
New Genetic Variants in CYP2B6 and SLC6A Support the Role of Oxidative Stress in Familial Ménière’s Disease

 ,
,
Abstract
:
1. Introduction
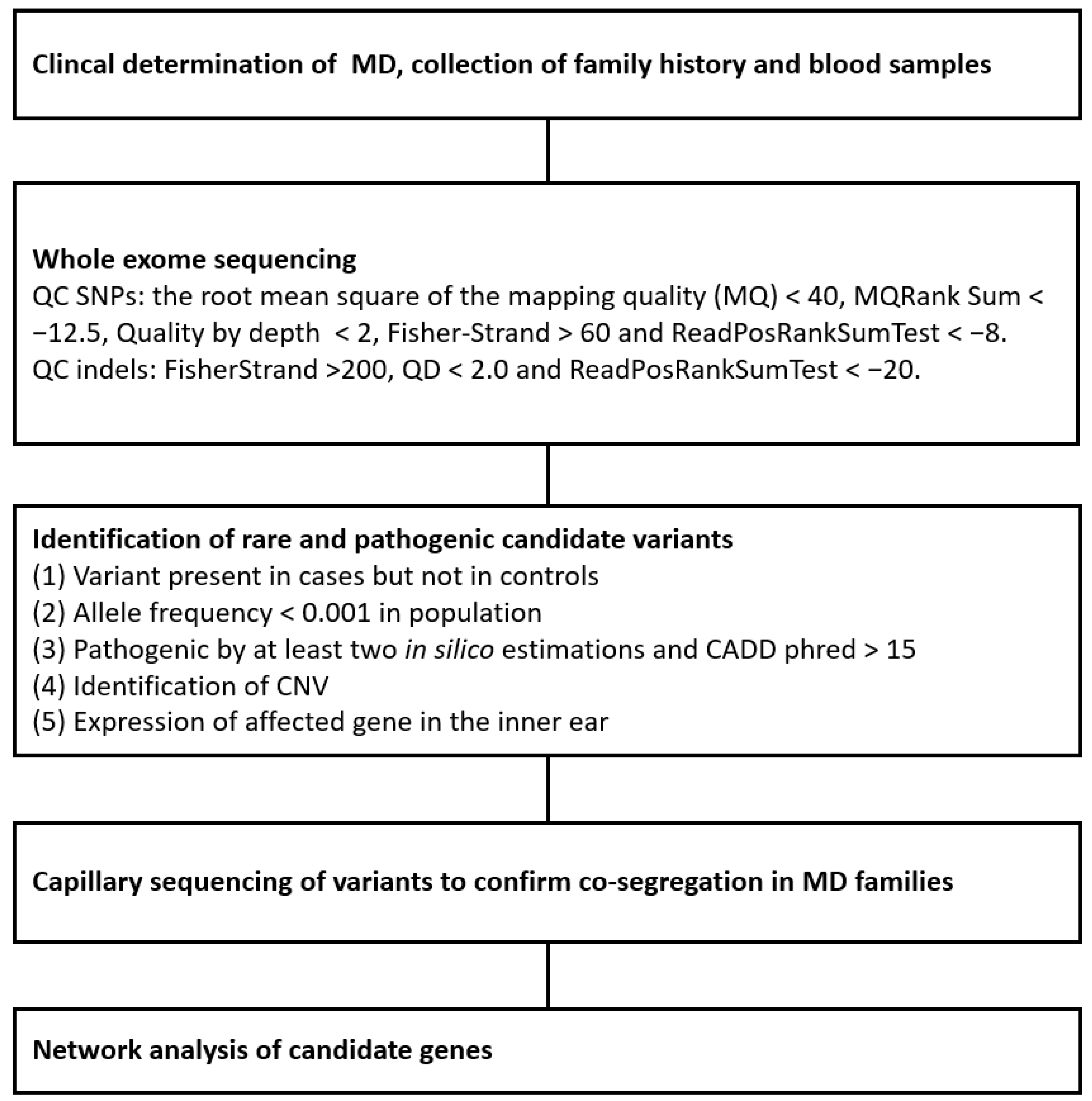
2. Materials and Methods
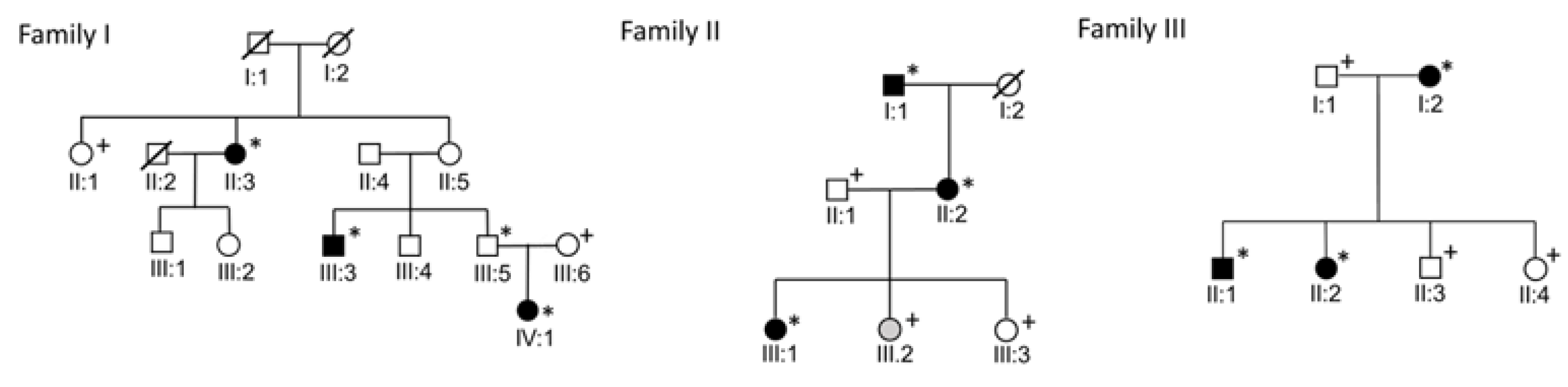
2.1. Families
2.2. Whole Exome Sequencing
2.3. Whole Exome Data Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Yamakawa, K. ber die Pathologische Veränderung bei einem Meniere-Kranken. J. Otolaryngol. Jpn. 1938, 44, 23102312. [Google Scholar]
- Hallpike, C.S.; Cairns, H. Observations on the Pathology of Meniere’s Syndrome: (Section of Otology). Proc. R. Soc. Med. 1938, 31, 1317–1336. [Google Scholar] [PubMed]
- Merchant, S.N.; Adams, J.C.; Nadol, J.B., Jr. Pathophysiology of Meniere’s syndrome: Are symptoms caused by endolymphatic hydrops? Otol. Neurotol. 2005, 26, 74–81. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alexander, T.H.; Harris, J.P. Current epidemiology of Meniere’s syndrome. Otolaryngol. Clin. North Am. 2010, 43, 965–970. [Google Scholar] [CrossRef] [PubMed]
- Ohmen, J.D.; White, C.H.; Li, X.; Wang, J.; Fisher, L.M.; Zhang, H.; Derebery, M.J.; Friedman, R.A. Genetic evidence for an ethnic diversity in the susceptibility to Meniere’s disease. Otol. Neurotol. 2013, 34, 1336–1341. [Google Scholar] [CrossRef]
- Hietikko, E.; Kotimäki, J.; Sorri, M.; Männikkö, M. High incidence of Meniere-like symptoms in relatives of Meniere patients in the areas of Oulu University Hospital and Kainuu Central Hospital in Finland. Eur. J. Med. Genet. 2013, 56, 279–285. [Google Scholar] [CrossRef]
- Gallego-Martinez, A.; Requena, T.; Roman-Naranjo, P.; Lopez-Escamez, J.A. Excess of Rare Missense Variants in Hearing Loss Genes in Sporadic Meniere Disease. Front. Genet. 2019, 10, 76. [Google Scholar] [CrossRef]
- Klar, J.; Frykholm, C.; Friberg, U.; Dahl, N. A Meniere’s disease gene linked to chromosome 12p12.3. Am. J. Med. Genet. B Neuropsychiatr. Genet. 2006, 141, 463–467. [Google Scholar] [CrossRef]
- Hietikko, E.; Kotimäki, J.; Kentala, E.; Klockars, T.; Sorri, M.; Männikkö, M. Finnish familial Meniere disease is not linked to chromosome 12p12.3, and anticipation and cosegregation with migraine are not common findings. Genet. Med. 2011, 13, 415–420. [Google Scholar] [CrossRef] [Green Version]
- Martín-Sierra, C.; Gallego-Martinez, A.; Requena, T.; Frejo, L.; Batuecas-Caletrío, A.; Lopez-Escamez, J.A. Variable expressivity and genetic heterogeneity involving DPT and SEMA3D genes in autosomal dominant familial Meniere’s disease. Eur. J. Hum. Genet. 2017, 25, 200–207. [Google Scholar] [CrossRef]
- Martín-Sierra, C.; Requena, T.; Frejo, L.; Price, S.D.; Gallego-Martinez, A.; Batuecas-Caletrio, A.; Santos-Pérez, S.; Soto-Varela, A.; Lysakowski, A.; Lopez-Escamez, J.A. A novel missense variant in PRKCB segregates low-frequency hearing loss in an autosomal dominant family with Meniere’s disease. Hum. Mol. Genet. 2016, 25, 3407–3415. [Google Scholar] [CrossRef] [Green Version]
- Requena, T.; Cabrera, S.; Martín-Sierra, C.; Price, S.D.; Lysakowski, A.; Lopez-Escamez, J.A. Identification of two novel mutations in FAM136A and DTNA genes in autosomal-dominant familial Meniere’s disease. Hum. Mol. Genet. 2015, 24, 1119–1126. [Google Scholar] [CrossRef] [PubMed]
- Skarp, S.; Kanervo, L.; Kotimäki, J.; Sorri, M.; Männikkö, M.; Hietikko, E. Whole-exome sequencing suggests multiallelic inheritance for childhood-onset Meniere’s disease. Ann. Hum. Genet. 2019, 83, 389–396. [Google Scholar] [CrossRef] [PubMed]
- Oh, E.H.; Shin, J.H.; Kim, H.S.; Cho, J.W.; Choi, S.Y.; Choi, K.D.; Rhee, J.K.; Lee, S.; Lee, C.; Choi, J.H. Rare Variants of Putative Candidate Genes Associated With Sporadic Meniere’s Disease in East Asian Population. Front. Neurol. 2019, 10, 1424. [Google Scholar] [CrossRef] [PubMed]
- Gallego-Martinez, A.; Requena, T.; Roman-Naranjo, P.; May, P.; Lopez-Escamez, J.A. Enrichment of damaging missense variants in genes related with axonal guidance signalling in sporadic Meniere’s disease. J. Med. Genet. 2020, 57, 82–88. [Google Scholar] [CrossRef]
- Roman-Naranjo, P.; Gallego-Martinez, A.; Soto-Varela, A.; Aran, I.; del Carmen Moleon, M.; Espinosa-Sanchez, J.M.; Amor-Dorado, J.C.; Batuecas-Caletrio, A.; Perez-Vazquez, P.; Lopez-Escamez, J.A. Burden of Rare Variants in the OTOG Gene in Familial Meniere’s Disease. Ear Hear. 2020, 41, 1598–1605. [Google Scholar] [CrossRef]
- Skuladottir, A.T.; Bjornsdottir, G.; Nawaz, M.S.; Petersen, H.; Rognvaldsson, S.; Moore, K.H.; Olafsson, P.I.; Magnusson, S.H.; Bjornsdottir, A.; Sveinsson, O.A.; et al. A genome-wide meta-analysis uncovers six sequence variants conferring risk of vertigo. Commun. Biol. 2021, 4, 1148. [Google Scholar] [CrossRef]
- Committee on Hearing and Equilibrium guidelines for the diagnosis and evaluation of therapy in Meniere’s disease. American Academy of Otolaryngology-Head and Neck Foundation, Inc. Otolaryngol. Head Neck Surg. 1995, 113, 181–185. [CrossRef]
- Quinlan, A.R.; Hall, I.M. BEDTools: A flexible suite of utilities for comparing genomic features. Bioinformatics 2010, 26, 841–842. [Google Scholar] [CrossRef] [Green Version]
- Yang, H.; Wang, K. Genomic variant annotation and prioritization with ANNOVAR and wANNOVAR. Nat. Protoc. 2015, 10, 1556–1566. [Google Scholar] [CrossRef]
- Kircher, M.; Witten, D.M.; Jain, P.; O’roak, B.J.; Cooper, G.M.; Shendure, J. A general framework for estimating the relative pathogenicity of human genetic variants. Nat. Genet. 2014, 46, 310–315. [Google Scholar] [CrossRef] [PubMed] [Green Version]
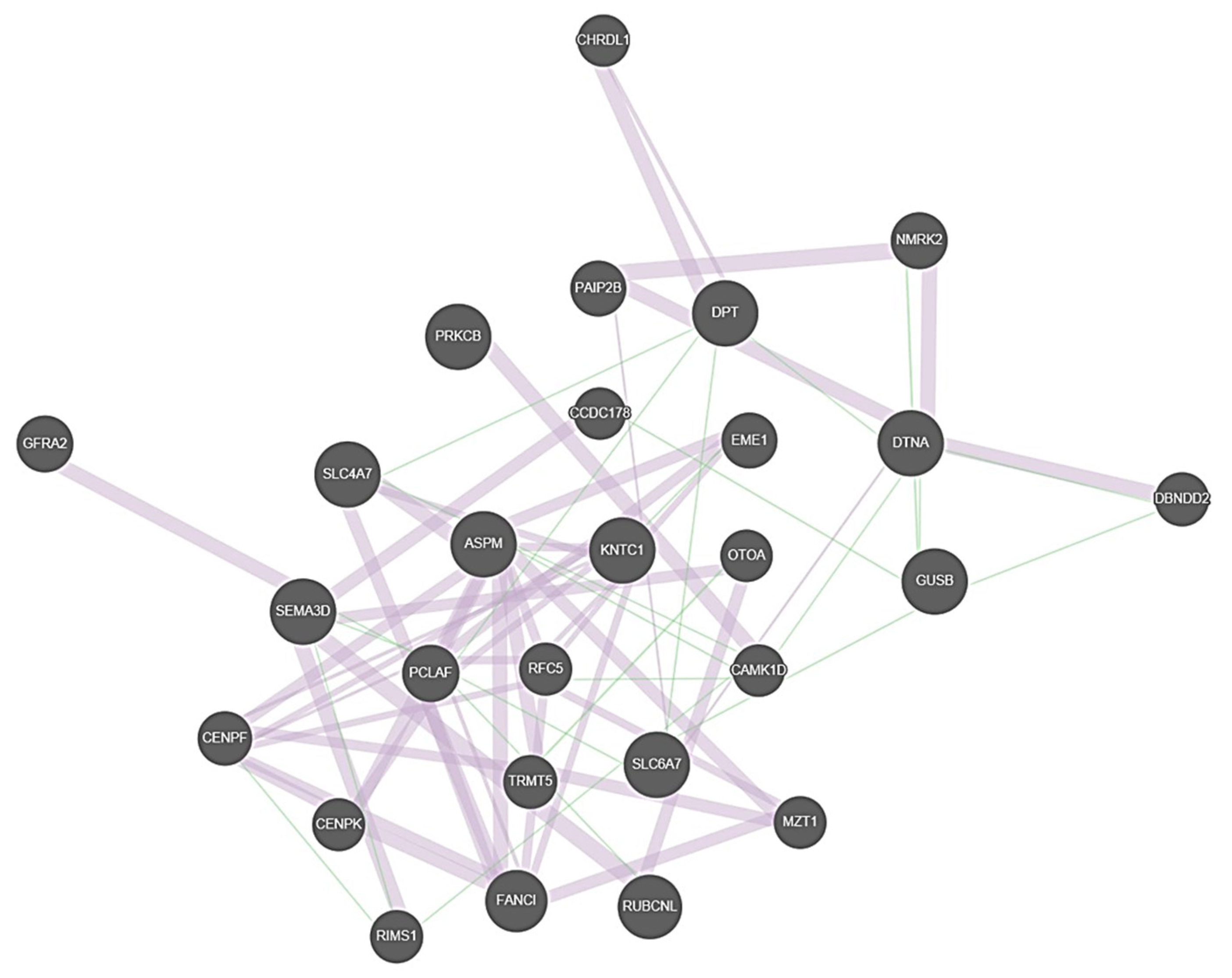
- Warde-Farley, D.; Donaldson, S.L.; Comes, O.; Zuberi, K.; Badrawi, R.; Chao, P.; Franz, M.; Grouios, C.; Kazi, F.; Lopes, C.T.; et al. The GeneMANIA prediction server: Biological network integration for gene prioritization and predicting gene function. Nucleic Acids Res. 2010, 38, W214–W220. [Google Scholar] [CrossRef] [PubMed]
- Klambauer, G.; Schwarzbauer, K.; Mayr, A.; Clevert, D.A.; Mitterecker, A.; Bodenhofer, U.; Hochreiter, S. cn.MOPS: Mixture of Poissons for discovering copy number variations in next-generation sequencing data with a low false discovery rate. Nucleic Acids Res. 2012, 40, e69. [Google Scholar] [CrossRef] [PubMed]
- MacDonald, J.R.; Ziman, R.; Yuen, R.K.; Feuk, L.; Scherer, S.W. The Database of Genomic Variants: A curated collection of structural variation in the human genome. Nucleic Acids Res. 2014, 42, D986–D992. [Google Scholar] [CrossRef] [Green Version]
- Nebert, D.W.; Wikvall, K.; Miller, W.L. Human cytochromes P450 in health and disease. Philos. Trans. R. Soc. B Biol. Sci. 2013, 368, 20120431. [Google Scholar] [CrossRef]
- Lee, Y.; Choi, J.H.; Oh, A.; Kim, G.H.; Park, S.H.; Moon, J.E.; Ko, C.W.; Cheon, C.K.; Yoo, H.W. Clinical, endocrinological, and molecular features of four Korean cases of cytochrome P450 oxidoreductase deficiency. Ann. Pediatr. Endocrinol. Metab. 2020, 25, 97–103. [Google Scholar] [CrossRef]
- Manche, S.K.; Jangala, M.; Putta, P.; Koralla, R.M.; Akka, J. Association of oxidative stress gene polymorphisms with presbycusis. Gene 2016, 593, 277–283. [Google Scholar] [CrossRef]
- Shi, X.; Nuttall, A.L. Upregulated iNOS and oxidative damage to the cochlear stria vascularis due to noise stress. Brain Res. 2003, 967, 1–10. [Google Scholar] [CrossRef]
- Benkafadar, N.; François, F.; Affortit, C.; Casas, F.; Ceccato, J.C.; Menardo, J.; Venail, F.; Malfroy-Camine, B.; Puel, J.L.; Wang, J. ROS-Induced Activation of DNA Damage Responses Drives Senescence-Like State in Postmitotic Cochlear Cells: Implication for Hearing Preservation. Mol. Neurobiol. 2019, 56, 5950–5969. [Google Scholar] [CrossRef] [Green Version]
- Wolfberg, J.; Chintalapati, K.; Tomatsu, S.; Nagao, K. Hearing Loss in Mucopolysaccharidoses: Current Knowledge and Future Directions. Diagnostics 2020, 10, 554. [Google Scholar] [CrossRef]
- Ohlemiller, K.K.; Hennig, A.K.; Lett, J.M.; Heidbreder, A.F.; Sands, M.S. Inner ear pathology in the mucopolysaccharidosis VII mouse. Hear. Res. 2002, 169, 69–84. [Google Scholar] [CrossRef]
- Broer, S.; Gether, U. The solute carrier 6 family of transporters. Br. J. Pharmacol. 2012, 167, 256–278. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brownstein, Z.N.; Dror, A.A.; Gilony, D.; Migirov, L.; Hirschberg, K.; Avraham, K.B. A novel SLC26A4 (PDS) deafness mutation retained in the endoplasmic reticulum. Arch. Otolaryngol. Head Neck Surg. 2008, 134, 403–407. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sun, S.; Zhang, D.; Sun, G.; Song, Y.; Cai, J.; Fan, Z.; Wang, H. Solute carrier family 4 member 1 might participate in the pathogenesis of Meniere’s disease in a murine endolymphatic hydrop model. Acta Oto-Laryngol. 2019, 139, 966–976. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Zeng, X.; Zhang, X.; Liu, H.; Xing, H. Ammonia exposure induces oxidative stress and inflammation by destroying the microtubule structures and the balance of solute carriers in the trachea of pigs. Ecotoxicol. Environ. Saf. 2021, 212, 111974. [Google Scholar] [CrossRef]
- Khan, N.M.; Hussain, B.; Zheng, C.; Khan, A.; Masoud, M.S.; Gu, Q.; Qiu, L.; Malik, N.A.; Qasim, M.; Tariq, M.; et al. Updates on Clinical and Genetic Heterogeneity of ASPM in 12 Autosomal Recessive Primary Microcephaly Families in Pakistani Population. Front. Pediatr. 2021, 9, 695133. [Google Scholar] [CrossRef]
- Colantonio, J.R.; Vermot, J.; Wu, D.; Langenbacher, A.D.; Fraser, S.; Chen, J.N.; Hill, K.L. The dynein regulatory complex is required for ciliary motility and otolith biogenesis in the inner ear. Nature 2009, 457, 205–209. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Family | Gene | Variant | rsID | Type | gnomAD Finn | gnomAD Total |
|---|---|---|---|---|---|---|
| I | CYP2B6 | c.200C>T; p.T67M | rs138264188 | Missense | 0.0001194 | 0.001253 |
| II | GUSB | c.323C>T; p.P108L | rs1268678201 | Missense | 0.0001995 | 0.00003199 |
| II | EPB42 | c.1089G>A; p.W363X | rs201351228 | Nonsense | 0.0009161 | 0.00008134 |
| III | OVCH1 | c.1316T>A; p.L439X | rs775251987 | Nonsense | 0.0006504 | 0.00008044 |
| III | KNTC1 | c.5242A>C; p.T1748P | rs1272541364 | Missense | 0.0001872 | 0.00001635 |
| III | ASPM | c.5207A>G; p.Q1736R | NA | Missense | NA | NA |
| III | SLC6A7 | c.322G>C; p.V108L | rs775035174 | Missense | 0.001314 | 0.0001238 |
| Family I | II:1 | II:3 M | III:3 M | III:5 C | III:6 | IV:1 M |
|---|---|---|---|---|---|---|
| CYP2B6 c.200C>T | C/C | C/T | C/T | C/T | C/C | C/T |
| Family II | I:1 M | II:1 | II:2 M | III:1 M | III:2 P | III:3 |
| GUSB c.323C>T | C/T | C/C | C/T | C/T | C/T | C/C |
| SLC8A2 c.1792G>T | G/T | G/G | G/T | G/T | NA | G/T |
| OTOA c.1387G>T | G/T | G/T | G/T | G/T | NA | G/T |
| FLJ44635 c. 244C>A | A/A | C/C | C/A | C/A | C/A | C/A |
| PNPLA2 c. 493G>A | G/A | G/G | G/A | G/A | G/A | G/A |
| SEC24C c.665G>A | G/A | G/G | G/A | G/A | G/G | G/A |
| EPB42 c.1089G>A | A/A | G/G | G/A | G/A | G/A | G/G |
| AR c.2395C>G | G/G | C/C | G/C | G/C | G/C | G/C |
| Family III | I:1 | I:2 M | II:1 M | II:2 M | II:3 | II:4 |
| OVCH1 c.1316T>A | T/T | T/A | T/A | T/A | T/T | T/T |
| KNTC1 c.5242A>C | A/A | A/C | A/C | A/C | A/A | A/A |
| RYR2 c.2807C>T | C/C | C/T | C/T | C/T | C/T | C/T |
| ASPM c.5207A>G | A/A | A/G | A/G | A/G | A/A | A/A |
| SLC6A7 c.322G>C | G/G | G/C | G/C | G/C | G/G | G/G |
| ATR c.6967A>C | C/C | A/C | A/C | A/C | A/C | C/C |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Skarp, S.; Korvala, J.; Kotimäki, J.; Sorri, M.; Männikkö, M.; Hietikko, E. New Genetic Variants in CYP2B6 and SLC6A Support the Role of Oxidative Stress in Familial Ménière’s Disease. Genes 2022, 13, 998. https://doi.org/10.3390/genes13060998
Skarp S, Korvala J, Kotimäki J, Sorri M, Männikkö M, Hietikko E. New Genetic Variants in CYP2B6 and SLC6A Support the Role of Oxidative Stress in Familial Ménière’s Disease. Genes. 2022; 13(6):998. https://doi.org/10.3390/genes13060998
Chicago/Turabian StyleSkarp, Sini, Johanna Korvala, Jouko Kotimäki, Martti Sorri, Minna Männikkö, and Elina Hietikko. 2022. "New Genetic Variants in CYP2B6 and SLC6A Support the Role of Oxidative Stress in Familial Ménière’s Disease" Genes 13, no. 6: 998. https://doi.org/10.3390/genes13060998
APA StyleSkarp, S., Korvala, J., Kotimäki, J., Sorri, M., Männikkö, M., & Hietikko, E. (2022). New Genetic Variants in CYP2B6 and SLC6A Support the Role of Oxidative Stress in Familial Ménière’s Disease. Genes, 13(6), 998. https://doi.org/10.3390/genes13060998