

CCNE1 Gene Amplification Might Be Associated with Lymph Node Metastasis of Gastric Cancer

Abstract
1. Introduction
2. Materials and Methods
2.1. MGPT Data from C-CAT
2.2. Extraction of Genetic Abnormalities
2.3. GC Tissue Specimens
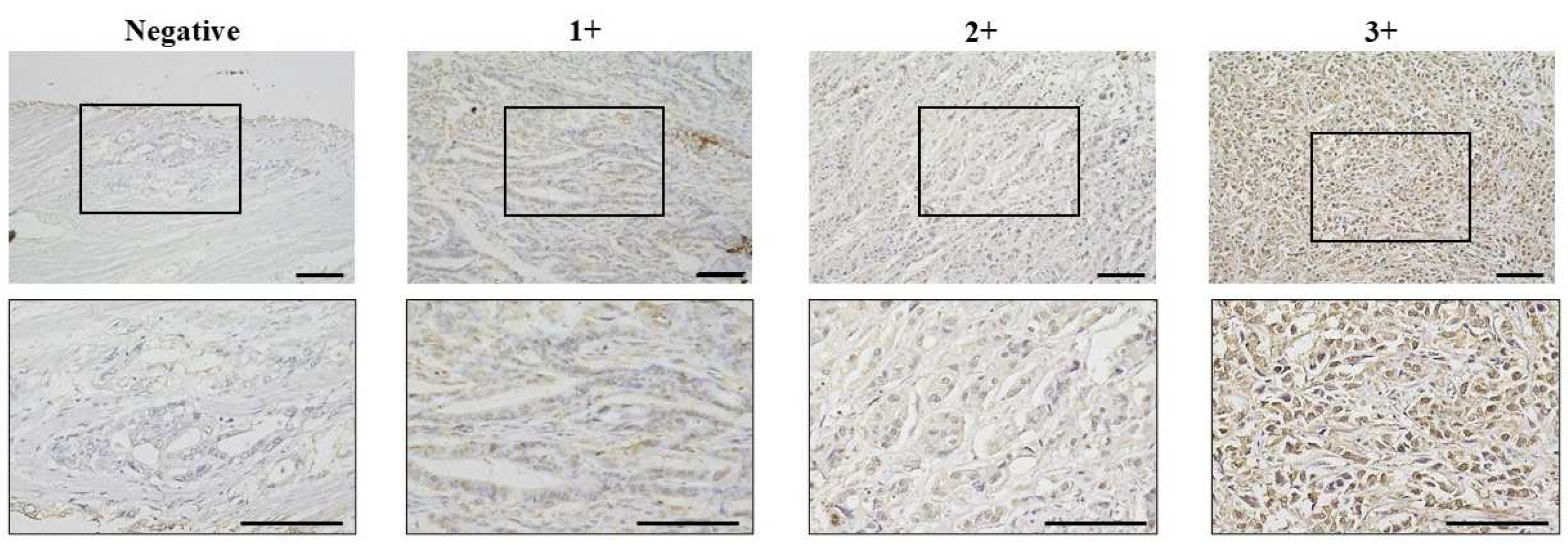
2.4. Immunostaining of CCNE1
2.5. Statistical Analysis
3. Results
3.1. Metastatic Lesions and Gene Amplification in 2028 GC Patients from the C-CAT Database
3.2. Correlation Between CCNE1 Expression and Clinicopathologic Features in 360 Patients with GC
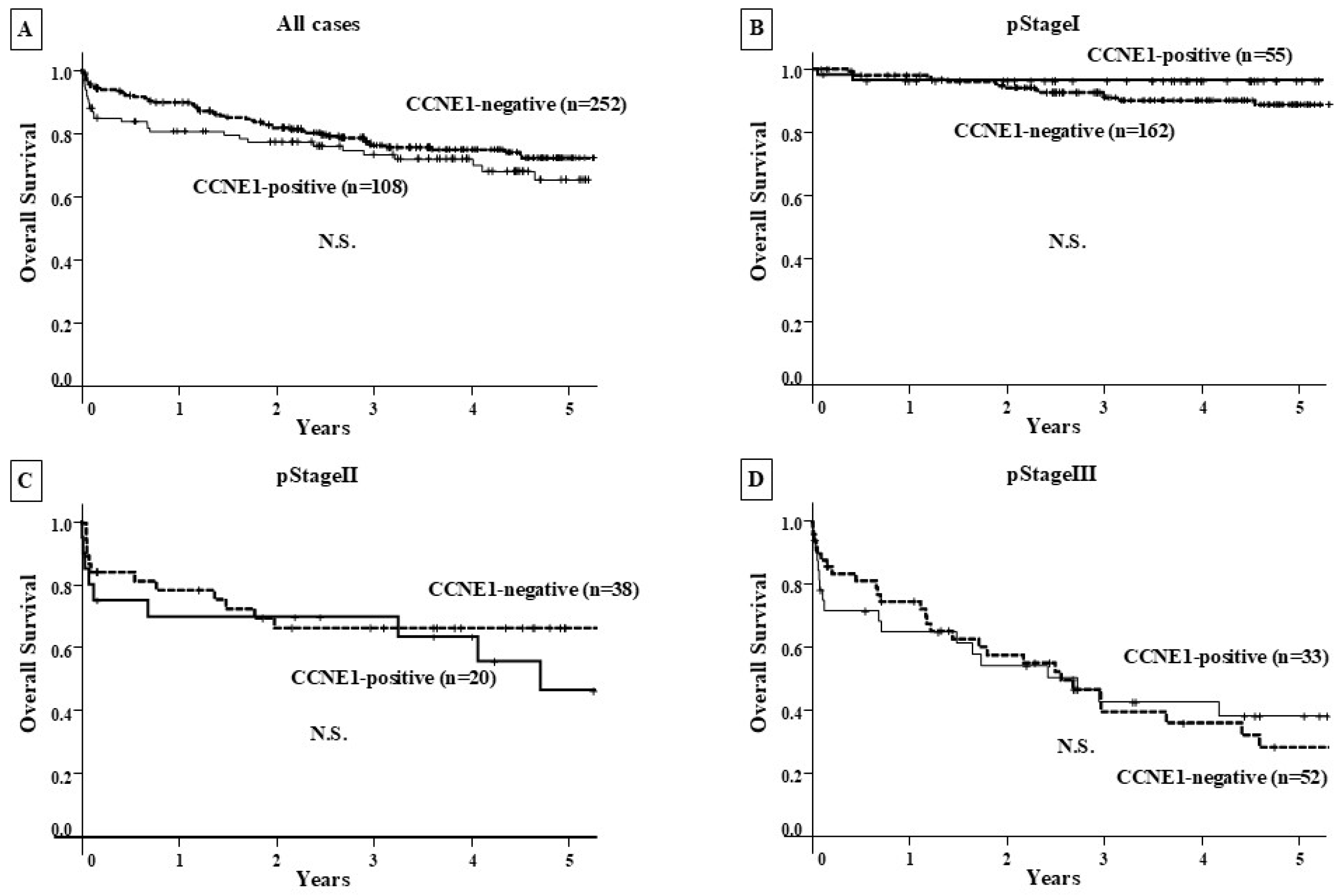
3.3. Correlation Between CCNE1 Expression and Patient Survival
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Siegel, R.L.; Giaquinto, A.N.; Jemal, A. Cancer statistics, 2024. CA Cancer J. Clin. 2024, 74, 12–49. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Ding, G.; Chu, C.; Cheng, X.D.; Qin, J.J. Genomic biology and therapeutic strategies of liver metastasis from gastric cancer. Crit. Rev. Oncol. 2024, 202, 104470. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.-Y.; Deng, J.-Y.; Zhang, N.-N.; Liu, H.-F.; Sun, W.-L.; He, W.-T.; Wang, Y.; Zhang, L.; Liang, H. Clinical significance of skip lymph-node metastasis in pN1 gastric-cancer patients after curative surgery. Gastroenterol. Rep. 2019, 7, 193–198. [Google Scholar] [CrossRef] [PubMed]
- Yordanagil, M.; Ercan, M.; Senturk, A.; Elcin, B. Prognostic significance of common hepatic artery lymph node metastasis in gastric cancer. Langenbeck’s Arch. Surg. 2023, 408, 247. [Google Scholar] [CrossRef] [PubMed]
- Kohno, T.; Kato, M.; Kohsaka, S.; Sudo, T.; Tamai, I.; Shiraishi, Y.; Okuma, Y.; Ogasawara, D.; Suzuki, T.; Yoshida, T.; et al. C-CAT: The National Datacenter for Cancer Genomic Medicine in Japan. Cancer Discov. 2022, 12, 2509–2515. [Google Scholar] [CrossRef] [PubMed]
- Mukai, Y.; Ueno, H. Establishment and implementation of Cancer Genomic Medicine in Japan. Cancer Sci. 2021, 112, 970–977. [Google Scholar] [CrossRef] [PubMed]
- Kouraklis, G.; Katsoulis, I.E.; Theocharis, S.; Tsourouflis, G.; Xipolitas, N.; Glinavou, A.; Sioka, C.; Kostakis, A. Does the expression of cyclin E, pRb, and p21 correlate with prognosis in gastric adenocarcinoma? Dig. Dis. Sci. 2009, 54, 1015–1020. [Google Scholar] [CrossRef] [PubMed]
- Hwang, H.C.; Clurman, B.E. Cyclin E in normal and neoplastic cell cycles. Oncogene 2005, 24, 2776–2786. [Google Scholar] [CrossRef] [PubMed]
- Caldon, C.E.; Sergio, C.M.; Sutherland, R.L.; Musgrove, E.A. Differences in degradation lead to asynchronous expression of cyclin E1 and cyclin E2 in cancer cells. Cell Cycle 2013, 12, 596–605. [Google Scholar] [CrossRef] [PubMed]
- Sano, T.; Aiko, T. New Japanese classifications and treatment guidelines for gastric cancer: Revision concepts and major revised points. Gastric Cancer 2011, 14, 97–100. [Google Scholar] [CrossRef] [PubMed]
- Sobin, L.H. TNM Classification of Malignant Tumours, Uicc International Union Against Cancer, 7th ed.; Wiley–Blackwell: Hoboken, NJ, USA, 2009; Volume 256. [Google Scholar]
- Matsuoka, T.; Yashiro, M. Molecular Insight into Gastric Cancer Invasion—Current Status and Future Directions. Cancers 2024, 16, 54. [Google Scholar] [CrossRef] [PubMed]
- Kim, B.; Shin, H.C.; Heo, Y.J.; Ha, S.Y.; Jang, K.-T.; Kim, S.T.; Kang, W.K.; Lee, J.; Kim, K.-M. CCNE1 amplification is associated with liver metastasis in gastric carcinoma. Pathol. Res. Pract. 2019, 215, 152434. Available online: https://www.sciencedirect.com/science/article/pii/S0344033819302511 (accessed on 17 May 2025). [CrossRef] [PubMed]
- Martínez-Gregorio, H.; Rojas-Jiménez, E.; Mejía-Gómez, J.C.; Díaz-Velásquez, C.; Quezada-Urban, R.; Vallejo-Lecuona, F.; de la Cruz-Montoya, A.; Porras-Reyes, F.I.; Pérez-Sánchez, V.M.; Maldonado-Martínez, H.A.; et al. The evolution of clinically aggressive triple-negative breast cancer shows a large mutational diversity and early metastasis to lymph nodes. Cancers 2021, 13, 5091. [Google Scholar] [CrossRef] [PubMed]
- Zhang, C.; Zhu, Q.; Gu, J.; Chen, S.; Li, Q.; Ying, L. Down-regulation of CCNE1 expression suppresses cell proliferation and sensitizes gastric carcinoma cells to Cisplatin. Biosci. Rep. 2019, 39, BSR20190381. [Google Scholar] [CrossRef] [PubMed]
- Zhao, H.; Wang, J.; Zhang, Y.; Yuan, M.; Yang, S.; Li, L.; Yang, H. Prognostic values of CCNE1 amplification and overexpression in cancer patients: A systematic review and meta-analysis. J. Cancer 2018, 9, 2397–2407. [Google Scholar] [CrossRef] [PubMed]
- Rustgi, N.; Wu, S.; Samec, T.; Walker, P.; Xiu, J.; Lou, E.; Goel, S.; Saeed, A.; Moy, R.H. Molecular Landscape and Clinical Implication of CCNE1-amplified Esophagogastric Cancer. Cancer Res. Commun. 2024, 4, 1399–1409. [Google Scholar] [CrossRef] [PubMed]
- Asghar, U.; Witkiewicz, A.K.; Turner, N.C.; Knudsen, E.S. The history and future of targeting cyclin-dependent kinases in cancer therapy. Nat. Rev. Drug Discov. 2015, 14, 130–146. [Google Scholar] [CrossRef] [PubMed]
- Turner, N.C.; Liu, Y.; Zhu, Z.; Loi, S.; Colleoni, M.; Loibl, S.; DeMichele, A.; Harbeck, N.; André, F.; Bayar, M.A.; et al. Cyclin E1 Expression and Palbociclib Efficacy in Previously Treated Hormone Receptor-Positive Metastatic Breast Cancer. J. Clin. Oncol. 2019, 37, 1169–1178. Available online: https://ascopubs.org/doi/10.1200/JCO.18.00925 (accessed on 17 May 2025). [CrossRef] [PubMed]
- Herrera-Abreu, M.T.; Palafox, M.; Asghar, U.; Rivas, M.A.; Cutts, R.J.; Garcia-Murillas, I.; Pearson, A.; Guzman, M.; Rodriguez, O.; Grueso, J.; et al. Early adaptation and acquired resistance to CDK4/6 inhibition in estrogen receptor-positive breast cancer. Cancer Res. 2016, 76, 2301–2313. [Google Scholar] [CrossRef] [PubMed]
- Scaltriti, M.; Eichhorn, P.J.; Cortés, J.; Prudkin, L.; Aura, C.; Jiménez, J.; Chandarlapaty, S.; Serra, V.; Prat, A.; Ibrahim, Y.H.; et al. Cyclin E amplification/overexpression is a mechanism of trastuzumab resistance in HER2+ breast cancer patients. Proc. Natl. Acad. Sci. USA 2011, 108, 3761–3766. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Clinicopathologic Features | CCNE1 Staining | |||
|---|---|---|---|---|
| Negative | Positive | p Value | ||
| N = 252 | N = 108 | |||
| Age | <65 | 102 (69.9%) | 44 (30.1%) | n.s. |
| ≥65 | 150 (70.1%) | 64 (29.9%) | ||
| Gender | female | 78 (78.0%) | 22 (22.0%) | 0.04 |
| male | 174 (66.9%) | 86 (33.1%) | ||
| Macroscopic type | Borrmann type 4 | 11 (78.6%) | 3 (21.4%) | n.s. |
| other types | 241 (69.7%) | 105 (30.3%) | ||
| Microscopic type | differentiated | 136 (69.4%) | 60 (30.6%) | n.s. |
| undifferentiated | 116 (70.7%) | 48 (29.3%) | ||
| Inf | α and β | 200 (70.7%) | 83 (29.3%) | n.s. |
| γ | 52 (67.5%) | 25 (32.5%) | ||
| T stage | T1 | 131 (76.2%) | 41 (23.8%) | 0.01 |
| T2,3,4 | 121 (64.4%) | 67 (35.6%) | ||
| Lymph node metastasis | negative | 161 (75.6%) | 52 (24.4%) | 0.01 |
| positive | 91 (61.9%) | 56 (38.1%) | ||
| Lymphatic invasion | negative | 128 (80.0%) | 32 (20.0%) | <0.001 |
| positive | 124 (62.0%) | 76 (38.0%) | ||
| Venous invasion | negative | 214 (70.4%) | 90 (29.6%) | n.s. |
| positive | 38 (67.9%) | 18 (32.1%) | ||
| Recurrence | negative | 213 (74.0%) | 75 (26.0%) | <0.001 |
| positive | 39 (54.2%) | 33 (45.8%) | ||
| Clinical stage | Ⅰ & Ⅱ | 200 (72.7%) | 75 (27.3%) | 0.04 |
| Ⅲ | 52 (61.2%) | 33 (38.8%) | ||
| Parameter | Univariate Analysis | Multivariate Analysis | ||||
|---|---|---|---|---|---|---|
| Hazard Ratio | 95% CI | p-Value | Hazard Ratio | 95% CI | p-Value | |
| CCNE1 | ||||||
| positive vs. negative | 2.12 | 1.34–3.38 | <0.001 | 1.63 | 1.01–2.63 | <0.05 |
| Age | ||||||
| <65 vs. ≥65 | 1.19 | 0.74–1.92 | n.s. | |||
| Gender | ||||||
| female vs. male | 0.90 | 0.54–1.49 | n.s. | |||
| Macroscopic type | ||||||
| Borrmann’s type 4 vs. Other types | 5.84 | 2.88–11.84 | <0.001 | 1.72 | 0.81–3.69 | n.s. |
| Microscopic type | ||||||
| differentiated vs. undifferentiated | 2.02 | 1.26–3.25 | <0.001 | 1.24 | 0.73–2.13 | n.s. |
| Inf | ||||||
| α and β vs. γ | 3.18 | 1.99–5.09 | <0.001 | 2.09 | 1.24–3.51 | 0.01 |
| T stage | ||||||
| T1 vs. T2–T4 | 15.46 | 6.23–38.38 | <0.001 | 4.72 | 1.76–12.61 | <0.001 |
| LN metastasis | ||||||
| negative vs. positive | 6.84 | 3.87–12.09 | <0.001 | 2.71 | 1.47–4.99 | <0.001 |
| Parameter | Unifactorial Analysis | Final Regression Model | ||||
|---|---|---|---|---|---|---|
| Hazard Ratio | 95% CI | p-Value | Hazard Ratio | 95% CI | p-Value | |
| CCNE1 | ||||||
| positive vs. negative | 2.74 | 1.13–6.67 | 0.03 | 2.89 | 1.10–7.55 | 0.03 |
| Age | ||||||
| <65 vs. ≥65 | 0.49 | 0.20–1.20 | 0.12 | 0.43 | 0.16–1.11 | n.s. |
| Gender | ||||||
| female vs. male | 0.68 | 0.44–3.50 | n.s. | |||
| Microscopic type | ||||||
| differentiated vs. undifferentiated | 0.89 | 0.37–2.17 | n.s. | |||
| Inf | ||||||
| α and β vs. γ | 1.16 | 0.41–3.27 | n.s. | |||
| T stage | ||||||
| T1 vs. T2,3,4 | 4.18 | 1.38–12.67 | 0.01 | 1.96 | 0.57–6.71 | n.s. |
| Venous invasion | ||||||
| negative vs. positive | 7.19 | 2.89–17.89 | <0.001 | 5.64 | 2.01–15.79 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nishikubo, H.; Kawabata, K.; Sano, T.; Kanei, S.; Aoyama, R.; Ma, D.; Imanishi, D.; Sakuma, T.; Maruo, K.; Yamamoto, Y.; et al. CCNE1 Gene Amplification Might Be Associated with Lymph Node Metastasis of Gastric Cancer. Genes 2025, 16, 617. https://doi.org/10.3390/genes16060617
Nishikubo H, Kawabata K, Sano T, Kanei S, Aoyama R, Ma D, Imanishi D, Sakuma T, Maruo K, Yamamoto Y, et al. CCNE1 Gene Amplification Might Be Associated with Lymph Node Metastasis of Gastric Cancer. Genes. 2025; 16(6):617. https://doi.org/10.3390/genes16060617
Chicago/Turabian StyleNishikubo, Hinano, Kyoka Kawabata, Tomoya Sano, Saki Kanei, Rika Aoyama, Dongheng Ma, Daiki Imanishi, Takashi Sakuma, Koji Maruo, Yurie Yamamoto, and et al. 2025. "CCNE1 Gene Amplification Might Be Associated with Lymph Node Metastasis of Gastric Cancer" Genes 16, no. 6: 617. https://doi.org/10.3390/genes16060617
APA StyleNishikubo, H., Kawabata, K., Sano, T., Kanei, S., Aoyama, R., Ma, D., Imanishi, D., Sakuma, T., Maruo, K., Yamamoto, Y., Fan, C., & Yashiro, M. (2025). CCNE1 Gene Amplification Might Be Associated with Lymph Node Metastasis of Gastric Cancer. Genes, 16(6), 617. https://doi.org/10.3390/genes16060617