
Association Study of PDCD1 Gene Variants and Its Gene Expression with Cutaneous Melanoma in a Mexican Population

 , , , ,
, , , ,  and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Population
2.3. Inclusion and Exclusion Criteria
- Patients diagnosed dermatoscopically and histologically with cutaneous melanoma.
- Patients over 18 years of age who voluntarily signed informed consent.
- Patients born in western Mexico (Jalisco, Nayarit, Michoacán, or Colima) with at least two previous generations (parents and grandparents) from those regions.
- Individuals with a history of other cancers, transplant recipients, or immunosuppressed.
- Individuals who had received blood transfusions in the three months prior to sample collection.
- Incomplete molecular typing due to insufficient or degraded samples.
- Voluntary withdrawal from the study.
2.4. Sample Size
- n is the minimum number of individuals required per group;
- Zα = 1.96, is the corresponding to a 5% significance level;
- Zβ = 0.84, is thecorresponding to 80% statistical power;
- S2 = 1.56, is the estimated variance of ΔCt values; and
- d = 1.0, is the minimum difference to detect (equivalent to a 2-fold change in gene expression)
2.5. Molecular Analysis
2.6. mRNA Expression
2.7. Statistical Analysis
2.8. Ethical Considerations
3. Results
3.1. Sociodemographic Characteristics
3.2. Clinical Characteristics of Melanoma Patients
3.3. Genotyping of PDCD1 Variants
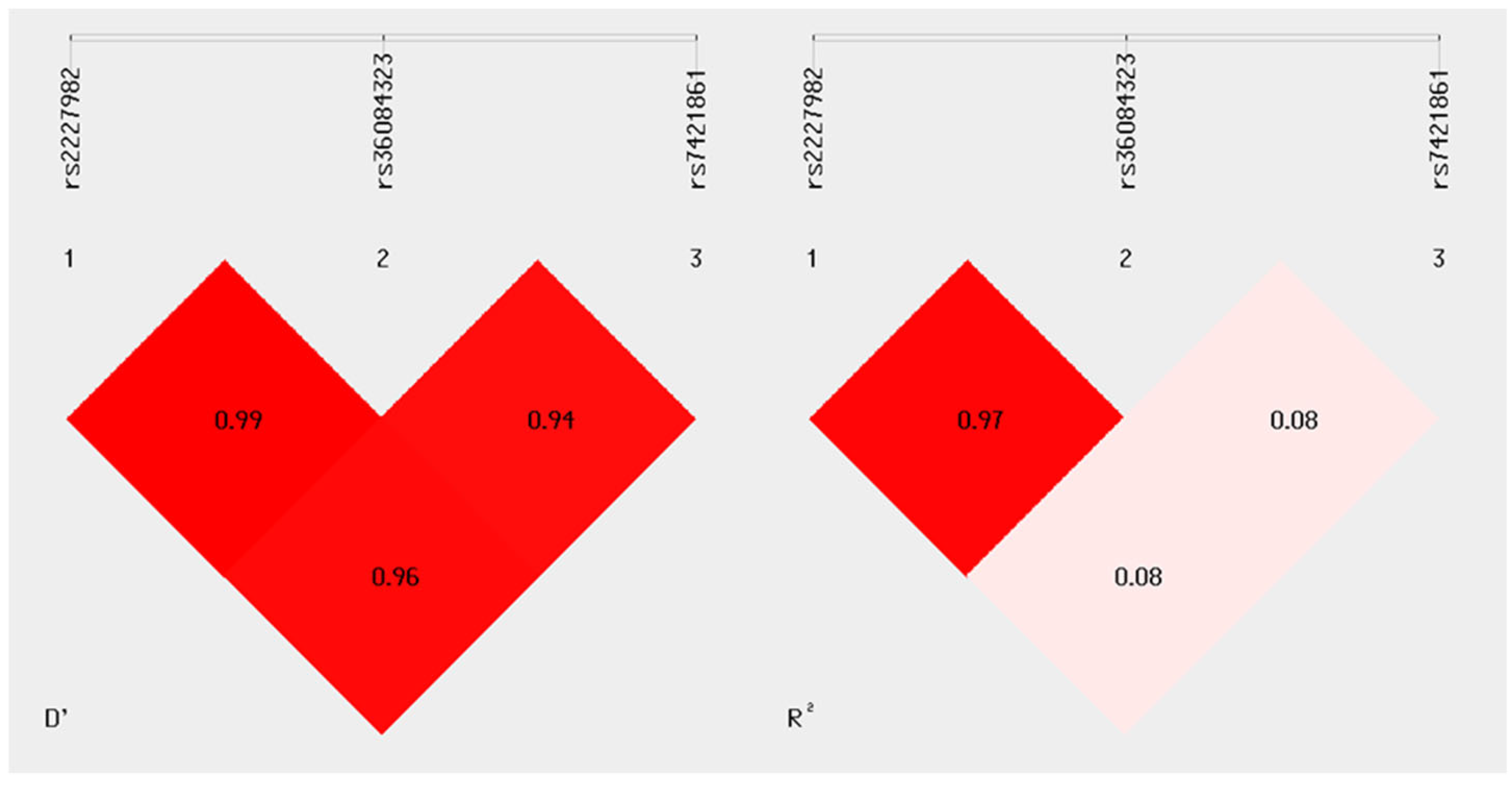
3.4. Linkage Disequilibrium
3.5. Haplotypes
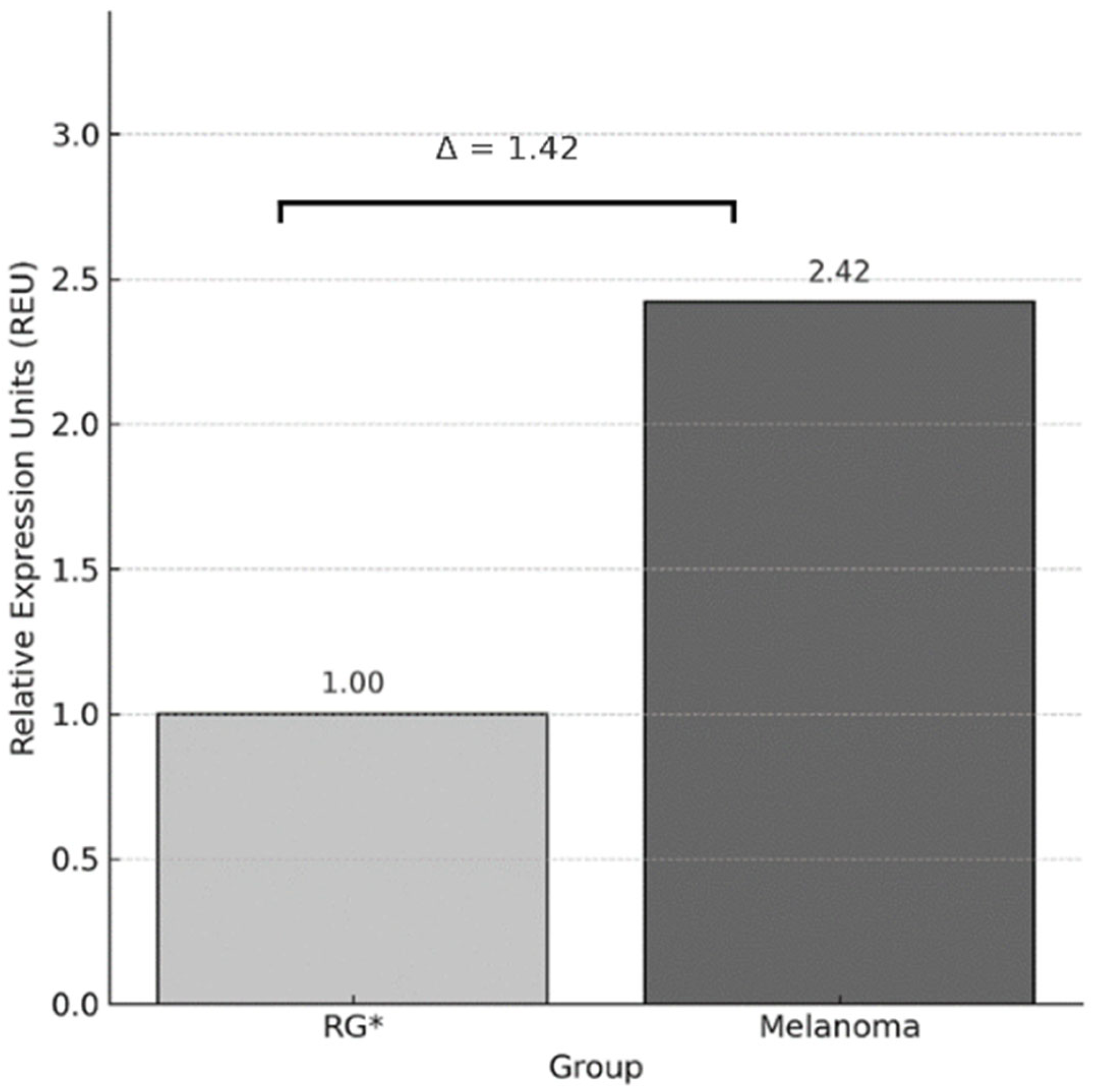
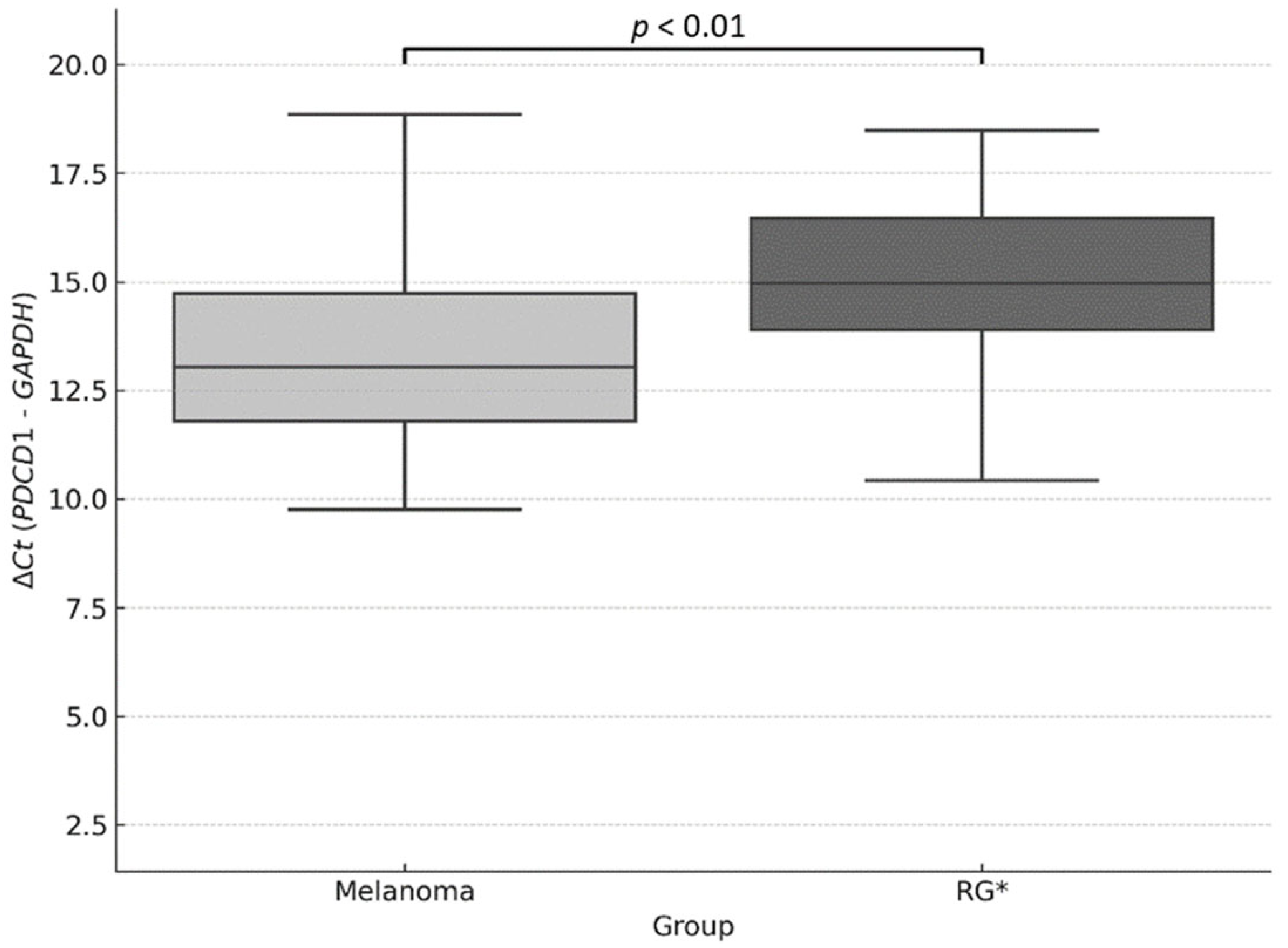
3.6. Relative Expression of PDCD1
3.7. Bivariate Analysis of Clinicopathological Characteristics
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Valdez-Salazar, F.; Jiménez-Del Rio, L.A.; Padilla-Gutiérrez, J.R.; Valle, Y.; Muñoz-Valle, J.F.; Valdés-Alvarado, E. Advances in Melanoma: From Genetic Insights to Therapeutic Innovations. Biomedicines 2024, 12, 1851. [Google Scholar] [CrossRef]
- Collatuzzo, G.; Boffetta, P.; Dika, E.; Visci, G.; Zunarelli, C.; Mastroeni, S.; Antonelli, G.; Fortes, C. Occupational exposure to arsenic, mercury and UV radiation and risk of melanoma: A case–control study from Italy. Int. Arch. Occup. Env. Health 2023, 96, 443–449. [Google Scholar] [CrossRef] [PubMed]
- Rezk, E.; Eltorki, M.; El-Dakhakhni, W. Interpretable Skin Cancer Classification based on Incremental Domain Knowledge Learning. J. Healthc. Inform. Res. 2023, 7, 59–83. [Google Scholar] [CrossRef] [PubMed]
- Macdonald, E.J. Epidemiology of melanoma. Prog. Clin. Cancer 2021, 6, 139–149. [Google Scholar] [CrossRef]
- Zambrano-Román, M.; Padilla-Gutiérrez, J.R.; Valle, Y.; Muñoz-Valle, J.F.; Valdés-Alvarado, E. Non-Melanoma Skin Cancer: A Genetic Update and Future Perspectives. Cancers 2022, 14, 2371. [Google Scholar] [CrossRef]
- Gao, J.; Gai, N.; Wang, L.; Liu, K.; Liu, X.-H.; Wei, L.-T.; Tian, T.; Li, S.-L.; Zheng, Y.; Deng, Y.-J.; et al. Meta-analysis of programmed cell death 1 polymorphisms with systemic lupus erythematosus risk. Oncotarget 2017, 8, 36885–36897. [Google Scholar] [CrossRef]
- Wagner, M.; Jasek, M.; Karabon, L. Immune Checkpoint Molecules—Inherited Variations as Markers for Cancer Risk. Front. Immunol. 2021, 11, 606721. [Google Scholar] [CrossRef]
- Lasithiotakis, K.G.; Petrakis, I.E.; Garbe, C. Cutaneous melanoma in the elderly: Epidemiology, prognosis and treatment. Melanoma Res. 2010, 20, 163–170. [Google Scholar] [CrossRef]
- Whiteman, D.C.; Green, A.C.; Olsen, C.M. The Growing Burden of Invasive Melanoma: Projections of Incidence Rates and Numbers of New Cases in Six Susceptible Populations through 2031. J. Investig. Dermatol. 2016, 136, 1161–1171. [Google Scholar] [CrossRef]
- Cámara-Salazar, A.; Paola Santos-Zaldívar, K.; Bracamonte-Barahona, R.; Sttephy Calderón-Sauri, I.; Fernanda Flores-Mendoza, K.; Mijangos-Vergara, F.; Méndez-Domínguez, N.I. Individual and by federal entity characteristics of mortality due to melanoma in Mexico from 2014 to 2018 n.d. Dermatol. Rev. Mex. 2020, 64, 248–254. [Google Scholar]
- Andrulonis, R.; Secrest, A.M.; McGuire, S.T.; Geskin, L.J.; Ferris, L.K. The Influence of Age and Sex on Reasons for Seeking and Expected Benefits of Skin Cancer Screening. Arch. Dermatol. 2010, 146, 1097–1102. [Google Scholar] [CrossRef]
- Joosse, A.; de Vries, E.; Eckel, R.; Nijsten, T.; Eggermont, A.M.M.; Hölzel, D.; Coebergh, J.W.W.; Engel, J. Gender Differences in Melanoma Survival: Female Patients Have a Decreased Risk of Metastasis. J. Investig. Dermatol. 2011, 131, 719–726. [Google Scholar] [CrossRef] [PubMed]
- Leonardi, G.C.; Falzone, L.; Salemi, R.; Zanghì, A.; Spandidos, D.A.; Mccubrey, J.A.; Candido, S.; Libra, M. Cutaneous melanoma: From pathogenesis to therapy (Review). Int. J. Oncol. 2018, 52, 1071–1080. [Google Scholar] [CrossRef] [PubMed]
- Eggermont, A.M.M.; Spatz, A.; Robert, C. Cutaneous melanoma. Lancet 2014, 383, 816–827. [Google Scholar] [CrossRef] [PubMed]
- Kiani, B.; Tabari, P.; Mohammadi, A.; Mostafavi, S.M.; Moghadami, M.; Amini, M.; Rezaianzadeh, A. Spatial epidemiology of skin cancer in Iran: Separating sun-exposed and non-sun-exposed parts of the body. Arch. Public Health 2022, 80, 35. [Google Scholar] [CrossRef]
- Hieken, T.J.; Glasgow, A.E.; Enninga, E.A.L.; Kottschade, L.A.; Dronca, R.S.; Markovic, S.N.; Block, M.S.; Habermann, E.B. Sex-Based Differences in Melanoma Survival in a Contemporary Patient Cohort. J. Women’s Health 2020, 29, 1160–1167. [Google Scholar] [CrossRef]
- Behbahani, S.; Maddukuri, S.; Cadwell, J.B.; Lambert, W.C.; Schwartz, R.A. Gender differences in cutaneous melanoma: Demographics, prognostic factors, and survival outcomes. Dermatol. Ther. 2020, 33, e14131. [Google Scholar] [CrossRef]
- Salman, P.; de Melo, A.C.; Rico-Restrepo, M.; Rodriguez, J.; Russi, A.; Schmerling, R.A.; Zambrano, A.; Cinat, G. Addressing the unmet needs of patients with BRAF-mutated melanoma in Latin America: Expert perspective. Front. Oncol. 2023, 13, 1032300. [Google Scholar] [CrossRef]
- Possik, P.A. Obstacles and opportunities in studying melanoma in Latin America. Nat. Cancer 2023, 4, 777–778. [Google Scholar] [CrossRef]
- Bravo-Garzón, M.A.; Bornstein-Quevedo, L.; Camargo, V.P.D.; Sanku, G.; Jansen, A.M.; Macedo, M.P.D.; Rico-Restrepo, M.; Chacón, M. BRAF-Mutated Melanoma Journey in Latin America: Expert Recommendations From Diagnosis to Treatment. Cancer Control. 2024, 31, 10732748241251572. [Google Scholar] [CrossRef]
- Costello, C.M.; Pittelkow, M.R.; Mangold, A.R. Acral Melanoma and Mechanical Stress on the Plantar Surface of the Foot. N. Engl. J. Med. 2017, 377, 395–396. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, T.; Santos, I.D.D.A.O.; Oliveira, A.F.; Ferreira, L.M. Estudo retrospectivo dos pacientes portadores de melanoma cutâneo atendidos na Universidade Federal de São Paulo. Rev. Col. Bras. Cir. 2018, 5. [Google Scholar] [CrossRef] [PubMed]
- Boutros, A.; Carosio, R.; Campanella, D.; Banelli, B.; Morabito, A.; Pistillo, M.P.; Croce, E.; Queirolo, P.; Tanda, E.T.; Raposio, E.; et al. Association between PD-1 single nucleotide gene variants and the risk of metastatic melanoma. Arch. Dermatol. Res. 2024, 316, 414. [Google Scholar] [CrossRef] [PubMed]
- Rangel-Villalobos, H.; Rubi-Castellanos, R.; Morales-Vallejo, M.E.; Molina-Araujo, V.; Licea-Cadena, R.A.; Rizzo-Juarez, S.; Muniz-Lozano, F.E.; Nuno-Arana, I.; Munoz-Valle, J.F. Admixture estimates and statistical parameters of forensic importance based on PowerPlex 16 system in Mexican-Mestizos from the States of Guanajuato (Center) and Veracruz (East). Forensic. Sci. Int. Genet. 2010, 4, 271–272. [Google Scholar] [CrossRef]
- Martinez-Cortes, G.; Salazar-Flores, J.; Gabriela Fernández-Rodríguez, L.; Rubi-Castellanos, R.; Rodríguez-Loya, C.; Velarde-Félix, J.S.; Franciso Muñoz-Valle, J.; Parra-Rojas, I.; Rangel-Villalobos, H. Admixture and population structure in Mexican-Mestizos based on paternal lineages. J. Hum. Genet. 2012, 57, 568–574. [Google Scholar] [CrossRef]
- Mayer-Jochimsen, M.; Fast, S.; Tintle, N.L. Assessing the Impact of Differential Genotyping Errors on Rare Variant Tests of Association. PLoS ONE 2013, 8, e56626. [Google Scholar] [CrossRef]
- Zhao, S.; Ye, Z.; Stanton, R. Misuse of RPKM or TPM normalization when comparing across samples and sequencing protocols. RNA 2020, 26, 903–909. [Google Scholar] [CrossRef]
- Holzgruber, J.; Martins, C.; Kulcsar, Z.; Duplaine, A.; Rasbach, E.; Migayron, L.; Singh, P.; Statham, E.; Landsberg, J.; Boniface, K.; et al. Type I interferon signaling induces melanoma cell-intrinsic PD-1 and its inhibition antagonizes immune checkpoint blockade. Nat. Commun. 2024, 15, 7165. [Google Scholar] [CrossRef]
- Shirley, C.A.; Chhabra, G.; Amiri, D.; Chang, H.; Ahmad, N. Immune escape and metastasis mechanisms in melanoma: Breaking down the dichotomy. Front. Immunol. 2024, 10, 1336023. [Google Scholar] [CrossRef]
- Lin, X.; Kang, K.; Chen, P.; Zeng, Z.; Li, G.; Xiong, W.; Yi, M.; Xiang, B. Regulatory mechanisms of PD-1/PD-L1 in cancers. Mol. Cancer 2024, 23, 108. [Google Scholar] [CrossRef]
- Martins, C.; Silva, M.; Rasbach, E.; Singh, P.; Itoh, Y.; Williams, J.B.; Statham, E.; Meurer, A.; Martinez, D.V.; Brandenburg, A.; et al. Distinct antibody clones detect PD-1 checkpoint expression and block PD-L1 interactions on live murine melanoma cells. Sci. Rep. 2022, 12, 12491. [Google Scholar] [CrossRef]
- Jung, H.; Kim, H.S.; Kim, J.Y.; Sun, J.M.; Ahn, J.S.; Ahn, M.J.; Park, K.; Esteller, M.; Lee, S.H.; Choi, J.K. DNA methylation loss promotes immune evasion of tumours with high mutation and copy number load. Nat. Commun. 2019, 10, 4278. [Google Scholar] [CrossRef] [PubMed]
- Röver, L.K.; Gevensleben, H.; Dietrich, J.; Bootz, F.; Landsberg, J.; Goltz, D.; Dietrich, D. PD-1 (PDCD1) Promoter Methylation Is a Prognostic Factor in Patients with Diffuse Lower-Grade Gliomas Harboring Isocitrate Dehydrogenase (IDH) Mutations. EBioMedicine 2018, 28, 97–104. [Google Scholar] [CrossRef] [PubMed]
- Ricci, C.; Morandi, L.; Righi, A.; Gibertoni, D.; Maletta, F.; Ambrosi, F.; Agostinelli, C.; Uccella, S.; Asioli, S.; Sessa, F.; et al. PD-1 (PDCD1) promoter methylation in Merkel cell carcinoma: Prognostic relevance and relationship with clinico-pathological parameters. Mod. Pathol. 2019, 32, 1359–1372. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Du, Y.; Liu, X.; Gao, R.; Xu, X.; Hou, X.; Liu, Z.; Xin, P.; Wu, W.; Liu, T.; et al. Enhancing curcumol delivery through PD-1 targeted nanocarriers: A novel therapeutic approach for prostate cancer. Phytomedicine 2025, 141, 156595. [Google Scholar] [CrossRef]
- Juneja, V.R.; McGuire, K.A.; Manguso, R.T.; LaFleur, M.W.; Collins, N.; Haining, W.N.; Freeman, G.J.; Sharpe, A.H. PD-L1 on tumor cells is sufficient for immune evasion in immunogenic tumors and inhibits CD8 T cell cytotoxicity. J. Exp. Med. 2017, 214, 895–904. [Google Scholar] [CrossRef]
- Zielińska, M.K.; Ciążyńska, M.; Sulejczak, D.; Rutkowski, P.; Czarnecka, A.M. Mechanisms of Resistance to Anti-PD-1 Immunotherapy in Melanoma and Strategies to Overcome It. Biomolecules 2025, 15, 269. [Google Scholar] [CrossRef]
- Wu, B.; Zhang, B.; Li, B.; Wu, H.; Jiang, M. Cold and hot tumors: From molecular mechanisms to targeted therapy. Signal Transduct. Target. Ther. 2024, 9, 274. [Google Scholar] [CrossRef]
- Rico, M.L.P.; Soto-García, D.; Penabad, C.P.; Rojas, M.S.A.; Flórez, Á.; Suh-Oh, H.J.; Jorge, B.F.; Molina, F.P.; Silva, O.F.; García, C.P.; et al. Melanoma Detection Patterns and Their Association With Breslow Thickness: The Dermatologist’s Role. Actas Dermo-Sifiliogr. 2025; in press. [Google Scholar] [CrossRef] [PubMed]
- Melanoma Pathology N.D. Available online: https://dermnetnz.org/topics/melanoma-pathology (accessed on 3 June 2025).
- Dessinioti, C.; Befon, A.; Plaka, M.; Polydorou, D.; Kypreou, K.; Champsas, G.; Stratigos, A.J. Independent association of sex, age and the melanoma subtype with histological regression in invasive melanomas: A retrospective study. EJC Skin Cancer 2024, 2, 100020. [Google Scholar] [CrossRef]
- De Giorgi, V.; Scarfì, F.; Gori, A.; Maida, P.; Trane, L.; Silvestri, F.; Portelli, F.; Massi, D.; Covarelli, P.; Gandini, S. Nevi and Breslow thickness in melanoma: Sex differences? Melanoma Res. 2020, 30, 179–184. [Google Scholar] [CrossRef]
- Antohe, M.; Coman, A.; Turcu, G.; Nedelcu, R.I.; Brinzea, A.; Balaban, M.; Moroianu, A.; Manea, L.; Hulea, I.; Balasescu, E.; et al. The prognostic significance of the clinical and histological parameters in primary cutaneous melanoma patients. Med. Pharm. Rep. 2022, 95, 229–235. [Google Scholar] [CrossRef]
- Wang, M.; Banik, I.; Shain, A.H.; Yeh, I.; Bastian, B.C. Integrated genomic analyses of acral and mucosal melanomas nominate novel driver genes. Genome. Med. 2022, 14, 65. [Google Scholar] [CrossRef]
- Bobos, M. Histopathologic classification and prognostic factors of melanoma: A 2021 update. Ital. J. Dermatol. Venereol. 2021, 156, 300–321. [Google Scholar] [CrossRef]
- Yeh, I.; Jorgenson, E.; Shen, L.; Xu, M.; North, J.P.; Shain, A.H.; Reuss, D.; Wu, H.; Robinson, W.A.; Olshen, A.; et al. Targeted Genomic Profiling of Acral Melanoma. J. Natl. Cancer Inst. 2019, 111, 1068–1077. [Google Scholar] [CrossRef]
- Shi, Q.; Liu, L.; Chen, J.; Zhang, W.; Guo, W.; Wang, X.; Wang, H.; Guo, S.; Yue, Q.; Ma, J.; et al. Integrative Genomic Profiling Uncovers Therapeutic Targets of Acral Melanoma in Asian Populations. Clin. Cancer Res. 2022, 28, 2690–2703. [Google Scholar] [CrossRef]
- Lopes, R.; Agami, R.; Korkmaz, G. GRO-seq, A Tool for Identification of Transcripts Regulating Gene Expression. Methods Mol. Biol. 2017, 1543, 45–55. [Google Scholar] [CrossRef] [PubMed]
- Sorroche, B.P.; Teixeira, R.D.J.; Pereira, C.A.D.; Santana, I.V.V.; Vujanovic, L.; Vazquez, V.D.L.; Arantes, L.M.R.B. PD-L1 Tumor Expression as a Predictive Biomarker of Immune Checkpoint Inhibitors’ Response and Survival in Advanced Melanoma Patients Brazil. Diagnostics 2023, 13, 1041. [Google Scholar] [CrossRef] [PubMed]
- Auslander, N.; Zhang, G.; Lee, J.S.; Frederick, D.T.; Miao, B.; Moll, T.; Tian, T.; Wei, Z.; Madan, S.; Sullivan, R.J.; et al. Robust prediction of response to immune checkpoint blockade therapy in metastatic melanoma. Nat. Med. 2018, 24, 1545–1549. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Characteristic | Melanoma | Reference Group | p |
|---|---|---|---|
| n | 131 | 131 | |
| Age | 62 (51–73) | 64 (53–73) | 0.75 |
| Sex n (%) | 0.45 | ||
| Female | 76 (58) | 69 (52.7) | |
| Male | 55 (42) | 62 (47.3) | |
| Skin phototype | |||
| I | 9 | 0 | |
| II | 36 | 12 | |
| III | 40 | 70 | |
| IV | 42 | 42 | |
| V | 3 | 3 |
| Characteristic | Level | Female n (%) | Male n (%) | Total n (%) | p |
|---|---|---|---|---|---|
| Anatomical location | Head/neck | 16 (22.2) | 17 (32.7) | 33 (25.2) | 0.14 |
| Trunk | 13 (18.1) | 14 (26.9) | 27 (20.6) | ||
| Upper limbs | 15 (20.8) | 10 (19.2) | 25 (19.1) | ||
| Lower limbs | 28 (38.9) | 11 (21.2) | 39 (29.8) | ||
| Histological subtype | Superficial spreading | 30 (44.1) | 19 (39.6) | 49 (37.4) | 0.90 |
| Nodular | 12 (17.6) | 10 (20.8) | 22 (16.8) | ||
| Acral lentiginous | 13 (19.1) | 8 (16.7) | 21 (16.0) | ||
| Lentigo maligna | 13 (19.1) | 11 (22.9) | 24 (18.3) | ||
| Breslow thickness | <1 mm | 19 (35.8) | 10 (24.4) | 29 (22.1) | 0.35 |
| 1.1–2 mm | 7 (13.2) | 11 (26.8) | 18 (13.7) | ||
| 2.1–4 mm | 12 (22.6) | 9 (22.0) | 21 (16.0) | ||
| >4 mm | 15 (28.3) | 11 (26.8) | 26 (19.8) | ||
| Clark level | I | 4 (9.3) | 6 (15.4) | 10 (7.6) | 0.77 |
| II | 10 (23.3) | 12 (30.8) | 22 (16.8) | ||
| III | 15 (34.9) | 11 (28.2) | 26 (19.8) | ||
| IV | 12 (27.9) | 8 (20.5) | 20 (15.3) | ||
| V | 2 (4.7) | 2 (5.1) | 4 (3.1) |
| Melanoma n = 131 (%) | Reference Group n = 131 (%) | OR (CI 95%) | p | |
|---|---|---|---|---|
| rs2227982 G>A | ||||
| Alleles | ||||
| G * | 210 (80.1) | 204 (77.8) | 1 | - |
| A | 52 (19.8) | 58 (22.1) | 0.87 (0.57–1.32) | 0.51 |
| Genotypes | ||||
| G/G * | 84 (64.1) | 82 (62.5) | 1 | - |
| G/A | 42 (32) | 40 (30.5) | 1.02 (0.60–1.74) | 0.92 |
| A/A | 5 (3.9) | 9 (7) | 0.54 (0.17–1.68) | 0.29 |
| HWE | 0.42 | |||
| rs36084323 C>T | ||||
| Alleles | ||||
| C * | 211 (80.5) | 201 (76.7) | 1 | - |
| T | 51 (19.4) | 61 (23.2) | 0.79 (0.52–1.21) | 0.28 |
| Genotypes | ||||
| C/C * | 86 (65.6) | 79 (60.3) | 1 | - |
| C/T | 39 (29.7) | 43 (32.8) | 0.83 (0.49–1.31) | 0.49 |
| T/T | 6 (4.7) | 9 (6.9) | 0.61 (0.20–1.79) | 0.37 |
| HWE | 0.64 | |||
| rs7421861 A>G | ||||
| Alleles | ||||
| A * | 67 (25.5) | 60 (22.9) | 1 | - |
| G | 195 (74.4) | 202 (77.1) | 1.15 (0.77–1.72) | 0.47 |
| Genotypes | ||||
| A/A * | 12 (9.1) | 8 (6.1) | 1 | - |
| A/G | 43 (32.8) | 44 (33.5) | 0.65 (0.24–1.75) | 0.39 |
| G/G | 76 (58.1) | 79 (60.4) | 0.64 (0.24–1.65) | 0.35 |
| HWE | 0.85 | |||
| Haplotype | Melanoma | Reference Group | OR (CI 95%) | p |
|---|---|---|---|---|
| GCA * | 145 (0.553) | 144 (0.549) | 1 | - |
| GCG | 62 (0.236) | 57 (0.217) | 1.08 (0.70–1.65) | 0.72 |
| ATA | 47 (0.179) | 58 (0.221) | 0.80 (0.51–1.26) | 0.34 |
| Breslow Thickness | Superficial Spreading | Nodular | Acral Lentiginous | Lentigo Maligna | p |
|---|---|---|---|---|---|
| <1 mm | 16 | 1 | 4 | 8 | <0.01 |
| 1.1 mm–2 mm | 15 | 0 | 2 | 0 | |
| 2.1 mm–4 mm | 6 | 7 | 5 | 3 | |
| >4 mm | 8 | 13 | 5 | 0 |
| Anatomical Location | Superficial Spreading | Nodular | Acral Lentiginous | Lentigo Maligna | p |
|---|---|---|---|---|---|
| Head/Neck | 10 | 4 | 0 | 17 | <0.01 |
| Trunk | 14 | 7 | 0 | 3 | |
| Upper limbs | 12 | 5 | 5 | 1 | |
| Lower limbs | 13 | 5 | 14 | 3 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Valdez-Salazar, F.; Jiménez-Del Rio, L.A.; Guevara-Gutiérrez, E.; Mendoza-Ochoa, A.M.; Zorrilla-Marina, M.J.; García-Nuño, D.K.; Padilla-Gutiérrez, J.R.; Muñoz-Valle, J.F.; Valdés-Alvarado, E. Association Study of PDCD1 Gene Variants and Its Gene Expression with Cutaneous Melanoma in a Mexican Population. Genes 2025, 16, 866. https://doi.org/10.3390/genes16080866
Valdez-Salazar F, Jiménez-Del Rio LA, Guevara-Gutiérrez E, Mendoza-Ochoa AM, Zorrilla-Marina MJ, García-Nuño DK, Padilla-Gutiérrez JR, Muñoz-Valle JF, Valdés-Alvarado E. Association Study of PDCD1 Gene Variants and Its Gene Expression with Cutaneous Melanoma in a Mexican Population. Genes. 2025; 16(8):866. https://doi.org/10.3390/genes16080866
Chicago/Turabian StyleValdez-Salazar, Fernando, Luis A. Jiménez-Del Rio, Elizabeth Guevara-Gutiérrez, Andrea Melissa Mendoza-Ochoa, María José Zorrilla-Marina, Diana Karla García-Nuño, Jorge R. Padilla-Gutiérrez, José F. Muñoz-Valle, and Emmanuel Valdés-Alvarado. 2025. "Association Study of PDCD1 Gene Variants and Its Gene Expression with Cutaneous Melanoma in a Mexican Population" Genes 16, no. 8: 866. https://doi.org/10.3390/genes16080866
APA StyleValdez-Salazar, F., Jiménez-Del Rio, L. A., Guevara-Gutiérrez, E., Mendoza-Ochoa, A. M., Zorrilla-Marina, M. J., García-Nuño, D. K., Padilla-Gutiérrez, J. R., Muñoz-Valle, J. F., & Valdés-Alvarado, E. (2025). Association Study of PDCD1 Gene Variants and Its Gene Expression with Cutaneous Melanoma in a Mexican Population. Genes, 16(8), 866. https://doi.org/10.3390/genes16080866