
Identification of New Genetic Determinants in Pediatric Patients with Familial Hypercholesterolemia Using a Custom NGS Panel

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
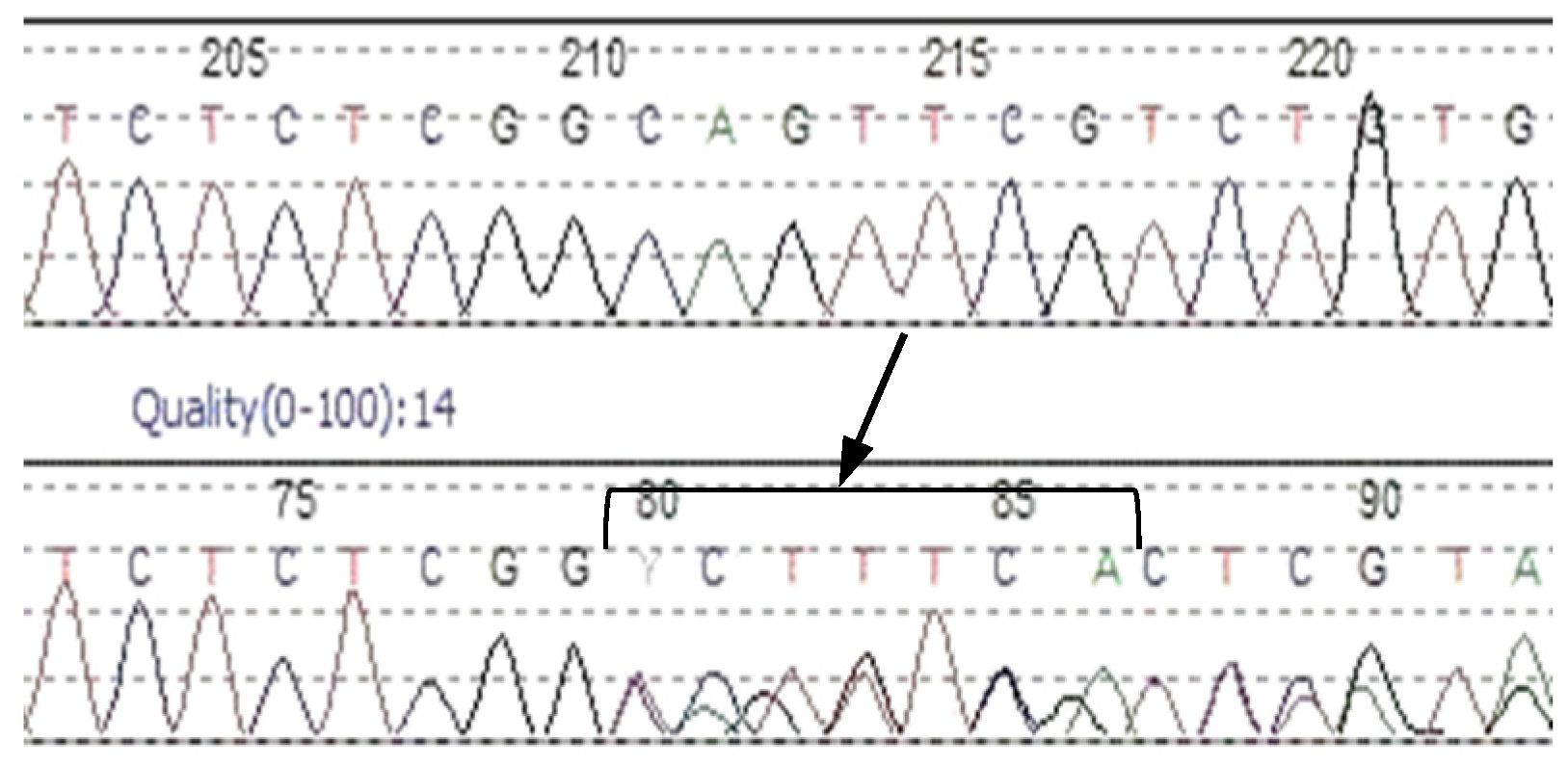
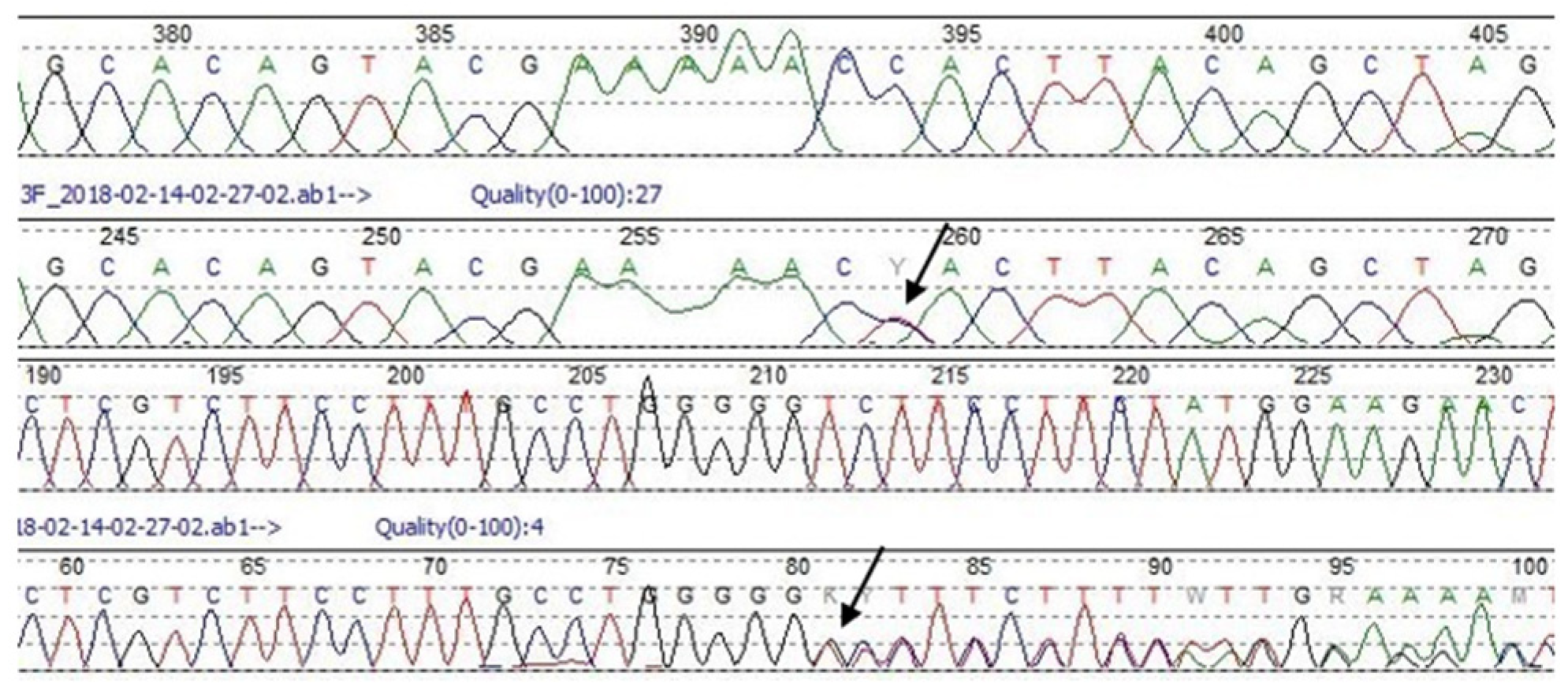
3.1. LDLR Gene
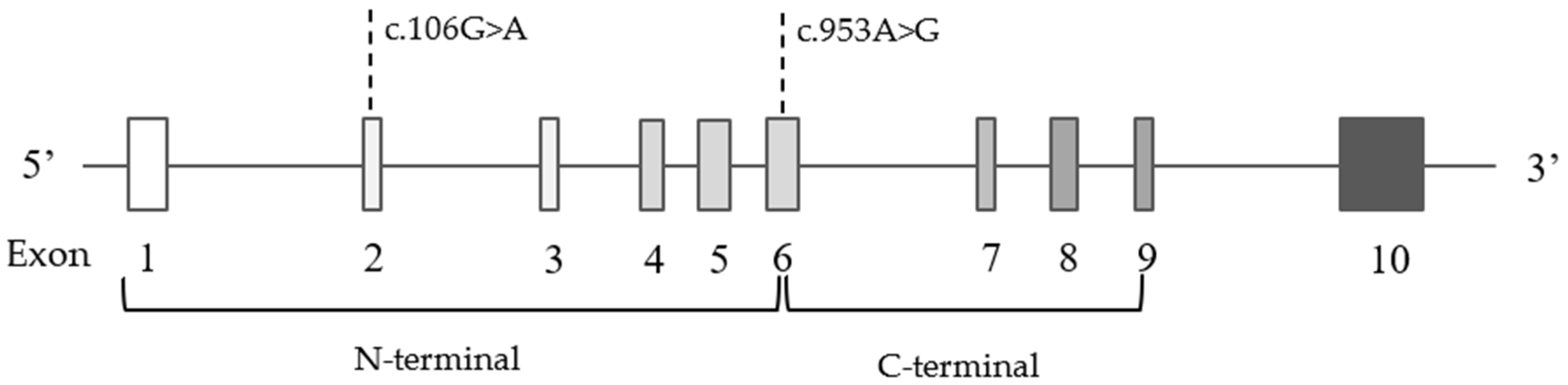
3.2. Other Affected Genes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Ruan, Y.; Guo, Y.; Zheng, Y.; Huang, Z.; Sun, S.; Kowal, P.; Shi, Y.; Wu, F. Cardiovascular disease (CVD) and associated risk factors among older adults in six low-and middle-income countries: Results from SAGE Wave 1. BMC Public Health 2018, 18, 778. [Google Scholar] [CrossRef] [Green Version]
- Stewart, J.; McCallin, T.; Martinez, J.; Chacko, S.; Yusuf, S. Hyperlipidemia. Pediatr. Rev. 2020, 41, 393–402. [Google Scholar] [CrossRef] [PubMed]
- Tada, H.; Takamura, M.; Kawashiri, M.-A. Familial hypercholesterolemia: A narrative review on diagnosis and management strategies for children and adolescents. Vasc. Health Risk Manag. 2021, 17, 59–67. [Google Scholar] [CrossRef] [PubMed]
- Wiegman, A.; Gidding, S.S.; Watts, G.F.; Chapman, M.J.; Ginsberg, H.N.; Cuchel, M.; Ose, L.; Averna, M.; Boileau, C.; Borén, J.; et al. Familial hypercholesterolaemia in children and adolescents: Gaining decades of life by optimizing detection and treatment. Eur. Heart J. 2015, 36, 2425–2437. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reijman, M.D.; Kusters, D.M.; Wiegman, A. Advances in familial hypercholesterolaemia in children. Lancet Child Adolesc. Health 2021, 5, 652–661. [Google Scholar] [CrossRef]
- Sharifi, M.; Futema, M.; Nair, D.; Humphries, S.E. Genetic Architecture of Familial Hypercholesterolaemia. Curr. Cardiol. Rep. 2017, 19, 44. [Google Scholar] [CrossRef]
- Xia, X.-D.; Peng, Z.-S.; Gu, H.-M.; Wang, M.; Wang, G.-Q.; Zhang, D.-W. Regulation of PCSK9 Expression and Function: Mechanisms and Therapeutic Implications. Front. Cardiovasc. Med. 2021, 8, 1325. [Google Scholar] [CrossRef]
- Defesche, J.C. Low-Density Lipoprotein Receptor-Its Structure, Function, and Mutations. Semin. Vasc. Med. 2004, 4, 5–11. [Google Scholar] [CrossRef]
- Lagace, T.A. PCSK9 and LDLR degradation: Regulatory mechanisms in circulation and in cells. Curr. Opin. Lipidol. 2014, 25, 387–393. [Google Scholar] [CrossRef]
- Danyel, M.; Ott, C.-E.; Grenkowitz, T.; Salewsky, B.; Hicks, A.A.; Fuchsberger, C.; Steinhagen-Thiessen, E.; Bobbert, T.; Kassner, U.; DeMuth, I. Evaluation of the role of STAP1 in Familial Hypercholesterolemia. Sci. Rep. 2019, 9, 11995. [Google Scholar] [CrossRef] [Green Version]
- Hegele, R.A.; Knowles, J.W.; Horton, J.D. Delisting STAP1: The rise and fall of a putative hypercholesterolemia gene. Arter. Thromb. Vasc. Biol. 2020, 40, 847–849. [Google Scholar] [CrossRef]
- Shaik, N.A.; Al-Qahtani, F.; Nasser, K.; Jamil, K.; Alrayes, N.; Elango, R.; Awan, Z.; Banaganapalli, B. Molecular insights into the coding region mutations of low-density lipoprotein receptor adaptor protein 1 (LDLRAP1) linked to familial hypercholesterolemia. J. Gene Med. 2020, 22, e3176. [Google Scholar] [CrossRef] [PubMed]
- Beigneux, A.P.; Miyashita, K.; Ploug, M.; Blom, D.J.; Ai, M.; Linton, M.F.; Khovidhunkit, W.; Dufour, R.; Garg, A.; McMahon, M.A.; et al. Autoantibodies against GPIHBP1 as a Cause of Hypertriglyceridemia. N. Engl. J. Med. 2017, 376, 1647–1658. [Google Scholar] [CrossRef] [PubMed]
- Sharifi, M.; Walus-Miarka, M.; Idzior-Waluś, B.; Malecki, M.T.; Sanak, M.; Whittall, R.; Li, K.W.; Futema, M.; Humphries, S.E. The genetic spectrum of familial hypercholesterolemia in south-eastern Poland. Metabolism 2015, 65, 48–53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cohen, H.; Stefanutti, C. Current Approach to the Diagnosis and Treatment of Heterozygote and Homozygous FH Children and Adolescents. Curr. Atheroscler. Rep. 2021, 23, 30. [Google Scholar] [CrossRef]
- Richards, S.; Aziz, N.; Bale, S.; Bick, D.; Das, S.; Gastier-Foster, J.; Grody, W.W.; Hegde, M.; Lyon, E.; Spector, E.; et al. Standards and guidelines for the interpretation of sequence variants: A joint consensus recommendation of the American College of Medical Genetics and Genomics and the Association for Molecular Pathology. Genet. Med. 2015, 17, 405–423. [Google Scholar] [CrossRef] [Green Version]
- Chmara, M.; Wasąg, B.; Żuk, M.; Kubalska, J.; Węgrzyn, A.; Bednarska-Makaruk, M.; Pronicka, E.; Wehr, H.; Defesche, J.C.; Rynkiewicz, A.; et al. Molecular characterization of Polish patients with familial hypercholesterolemia: Novel and recurrentLDLR mutations. J. Appl. Genet. 2010, 51, 95–106. [Google Scholar] [CrossRef]
- Varret, M.; Rabès, J.-P. Missense Mutation in the LDLR Gene: A Wide Spectrum in the Severity of Familial Hypercholesterolemia. In Mutations in Human Genetic Disease; IntechOpen: London, UK, 2012. [Google Scholar] [CrossRef] [Green Version]
- Garg, A. Dyslipidemias: Pathophysiology, Evaluation and Management; Humana Press Inc.: Totowa, NJ, USA, 2015. [Google Scholar]
- Chmara, M. Mutacje Genów LDLR i APOB w Hipercholesterolemii Rodzinnej. Ph.D. Thesis, Medical University of Gdańsk, Gdańsk, Poland, 2005. [Google Scholar]
- Fernández-Higuero, J.A.; Etxebarria, A.; Benito-Vicente, A.; Alves, A.C.; Arrondo, J.L.R.; Ostolaza, H.; Bourbon, M.; Martin, C. Structural analysis of APOB variants, p.(Arg3527Gln), p.(Arg1164Thr) and p.(Gln4494del), causing Familial Hypercholesterolaemia provides novel insights into variant pathogenicity. Sci. Rep. 2015, 5, 18184. [Google Scholar] [CrossRef] [Green Version]
- Wright, W.T.; Young, I.S.; Nicholls, D.P.; Graham, C.A. Genetic screening of the LPL gene in hypertriglyceridaemic patients. Atherosclerosis 2008, 199, 187–192. [Google Scholar] [CrossRef]
- Merkel, M.; Eckel, R.H.; Goldberg, I.J. Lipoprotein lipase: Genetics, lipid uptake, and regulation. J. Lipid Res. 2002, 43, 1997–2006. [Google Scholar] [CrossRef] [Green Version]
- Surendran, R.P.; Visser, M.E.; Heemelaar, S.; Wang, J.; Peter, J.; Defesche, J.C.; Kuivenhoven, J.A.; Hosseini, M.; Péterfy, M.; Kastelein, J.J.P.; et al. Mutations in LPL, APOC2, APOA5, GPIHBP1 and LMF1 in patients with severe hypertriglyceridaemia. J. Intern. Med. 2012, 272, 185–196. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Daniels, S.R.; Gidding, S.; de Ferranti, S.D. Pediatric aspects of Familial Hypercholesterolemias: Recommendations from the National Lipid Association Expert Panel on Familial Hypercholesterolemia. J. Clin. Lipidol. 2011, 5, S30–S37. [Google Scholar] [CrossRef] [PubMed]
- Groselj, U.; Kovac, J.; Sustar, U.; Mlinaric, M.; Fras, Z.; Podkrajsek, K.T.; Battelino, T. Universal screening for familial hypercholesterolemia in children: The Slovenian model and literature review. Atherosclerosis 2018, 277, 383–391. [Google Scholar] [CrossRef] [PubMed]
- Gabcova-Balaziova, D.; Stanikova, D.; Vohnout, B.; Huckova, M.; Stanik, J.; Klimes, I.; Raslova, K.; Gasperikova, D. Molecular-genetic aspects of familial hypercholesterolemia. Endocr. Regul. 2015, 49, 164–181. [Google Scholar] [CrossRef]
- Südhof, T.C.; Goldstein, J.L.; Brown, M.S.; Russell, D.W. The LDL receptor gene: A mosaic of exons shared with different proteins. Science 1985, 228, 815–822. [Google Scholar] [CrossRef] [Green Version]
- Wong, K.H.; Levy-Sakin, M.; Ma, W.; Gonzaludo, N.; Mak, A.C.; Vaka, D.; Poon, A.; Chu, C.; Lao, R.; Balamir, M.; et al. Three patients with homozygous familial hypercholesterolemia: Genomic sequencing and kindred analysis. Mol. Genet. Genom. Med. 2019, 7, e1007. [Google Scholar] [CrossRef]
- Romano, M.; Di Taranto, M.D.; D’Agostino, M.N.; Marotta, G.; Gentile, M.; Abate, G.; Mirabelli, P.; Di Noto, R.; Del Vecchio, L.; Rubba, P.; et al. Identification and functional characterization of LDLR mutations in familial hypercholesterolemia patients from Southern Italy. Atherosclerosis 2010, 210, 493–496. [Google Scholar] [CrossRef]
- Hobbs, H.H.; Brown, M.S.; Goldstein, J.L. Molecular genetics of the LDL receptor gene in familial hypercholesterolemia. Hum. Mutat. 1992, 1, 445–466. [Google Scholar] [CrossRef]
- Kubalska, J.; Chmara, M.; Limon, J.; Wierzbicka-Rucinska, A.; Prokurat, S.; Szaplyko, J.; Kowalik, A.; Mierzewska, H.; Defesche, J.C.; Pronicka, E. Clinical course of homozygous familial hypercholesterolemia during childhood: Report on 4 unrelated patients with homozygous or compound heterozygous mutations in theLDLR gene. J. Appl. Genet. 2008, 49, 109–113. [Google Scholar] [CrossRef]
- Miltiadous, G.; Elisaf, M.; Bairaktari, H.; Xenophontos, S.L.; Manoli, P.; Cariolou, M.A. Characterization and geographic distribution of the low density lipoprotein receptor (LDLR) gene mutations in northwestern Greece. Hum. Mutat. 2001, 17, 432–433. [Google Scholar] [CrossRef]
- Susan-Resiga, D.; Girard, E.; Kiss, R.S.; Essalmani, R.; Hamelin, J.; Asselin, M.-C.; Awan, Z.; Butkinaree, C.; Fleury, A.; Soldera, A.; et al. The proprotein convertase subtilisin/kexin type 9-resistant R410S low density lipoprotein receptor mutation: A novel mechanism causing familial hypercholesterolemia. J. Biol. Chem. 2017, 292, 1573–1590. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benito-Vicente, A.; Uribe, K.B.; Jebari, S.; Galicia-Garcia, U.; Ostolaza, H.; Martin, C. Validation of LDLr Activity as a Tool to Improve Genetic Diagnosis of Familial Hypercholesterolemia: A Retrospective on Functional Characterization of LDLr Variants. Int. J. Mol. Sci. 2018, 19, 1676. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krawczak, M.; Cooper, D.N. Gene deletions causing human genetic disease: Mechanisms of mutagenesis and the role of the local DNA sequence environment. Qual. Life Res. 1991, 86, 425–441. [Google Scholar] [CrossRef] [PubMed]
- Ball, E.V.; Stenson, P.D.; Abeysinghe, S.S.; Krawczak, M.; Cooper, D.N.; Chuzhanova, N.A. Microdeletions and microinsertions causing human genetic disease: Common mechanisms of mutagenesis and the role of local DNA sequence complexity. Hum. Mutat. 2005, 26, 205–213. [Google Scholar] [CrossRef]
- Hattori, H.; Hirayama, T.; Nobe, Y.; Nagano, M.; Kujiraoka, T.; Egashira, T.; Ishii, J.; Tsuji, M.; Emi, M. Eight novel mutations and functional impairments of the LDL receptor in familial hypercholesterolemia in the north of Japan. J. Hum. Genet. 2002, 47, 80–87. [Google Scholar] [CrossRef] [Green Version]
- Fairoozy, R.H. Genetic Functional Studies of Low Density Lipoprotein-Cholesterol (LDL-C) Associated Variants and the Genetic Spectrum of Familial Hypercholesterolemia in Different Ethnic Groups. 2018. Available online: https://ethos.bl.uk/OrderDetails.do?did=1&uin=uk.bl.ethos.747249 (accessed on 9 May 2022).
- Müllertz, K.M.; Christiansen, M.K.; Broendberg, A.K.; Pedersen, L.N.; Jensen, H.K. Outcome of clinical management in relatives of sudden cardiac death victims. Int. J. Cardiol. 2018, 262, 45–50. [Google Scholar] [CrossRef]
- Bamimore, M.A.; Zaid, A.; Banerjee, Y.; Al-Sarraf, A.; Abifadel, M.; Seidah, N.G.; Al-Waili, K.; Al-Rasadi, K.; Awan, Z. Familial hypercholesterolemia mutations in the Middle Eastern and North African region: A need for a national registry. J. Clin. Lipidol. 2015, 9, 187–194. [Google Scholar] [CrossRef]
- Juhász, L.; Balogh, I.; Madar, L.; Kovács, B.; Harangi, M. A Rare Double Heterozygous Mutation in Low-Density Lipoprotein Receptor and Apolipoprotein B-100 Genes in a Severely Affected Familial Hypercholesterolaemia Patient. Cureus 2020, 12, e12184. [Google Scholar] [CrossRef]
- Wittrup, H.H.; Tybjærg-Hansen, A.; Nordestgaard, B.G. Lipoprotein lipase mutations, plasma lipids and lipoproteins, and risk of ischemic heart disease: A meta-analysis. Circulation 1999, 99, 2901–2907. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient | Age | Sex | TC [mg/dL] | LDL-C [mg/dL] | HDL-C [mg/dL] | TG [mg/dL] | NGS Result | |
|---|---|---|---|---|---|---|---|---|
| HGVSc | Gene | |||||||
| 1. | 15 | M | 293 | 253 | 42 | 45 | - | |
| 2A. | 6 | F | 228 | 152 | NA | 47 | - | |
| 2B. | 10 | F | 226 | 155 | 51 | 98 | - | |
| 3. | 11 | M | 228 | 134 | 55 | 190 | NM_022436.2:c.593G>A | ABCG5 |
| 4. | 3 | F | 277 | 222 | 47 | 43 | - | |
| 5. | 9 | F | 312 | 248 | 37 | 137 | NM_000527.4:c.1846-2A>C | LDLR |
| 6. | 16 | F | 280 | 200 | 50 | 102 | NM_000527.4:c.2416dupG | LDLR |
| NM_000384.2:c.10708C>T | APOB | |||||||
| 7A. | 5 | F | 278 | 170 | 61 | 110 | NM_000527.4:c.373_379delCAGTTCG | LDLR |
| 7B. | 10 | M | 426 | 348 | 56 | 82 | NM_000527.4:c.373_379delCAGTTCG | LDLR |
| 8. | 12 | M | 318 | 237 | 67 | 73 | NM_000527.4:c.190+1G>A | LDLR |
| 9A. | 13 | M | 303 | 237 | 49 | 137 | NM_000527.4:c.1775G>A | LDLR |
| 9B. | 17 | F | 289 | 218 | 39 | 162 | NM_000527.4:c.1775G>A | LDLR |
| 10. | 8 | F | 265 | 165 | 73 | 138 | NM_022436.2:c.1285G>A | ABCG5 |
| 11. | 13 | M | 218 | 156 | 48 | 121 | NM_000527.4:c.1775G>A | LDLR |
| 12A. | 13 | F | 234 | 171 | 40 | 90 | - | |
| 12B. | 14 | F | 233 | 191 | 42 | 102 | - | |
| 13. | 10 | M | 193 | 135 | 45 | NA | - | |
| 14. | 10 | M | 279 | 150 | 44 | 138 | NM_000237.2:c.106G>A | LPL |
| 15. | 14 | F | 336 | 267 | 52 | 106 | - | |
| 16. | 10 | M | 239 | 174 | 53 | 125 | - | |
| 17. | 9 | F | 252 | 165 | 53 | 47 | NM_000527.4:c.1775G>A | LDLR |
| 18. | 4 | F | 266 | 200 | 44 | 111 | NM_000384.2:c.10580G>A | APOB |
| 19. | 9 | F | 283 | 201 | 69 | 65 | - | |
| 20. | 9 | F | 290 | 188 | 64 | 188 | - | |
| 21. | 6 | F | 219 | 137 | 76 | 50 | - | |
| 22. | 2 | F | 278 | 216 | 25 | 546 | - | |
| 23. | 5 | M | 307 | 240 | 52 | 73 | NM_000527.4:c.1775G>A | LDLR |
| 24. | 13 | F | NA | NA | NA | NA | NM_000527.4:c.284G>T | LDLR |
| 25. | 6 | F | 348 | 263 | NA | NA | NM_000527.4:c.1775G>A | LDLR |
| 26. | 16 | F | 440 | 367 | 43 | 144 | - | |
| 27. | 17 | F | 380 | 303 | 61 | 81 | NM_000527.4:c.1775G>A | LDLR |
| 28. | 4 | M | 265 | 198 | 47 | 100 | - | |
| 29. | 9 | F | 233 | 143 | 56 | 178 | - | |
| 30. | 9 | F | 402 | 316 | 68 | 84 | NM_000527.4:c.530C>T | LDLR |
| 31. | 5 | F | 345 | 273 | 55 | 86 | NM_000527.4:c.190+1G>A | LDLR |
| 32. | 14 | M | 320 | 263 | 54 | 92 | NM_000527.4:c.1775G>A | LDLR |
| NM_000237.2:c.953A>G | LPL | |||||||
| 33. | 13 | M | 331 | 245 | 74 | 62 | NM_000527.4:c.1916T>A | LDLR |
| 34. | 10 | F | 350 | 310 | 42 | 78 | NM_000527.4:c.324_325delGTinsTC | LDLR |
| 35. | 11 | M | 459 | 398 | 42 | 83 | NM_000527.4:c.2063delA | LDLR |
| 36. | 3 | M | 314 | 252 | 44 | 80 | NM_000527.4:c.1061A>G | LDLR |
| 37. | 15 | F | 364 | 294 | 45 | 124 | NM_000527.4:c.324_325delGTinsTC | LDLR |
| 38. | 5 | F | 745 | 693 | 37 | 73 | NM_000527.4:c.1747C>T | LDLR |
| 39. | 10 | F | 331 | 247 | 73 | 54 | - | |
| 40. | 9 | F | 288 | 216 | 57 | 74 | NM_000527.4:c.798T>A | LDLR |
| 41. | 13 | F | 387 | 316 | 53 | 86 | NM_000527.4:c.1433G>A | LDLR |
| 42. | 14 | F | 274 | 196 | 66 | 63 | NM_000384.2:c.10580G>A | APOB |
| 43. | 12 | F | 290 | 206 | 59 | 80 | - | |
| 44. | 17 | M | 280 | 262 | 49 | 97 | NM_000527.4:c.1061A>G | LDLR |
| 45. | 9 | M | 265 | 144 | 73 | 95 | NM_000527.4:c.1775G>A | LDLR |
| 46. | 2 | F | 228 | 170 | 48 | 52 | NM_000384.2:c.10580G>A | APOB |
| 47. | 6 | F | 248 | 177 | 68 | 103 | - | |
| 48. | 8 | F | 230 | 185 | 42 | 106 | - | |
| 49. | 3 | M | 209 | 101 | 77 | 74 | NM_022436.2:c.1336C>T | ABCG5 |
| 50. | 15 | F | 229 | 170 | 46 | 109 | - | |
| 51. | 10 | M | 219 | 177 | 16 | 72 | - | |
| 52. | 10 | M | 242 | 170 | 46 | 135 | - | |
| 53. | 6 | F | 235 | 154 | NA | 49 | NM_000527.4:c.907C>T | LDLR |
| TC [mg/dL] Mean ± SD | LDL [mg/dL] Mean ± SD | HDL [mg/dL] Mean ± SD | TG [mg/dL] Mean ± SD | |
|---|---|---|---|---|
| Study group | 296.4 ± 85.2 | 224.0 ± 89.2 | 52.4 ± 12.7 | 104.4 ± 70.4 |
| Patients with genetic findings | 329.1 ± 92.8 | 257.4 ± 98.1 | 51.6 ± 9.8 | 90.6 ± 30.4 |
| Patients without genetic findings | 245.1 ± 31.6 | 175.8 ± 31.4 | 53.5 ± 15.9 | 126.2 ± 102.5 |
| Gene | Exon /Intron | Hgvsc | Hgvsp | Genotype | Variant Type | In Silico Prediction | Classification | Nr. of Cases | ||
|---|---|---|---|---|---|---|---|---|---|---|
| Polyphen | SIFT | Mutation Taster | ||||||||
| LDLR | 12 | NM_000527.4:c.1775G>A | NP_000518.1:p. Gly592Glu | het | missense | probably damaging (0.927) | deleterious (0.01) | disease causing | pathogenic | 9 |
| LDLR | 4 | NM_000527.4:c.373_ 379delCAGTTCG | NP_000518.1:p. Gln125SerfsTer79 | het | deletion | NA | NA | disease causing | presumed pathogenic | 2 |
| LDLR | 2 | NM_000527.4:c.190+1G>A | NA | het | splice donor | NA | NA | NA | presumed pathogenic | 2 |
| LDLR | 4 | NM_000527.4:c.324_ 325delGTinsTC | NP_000518.1:p. Cys109Arg | het | missense | NA | NA | NA | presumed pathogenic | 2 |
| LDLR | 8 | NM_000527.4:c.1061A>G | NP_000518.1:p. Asp354Gly | het | missense | probably damaging (1) | deleterious (0) | disease causing | presumed pathogenic | 2 |
| LDLR | 17 | NM_000527.4:c.2416dupG | NP_000518.1:p. Val806GlyfsTer11 | het | duplication | NA | NA | NA | presumed pathogenic | 1 |
| LDLR | 12 | NM_000527.4:c.1846-2A>C | NA | het | splice acceptor | NA | NA | NA | presumed pathogenic | 1 |
| LDLR | 3 | NM_000527.4:c.284G>T | NP_000518.1:p. Cys95Phe | het | missense | probably damaging (0.999) | deleterious (0) | disease causing | presumed pathogenic | 1 |
| LDLR | 4 | NM_000527.4:c.530C>T | NP_000518.1:p. Ser177Leu | het | missense | probably damaging (1) | deleterious (0.01) | disease causing | presumed pathogenic | 1 |
| LDLR | 13 | NM_000527.4:c.1916T>A | NP_000518.1:p. Val639Asp | het | missense | benign (0.245) | deleterious (0) | disease causing | presumed pathogenic | 1 |
| LDLR | 14 | NM_000527.4:c.2063delA | NP_000518.1:p. Asn688ThrfsTer21 | het | deletion | NA | NA | NA | presumed pathogenic | 1 |
| LDLR | 12 | NM_000527.4:c.1747C>T | NP_000518.1:p. His583Tyr | het | missense | probably damaging (1) | deleterious (0) | disease causing | presumed pathogenic | 1 |
| LDLR | 5 | NM_000527.4:c.798T>A | NP_000518.1:p. Asp266Glu | het | missense | probably damaging (0.979) | deleterious (0) | disease causing | presumed pathogenic | 1 |
| LDLR | 10 | NM_000527.4:c.1433G>A | NP_000518.1:p. Gly478Glu | het | missense | probably damaging (0.998) | deleterious (0) | disease causing | presumed pathogenic | 1 |
| LDLR | 6 | NM_000527.4:c.907C>T | NP_000581.1:p. Arg303Trp | het | missense | probably damaging (0.998) | Tolerated (0.37) | disease causing | presumed pathogenic | 1 |
| Sum of LDLR-positive patients | 27 | |||||||||
| APOB | 26 | NM_000384.2:c.10580G>A | NP_000375.2:p. Arg3527Gln | het | missense | probably damaging (0.93) | NA | disease causing | pathogenic | 3 |
| APOB | 26 | NM_000384.2:c.10708C>T | NP_000375.2:p. His3570Tyr | het | missense | benign (0.003) | NA | polymorphism | uncertain significance | 1 |
| Sum of APOB-positive patients | 4 | |||||||||
| ABCG5 | 5 | NM_022436.2:c.593G>A | NP_071881.1:p. Arg198Gln | het | missense | probably damaging (1) | deleterious (0) | disease causing | uncertain significance | 1 |
| ABCG5 | 9 | NM_022436.2:c.1285G>A | NP_071881.1:p. Ala429Thr | het | missense | possibly damaging (0.558) | deleterious (0) | polymorphism | uncertain significance | 1 |
| Sum of ABCG5-positive patients | 2 | |||||||||
| LPL | 2 | NM_000237.2:c.106G>A | NP_000228.1:p. Asp36Asn | het | missense | benign (0.066) | tolerated (0.16) | disease causing | risk factor | 1 |
| LPL | 6 | NM_000237.2:c.953A>G | NP_000228.1:p. Asn318Ser | het | missense | benign (0.019) | tolerated (0.24) | disease causing | presumed pathogenic | 1 |
| Sum of LPL-positive patients | 2 | |||||||||
| Total sum of NGS-positive patients | 35 | |||||||||
| Subject | Age | TC | LDL | HDL | TG | c.373_379delCAGTTCG Presence |
|---|---|---|---|---|---|---|
| mg/dL | ||||||
| Child 1 | 10 | 426 | 348 | 56 | 82 | + |
| Child 2 | 5 | 278 | 170 | 61 | 110 | + |
| Mother | 41 | 266 | 132 | 97 | 186 | - |
| Father | 43 | 384 | 317 | 51 | 83 | + |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rutkowska, L.; Sałacińska, K.; Salachna, D.; Matusik, P.; Pinkier, I.; Kępczyński, Ł.; Piotrowicz, M.; Starostecka, E.; Lewiński, A.; Gach, A. Identification of New Genetic Determinants in Pediatric Patients with Familial Hypercholesterolemia Using a Custom NGS Panel. Genes 2022, 13, 999. https://doi.org/10.3390/genes13060999
Rutkowska L, Sałacińska K, Salachna D, Matusik P, Pinkier I, Kępczyński Ł, Piotrowicz M, Starostecka E, Lewiński A, Gach A. Identification of New Genetic Determinants in Pediatric Patients with Familial Hypercholesterolemia Using a Custom NGS Panel. Genes. 2022; 13(6):999. https://doi.org/10.3390/genes13060999
Chicago/Turabian StyleRutkowska, Lena, Kinga Sałacińska, Dominik Salachna, Paweł Matusik, Iwona Pinkier, Łukasz Kępczyński, Małgorzata Piotrowicz, Ewa Starostecka, Andrzej Lewiński, and Agnieszka Gach. 2022. "Identification of New Genetic Determinants in Pediatric Patients with Familial Hypercholesterolemia Using a Custom NGS Panel" Genes 13, no. 6: 999. https://doi.org/10.3390/genes13060999
APA StyleRutkowska, L., Sałacińska, K., Salachna, D., Matusik, P., Pinkier, I., Kępczyński, Ł., Piotrowicz, M., Starostecka, E., Lewiński, A., & Gach, A. (2022). Identification of New Genetic Determinants in Pediatric Patients with Familial Hypercholesterolemia Using a Custom NGS Panel. Genes, 13(6), 999. https://doi.org/10.3390/genes13060999