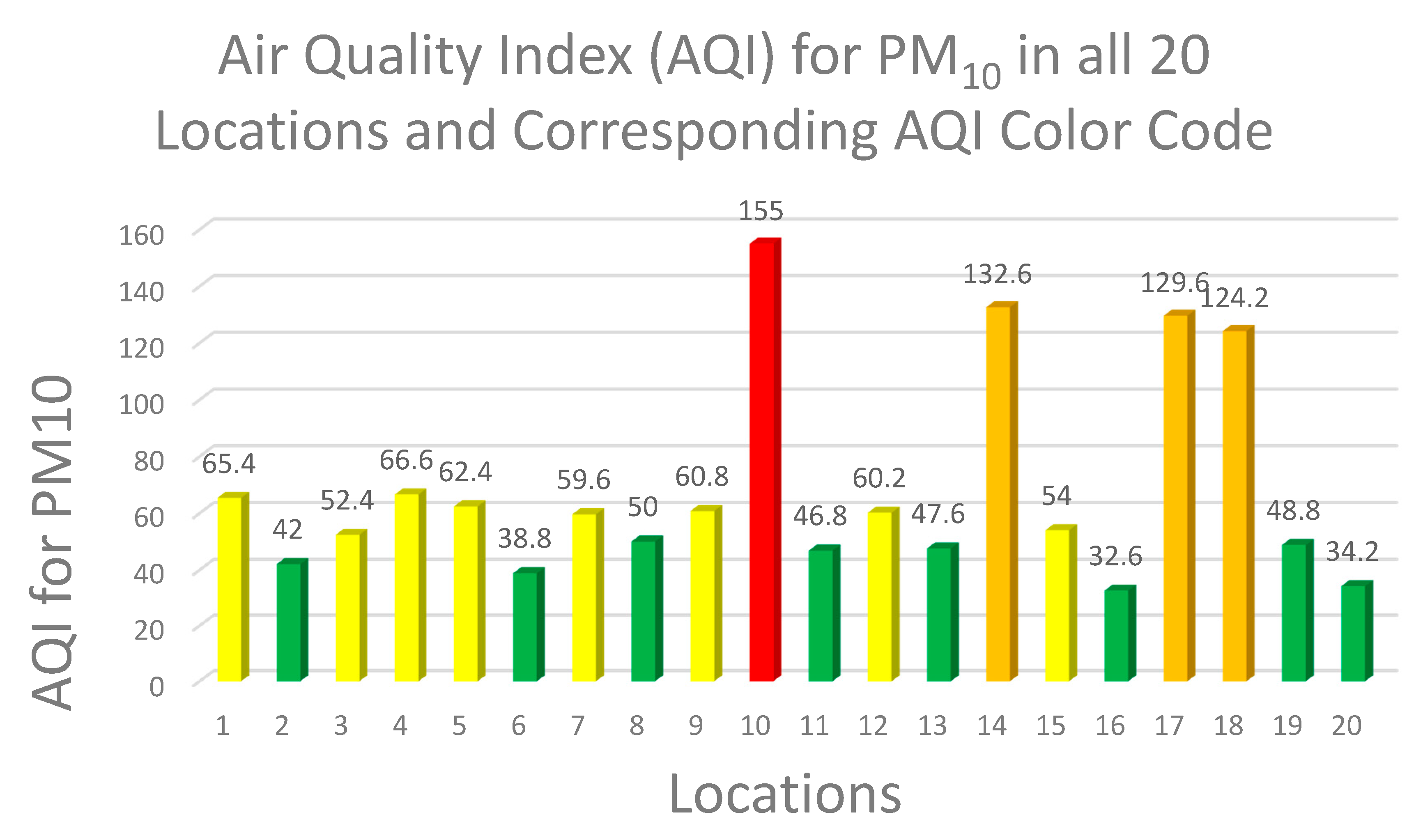
- PM10– of the 20 locations, 16 location were below the 50 µg/m3 WHO standard 24 h mean value while 4 locations were higher than the standards. The highest mean value was 77.50 µg/m3 with 16.30 µg/m3 as the lowest;
4. Relative Humidity, Temperature, Volatile Organic Compounds (VOCs) and Formaldehyde (HCHO)
- Short term exposure (hours to days): eye, nose and throat irritation, headaches, nausea/vomiting, dizziness, visual disorders and memory impairment, worsening of asthma symptoms;
- Chronic exposure (years to a lifetime): cancer, liver and kidney damage, central nervous system damage.
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- WHO. Factsheet on Ambient Air Quality and Health; WHO: Geneva, Switzerland, 2018; Available online: http://www.who.int/news-room/fact-sheets/detail/ambient-(outdoor)-air-quality-and-health (accessed on 4 October 2018).
- Chen, B.; Kan, H. Air Pollution and population health: A global challenge. Environ. Health Prev. Med. 2008, 13, 94–101. [Google Scholar]
- Health Effects Institute. State of Global Air 2019; Special Report; Health Effects Institute: Boston, MA, USA, 2019; ISSN 2578-6873. [Google Scholar]
- WHO. Air Pollution: Ambient Air Pollution: Health Impacts; WHO: Geneva, Switzerland, 2018; Available online: https://www.who.int/airpollution/ambient/health-impacts/en/ (accessed on 4 October 2018).
- Cohen, A.J.; Brauer, M.; Burnett, R.; Anderson, H.R.; Frostad, J.; Estep, K.; Balakrishnan, K.; Brunekreef, B.; Dandona, L.; Dandona, R.; et al. Estimates and 25-year trends of the global burden of disease attributable to ambient air pollution: An analysis of data from the Global Burden of Diseases Study 2015. Lancet 2017, 389, 1907–1918. [Google Scholar]
- U.S. EPA. Particulate Matter (PM) Pollution; U.S. EPA: Washington, DC, USA, 2017. Available online: https://www.epa.gov/pm-pollution/particulate-matter-pm-basics (accessed on 15 December 2019).
- Andrella Tersoo 2018. Available online: https://www.naija.ng/1176017-causes-effects-air-pollution-nigeria.html#1176017 (accessed on 4 October 2018).
- Aga, C. Nigeria: State by State. 2009. Available online: www.nigeriabookofrecords.com (accessed on 11 October 2018).
- Abuja Population. 17 December 2017. Available online: http://worldpopulationreview.com/world-cities/abuja/ (accessed on 11 October 2018).
- E+E Elecktronik. Omniport 30. 2019. Available online: http://downloads.epluse.com/fileadmin/data/product/omniport30/datasheet_Omniport30.pdf (accessed on 15 June 2020).
- BLATN. Product-BLATN Air Quality Monitoring: BR-Smart Air Quality Detector. 2018. Available online: http://www.blatn.com/Content/details/id/904.html (accessed on 12 October 2018).
- GMM Technoworld Pte Ltd. BRAMC 4-in-1 Air Quality Monitor PM2.5 PM10 Formaldehyde (HCHO) VOCs; GMM Technoworld Pte Ltd.: Trivex, Singapore, 2018; Available online: https://www.testmeter.sg/products/BRAMC-4-in-1-Air-Quality-Monitor-PM2.5-PM10-Formaldehyde-(HCHO)-VOCs/537 (accessed on 12 October 2018).
- Shan, W.P.; Yin, Y.Q.; Lu, H.X.; Liang, S.X. A Meteorological analysis of ozone episodes using HYSPLIT model and surface data. Atmos. Res. 2009, 93, 767–776. [Google Scholar]
- Li, M.M.; Huang, X.; Zhu, L.; Li JFSong, Y.; Cai, X.H.; Xie, S.D. Analysis of the transport pathways and potential sources of PM10 in Shanghai based on three methods. Sci. Total Environ. 2012, 414, 525–534. [Google Scholar]
- Zemmer, F.; Karaca, F.; Ozkaragoz, F. Ragweed pollen observed in turkey: Detection of sources using back trajectory models. Sci. Total Environ. 2012, 430, 101–108. [Google Scholar]
- Air Resources Laboratory. HYSPLIT-2; Air Resources Laboratory: Silver Spring, MD, USA, 2019. Available online: https://www.arl.noaa.gov/hysplit/hysplit/ (accessed on 11 February 2019).
- Ready.arl.noaa.gov.READY—Real-time Environmental Applications and Display sYstem. 2019. Available online: https://ready.arl.noaa.gov/index.php (accessed on 11 February 2019).
- U.S. EPA. Air Quality Index (AQI). A Guide to Air Quality and Your Health; EPA-456/F-14-002; U.S. Environmental Protection Agency Office of Air Quality Planning and Standards Outreach and Information Division Research: Triangle Park, NC, USA, 2014; pp. 1–12. [Google Scholar]
- U.S. EPA. Air Quality Index—A Guide to Air Quality and Your Health; Brochure; EPA-456/F-14-002; U.S. EPA: Washington, DC, USA, 2014. Available online: https://www3.epa.gov/airnow/aqi_brochure_02_14.pdf (accessed on 18 October 2018).
- Longinus, N.K.; John, R.T.; Olatunde, A.M.; Alex, A.A.; Omosileola, J.A. Ambient Air Quality Monitoring in Metropolitan City of Lagos, Nigeria. J. Appl. Sci. Environ. Manage. March. 2016, 20, 178–185. [Google Scholar]
- AirNow. AirNow.gov—Home of the Air Quality Index: AQI Basics. 2018. Available online: https://airnow.gov/aqi/aqi-basics (accessed on 18 October 2018).
- AirNow. AQI to Concentration Calculator. 2018. Available online: https://www.airnow.gov/aqi/aqi-calculator (accessed on 18 October 2018).
- OECD.Stat. Exposure to PM2.5 in Countries and Regions: Exposure to PM2.5 in Macroregions. 2018. Available online: https://stats.oecd.org/index.aspx?queryid=72722 (accessed on 23 May 2019).
- Dominici, F.; Peng, R.D.; Bell, M.L.; Pham, L.; McDermott, A.; Zeger, S.L.; Samet, J.M. Fine particulate air pollution and hospital admission for cardiovascular and respiratory diseases. J. Am. Med. Assoc. 2006, 295, 1127–1134. [Google Scholar]
- Yang, W.; Wang, G.; Bi, C. Analysis of longrange transport effects on PM2.5 during a short severe haze in Beijing, China. Aerosol. Air Qual. Res. 2017, 17, 1610–1622. [Google Scholar]
- Yang, X.; Jiang, L.; Zhao, W.; Xiong, Q.; Zhao, W.; Yan, X. Comparison of Ground-Based PM2.5 and PM10 Concentrations in China, India, and the U.S. Int. J. Environ. Res. Public Health 2018, 15, 1382. [Google Scholar]
- Li, R.; Zhou, R.; Zhang, J. Function of PM2.5 in the pathogenesis of lung cancer and chronic airway inflammatory diseases. Oncol. Lett. 2018, 15, 7506–7514. [Google Scholar]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Erlbaum: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Zhou, T.; Sun, J.; Yu, H. Temporal and spatial patterns of China’s main air pollutants: Years 2014 and 2015. Atmosphere 2017, 8, 137. [Google Scholar]
- Perrone, M.R.; Becagli, S.; Orza JGVecchi, R.; Dinoi, A.; Udisti, R.; Cabello, M. The impact of long-range-transport on PM1 and PM2.5 at a central Mediterranean site. Atmos. Environ. 2013, 71, 176–186. [Google Scholar]
- Dublin-Green, C.O.; Awosika, L.F.; Folorunsho, R. Climate Variability Research Activities in Nigeria; Nigerian Institute for Oceanography and Marine Research: Victoria Island, Lagos, Nigeria, 1999. [Google Scholar]
- David, O.; Charles, O.; Esu, O. Estimating greenhouse gas emissions from port vessel operations at the Lagos and Tin Can ports of Nigeria. Cogent Eng. 2018, 5, 1507267. [Google Scholar]
- Oyedepo, S.O. Towards achieving energy for sustainable development in Nigeria. Renew. Sustain. Energy Rev. 2014, 34, 255–272. [Google Scholar]
- U.S. EIA (United States Energy Information Administration). Country Analysis Brief: Nigeria; U.S. EIA: Washington, DC, USA, May 2016. Available online: https://www.eia.gov/beta/international/analysis_includes/countries_long/Nigeria/nigeria.pdf (accessed on 6 March 2019).
- Giwa, S.O.; Adama, O.O.; Akinyemi, O.O. Baseline black carbon emissions for gas flaring in the Niger Delta region of Nigeria. J. Nat. Gas Sci. Eng. 2014, 20, 373–379. [Google Scholar]
- McEwen, J.D.; Johnson, M.R. Black carbon particulate matter emission factors for buoyancy-driven associated gas flares. J. Air Waste Manag. Assoc. 2012, 62, 307–321. [Google Scholar]
- Obanijesu, E.; Adebiyi, F.; Sonibare, J.; Okelana, O. Air-borne SO2 pollution monitoring in the upstream petroleum operation areas of Niger-Delta, Nigeria. Energy Sour. Part A 2009, 31, 223–231. [Google Scholar]
- Sonibare, J.; Adebiyi, F.; Obanijesu, E.; Okelana, O. Air quality index pattern around petroleum production facilities. Manag. Environ. Qual. Int. J. 2010, 21, 379–392. [Google Scholar]
- Gobo, A.E.; Richard, G.; Ubang, I.U. Health impact of gas flares on Igwuruta/Umuechem communities in Rivers State. J. Appl. Sci. Environ. Manag. 2009, 13, 27–33. [Google Scholar]
- Ovuakporaye, S.I.; Aloamaka, C.P.; Ojieh, A.E.; Ejebe, D.E.; Mordi, J.C. Effect of gas flaring on lung function among residents in gas flaring community in Delta State, Nigeria. Res. J. Environ. Earth Sci. 2012, 4, 525–528. [Google Scholar]
- Adienbo, O.M.; Nwafor, A. Effect of prolong exposure to gas flaring on some haematological parameters of humans in the Niger Delta Region of Nigeria. J. Appl. Sci. Environ. Manag. 2010, 14, 13–15. [Google Scholar]
- Ristovski, Z.D.; Miljevic, B.; Surawski, N.C.; Morawska, L.; Fong, K.M.; Goh, F.; Yang, I.A. Respiratory health effects of diesel particulate matter. Respirology 2011, 29. [Google Scholar] [CrossRef]
- Ayres, J.G.; Borm, P.; Cassee, F.R.; Castranova, V.; Donaldson, K.; Ghio, A.; Harrison, R.M.; Hider, R.; Kelly, F.; Kooter, I.M.; et al. Evaluating the toxicity of airborne particulate matter and nanoparticles by measuring oxidative stress potential—A workshop report and consensus statement. Inhal. Toxicol. 2008, 20, 75–99. [Google Scholar]
- Mortimer, K.M.; Neas, L.M.; Dockery, D.W.; Redline, S.; Tager, I.B. The effect of air pollution on inner-city children with asthma. Eur. Respir. J. 2002, 19, 699–705. [Google Scholar]
- Jang, A.-S. Particulate Air Pollutants and Respiratory Diseases, Air Pollution—A Comprehensive Perspective, Budi Haryanto; IntechOpen: London, UK, 22 August 2012; pp. 153–174. Available online: https://www.intechopen.com/books/air-pollution-a-comprehensive-perspective/particulate-air-pollutants-and-respiratory-diseases (accessed on 30 November 2018). [CrossRef]
- Pope, C.A.; Dockery, D.W. Health effects of fine particulate air pollution: Lines thatconnect. J. Air Waste Manage. Assoc. 2006, 56, 709–742. [Google Scholar]
- Breysse, P.N.; Diette, G.B.; Matsui, E.C.; Butz, A.M.; Hansel, N.N.; Mc Cormack, M.C. Indoor air pollution and asthma in children. Proc. Am. Thorac. Soc. 2010, 7, 102–106. [Google Scholar]
- U.S. EPA. Volatile Organic Compounds’ Impact on Indoor Air Quality; U.S. EPA: Washington, DC, USA, 2017. Available online: https://www.epa.gov/indoor-air-quality-iaq/volatile-organic-compounds-impact-indoor-air-quality (accessed on 30 November 2018).
- European Commission Joint Research Centre—Environment. Total Volatile Organic Compounds (TVOC) in Indoor Air Quality Investigations; report 19, Brussels1997 Contract No.: EUR 17675 EN; European Commission Joint Research Centre: Ispra, Italy, 1997; Available online: http://ihcp.jrc.ec.europa.eu/our_activities/publichealth/indoor_air_quality/eca/eca_report_19 (accessed on 30 November 2018).
- Environemntal Analtical Sevrices, Inc. Total Volatile Organic Compounds; Environemntal Analtical Sevrices, Inc.: New York, NY, USA, 2015; Available online: https://easlab.com/iaqref.htm (accessed on 15 June 2020).






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| AQI Value of Index | Levels of Health Concern | PM2.5 Conc. (µg/m3) | PM10 Conc. (µg/m3) | Daily AQI Color | Air Pollution Level |
|---|---|---|---|---|---|
| 0–50 | Good | 0–12 | 0–54 | green | Level 1 |
| 51–100 | Moderate | 12.1–35.4 | 55–154 | yellow | Level 2 |
| 101–150 | Unhealthy for sensitive groups | 35.5–55.4 | 155–254 | orange | Level 3 |
| 151–200 | unhealthy | 55.5–150.4 | 255–354 | Red | Level 4 |
| 201–300 | Very unhealthy | 150.5–250.4 | 355–424 | Purple | Level 5 |
| 301 and Higher | Hazardous | 250.5–Higher | 425–Higher | Maroon | Level 6 |
| Location | Location Purpose | GPS Coordinate | Mean Monitoring Readings (µg/m3) | Mean Monitoring Readings (mg/m3) | Humidity (%) | Temp. (°C) | Atm. Pressure (kPa) | ||
|---|---|---|---|---|---|---|---|---|---|
| PM2.5 | PM10 | VOCs | HCHO | ||||||
| 1 | Mixed use | 9.08, 7.47 | 31.50 | 32.70 | 1.74 | 0.56 | 92 | 24 | 101.80 |
| 2 | Residential | 9.09, 7.49 | 20.20 | 21.00 | 2.09 | 0.33 | 90 | 25 | 101.33 |
| 3 | Residential | 8.99, 7.46 | 25.30 | 26.20 | 1.66 | 0.23 | 96 | 22 | 101.55 |
| 4 | Commercial/business | 9.09, 7.49 | 32.40 | 33.30 | 1.96 | 0.17 | 77 | 27 | 101.30 |
| 5 | Mixed use | 9.08, 7.50 | 28.60 | 31.20 | 2.30 | 0.19 | 85 | 26 | 101.60 |
| 6 | Commercial | 9.08, 7.48 | 18.30 | 19.40 | 3.26 | 0.18 | 80 | 24 | 101.70 |
| 7 | Airport | 9.00, 7.27 | 28.90 | 29.80 | 2.12 | 0.17 | 36 | 27 | 101.70 |
| 8 | Commercial | 9.07, 7.49 | 23.60 | 25.00 | 5.80 | 0.40 | 85 | 25 | 101.40 |
| 9 | Commercial/offices | 9.05, 7.50 | 30.00 | 30.40 | 2.02 | 1.10 | 87 | 28 | 101.60 |
| 10 | Business | 9.04, 7.48 | 70.20 | 77.50 | 6.53 | 0.08 | 90 | 24 | 101.60 |
| 11 | Commercial/business | 9.10, 7.41 | 22.20 | 23.40 | 4.88 | 0.32 | 87 | 26 | 101.30 |
| 12 | Offices | 9.05, 7.46 | 29.30 | 30.10 | 6.08 | 0.48 | 87 | 25 | 101.30 |
| 13 | Offices | 9.06, 7.49 | 23.60 | 23.80 | 1.97 | 0.78 | 93 | 24 | 101.60 |
| 14 | Market | 9.07, 7.46 | 60.10 | 66.30 | 7.49 | 0.59 | 91 | 24 | 101.66 |
| 15 | Commercial | 9.07, 7.46 | 26.20 | 27.00 | 4.96 | 0.54 | 90 | 24 | 101.70 |
| 16 | Commercial/business | 9.12, 7.40 | 15.30 | 16.30 | 9.07 | 0.27 | 86 | 26 | 101.30 |
| 17 | Business | 9.06, 7.47 | 62.60 | 64.80 | 9.98 | 0.22 | 80 | 26 | 101.20 |
| 18 | Transport Services | 9.06, 7.43 | 58.30 | 62.10 | 9.53 | 0.24 | 87 | 25 | 101.70 |
| 19 | Business | 9.07, 7.43 | 24.00 | 24.40 | 9.32 | 0.20 | 88 | 25 | 101.70 |
| 20 | Commercial/business | 9.07, 7.43 | 16.40 | 17.10 | 8.12 | 0.12 | 97 | 24 | 101.70 |
| VOCs Conc. (mg/m3) | Level of Health Concern |
|---|---|
| <0.3 | No irritation or discomfort |
| 0.3–0.5 | Irritation and discomfort possible if other exposures interact |
| 0.5–1.0 | Exposure effect and probable headache possible if other exposure interact |
| 1.0–3.0 | Headache and additional neurotoxic effects may occur |
| >3 | Irritation and discomfort are very possible |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wambebe, N.M.; Duan, X. Air Quality Levels and Health Risk Assessment of Particulate Matters in Abuja Municipal Area, Nigeria. Atmosphere 2020, 11, 817. https://doi.org/10.3390/atmos11080817
Wambebe NM, Duan X. Air Quality Levels and Health Risk Assessment of Particulate Matters in Abuja Municipal Area, Nigeria. Atmosphere. 2020; 11(8):817. https://doi.org/10.3390/atmos11080817
Chicago/Turabian StyleWambebe, Nathaniel Mopa, and Xiaoli Duan. 2020. "Air Quality Levels and Health Risk Assessment of Particulate Matters in Abuja Municipal Area, Nigeria" Atmosphere 11, no. 8: 817. https://doi.org/10.3390/atmos11080817
APA StyleWambebe, N. M., & Duan, X. (2020). Air Quality Levels and Health Risk Assessment of Particulate Matters in Abuja Municipal Area, Nigeria. Atmosphere, 11(8), 817. https://doi.org/10.3390/atmos11080817