
PROZ Associated with Sorafenib Sensitivity May Serve as a Potential Target to Enhance the Efficacy of Combined Immunotherapy for Hepatocellular Carcinoma

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Tissue Microarrays (TMAs) Construction
2.2. Patients
2.3. Immunohistochemical (IHC)
2.4. Cell Lines and Cell Culture
2.5. Gene Interfering of PROZ in HepG2 Cells Using shRNA
2.6. Western Blot Analysis
2.6.1. The Cancer Genome Atlas (TCGA) and Gene Expression Omnibus (GEO) Database Analysis
2.6.2. GO and KEGG Analysis
2.7. Statistical Analysis
3. Results
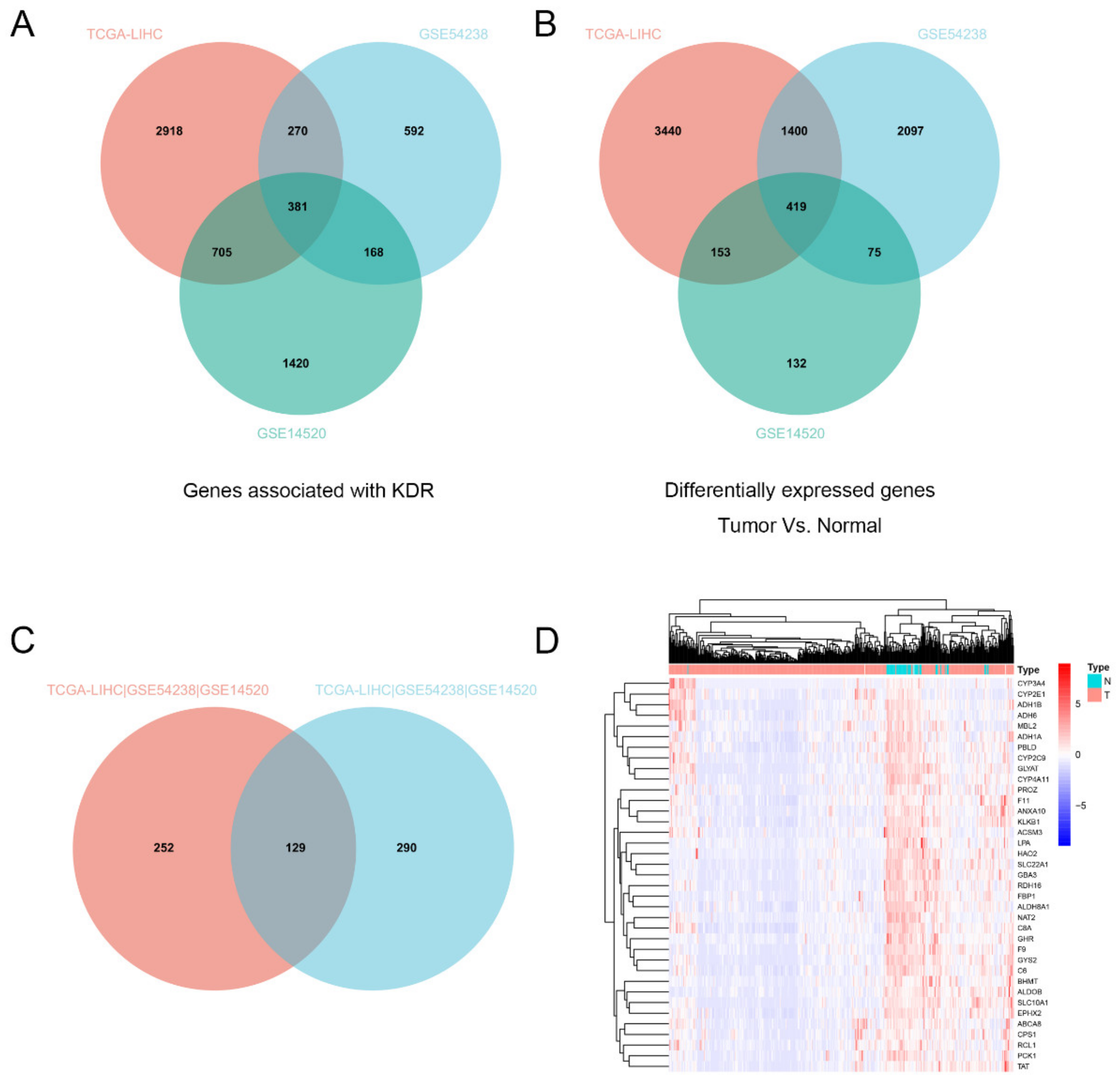
3.1. PROZ Was Correlated with KDR Expression
3.2. Expression of PROZ in Hepatocellular Carcinoma and Its Correlation with Prognosis of HCC Based on TCGA
3.3. The Correlation between the Expression of PROZ in Tissue and Prognosis of HCC Based on Our Database
3.4. Analysis of PROZ-Related Signaling Pathways
3.5. PROZ Is Associated with Sorafenib Therapy in HCC
3.6. Potential Relevance of PROZ to Immunotherapy
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Finn, R.S.; Qin, S.; Ikeda, M.; Galle, P.R.; Ducreux, M.; Kim, T.Y.; Kudo, M.; Breder, V.; Merle, P.; Kaseb, A.O.; et al. Atezolizumab plus Bevacizumab in Unresectable Hepatocellular Carcinoma. N. Engl. J. Med. 2020, 382, 1894–1905. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.S.; Ryoo, B.Y.; Hsu, C.H.; Numata, K.; Stein, S.; Verret, W.; Hack, S.P.; Spahn, J.; Liu, B.; Abdullah, H.; et al. Atezolizumab with or without bevacizumab in unresectable hepatocellular carcinoma (GO30140): An open-label, multicentre, phase 1b study. Lancet Oncol. 2020, 21, 808–820. [Google Scholar] [CrossRef]
- Kim, H.D.; Park, S.; Jeong, S.; Lee, Y.J.; Lee, H.; Kim, C.G.; Kim, K.H.; Hong, S.M.; Lee, J.Y.; Kim, S.; et al. 4-1BB Delineates Distinct Activation Status of Exhausted Tumor-Infiltrating CD8(+) T Cells in Hepatocellular Carcinoma. Hepatology 2020, 71, 955–971. [Google Scholar] [CrossRef] [PubMed]
- Zhu, A.X.; Abbas, A.R.; de Galarreta, M.R.; Guan, Y.; Lu, S.; Koeppen, H.; Zhang, W.; Hsu, C.H.; He, A.R.; Ryoo, B.Y.; et al. Molecular correlates of clinical response and resistance to atezolizumab in combination with bevacizumab in advanced hepatocellular carcinoma. Nat. Med. 2022, 28, 1599–1611. [Google Scholar] [CrossRef] [PubMed]
- Cheng, A.L.; Kang, Y.K.; Chen, Z.; Tsao, C.J.; Qin, S.; Kim, J.S.; Luo, R.; Feng, J.; Ye, S.; Yang, T.S.; et al. Efficacy and safety of sorafenib in patients in the Asia-Pacific region with advanced hepatocellular carcinoma: A phase III randomised, double-blind, placebo-controlled trial. Lancet Oncol. 2009, 10, 25–34. [Google Scholar] [CrossRef]
- Llovet, J.M.; Ricci, S.; Mazzaferro, V.; Hilgard, P.; Gane, E.; Blanc, J.F.; de Oliveira, A.C.; Santoro, A.; Raoul, J.L.; Forner, A.; et al. Sorafenib in advanced hepatocellular carcinoma. N. Engl. J. Med. 2008, 359, 378–390. [Google Scholar] [CrossRef]
- Qin, J.; Huang, Y.; Zhou, H.; Yi, S. Efficacy of Sorafenib Combined With Immunotherapy Following Transarterial Chemoembolization for Advanced Hepatocellular Carcinoma: A Propensity Score Analysis. Front. Oncol. 2022, 12, 807102. [Google Scholar] [CrossRef]
- Zheng, L.; Fang, S.; Wu, F.; Chen, W.; Chen, M.; Weng, Q.; Wu, X.; Song, J.; Zhao, Z.; Ji, J. Efficacy and Safety of TACE Combined With Sorafenib Plus Immune Checkpoint Inhibitors for the Treatment of Intermediate and Advanced TACE-Refractory Hepatocellular Carcinoma: A Retrospective Study. Front. Mol. Biosci. 2020, 7, 609322. [Google Scholar] [CrossRef]
- Almawi, W.Y.; Al-Shaikh, F.S.; Melemedjian, O.K.; Almawi, A.W. Protein Z, an anticoagulant protein with expanding role in reproductive biology. Reproduction 2013, 146, R73–R80. [Google Scholar] [CrossRef]
- Wu, D.H.; Wang, T.T.; Ruan, D.Y.; Li, X.; Chen, Z.H.; Wen, J.Y.; Lin, Q.; Ma, X.K.; Wu, X.Y.; Jia, C.C. Combination of ULK1 and LC3B improve prognosis assessment of hepatocellular carcinoma. Biomed. Pharmacother. 2018, 97, 195–202. [Google Scholar] [CrossRef]
- Wu, D.H.; Jia, C.C.; Chen, J.; Lin, Z.X.; Ruan, D.Y.; Li, X.; Lin, Q.; Ma, X.K.; Wan, X.B.; Cheng, N.; et al. Autophagic LC3B overexpression correlates with malignant progression and predicts a poor prognosis in hepatocellular carcinoma. Tumour Biol. 2014, 35, 12225–12233. [Google Scholar] [CrossRef] [PubMed]
- Jia, C.C.; Wang, T.T.; Liu, W.; Fu, B.S.; Hua, X.; Wang, G.Y.; Li, T.J.; Li, X.; Wu, X.Y.; Tai, Y.; et al. Cancer-associated fibroblasts from hepatocellular carcinoma promote malignant cell proliferation by HGF secretion. PLoS ONE 2013, 8, e63243. [Google Scholar] [CrossRef] [PubMed]
- Wu, X.; Zhang, Z.X.; Chen, X.Y.; Xu, Y.L.; Yin, N.; Yang, J.; Zhu, D.M.; Li, D.C.; Zhou, J. A Panel of Three Biomarkers Identified by iTRAQ for the Early Diagnosis of Pancreatic Cancer. Proteom. Clin. Appl. 2019, 13, e1800195. [Google Scholar] [CrossRef] [PubMed]
- Jiang, X.; Song, T.; Pan, X.; Zhang, X.; Lan, Y.; Bai, L. PROZ May Serve as a Prognostic Biomarker for Early Hepatocellular Carcinoma. Int. J. Gen. Med. 2021, 14, 4209–4218. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Xu, J.; Cui, H.; Song, J.; Chen, J.; Wei, J. Bioinformatics analysis of key biomarkers and potential molecular mechanisms in hepatocellular carcinoma induced by hepatitis B virus. Medicine 2020, 99, e20302. [Google Scholar] [CrossRef]
- Huang, X.; Swanson, R.; Kroh, H.K.; Bock, P.E. Protein Z-dependent protease inhibitor (ZPI) is a physiologically significant inhibitor of prothrombinase function. J. Biol. Chem. 2019, 294, 7644–7657. [Google Scholar] [CrossRef]
- Corral, J.; Gonzalez-Conejero, R.; Hernandez-Espinosa, D.; Vicente, V. Protein Z/Z-dependent protease inhibitor (PZ/ZPI) anticoagulant system and thrombosis. Br. J. Haematol. 2007, 137, 99–108. [Google Scholar] [CrossRef]
- Salloum-Asfar, S.; Arroyo, A.B.; Teruel-Montoya, R.; Garcia-Barbera, N.; Roldan, V.; Vicente, V.; Martinez, C.; Gonzalez-Conejero, R. MiRNA-Based Regulation of Hemostatic Factors through Hepatic Nuclear Factor-4 α. PLoS ONE 2016, 11, e154751. [Google Scholar] [CrossRef]
- Liang, P.; Ballou, B.; Lv, X.; Si, W.; Bruchez, M.P.; Huang, W.; Dong, X. Monotherapy and Combination Therapy Using Anti-Angiogenic Nanoagents to Fight Cancer. Adv. Mater. 2021, 33, e2005155. [Google Scholar] [CrossRef]
- Vasudev, N.S.; Reynolds, A.R. Anti-angiogenic therapy for cancer: Current progress, unresolved questions and future directions. Angiogenesis 2014, 17, 471–494. [Google Scholar] [CrossRef] [Green Version]
- Wakelee, H.A.; Dahlberg, S.E.; Keller, S.M.; Tester, W.J.; Gandara, D.R.; Graziano, S.L.; Adjei, A.A.; Leighl, N.B.; Aisner, S.C.; Rothman, J.M.; et al. Adjuvant chemotherapy with or without bevacizumab in patients with resected non-small-cell lung cancer (E1505): An open-label, multicentre, randomised, phase 3 trial. Lancet Oncol. 2017, 18, 1610–1623. [Google Scholar] [CrossRef]
- Cremolini, C.; Loupakis, F.; Antoniotti, C.; Lupi, C.; Sensi, E.; Lonardi, S.; Mezi, S.; Tomasello, G.; Ronzoni, M.; Zaniboni, A.; et al. FOLFOXIRI plus bevacizumab versus FOLFIRI plus bevacizumab as first-line treatment of patients with metastatic colorectal cancer: Updated overall survival and molecular subgroup analyses of the open-label, phase 3 TRIBE study. Lancet Oncol. 2015, 16, 1306–1315. [Google Scholar] [CrossRef]
- Al-Salama, Z.T.; Syed, Y.Y.; Scott, L.J. Lenvatinib: A Review in Hepatocellular Carcinoma. Drugs 2019, 79, 665–674. [Google Scholar] [CrossRef] [PubMed]
- Keenan, T.E.; Tolaney, S.M. Role of Immunotherapy in Triple-Negative Breast Cancer. J. Natl. Compr. Cancer Netw. 2020, 18, 479–489. [Google Scholar] [CrossRef] [PubMed]
- Duma, N.; Santana-Davila, R.; Molina, J.R. Non-Small Cell Lung Cancer: Epidemiology, Screening, Diagnosis, and Treatment. Mayo Clin. Proc. 2019, 94, 1623–1640. [Google Scholar] [CrossRef]
- Liu, F.; Yang, X.; Geng, M.; Huang, M. Targeting ERK, an Achilles’ Heel of the MAPK pathway, in cancer therapy. Acta Pharm. Sin. B 2018, 8, 552–562. [Google Scholar] [CrossRef]
- Li, Z.; Zhou, W.; Zhang, Y.; Sun, W.; Yung, M.; Sun, J.; Li, J.; Chen, C.W.; Li, Z.; Meng, Y.; et al. ERK Regulates HIF1alpha-Mediated Platinum Resistance by Directly Targeting PHD2 in Ovarian Cancer. Clin. Cancer Res. 2019, 25, 5947–5960. [Google Scholar] [CrossRef]
- Kim, S.H.; Kim, M.O.; Cho, Y.Y.; Yao, K.; Kim, D.J.; Jeong, C.H.; Yu, D.H.; Bae, K.B.; Cho, E.J.; Jung, S.K.; et al. ERK1 phosphorylates Nanog to regulate protein stability and stem cell self-renewal. Stem Cell Res. 2014, 13, 1–11. [Google Scholar] [CrossRef]
- Yeh, E.; Cunningham, M.; Arnold, H.; Chasse, D.; Monteith, T.; Ivaldi, G.; Hahn, W.C.; Stukenberg, P.T.; Shenolikar, S.; Uchida, T.; et al. A signalling pathway controlling c-Myc degradation that impacts oncogenic transformation of human cells. Nat. Cell Biol. 2004, 6, 308–318. [Google Scholar] [CrossRef]
- Li, W.; Liu, Z.; Chen, W.; Jia, X.; Yin, C. PROZ is a Biomarker for Progression of Early Hepatocellular Carcinoma and Correlated with Tumor- Infiltrating Immune Cells. Clin. Surg. 2022, 7, 3433. [Google Scholar]
- Hossain, M.A.; Liu, G.; Dai, B.; Si, Y.; Yang, Q.; Wazir, J.; Birnbaumer, L.; Yang, Y. Reinvigorating exhausted CD8(+) cytotoxic T lymphocytes in the tumor microenvironment and current strategies in cancer immunotherapy. Med. Res. Rev. 2021, 41, 156–201. [Google Scholar] [CrossRef] [PubMed]
- Farhood, B.; Najafi, M.; Mortezaee, K. CD8(+) cytotoxic T lymphocytes in cancer immunotherapy: A review. J. Cell. Physiol. 2019, 234, 8509–8521. [Google Scholar] [CrossRef] [PubMed]
- Leone, P.; Solimando, A.G.; Fasano, R.; Argentiero, A.; Malerba, E.; Buonavoglia, A.; Lupo, L.G.; De Re, V.; Silvestris, N.; Racanelli, V. The Evolving Role of Immune Checkpoint Inhibitors in Hepatocellular Carcinoma Treatment. Vaccines 2021, 9, 532. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | PROZ Positive (n = 124) | p-Value | |
|---|---|---|---|
| Less | More | ||
| Age (yrs) | 0.067 | ||
| <50 | 53 | 7 | |
| ≥50 | 48 | 16 | |
| Gender | 0.208 | ||
| Male | 92 | 23 | |
| Female | 9 | 0 | |
| Tumor size | 0.020 | ||
| ≤5 cm | 51 | 18 | |
| >5 cm | 50 | 5 | |
| Vascular invasion | 0.241 | ||
| Positive | 22 | 2 | |
| Negative | 79 | 21 | |
| HBV infection | 0.392 | ||
| Positive | 94 | 20 | |
| Negative | 7 | 3 | |
| Liver cirrhosis | 1.000 | ||
| Negative | 16 | 4 | |
| Positive | 85 | 19 | |
| Tumor number | 1.000 | ||
| >1 | 26 | 6 | |
| =1 | 75 | 17 | |
| Pathologic stage | 0.087 | ||
| I + II | 90 | 17 | |
| III + IV | 11 | 6 | |
| TNM stage | 0.064 | ||
| 1 + 2 | 47 | 16 | |
| 3 + 4 | 54 | 7 | |
| Serum AFP | 0.786 | ||
| <400 ug/L | 52 | 16 | |
| ≥400 ug/L | 49 | 7 | |
| Variable | OS | PFS | ||
|---|---|---|---|---|
| Hazard Ratio (95% CI) | p-Value | Hazard Ratio (95% CI) | p-Value | |
| Tumor size (<5 cm vs. ≥5 cm) | 0.516 (0.225–1.182) | 0.117 | 0.576 (0.293–1.132) | 0.109 |
| Vascular invasion (Negative vs. Positive) | 0.500 (0.256–0.977) | 0.042 | 0.563 (0.306–1.037) | 0.065 |
| TNM stage (1 + 2 vs. 3 + 4) | 0.822 (0.329–2.055) | 0.676 | 0.707 (0.335–1.493) | 0.364 |
| PROZ expression (High vs. Low) | 0.342 (0.135–0.865) | 0.024 | 0.385 (0.197–0.754) | 0.005 |
| Characteristics | PROZ Positive | p-Value | ||
|---|---|---|---|---|
| Low | High | Total, n | ||
| Age (yrs) | 369 | 0.898 | ||
| <50 | 39 | 38 | ||
| ≥50 | 145 | 146 | ||
| Gender | 368 | 0.416 | ||
| Male | 128 | 120 | ||
| Female | 57 | 64 | ||
| Lymphocyte infiltration | 232 | 0.204 | ||
| Absent | 52 | 65 | ||
| Mild | 48 | 49 | ||
| Severe | 12 | 6 | ||
| Vascular invasion | 313 | 0.161 | ||
| None | 107 | 98 | ||
| Micro | 41 | 51 | ||
| Macro | 11 | 5 | ||
| Neoplasm grade | 364 | 0.383 | ||
| G1 + G2 | 112 | 120 | ||
| G3 + G4 | 70 | 62 | ||
| Pathologic stage | 345 | 0.232 | ||
| I + II | 132 | 123 | ||
| III + IV | 40 | 50 | ||
| AFP level (ng/mL) | 276 | 0.296 | ||
| <400 | 113 | 98 | ||
| ≥400 | 30 | 35 | ||
| Child-Pugh classification grade | 237 | 0.610 | ||
| A | 110 | 105 | ||
| B + C | 10 | 12 | ||
| Liver fibrosis Ishak score | 210 | 0.643 | ||
| ≤4 | 62 | 69 | ||
| >4 | 40 | 39 | ||
| Relapse | 267 | 0.437 | ||
| Yes | 44 | 49 | ||
| No | 91 | 83 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, Y.; Qiu, X.; Wu, D.; Lu, X.; Li, G.; Tang, Y.; Jia, C.; Xiong, Z.; Wang, T. PROZ Associated with Sorafenib Sensitivity May Serve as a Potential Target to Enhance the Efficacy of Combined Immunotherapy for Hepatocellular Carcinoma. Genes 2022, 13, 1535. https://doi.org/10.3390/genes13091535
Chen Y, Qiu X, Wu D, Lu X, Li G, Tang Y, Jia C, Xiong Z, Wang T. PROZ Associated with Sorafenib Sensitivity May Serve as a Potential Target to Enhance the Efficacy of Combined Immunotherapy for Hepatocellular Carcinoma. Genes. 2022; 13(9):1535. https://doi.org/10.3390/genes13091535
Chicago/Turabian StyleChen, Yinkui, Xiusheng Qiu, Donghao Wu, Xu Lu, Guanghui Li, Yongsheng Tang, Changchang Jia, Zhiyong Xiong, and Tiantian Wang. 2022. "PROZ Associated with Sorafenib Sensitivity May Serve as a Potential Target to Enhance the Efficacy of Combined Immunotherapy for Hepatocellular Carcinoma" Genes 13, no. 9: 1535. https://doi.org/10.3390/genes13091535
APA StyleChen, Y., Qiu, X., Wu, D., Lu, X., Li, G., Tang, Y., Jia, C., Xiong, Z., & Wang, T. (2022). PROZ Associated with Sorafenib Sensitivity May Serve as a Potential Target to Enhance the Efficacy of Combined Immunotherapy for Hepatocellular Carcinoma. Genes, 13(9), 1535. https://doi.org/10.3390/genes13091535