
A Modified FLT3 PCR Assay Using a TapeStation Readout


Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Outline of the Validation Strategy
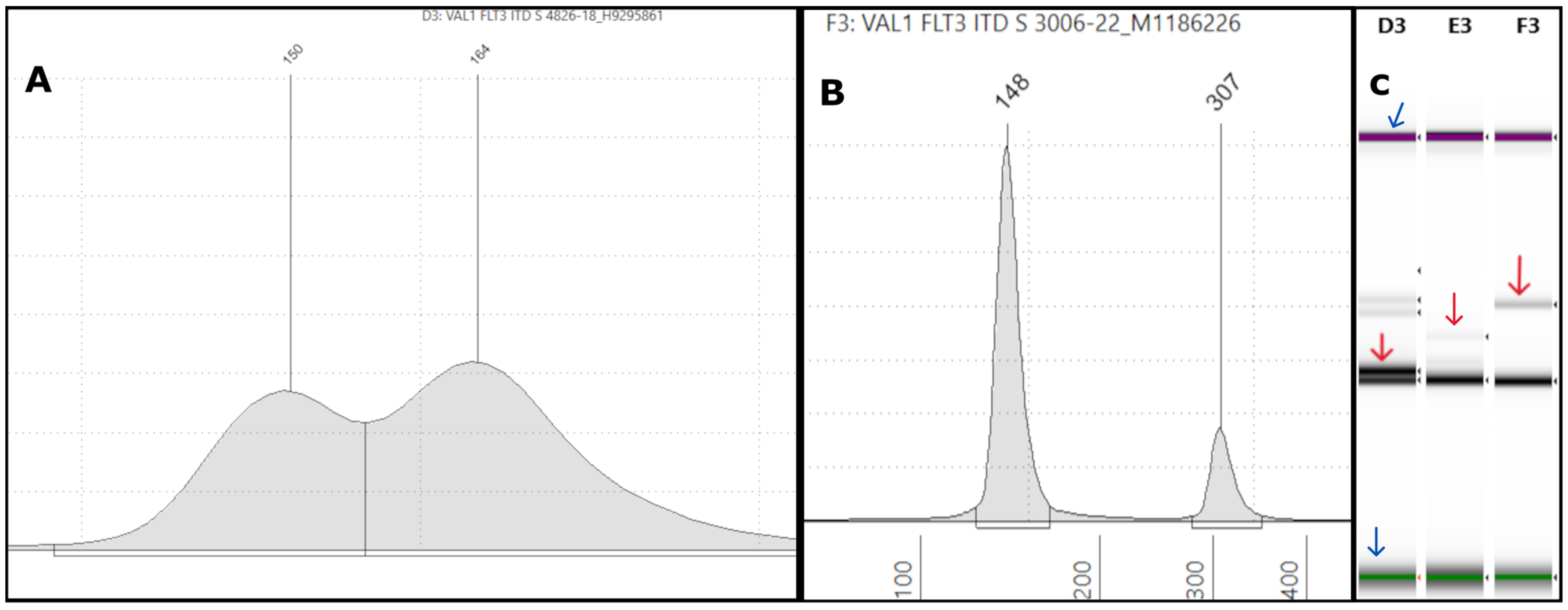
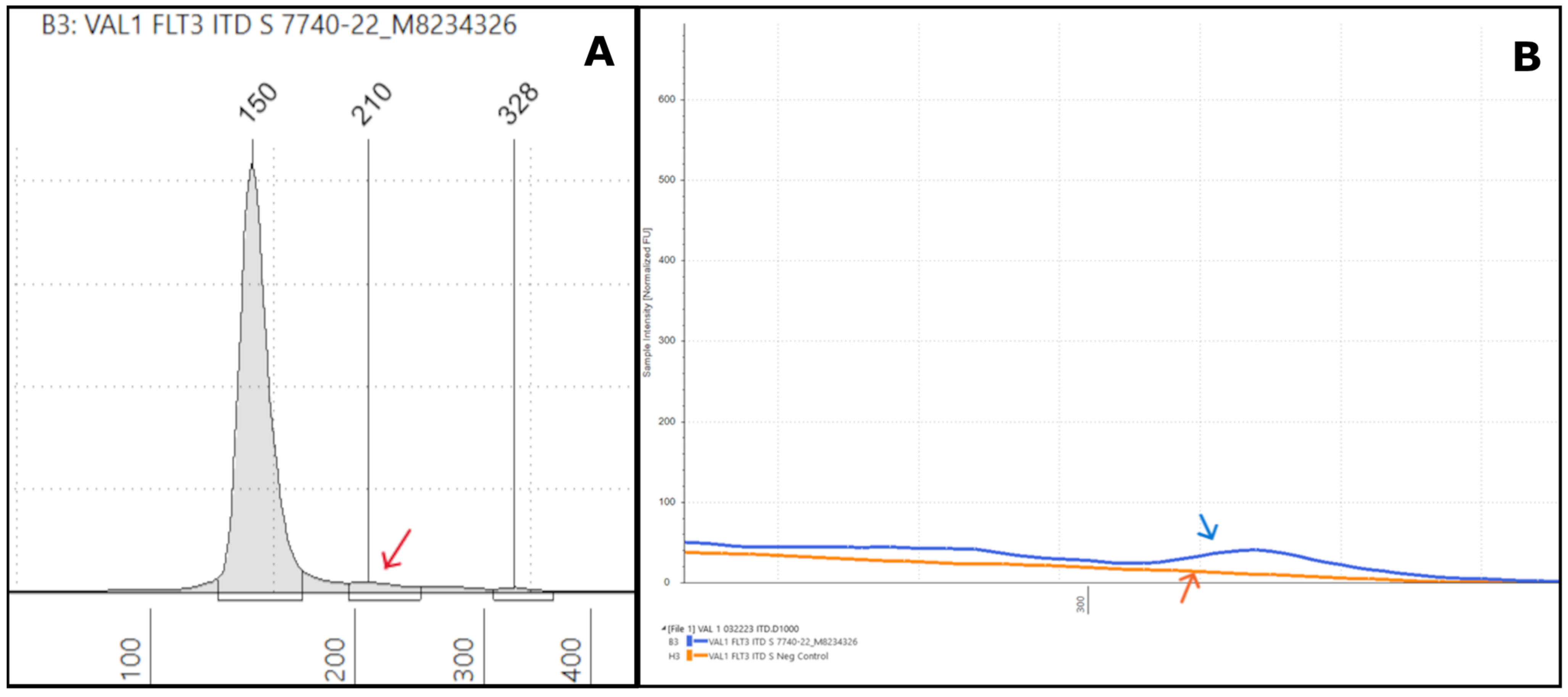
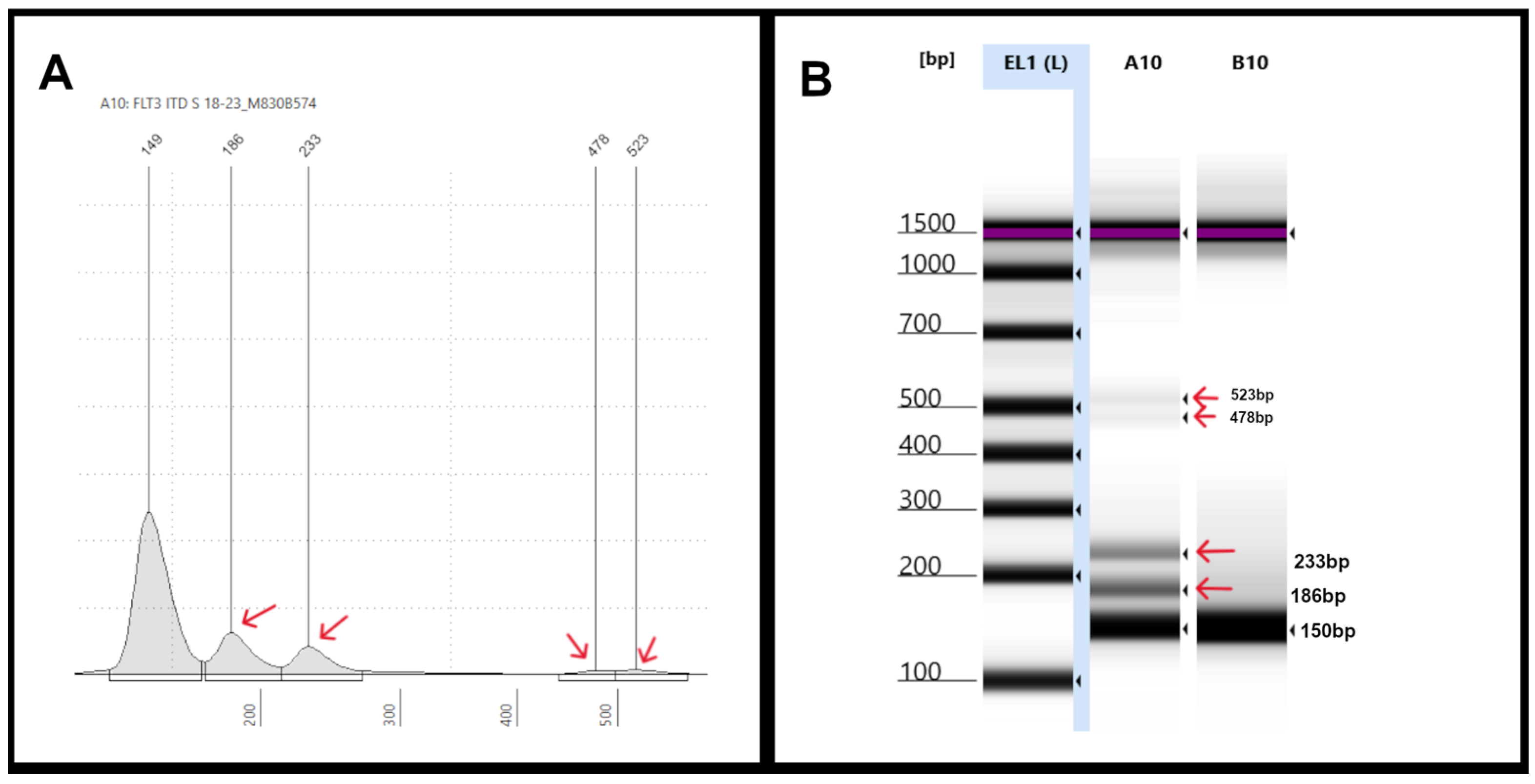
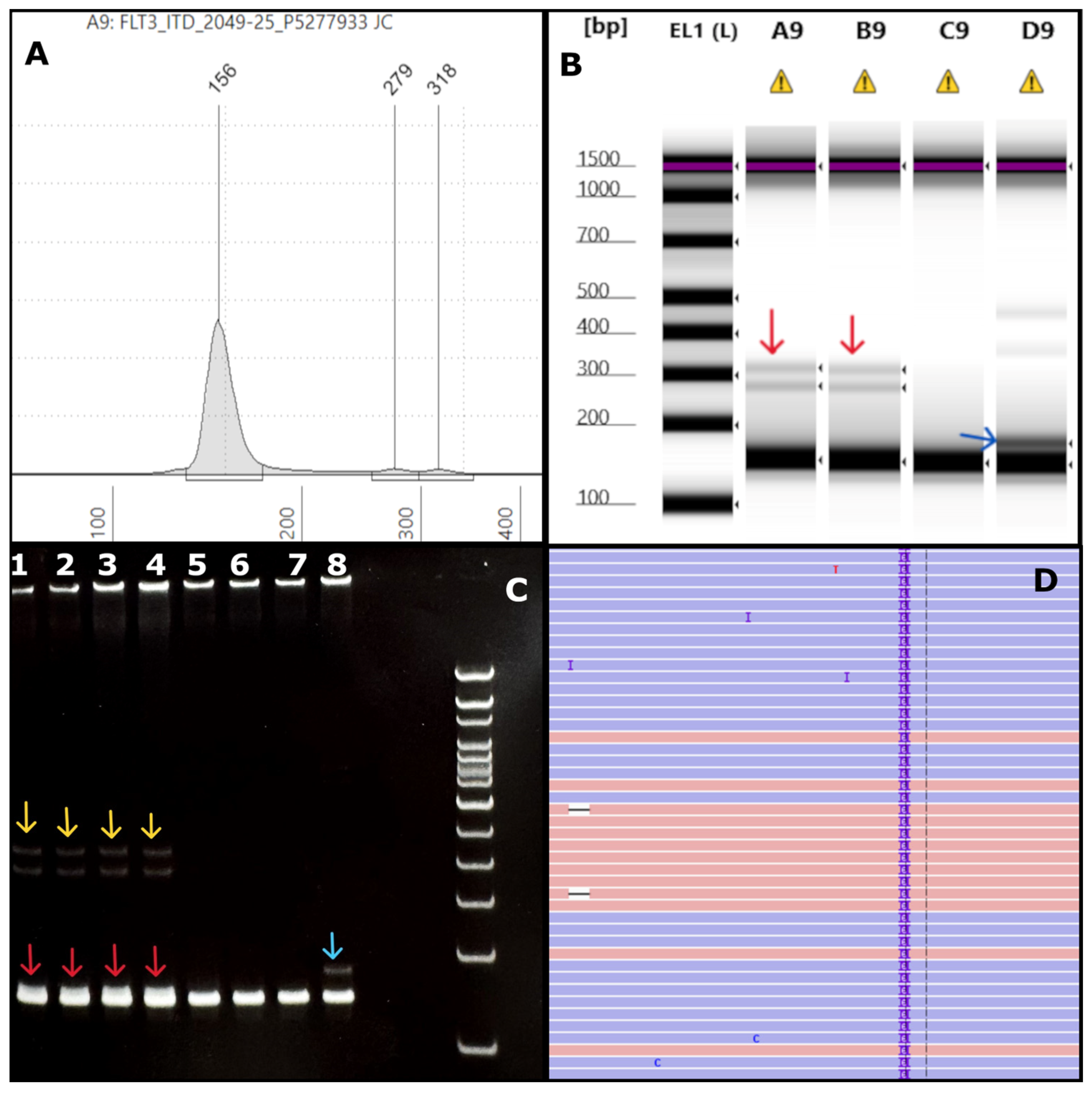
3.2. Validation of the FLT3-ITD Assay with TapeStation Readout
3.3. Validation of the FLT3-TKD Assay with TapeStation Readout
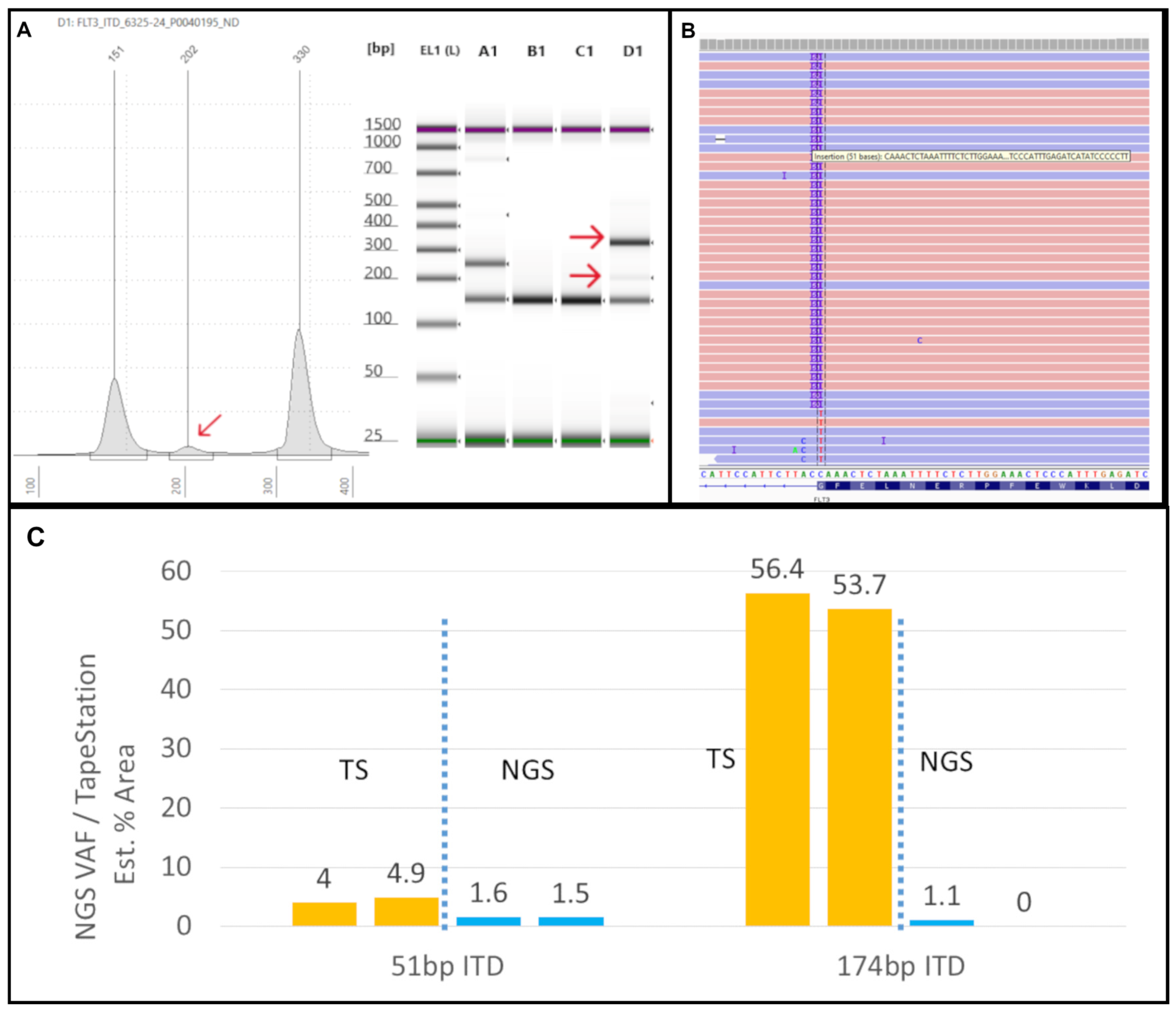
3.4. Limitations of the Modified FLT3 Assay in Detecting Very Small FLT3-ITDs
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AML | Acute myeloid leukemia |
| ITD(s) | Internal tandem duplication(s) |
| JMD | Juxtamembrane domain |
| TKD | Tyrosine kinase domain |
| PCR | Polymerase chain reaction |
| CE | Capillary electrophoresis |
| wt | Wild type |
| PAGE | Polyacrylamide gel electrophoresis |
| NGS | Next-generation sequencing |
| bp | Base pairs |
| NTC | No template control |
| VAF | Variant allele frequency |
| EPG | Electropherogram |
| VSI(s) | Very short insert(s) |
References
- Fedorov, K.; Maiti, A.; Konopleva, M. Targeting FLT3 Mutation in Acute Myeloid Leukemia: Current Strategies and Future Directions. Cancers 2023, 15, 2312. [Google Scholar] [CrossRef] [PubMed]
- Grafone, T.; Palmisano, M.; Nicci, C.; Storti, S. An overview on the role of FLT3-tyrosine kinase receptor in acute myeloid leukemia: Biology and treatment. Oncol. Rev. 2012, 6, e8. [Google Scholar] [CrossRef]
- National Center for Biotechnology Information (NCBI). Gene ID: 2322, FLT3 fms Related Receptor Tyrosine Kinase 3 [Homo sapiens (Human)]–Gene. Available online: https://www.ncbi.nlm.nih.gov/gene/2322 (accessed on 20 May 2025).
- Spiekermann, K.; Bagrintseva, K.; Schwab, R.; Schmieja, K.; Hiddemann, W. Overexpression and constitutive activation of FLT3 induces STAT5 activation in primary acute myeloid leukemia blast cells. Clin. Cancer Res. 2003, 9, 2140–2150. [Google Scholar] [PubMed]
- Moore, M.A.; Dorn, D.C.; Schuringa, J.J.; Chung, K.Y.; Morrone, G. Constitutive activation of Flt3 and STAT5A enhances self-renewal and alters differentiation of hematopoietic stem cells. Exp. Hematol. 2007, 35, 105–116. [Google Scholar] [CrossRef]
- Thiede, C.; Steudel, C.; Mohr, B.; Schaich, M.; Schäkel, U.; Platzbecker, U.; Wermke, M.; Bornhäuser, M.; Ritter, M.; Neubauer, A.; et al. Analysis of FLT3-activating mutations in 979 patients with acute myelogenous leukemia: Association with FAB subtypes and identification of subgroups with poor prognosis. Blood 2002, 99, 4326–4335. [Google Scholar] [CrossRef]
- Bergeron, J.; Capo-Chichi, J.-M.; Tsui, H.; Mahe, E.; Berardi, P.; Minden, M.D.; Brandwein, J.M.; Schuh, A.C. The Clinical Utility of FLT3 Mutation Testing in Acute Leukemia: A Canadian Consensus. Curr. Oncol. 2023, 30, 10410–10436. [Google Scholar] [CrossRef] [PubMed]
- Shimony, S.; Stahl, M.; Stone, R.M. Acute Myeloid Leukemia: 2025 Update on Diagnosis, Risk-Stratification, and Management. Am. J. Hematol. 2025, 100, 860–891. [Google Scholar] [CrossRef]
- Stone, R.M.; Mandrekar, S.J.; Sanford, B.L.; Laumann, K.; Geyer, S.; Bloomfield, C.D.; Thiede, C.; Prior, T.W.; Döhner, K.; Marcucci, G.; et al. Midostaurin plus Chemotherapy for Acute Myeloid Leukemia with a FLT3 Mutation. N. Engl. J. Med. 2017, 377, 454–464. [Google Scholar] [CrossRef]
- Daver, N.; Schlenk, R.F.; Russell, N.H.; Levis, M.J. Targeting FLT3 mutations in AML: Review of current knowledge and evidence. Leukemia 2019, 33, 299–312. [Google Scholar] [CrossRef]
- O’Donnell, M.R.; Tallman, M.S.; Abboud, C.N.; Altman, J.K.; Appelbaum, F.R.; Arber, D.A.; Bhatt, V.; Bixby, D.; Blum, W.; Coutre, S.E.; et al. Acute Myeloid Leukemia, Version 3.2017, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2017, 15, 926–957. [Google Scholar] [CrossRef]
- Döhner, H.; Wei, A.H.; Appelbaum, F.R.; Craddock, C.; DiNardo, C.D.; Dombret, H.; Ebert, B.L.; Fenaux, P.; Godley, L.A.; Hasserjian, R.P.; et al. Diagnosis and management of AML in adults: 2022 recommendations from an international expert panel on behalf of the ELN. Blood 2022, 140, 1345–1377. [Google Scholar] [CrossRef] [PubMed]
- Murphy, K.M.; Levis, M.; Hafez, M.J.; Geiger, T.; Cooper, L.C.; Smith, B.D.; Small, D.; Berg, K.D. Detection of FLT3 internal tandem duplication and D835 mutations by a multiplex polymerase chain reaction and capillary electrophoresis assay. J. Mol. Diagn. 2003, 5, 96–102. [Google Scholar] [CrossRef]
- Kim, Y.; Lee, G.D.; Park, J.; Yoon, J.H.; Kim, H.J.; Min, W.S.; Kim, M. Quantitative fragment analysis of FLT3-ITD efficiently identifying poor prognostic group with high mutant allele burden or long ITD length. Blood Cancer J. 2015, 5, e336. [Google Scholar] [CrossRef] [PubMed]
- Sakaguchi, M.; Nakajima, N.; Yamaguchi, H.; Najima, Y.; Shono, K.; Marumo, A.; Omori, I.; Fujiwara, Y.; Terada, K.; Yui, S.; et al. The sensitivity of the FLT3-ITD detection method is an important consideration when diagnosing acute myeloid leukemia. Leuk. Res. Rep. 2020, 13, 100198. [Google Scholar] [CrossRef]
- Meshinchi, S.; Woods, W.G.; Stirewalt, D.L.; Sweetser, D.A.; Buckley, J.D.; Tjoa, T.K.; Bernstein, I.D.; Radich, J.P. Prevalence and prognostic significance of Flt3 internal tandem duplication in pediatric acute myeloid leukemia. Blood 2001, 97, 89–94. [Google Scholar] [CrossRef]
- Nakao, M.; Yokota, S.; Iwai, T.; Kaneko, H.; Horiike, S.; Kashima, K.; Sonoda, Y.; Fujimoto, T.; Misawa, S. Internal tandem duplication of the flt3 gene found in acute myeloid leukemia. Leukemia 1996, 10, 1911–1918. [Google Scholar] [PubMed]
- Abu-Duhier, F.M.; Goodeve, A.C.; Wilson, G.A.; Care, R.S.; Peake, I.R.; Reilly, J.T. Genomic structure of human FLT3: Implications for mutational analysis. Br. J. Haematol. 2001, 113, 1076–1077. [Google Scholar] [CrossRef]
- Abu-Duhier, F.M.; Goodeve, A.C.; Wilson, G.A.; Care, R.S.; Peake, I.R.; Reilly, J.T. Identification of novel FLT-3 Asp835 mutations in adult acute myeloid leukaemia. Br. J. Haematol. 2001, 113, 983–988. [Google Scholar] [CrossRef]
- Koga, S.; Du, W.; Yang, G.; Zhang, L. Molecular Testing of FLT3 Mutations in Hematolymphoid Malignancies in the Era of Next-generation Sequencing. J. Clin. Transl. Pathol. 2025, 5, 30–40. [Google Scholar] [CrossRef]
- Spencer, D.H.; Abel, H.J.; Lockwood, C.M.; Payton, J.E.; Szankasi, P.; Kelley, T.W.; Kulkarni, S.; Pfeifer, J.D.; Duncavage, E.J. Detection of FLT3 internal tandem duplication in targeted, short-read-length, next-generation sequencing data. J. Mol. Diagn. 2013, 15, 81–93. [Google Scholar] [CrossRef]
- Noguera, N.I.; Ammatuna, E.; Zangrilli, D.; Lavorgna, S.; Divona, M.; Buccisano, F.; Amadori, S.; Mecucci, C.; Falini, B.; Lo-Coco, F. Simultaneous detection of NPM1 and FLT3-ITD mutations by capillary electrophoresis in acute myeloid leukemia. Leukemia 2005, 19, 1479–1482. [Google Scholar] [CrossRef] [PubMed]
- Yuan, D.; He, X.; Han, X.; Yang, C.; Liu, F.; Zhang, S.; Luan, H.; Li, R.; He, J.; Duan, X.; et al. Comprehensive review and evaluation of computational methods for identifying FLT3-internal tandem duplication in acute myeloid leukaemia. Brief. Bioinform. 2021, 22, bbab099. [Google Scholar] [CrossRef] [PubMed]
- Tung, J.K.; Suarez, C.J.; Chiang, T.; Zehnder, J.L.; Stehr, H. Accurate Detection and Quantification of FLT3 Internal Tandem Duplications in Clinical Hybrid Capture Next-Generation Sequencing Data. J. Mol. Diagn. 2021, 23, 1404–1413. [Google Scholar] [CrossRef] [PubMed]
- Tsai, H.K.; Brackett, D.G.; Szeto, D.; Frazier, R.; MacLeay, A.; Davineni, P.; Manning, D.K.; Garcia, E.; Lindeman, N.I.; Le, L.P.; et al. Targeted Informatics for Optimal Detection, Characterization, and Quantification of FLT3 Internal Tandem Duplications Across Multiple Next-Generation Sequencing Platforms. J. Mol. Diagn. 2020, 22, 1162–1178. [Google Scholar] [CrossRef]
- Ven, S.; Rani, A. Discriminatory Power of Agarose Gel Electrophoresis in DNA Fragments Analysis. In Gel Electrophoresis: Principles and Basics; InTech: Rijeka, Croatia, 2012. [Google Scholar]
- Greenough, L.; Schermerhorn, K.M.; Mazzola, L.; Bybee, J.; Rivizzigno, D.; Cantin, E.; Slatko, B.E.; Gardner, A.F. Adapting capillary gel electrophoresis as a sensitive, high-throughput method to accelerate characterization of nucleic acid metabolic enzymes. Nucleic Acids Res. 2016, 44, e15. [Google Scholar] [CrossRef]
- Karger, B.L.; Guttman, A. DNA sequencing by CE. Electrophoresis 2009, 30 (Suppl. S1), S196–S202. [Google Scholar] [CrossRef]
- Mitchelson, K.R. The application of capillary electrophoresis for DNA polymorphism analysis. Methods Mol. Biol. 2001, 162, 3–26. [Google Scholar] [CrossRef]
- Levis, M.; Small, D. FLT3: ITDoes matter in leukemia. Leukemia 2003, 17, 1738–1752. [Google Scholar] [CrossRef]
- Kim, J.J.; Lee, K.S.; Lee, T.G.; Lee, S.; Shin, S.; Lee, S.-T. A comparative study of next-generation sequencing and fragment analysis for the detection and allelic ratio determination of FLT3 internal tandem duplication. Diagn. Pathol. 2022, 17, 14. [Google Scholar] [CrossRef]
- Bacher, U.; Haferlach, C.; Kern, W.; Haferlach, T.; Schnittger, S. Prognostic relevance of FLT3-TKD mutations in AML: The combination matters—An analysis of 3082 patients. Blood 2008, 111, 2527–2537. [Google Scholar] [CrossRef]
- Yamamoto, Y.; Kiyoi, H.; Nakano, Y.; Suzuki, R.; Kodera, Y.; Miyawaki, S.; Asou, N.; Kuriyama, K.; Yagasaki, F.; Shimazaki, C.; et al. Activating mutation of D835 within the activation loop of FLT3 in human hematologic malignancies. Blood 2001, 97, 2434–2439. [Google Scholar] [CrossRef] [PubMed]
- Mehta, A.; Nathany, S.; Chopra, A.; Mattoo, S.; Kumar, D.; Panigrahi, M.K. Robust home brew fragment sizing assay for detection of MET exon 14 skipping mutation in non-small cell lung cancer patients in resource constrained community hospitals. J. Pathol. Transl. Med. 2021, 55, 324–329. [Google Scholar] [CrossRef] [PubMed]
- Rücker, F.G.; Du, L.; Luck, T.J.; Benner, A.; Krzykalla, J.; Gathmann, I.; Voso, M.T.; Amadori, S.; Prior, T.W.; Brandwein, J.M.; et al. Molecular landscape and prognostic impact of FLT3-ITD insertion site in acute myeloid leukemia: RATIFY study results. Leukemia 2022, 36, 90–99. [Google Scholar] [CrossRef]
- Bagrintseva, K.; Geisenhof, S.; Kern, R.; Eichenlaub, S.; Reindl, C.; Ellwart, J.W.; Hiddemann, W.; Spiekermann, K. FLT3-ITD-TKD dual mutants associated with AML confer resistance to FLT3 PTK inhibitors and cytotoxic agents by overexpression of Bcl-x(L). Blood 2005, 105, 3679–3685. [Google Scholar] [CrossRef] [PubMed]
- Tamburini, J.; Mouche, S.; Larrue, C.; Duployez, N.; Bidet, A.; Salotti, A.; Hirsch, P.; Rigolot, L.; Carras, S.; Templé, M.; et al. Very short insertions in the FLT3 gene are of therapeutic significance in acute myeloid leukemia. Blood Adv. 2023, 7, 7576–7580. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Primer Name | Primer Sequence | Position on Sequence in Accession AL445262.7 |
|---|---|---|
| FLT3-11F | GCAATTTAGGTATGAAAGCCAGC | 17,469–17,447 |
| FLT3-11R | CCAAACTCTAAATTTTCTCTTGGAAAC | 17,335–17,361 |
| FLT3-AF | GCTTGTCACCCACGGGAAAG | 1811–1792 |
| FLT3-AD | AGTGAGTGCAGTTGTTTACCATGATATC | 1642–1669 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Blake, E.A.; Ramineni, M.; Oltvai, Z.N. A Modified FLT3 PCR Assay Using a TapeStation Readout. Genes 2025, 16, 684. https://doi.org/10.3390/genes16060684
Blake EA, Ramineni M, Oltvai ZN. A Modified FLT3 PCR Assay Using a TapeStation Readout. Genes. 2025; 16(6):684. https://doi.org/10.3390/genes16060684
Chicago/Turabian StyleBlake, Elizabeth Adele, Madhurya Ramineni, and Zoltán N. Oltvai. 2025. "A Modified FLT3 PCR Assay Using a TapeStation Readout" Genes 16, no. 6: 684. https://doi.org/10.3390/genes16060684
APA StyleBlake, E. A., Ramineni, M., & Oltvai, Z. N. (2025). A Modified FLT3 PCR Assay Using a TapeStation Readout. Genes, 16(6), 684. https://doi.org/10.3390/genes16060684