
Polymorphisms within the SARS-CoV-2 Human Receptor Genes Associate with Variable Disease Outcomes across Ethnicities

 ,
,
Abstract
:1. Importance
2. Introduction
3. Methods
3.1. Study Design
3.2. SNPs Included in the Study
3.3. ACE2, NRP1 and SARS-CoV-2 Viral Load Quantification
3.4. Statistical and Bioinformatics Analysis
4. Results
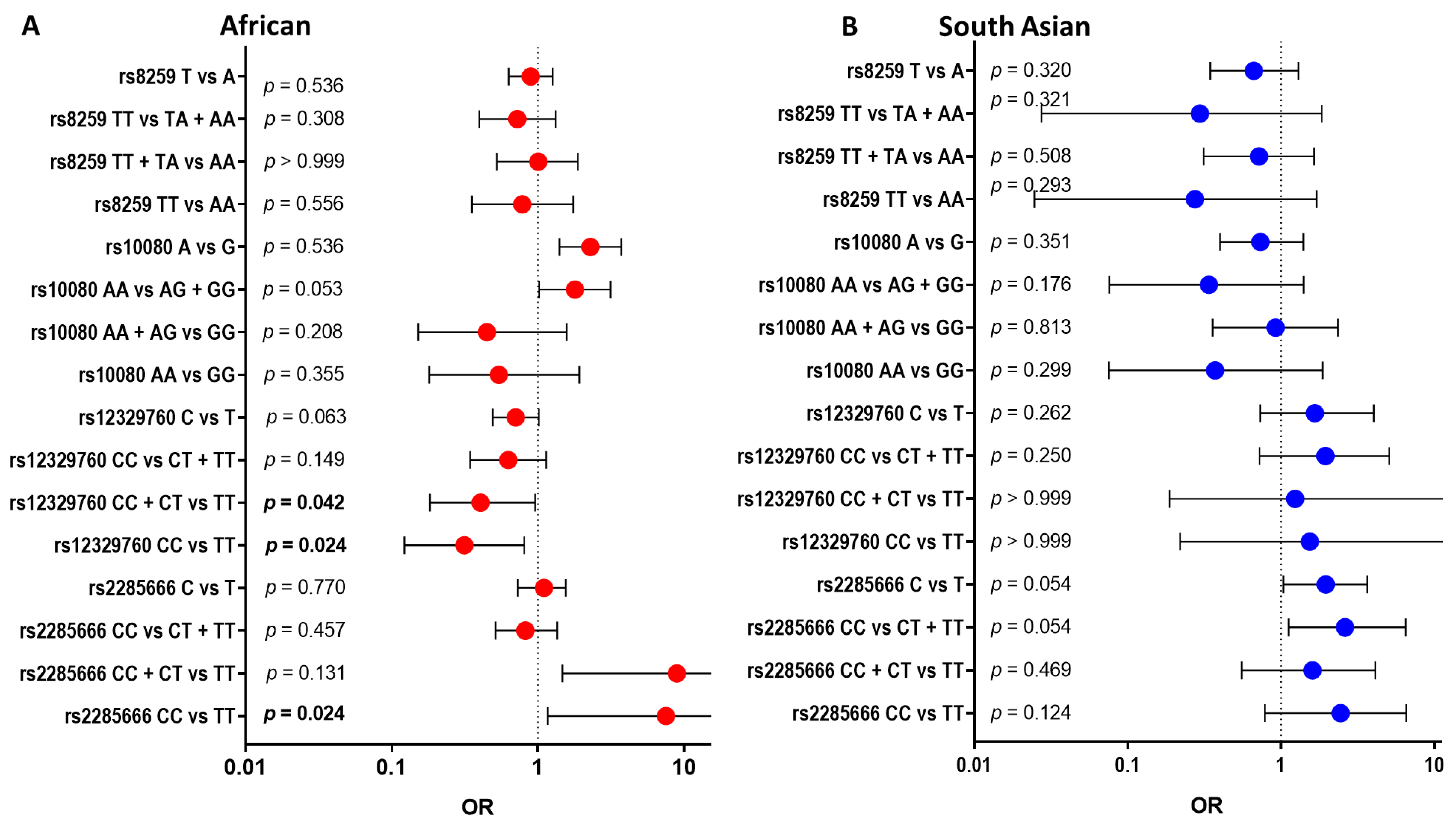
4.1. Variants within SARS-CoV-2 Receptor Genes Are Associated with COVID-19 Severity across Ethnic Groups
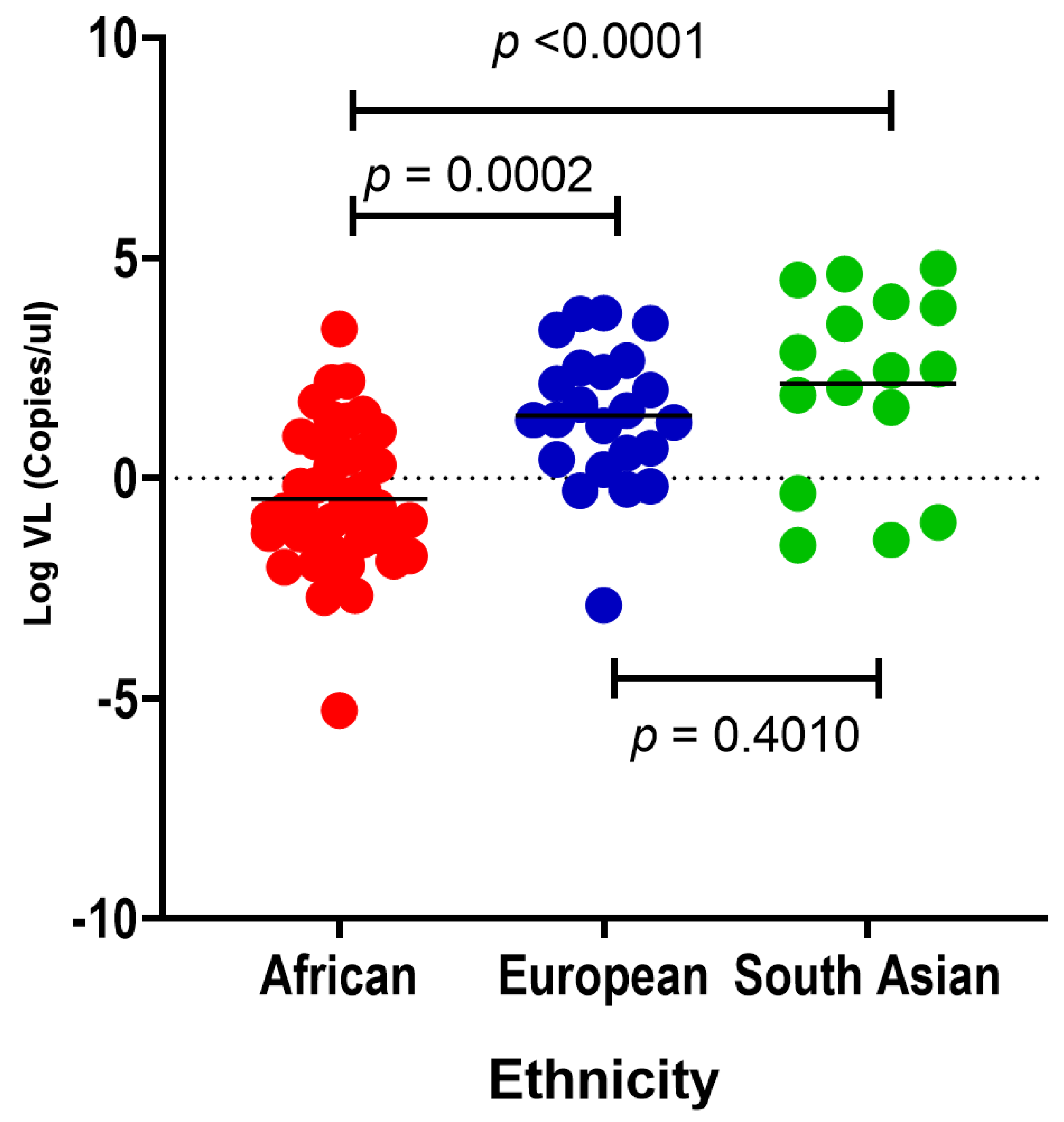
4.2. SARS-CoV-2 Viral Load Is Different across Ethnic Groups
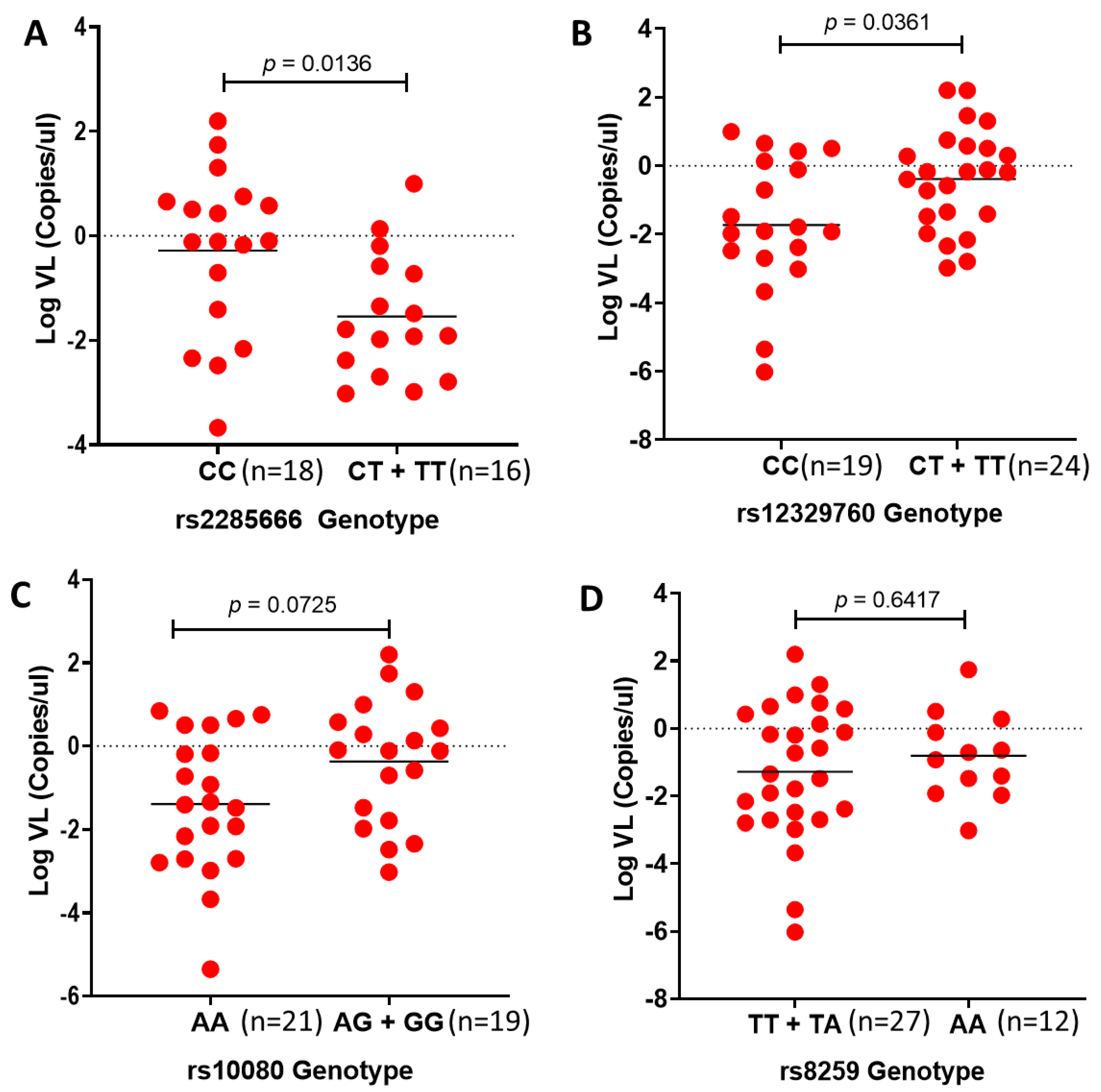
4.3. SARS-CoV-2 Viral Load Associates with rs2285666 (ACE2) and rs12329760 (TMPRSS2) in African Individuals
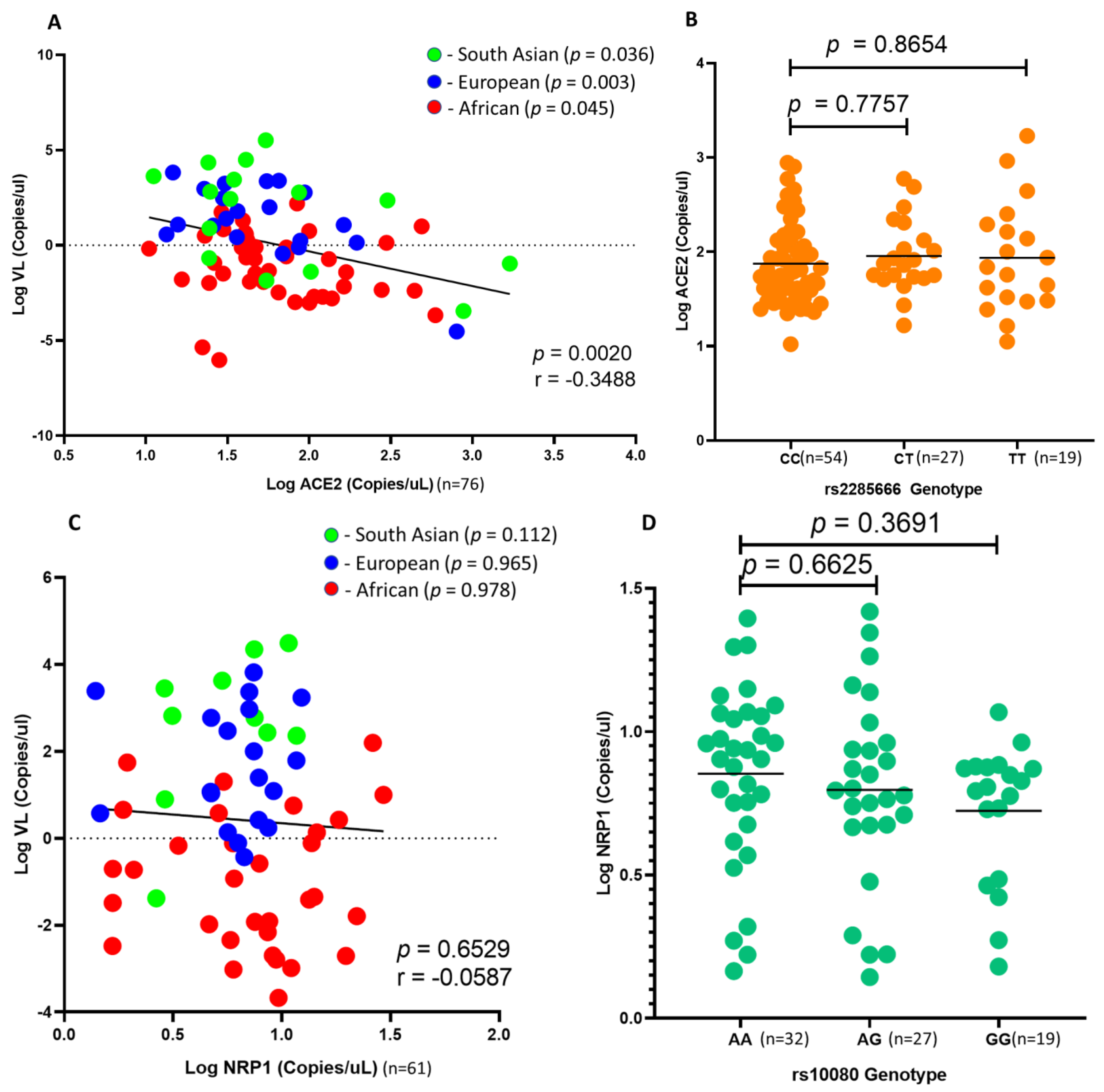
4.4. ACE2 and NRP1 Expression and SARS-CoV-2 Viral Load in African Individuals
5. Discussion
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Moore, M.; Gelfeld, B.; Okunogbe, A.; Paul, C. Identifying Future Disease Hot Spots: Infectious Disease Vulnerability Index. Rand Health Q 2017, 6, 5. [Google Scholar] [PubMed]
- Lone, S.A.; Ahmad, A. COVID-19 pandemic—An African perspective. Emerg. Microbes Infect 2020, 9, 1300–1308. [Google Scholar] [CrossRef]
- Massinga Loembé, M.; Tshangela, A.; Salyer, S.J.; Varma, J.K.; Ouma, A.E.O.; Nkengasong, J.N. COVID-19 in Africa: The spread and response. Nat. Med. 2020, 26, 999–1003. [Google Scholar] [CrossRef] [PubMed]
- Farhaan, S.V.; Juan Carlos, N.; Jennifer, R.M.; Osman, K.; Alan, P.; Stephen, L.J.; Faisal, M.; Sostman, H.D.; Robert, P.; Julia, D.A.; et al. Racial and ethnic disparities in SARS-CoV-2 pandemic: Analysis of a COVID-19 observational registry for a diverse US metropolitan population. BMJ Open 2020, 10, e039849. [Google Scholar]
- Robertson, M.M.; Shamsunder, M.G.; Brazier, E.; Mantravadi, M.; Zimba, R.; Rane, M.S.; Westmoreland, D.A.; Parcesepe, A.M.; Maroko, A.R.; Kulkarni, S.G.; et al. Racial/Ethnic Disparities in Exposure, Disease Susceptibility, and Clinical Outcomes during COVID-19 Pandemic in National Cohort of Adults, United States. Emerg. Infect. Dis. 2022, 28, 2171–2180. [Google Scholar] [CrossRef] [PubMed]
- Mathur, R.; Rentsch, C.T.; Morton, C.E.; Hulme, W.J.; Schultze, A.; MacKenna, B.; Eggo, R.M.; Bhaskaran, K.; Wong, A.Y.S.; Williamson, E.J.; et al. Ethnic differences in SARS-CoV-2 infection and COVID-19-related hospitalisation, intensive care unit admission, and death in 17 million adults in England: An observational cohort study using the OpenSAFELY platform. Lancet 2021, 397, 1711–1724. [Google Scholar] [CrossRef]
- Docherty, A.B.; Harrison, E.M.; Green, C.A.; Hardwick, H.E.; Pius, R.; Norman, L.; Holden, K.A.; Read, J.M.; Dondelinger, F.; Carson, G.; et al. Features of 20 133 UK patients in hospital with covid-19 using the ISARIC WHO Clinical Characterisation Protocol: Prospective observational cohort study. BMJ 2020, 369, m1985. [Google Scholar] [CrossRef]
- Kwok, A.J.; Mentzer, A.; Knight, J.C. Host genetics and infectious disease: New tools, insights and translational opportunities. Nat. Rev. Genet. 2021, 22, 137–153. [Google Scholar] [CrossRef]
- Adimulam, T.; Arumugam, T.; Gokul, A.; Ramsuran, V. Genetic Variants within SARS-CoV-2 Human Receptor Genes May Contribute to Variable Disease Outcomes in Different Ethnicities. Int. J. Mol. Sci. 2023, 24, 8711. [Google Scholar] [CrossRef]
- National Institutes of Health. COVID-19 Treatment Guidelines Panel. Coronavirus Disease 2019 (COVID-19) Treatment Guidelines. Available online: https://www.covid19treatmentguidelines.nih.gov/ (accessed on 20 April 2023).
- Doeschl-Wilson, A.B.; Davidson, R.; Conington, J.; Roughsedge, T.; Hutchings, M.R.; Villanueva, B. Implications of host genetic variation on the risk and prevalence of infectious diseases transmitted through the environment. Genetics 2011, 188, 683–693. [Google Scholar] [CrossRef]
- Frodsham, A.J.; Hill, A.V.S. Genetics of infectious diseases. Hum. Mol. Genet. 2004, 13 (Suppl. S2), R187–R194. [Google Scholar] [CrossRef] [PubMed]
- Hou, Y.; Zhao, J.; Martin, W.; Kallianpur, A.; Chung, M.K.; Jehi, L.; Sharifi, N.; Erzurum, S.; Eng, C.; Cheng, F. New insights into genetic susceptibility of COVID-19: An ACE2 and TMPRSS2 polymorphism analysis. BMC Med. 2020, 18, 216. [Google Scholar] [CrossRef] [PubMed]
- Namkoong, H.; Edahiro, R.; Takano, T.; Nishihara, H.; Shirai, Y.; Sonehara, K.; Tanaka, H.; Azekawa, S.; Mikami, Y.; Lee, H.; et al. DOCK2 is involved in the host genetics and biology of severe COVID-19. Nature 2022, 609, 754–760. [Google Scholar] [CrossRef] [PubMed]
- Cruz, R.; Diz-de Almeida, S.; López de Heredia, M.; Quintela, I.; Ceballos, F.C.; Pita, G.; Lorenzo-Salazar, J.M.; González-Montelongo, R.; Gago-Domínguez, M.; Sevilla Porras, M.; et al. Novel genes and sex differences in COVID-19 severity. Hum. Mol. Genet. 2022, 31, 3789–3806. [Google Scholar] [CrossRef]
- Anastassopoulou, C.; Gkizarioti, Z.; Patrinos, G.P.; Tsakris, A. Human genetic factors associated with susceptibility to SARS-CoV-2 infection and COVID-19 disease severity. Hum. Genom. 2020, 14, 40. [Google Scholar] [CrossRef] [PubMed]
- Molyneux, D.; Bush, S.; Bannerman, R.; Downs, P.; Shu’aibu, J.; Boko-Collins, P.; Radvan, I.; Wohlgemuth, L.; Boyton, C. Neglected tropical diseases activities in Africa in the COVID-19 era: The need for a “hybrid” approach in COVID-endemic times. Infect. Dis. Poverty 2021, 10, 1. [Google Scholar] [CrossRef]
- Molyneux, D.H.; Aboe, A.; Isiyaku, S.; Bush, S. COVID-19 and neglected tropical diseases in Africa: Impacts, interactions, consequences. Int. Health 2020, 12, 367–372. [Google Scholar] [CrossRef]
- Campbell, M.C.; Tishkoff, S.A. African genetic diversity: Implications for human demographic history, modern human origins, and complex disease mapping. Annu. Rev. Genom. Hum. Genet. 2008, 9, 403–433. [Google Scholar] [CrossRef]
- Winkler, C. Is there a genetic basis for health disparities in human immunodeficiency virus disease? Mt. Sinai J. Med. 2010, 77, 149–159. [Google Scholar] [CrossRef]
- Hoffmann, M.; Kleine-Weber, H.; Schroeder, S.; Krüger, N.; Herrler, T.; Erichsen, S.; Schiergens, T.S.; Herrler, G.; Wu, N.-H.; Nitsche, A.; et al. SARS-CoV-2 cell entry depends on ACE2 and TMPRSS2 and is blocked by a clinically proven protease inhibitor. Cell 2020, 181, 271–280.e8. [Google Scholar] [CrossRef]
- Zhou, P.; Yang, X.-L.; Wang, X.-G.; Hu, B.; Zhang, L.; Zhang, W.; Si, H.-R.; Zhu, Y.; Li, B.; Huang, C.-L. A pneumonia outbreak associated with a new coronavirus of probable bat origin. Nature 2020, 579, 270–273. [Google Scholar] [CrossRef] [PubMed]
- Scialo, F.; Daniele, A.; Amato, F.; Pastore, L.; Matera, M.G.; Cazzola, M.; Castaldo, G.; Bianco, A. ACE2: The major cell entry receptor for SARS-CoV-2. Lung 2020, 198, 867–877. [Google Scholar] [CrossRef] [PubMed]
- Jackson, C.B.; Farzan, M.; Chen, B.; Choe, H. Mechanisms of SARS-CoV-2 entry into cells. Nat. Rev. Mol. Cell Biol. 2022, 23, 3–20. [Google Scholar] [CrossRef] [PubMed]
- Samavati, L.; Uhal, B.D. ACE2, much more than just a receptor for SARS-COV-2. Front. Cell. Infect. Microbiol. 2020, 10, 317. [Google Scholar] [CrossRef]
- Li, W.; Moore, M.J.; Vasilieva, N.; Sui, J.; Wong, S.K.; Berne, M.A.; Somasundaran, M.; Sullivan, J.L.; Luzuriaga, K.; Greenough, T.C. Angiotensin-converting enzyme 2 is a functional receptor for the SARS coronavirus. Nature 2003, 426, 450–454. [Google Scholar] [CrossRef]
- Yan, R.; Zhang, Y.; Li, Y.; Xia, L.; Guo, Y.; Zhou, Q. Structural basis for the recognition of SARS-CoV-2 by full-length human ACE2. Science 2020, 367, 1444–1448. [Google Scholar] [CrossRef]
- Mayi, B.S.; Leibowitz, J.A.; Woods, A.T.; Ammon, K.A.; Liu, A.E.; Raja, A. The role of Neuropilin-1 in COVID-19. PLoS Pathog. 2021, 17, e1009153. [Google Scholar] [CrossRef]
- Wang, K.; Chen, W.; Zhang, Z.; Deng, Y.; Lian, J.-Q.; Du, P.; Wei, D.; Zhang, Y.; Sun, X.-X.; Gong, L. CD147-spike protein is a novel route for SARS-CoV-2 infection to host cells. Signal Transduct. Target. Ther. 2020, 5, 283. [Google Scholar] [CrossRef]
- Hashemi, S.M.A.; Thijssen, M.; Hosseini, S.Y.; Tabarraei, A.; Pourkarim, M.R.; Sarvari, J. Human gene polymorphisms and their possible impact on the clinical outcome of SARS-CoV-2 infection. Arch. Virol. 2021, 166, 2089–2108. [Google Scholar] [CrossRef]
- Samson, M.; Libert, F.; Doranz, B.J.; Rucker, J.; Liesnard, C.; Farber, C.-M.; Saragosti, S.; Lapouméroulie, C.; Cognaux, J.; Forceille, C. Resistance to HIV-1 infection in caucasian individuals bearing mutant alleles of the CCR-5 chemokine receptor gene. Nature 1996, 382, 722–725. [Google Scholar] [CrossRef]
- de Silva, E.; Stumpf, M.P.H. HIV and the CCR5-Δ32 resistance allele. FEMS Microbiol. Lett. 2004, 241, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Martinson, J.J.; Chapman, N.H.; Rees, D.C.; Liu, Y.-T.; Clegg, J.B. Global distribution of the CCR5 gene 32-basepair deletion. Nat. Genet. 1997, 16, 100–103. [Google Scholar] [CrossRef] [PubMed]
- Ovsyannikova, I.G.; Haralambieva, I.H.; Crooke, S.N.; Poland, G.A.; Kennedy, R.B. The role of host genetics in the immune response to SARS-CoV-2 and COVID-19 susceptibility and severity. Immunol. Rev. 2020, 296, 205–219. [Google Scholar] [CrossRef] [PubMed]
- Fernández-de-Las-Peñas, C.; Arendt-Nielsen, L.; Díaz-Gil, G.; Gómez-Esquer, F.; Gil-Crujera, A.; Gómez-Sánchez, S.M.; Ambite-Quesada, S.; Palomar-Gallego, M.A.; Pellicer-Valero, O.J.; Giordano, R. Genetic Association between ACE2 (rs2285666 and rs2074192) and TMPRSS2 (rs12329760 and rs2070788) Polymorphisms with Post-COVID Symptoms in Previously Hospitalized COVID-19 Survivors. Genes 2022, 13, 1935. [Google Scholar] [CrossRef]
- Abdelsattar, S.; Kasemy, Z.A.; Ewida, S.F.; Abo-Elsoud, R.A.A.; Zytoon, A.A.; Abdelaal, G.A.; Abdelgawad, A.S.; Khalil, F.O.; Kamel, H.F.M. ACE2 and TMPRSS2 SNPs as Determinants of Susceptibility to, and Severity of, a COVID-19 Infection. Br. J. Biomed. Sci. 2022, 79, 10238. [Google Scholar] [CrossRef]
- Fan, S.-H.; Shen, Z.-Y.; Xiao, Y.-M. Functional polymorphisms of the neuropilin 1 gene are associated with the risk of tetralogy of Fallot in a Chinese Han population. Gene 2018, 653, 72–79. [Google Scholar] [CrossRef]
- Agúndez, J.A.; García-Martín, E.; Martínez, C.; Benito-León, J.; Millán-Pascual, J.; Díaz-Sánchez, M.; Calleja, P.; Pisa, D.; Turpín-Fenoll, L.; Alonso-Navarro, H.; et al. Heme Oxygenase-1 and 2 Common Genetic Variants and Risk for Multiple Sclerosis. Sci. Rep. 2016, 6, 20830. [Google Scholar] [CrossRef]
- Wu, L.-S.; Li, F.-F.; Sun, L.-D.; Li, D.; Su, J.; Kuang, Y.-H.; Chen, G.; Chen, X.-P.; Chen, X. A miRNA-492 binding-site polymorphism in BSG (basigin) confers risk to psoriasis in central south Chinese population. Hum. Genet. 2011, 130, 749–757. [Google Scholar] [CrossRef]
- Rosner, B. Fundamentals of Biostatistics, 7th, ed.; Brooks/Cole: Boston, MA, USA, 2011. [Google Scholar]
- Petersen, J.; Jhala, D. Ethnicity, Comorbid Medical Conditions, and SARS-CoV-2 Test Cycle Thresholds in the Veteran Population. J. Racial Ethn. Health Disparities 2021, 9, 1775–1782. [Google Scholar] [CrossRef]
- Wrapp, D.; Wang, N.; Corbett, K.S.; Goldsmith, J.A.; Hsieh, C.L.; Abiona, O.; Graham, B.S.; McLellan, J.S. Cryo-EM structure of the 2019-nCoV spike in the prefusion conformation. Science 2020, 367, 1260–1263. [Google Scholar] [CrossRef]
- Najafi, M.; Mahdavi, M.R. Association investigations between ACE1 and ACE2 polymorphisms and severity of COVID-19 disease. Mol. Genet. Genom. 2023, 298, 27–36. [Google Scholar] [CrossRef]
- Beyranvand, S.; Davoodian, P.; Alizade, H.; Gouklani, H.; Nejatizadeh, A.; Eftekhar, E.; Nikpoor, A.R. Study of frequency and inheritance model of ACE1 I/D and ACE2 rs2285666 polymorphisms in COVID-19 patients with varying severity of lung involvement and its effect on serum cytokines levels. Cell Biol. Int. 2023, 47, 731–741. [Google Scholar] [CrossRef]
- Keikha, M. and M. Karbalaei, Global distribution of ACE1 (rs4646994) and ACE2 (rs2285666) polymorphisms associated with COVID-19: A systematic review and meta-analysis. Microb. Pathog. 2022, 172, 105781. [Google Scholar] [CrossRef]
- Latini, A.; Agolini, E.; Novelli, A.; Borgiani, P.; Giannini, R.; Gravina, P.; Smarrazzo, A.; Dauri, M.; Andreoni, M.; Rogliani, P.; et al. COVID-19 and Genetic Variants of Protein Involved in the SARS-CoV-2 Entry into the Host Cells. Genes 2020, 11, 1010. [Google Scholar] [CrossRef]
- Singh, H.; Choudhari, R.; Nema, V.; Khan, A.A. ACE2 and TMPRSS2 polymorphisms in various diseases with special reference to its impact on COVID-19 disease. Microb. Pathog. 2021, 150, 104621. [Google Scholar] [CrossRef]
- Dos Santos Nascimento, I.J.; da Silva-Júnior, E.F.; de Aquino, T.M. Molecular Modeling Targeting Transmembrane Serine Protease 2 (TMPRSS2) as an Alternative Drug Target Against Coronaviruses. Curr. Drug Targets 2022, 23, 240–259. [Google Scholar] [CrossRef]
- Khalilzadeh, F.; Sakhaee, F.; Sotoodehnejadnematalahi, F.; Zamani, M.S.; Ahmadi, I.; Anvari, E.; Fateh, A. Angiotensin-converting enzyme 2 rs2285666 polymorphism and clinical parameters as the determinants of COVID-19 severity in Iranian population. Int. J. Immunogenet. 2022, 49, 325–332. [Google Scholar] [CrossRef]
- Beheshti Shirazi, S.S.; Sakhaee, F.; Sotoodehnejadnematalahi, F.; Zamani, M.S.; Ahmadi, I.; Anvari, E.; Fateh, A. rs12329760 Polymorphism in Transmembrane Serine Protease 2 Gene and Risk of Coronavirus Disease 2019 Mortality. Biomed. Res. Int. 2022, 2022, 7841969. [Google Scholar] [CrossRef]
- Sabater Molina, M.; Nicolás Rocamora, E.; Bendicho, A.I.; Vázquez, E.G.; Zorio, E.; Rodriguez, F.D.; Gil Ortuño, C.; Rodríguez, A.I.; Sánchez-López, A.J.; Jara Rubio, R. Polymorphisms in ACE, ACE2, AGTR1 genes and severity of COVID-19 disease. PLoS ONE 2022, 17, e0263140. [Google Scholar] [CrossRef]
- Wulandari, L.; Hamidah, B.; Pakpahan, C.; Damayanti, N.S.; Kurniati, N.D.; Adiatmaja, C.O.; Wigianita, M.R.; Soedarsono; Husada, D.; Tinduh, D.; et al. Initial study on TMPRSS2 p.Val160Met genetic variant in COVID-19 patients. Hum. Genom. 2021, 15, 29. [Google Scholar] [CrossRef]
- Torre-Fuentes, L.; Matías-Guiu, J.; Hernández-Lorenzo, L.; Montero-Escribano, P.; Pytel, V.; Porta-Etessam, J.; Gómez-Pinedo, U.; Matías-Guiu, J.A. ACE2, TMPRSS2, and Furin variants and SARS-CoV-2 infection in Madrid, Spain. J. Med. Virol. 2021, 93, 863–869. [Google Scholar] [CrossRef] [PubMed]
- Schönfelder, K.; Breuckmann, K.; Elsner, C.; Dittmer, U.; Fistera, D.; Herbstreit, F.; Risse, J.; Schmidt, K.; Sutharsan, S.; Taube, C.; et al. Transmembrane serine protease 2 Polymorphisms and Susceptibility to Severe Acute Respiratory Syndrome Coronavirus Type 2 Infection: A German Case-Control Study. Front. Genet. 2021, 12, 667231. [Google Scholar] [CrossRef] [PubMed]
- Karakaş Çelik, S.; Çakmak Genç, G.; Pişkin, N.; Açikgöz, B.; Altinsoy, B.; Kurucu İşsiz, B.; Dursun, A. Polymorphisms of ACE (I/D) and ACE2 receptor gene (Rs2106809, Rs2285666) are not related to the clinical course of COVID-19: A case study. J. Med. Virol. 2021, 93, 5947–5952. [Google Scholar] [CrossRef] [PubMed]
- Srivastava, A.; Pandey, R.K.; Singh, P.P.; Kumar, P.; Rasalkar, A.A.; Tamang, R.; van Driem, G.; Shrivastava, P.; Chaubey, G. Most frequent South Asian haplotypes of ACE2 share identity by descent with East Eurasian populations. PLoS ONE 2020, 15, e0238255. [Google Scholar] [CrossRef] [PubMed]
- Nhung, V.P.; Ton, N.D.; Ngoc, T.T.B.; Thuong, M.T.H.; Hai, N.T.T.; Oanh, K.T.P.; Hien, L.T.T.; Thach, P.N.; Hai, N.V.; Ha, N.H. Host Genetic Risk Factors Associated with COVID-19 Susceptibility and Severity in Vietnamese. Genes 2022, 13, 1884. [Google Scholar] [CrossRef]
- Sekiya, T.; Ogura, Y.; Kai, H.; Kawaguchi, A.; Okawa, S.; Hirohama, M.; Kuroki, T.; Morii, W.; Hara, A.; Hiramatsu, Y.; et al. TMPRSS2 gene polymorphism common in East Asians confers decreased COVID-19 susceptibility. Front. Microbiol. 2022, 13, 943877. [Google Scholar] [CrossRef]
- Yaghoobi, A.; Lord, J.S.; Rezaiezadeh, J.S.; Yekaninejad, M.S.; Amini, M.; Izadi, P. TMPRSS2 polymorphism (rs12329760) and the severity of the COVID-19 in Iranian population. PLoS ONE 2023, 18, e0281750. [Google Scholar] [CrossRef]
- Posadas-Sánchez, R.; Fragoso, J.M.; Sánchez-Muñoz, F.; Rojas-Velasco, G.; Ramírez-Bello, J.; López-Reyes, A.; Martínez-Gómez, L.E.; Sierra-Fernández, C.; Rodríguez-Reyna, T.; Regino-Zamarripa, N.E.; et al. Association of the Transmembrane Serine Protease-2 (TMPRSS2) Polymorphisms with COVID-19. Viruses 2022, 14, 1976. [Google Scholar] [CrossRef]
- Senapati, S.; Kumar, S.; Singh, A.K.; Banerjee, P.; Bhagavatula, S. Assessment of risk conferred by coding and regulatory variations of TMPRSS2 and CD26 in susceptibility to SARS-CoV-2 infection in human. J. Genet. 2020, 99, 53. [Google Scholar] [CrossRef]
- Chapoval, S.; Keegan, A.D. Perspectives and potential approaches for targeting neuropilin 1 in SARS-CoV-2 infection. Mol. Med. 2021, 27, 162. [Google Scholar] [CrossRef]
- Fenizia, C.; Galbiati, S.; Vanetti, C.; Vago, R.; Clerici, M.; Tacchetti, C.; Daniele, T. SARS-CoV-2 Entry: At the Crossroads of CD147 and ACE2. Cells 2021, 10, 1434. [Google Scholar] [CrossRef] [PubMed]
- Kaidashev, I.; Izmailova, O.; Shlykova, O.; Kabaliei, A.; Vatsenko, A.; Ivashchenko, D.; Dudchenko, M.; Volianskyi, A.; Zelinskyy, G.; Koval, T.; et al. Polymorphism of tmprss2 (rs12329760) but not ace2 (rs4240157), tmprss11a (rs353163) and cd147 (rs8259) is associated with the severity of COVID-19 in the Ukrainian population. Acta Biomed. 2023, 94, e2023030. [Google Scholar] [PubMed]
- Nikiforuk, A.M.; Kuchinski, K.S.; Twa, D.D.W.; Lukac, C.D.; Sbihi, H.; Basham, C.A.; Steidl, C.; Prystajecky, N.A.; Jassem, A.N.; Krajden, M.; et al. The contrasting role of nasopharyngeal angiotensin converting enzyme 2 (ACE2) transcription in SARS-CoV-2 infection: A cross-sectional study of people tested for COVID-19 in British Columbia, Canada. EBioMedicine 2021, 66, 103316. [Google Scholar]
- Gutiérrez-Chamorro, L.; Riveira-Muñoz, E.; Barrios, C.; Palau, V.; Nevot, M.; Pedreño-López, S.; Senserrich, J.; Massanella, M.; Clotet, B.; Cabrera, C.; et al. SARS-CoV-2 Infection Modulates ACE2 Function and Subsequent Inflammatory Responses in Swabs and Plasma of COVID-19 Patients. Viruses 2021, 13, 1715. [Google Scholar] [CrossRef] [PubMed]
- Fajnzylber, J.; Regan, J.; Coxen, K.; Corry, H.; Wong, C.; Rosenthal, A.; Worrall, D.; Giguel, F.; Piechocka-Trocha, A.; Atyeo, C. SARS-CoV-2 viral load is associated with increased disease severity and mortality. Nat. Commun. 2020, 11, 5493. [Google Scholar] [CrossRef]
- To, K.K.-W.; Tsang, O.T.-Y.; Leung, W.-S.; Tam, A.R.; Wu, T.-C.; Lung, D.C.; Yip, C.C.-Y.; Cai, J.-P.; Chan, J.M.-C.; Chik, T.S.-H. Temporal profiles of viral load in posterior oropharyngeal saliva samples and serum antibody responses during infection by SARS-CoV-2: An observational cohort study. Lancet Infect. Dis. 2020, 20, 565–574. [Google Scholar] [CrossRef]
- Zoufaly, A.; Poglitsch, M.; Aberle, J.H.; Hoepler, W.; Seitz, T.; Traugott, M.; Grieb, A.; Pawelka, E.; Laferl, H.; Wenisch, C. Human recombinant soluble ACE2 in severe COVID-19. Lancet Respir. Med. 2020, 8, 1154–1158. [Google Scholar] [CrossRef]
- Gonzalez, S.M.; Siddik, A.B.; Su, R.-C. Regulated Intramembrane proteolysis of ACE2: A potential mechanism contributing to COVID-19 pathogenesis? Front. Immunol. 2021, 12, 612807. [Google Scholar] [CrossRef]
- Garcia-Escobar, A.; Jimenez-Valero, S.; Galeote, G.; Jurado-Roman, A.; Garcia-Rodriguez, J.; Moreno, R. The soluble catalytic ectodomain of ACE2 a biomarker of cardiac remodelling: New insights for heart failure and COVID19. Heart Fail. Rev. 2021, 26, 961–971. [Google Scholar]
- Singh, R.; Ramsuran, V.; Naranbhai, V.; Yende-Zuma, N.; Garrett, N.; Mlisana, K.; Dong, K.L.; Walker, B.D.; Abdool Karim, S.S.; Carrington, M.; et al. Epigenetic Regulation of BST-2 Expression Levels and the Effect on HIV-1 Pathogenesis. Front. Immunol. 2021, 12, 669241. [Google Scholar] [CrossRef]
- Ortiz, M.E.; Thurman, A.; Pezzulo, A.A.; Leidinger, M.R.; Klesney-Tait, J.A.; Karp, P.H.; Tan, P.; Wohlford-Lenane, C.; McCray, P.B.; Meyerholz, D.K. Heterogeneous expression of the SARS-Coronavirus-2 receptor ACE2 in the human respiratory tract. EBioMedicine 2020, 60. [Google Scholar] [CrossRef]
- Bubar, K.M.; Reinholt, K.; Kissler, S.M.; Lipsitch, M.; Cobey, S.; Grad, Y.H.; Larremore, D.B. Model-informed COVID-19 vaccine prioritization strategies by age and serostatus. Science 2021, 371, 916–921. [Google Scholar] [PubMed]
- Bruce, J.; Johnson, S.B. Exploring the ethics of genetic prioritisation for COVID-19 vaccines. Eur. J. Hum. Genet. 2022, 30, 875–879. [Google Scholar] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No Clinical Presentations (n = 133) | Clinical Presentations Present (n = 427) | |
|---|---|---|
| Primary Factors | ||
| Asymptomatic | Yes | No |
| Symptomatic | No | Yes |
| Secondary Factors | ||
| Oxygen required | No | Yes |
| Hospitalised | No | Yes |
| Pneumonia | No | Yes |
| Confusion | No | Yes |
| Sore throat | No | Yes |
| Loss of taste/smell | No | Yes |
| Nausea/Vomiting | No | Yes |
| Headache | No | Yes |
| Shortness of breath | No | Yes |
| Body aches | No | Yes |
| Fatigue | No | Yes |
| Cough | No | Yes |
| Fever and chills | No | Yes |
| Ethnicity | No Clinical Presentations (n = 133) | Have Clinical Presentations (n = 427) | Total |
|---|---|---|---|
| African | 102 (35%) | 188 (65%) | 290 |
| South Asian | 26 (11%) | 220 (89%) | 246 |
| European | 5 (21%) | 19 (79%) | 24 |
| Chr | Gene | Locus | rs Number | Variant | Variant Type | MAF (1000 Genome) | Freq in SAP Cohort |
|---|---|---|---|---|---|---|---|
| x | ACE2 | NG_012575.2 | rs2285666 | C > T | Intron variant | EUR:C = 0.76; T = 0.24 AFR:C = 0.79; T = 0.21 SAS:C = 0.51; T = 0.49 | EUR:C = 0.69; T = 0.31 AFR:C = 0.73; T = 0.27 SAS:C = 0.54; T = 0.46 |
| 21 | TMPRSS2 | NG_047085.2 | rs12329760 | C > T | Missense variant (Valine to Methionine) | EUR:C = 0.76; T = 0.24 AFR:C = 0.71; T = 0.29 SAS:C = 0.77; T = 0.23 | EUR:C = 0.77; T = 0.23 AFR:C = 0.78; T = 0.22 SAS:C = 0.78; T = 0.22 |
| 10 | NRP1 | NG_030328.1 | rs10080 | A > G | 3′UTR variant | EUR:G = 0.57; A = 0.43 AFR:G = 0.30; A = 0.70 SAS:G = 0.50; A = 0.50 | EUR:G = 0.61; A = 0.39 AFR:G = 0.28; A = 0.72 SAS:G = 0.63; A = 0.37 |
| 19 | CD147 | NG_007468.1 | rs8259 | T > A | 3′UTR variant | EUR:T = 0.70; A = 0.30 AFR:T = 0.44; A = 0.56 SAS:T = 0.37; A = 0.63 | EUR:T = 0.50; A = 0.50 AFR:T = 0.40; A = 0.60 SAS:T = 0.19; A = 0.81 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Adimulam, T.; Arumugam, T.; Naidoo, A.; Naidoo, K.; Ramsuran, V. Polymorphisms within the SARS-CoV-2 Human Receptor Genes Associate with Variable Disease Outcomes across Ethnicities. Genes 2023, 14, 1798. https://doi.org/10.3390/genes14091798
Adimulam T, Arumugam T, Naidoo A, Naidoo K, Ramsuran V. Polymorphisms within the SARS-CoV-2 Human Receptor Genes Associate with Variable Disease Outcomes across Ethnicities. Genes. 2023; 14(9):1798. https://doi.org/10.3390/genes14091798
Chicago/Turabian StyleAdimulam, Theolan, Thilona Arumugam, Anushka Naidoo, Kogieleum Naidoo, and Veron Ramsuran. 2023. "Polymorphisms within the SARS-CoV-2 Human Receptor Genes Associate with Variable Disease Outcomes across Ethnicities" Genes 14, no. 9: 1798. https://doi.org/10.3390/genes14091798
APA StyleAdimulam, T., Arumugam, T., Naidoo, A., Naidoo, K., & Ramsuran, V. (2023). Polymorphisms within the SARS-CoV-2 Human Receptor Genes Associate with Variable Disease Outcomes across Ethnicities. Genes, 14(9), 1798. https://doi.org/10.3390/genes14091798