
Strategy to Estimate Sample Sizes to Justify the Association between MMP1 SNP and Osteoarthritis

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Case–Control Study
2.1.1. Ethical Issues
2.1.2. Subjects
2.1.3. Genomic DNA Extraction and Genotyping
2.1.4. Statistical Analysis
2.2. Meta-Analysis
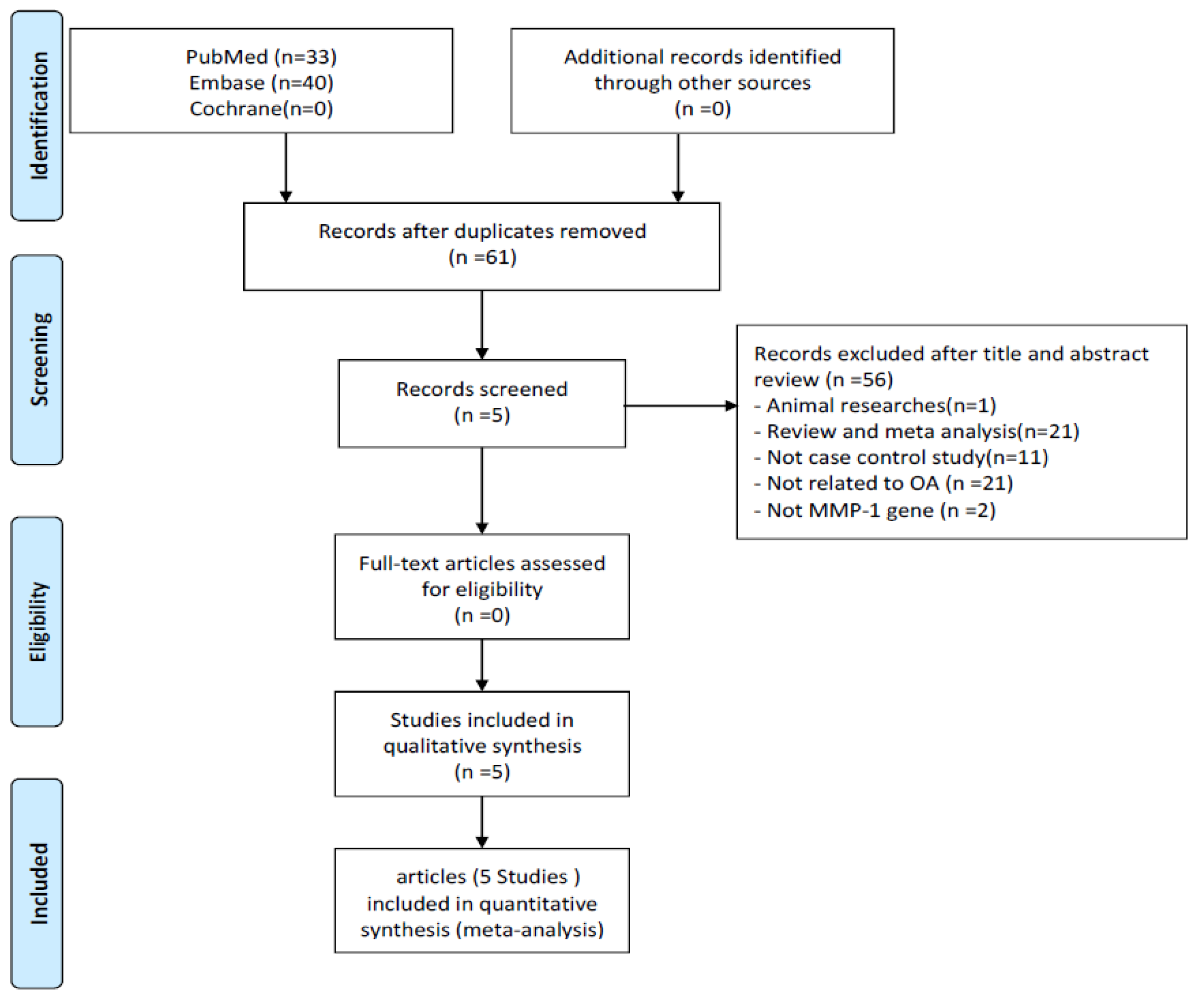
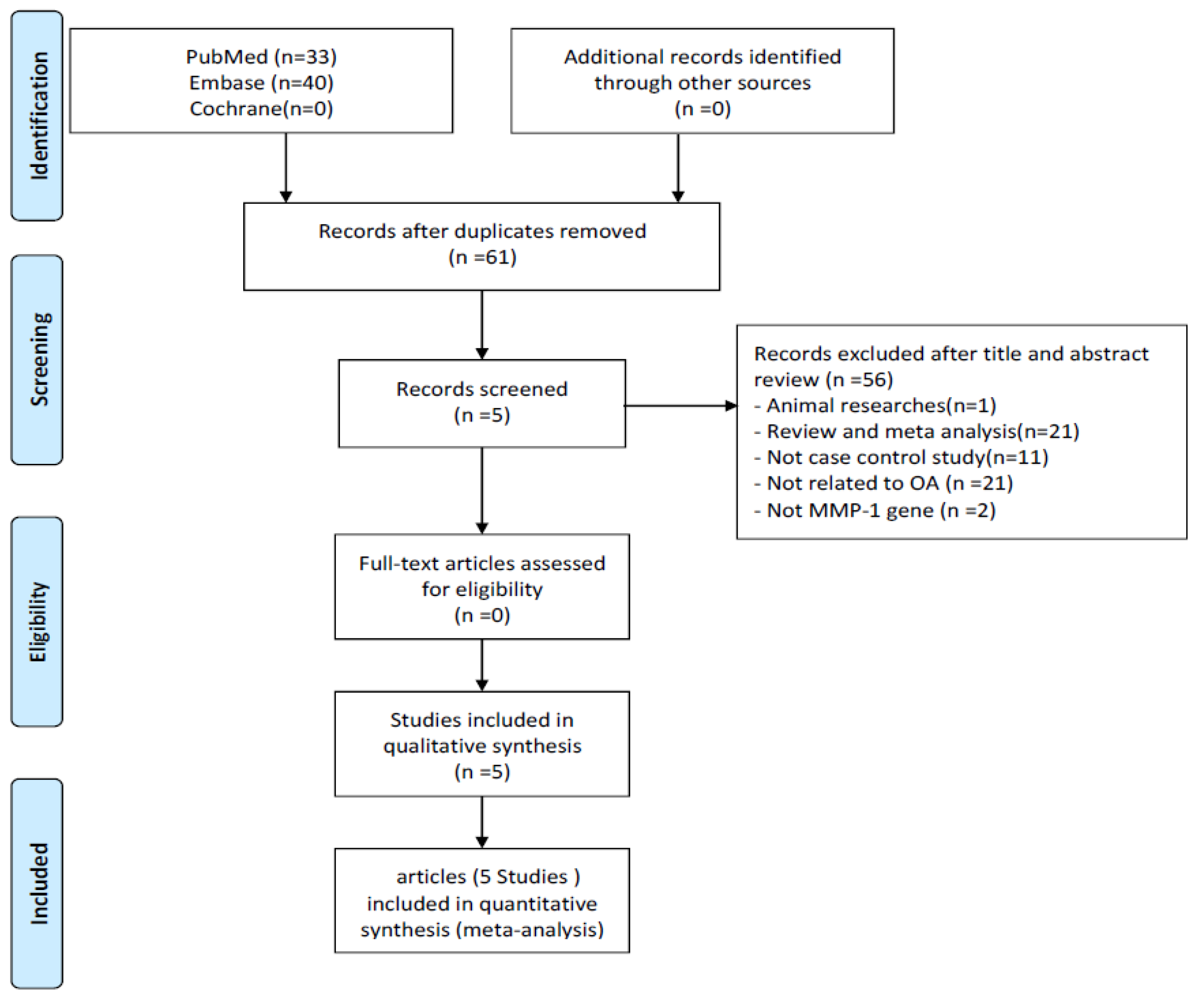
2.2.1. Search Methods and Criteria for Study Consideration
2.2.2. Data Extraction
2.2.3. Statistical Analysis
3. Results
3.1. Case–Control Study
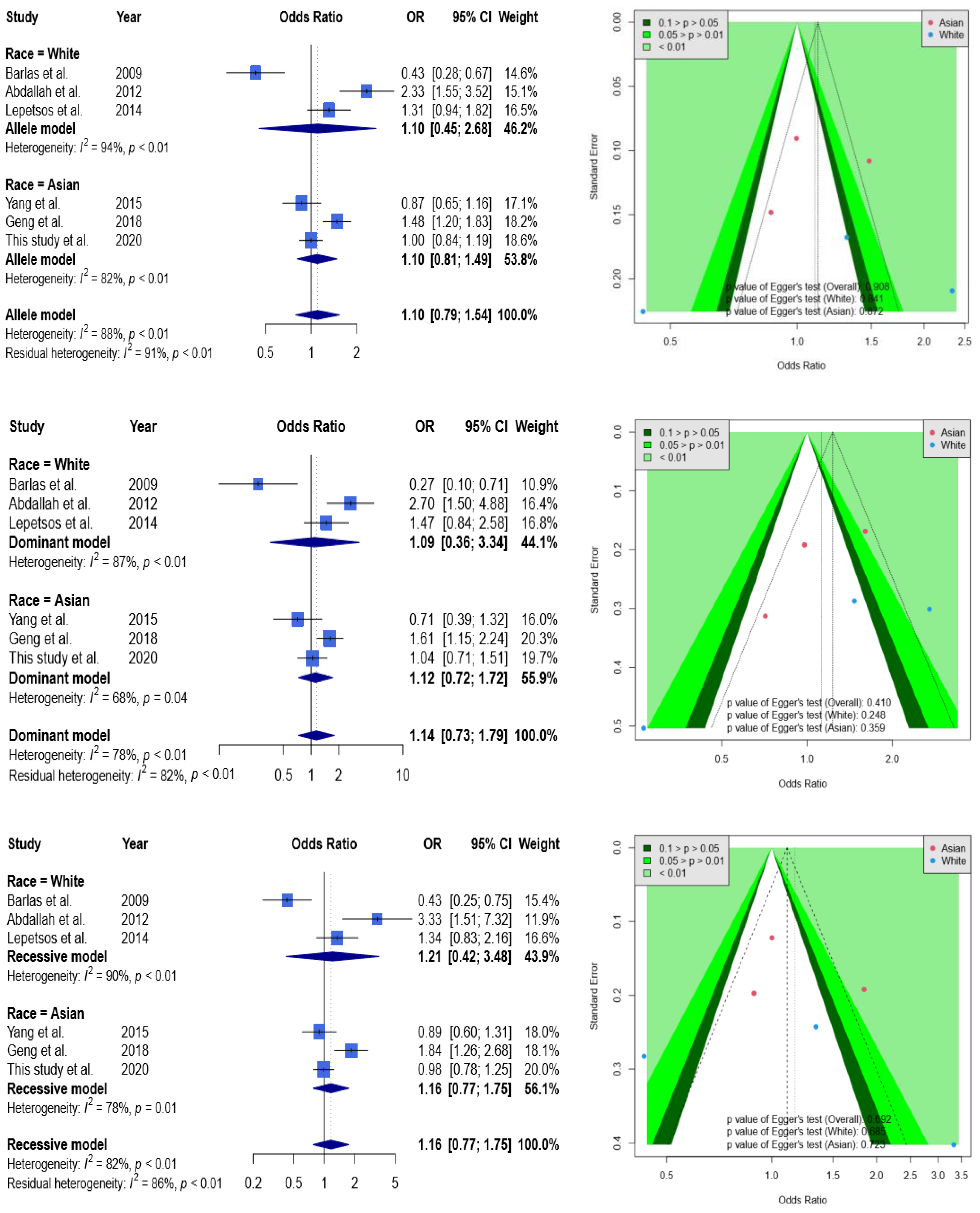
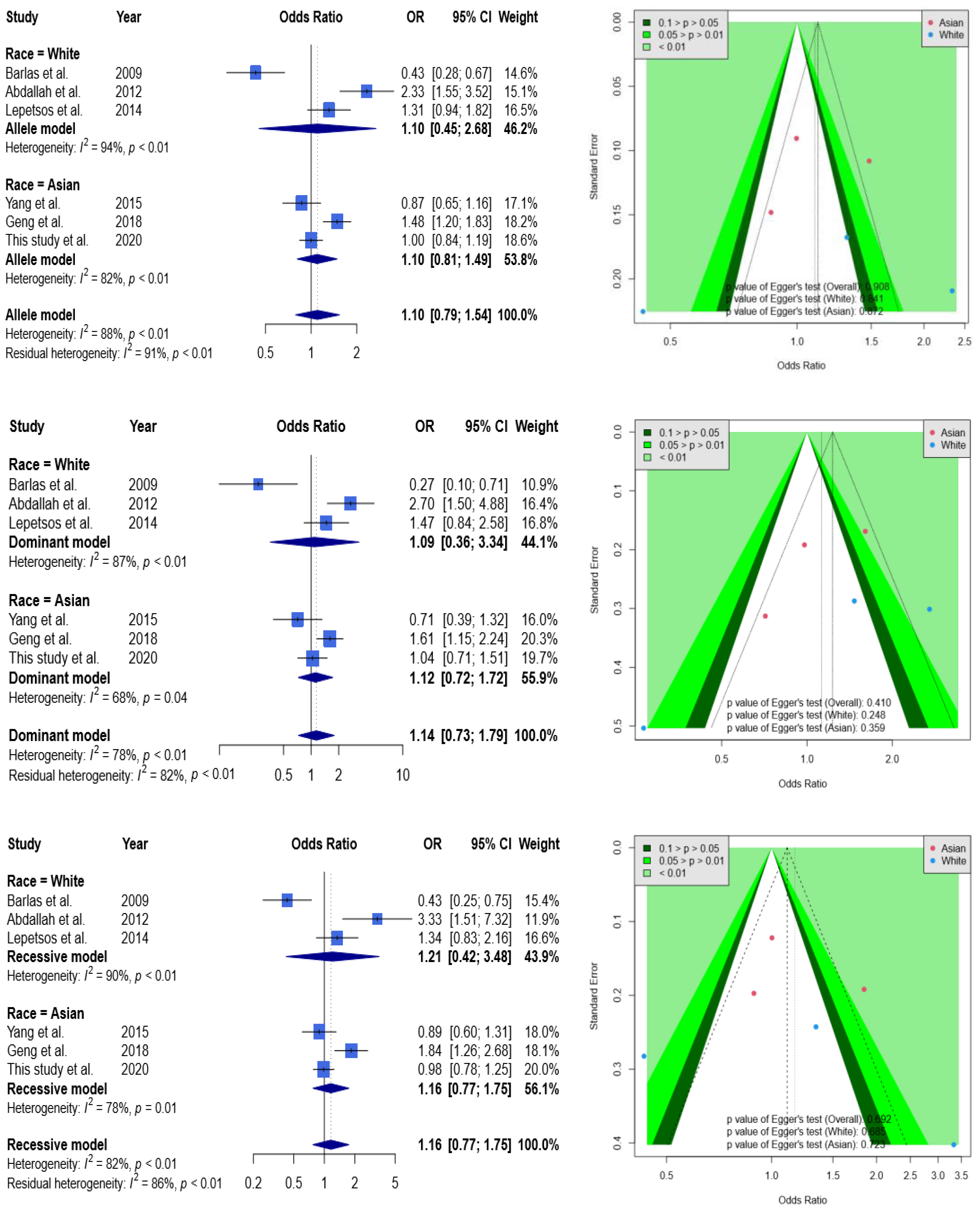
3.2. Meta-Analysis
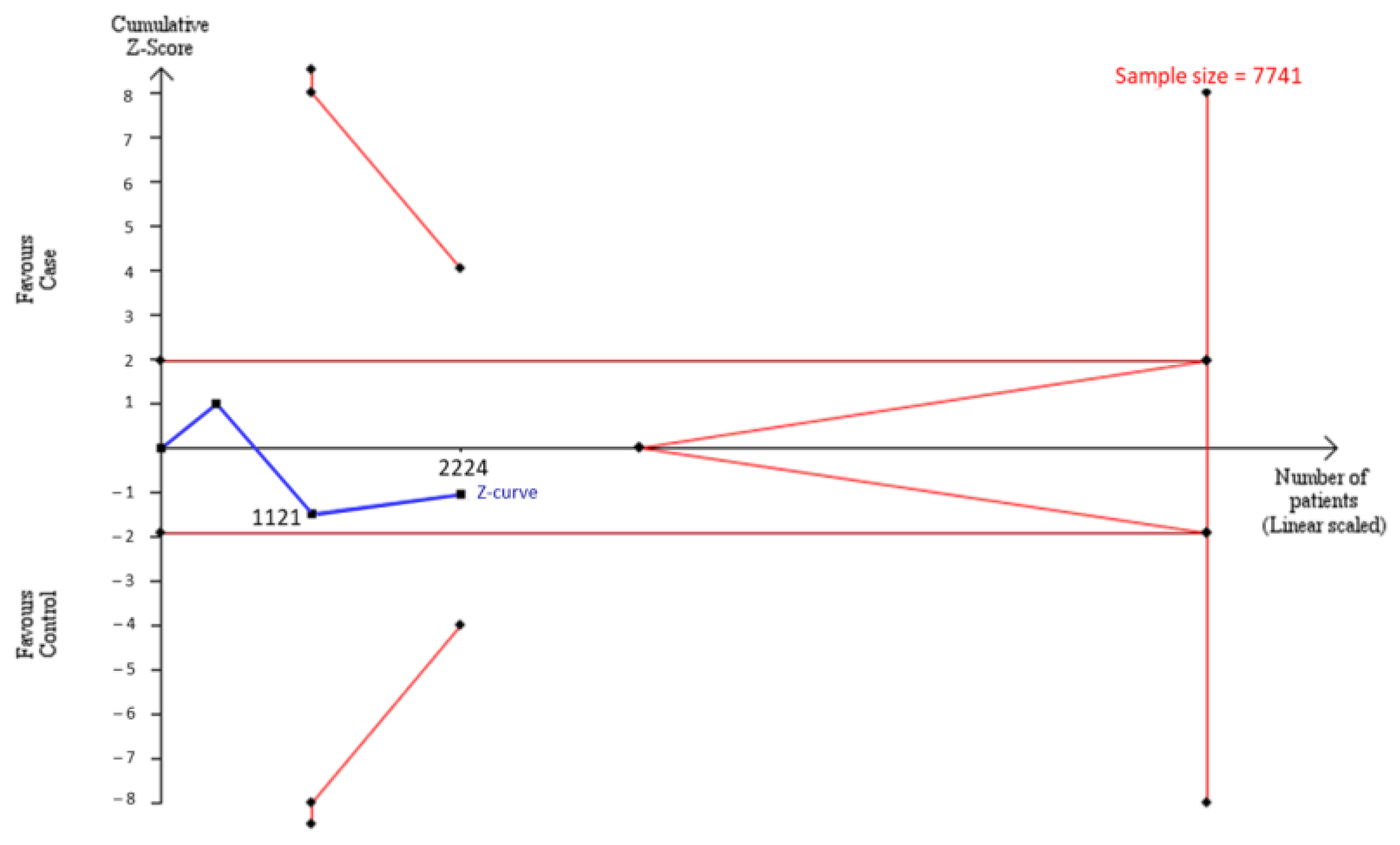
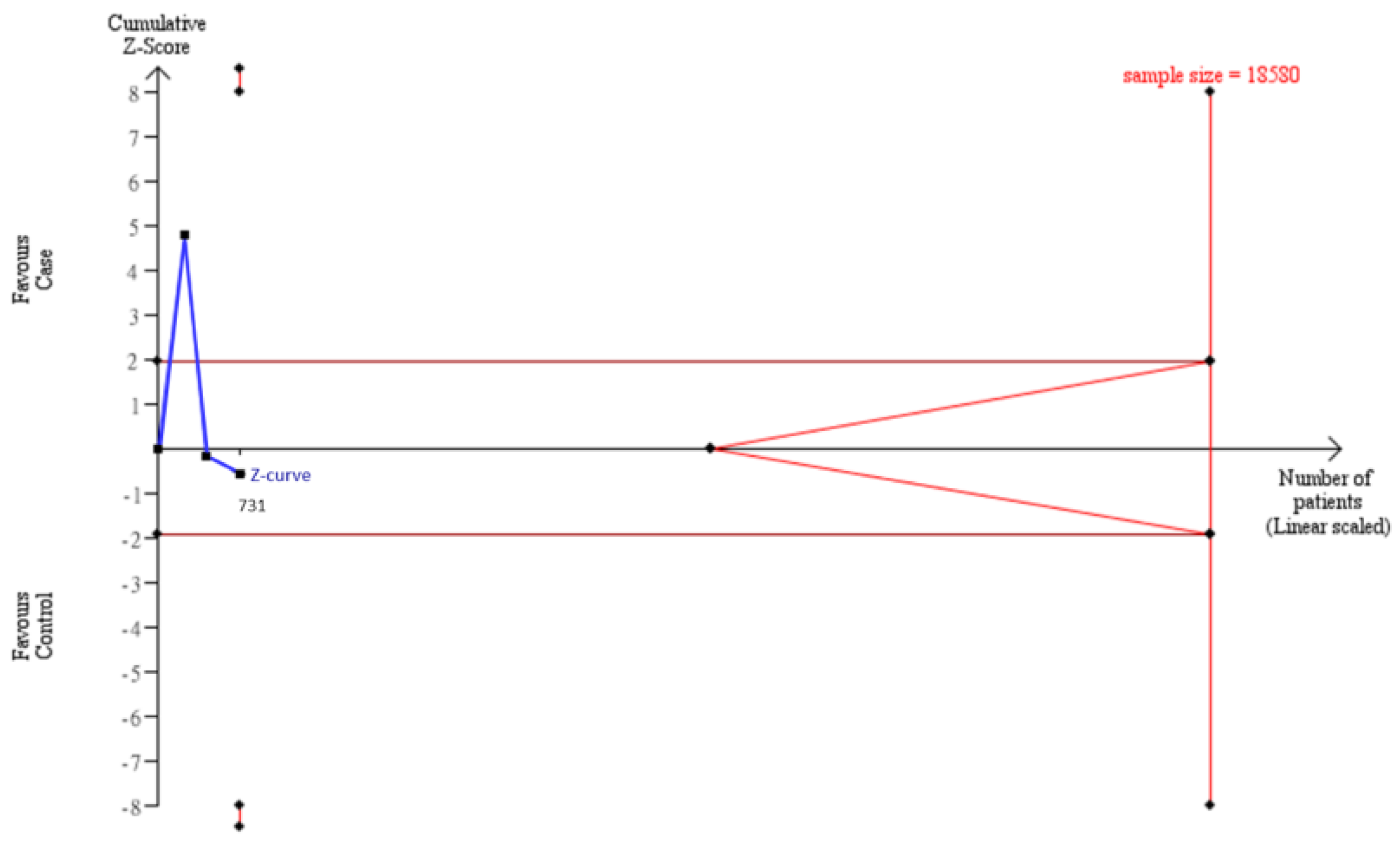
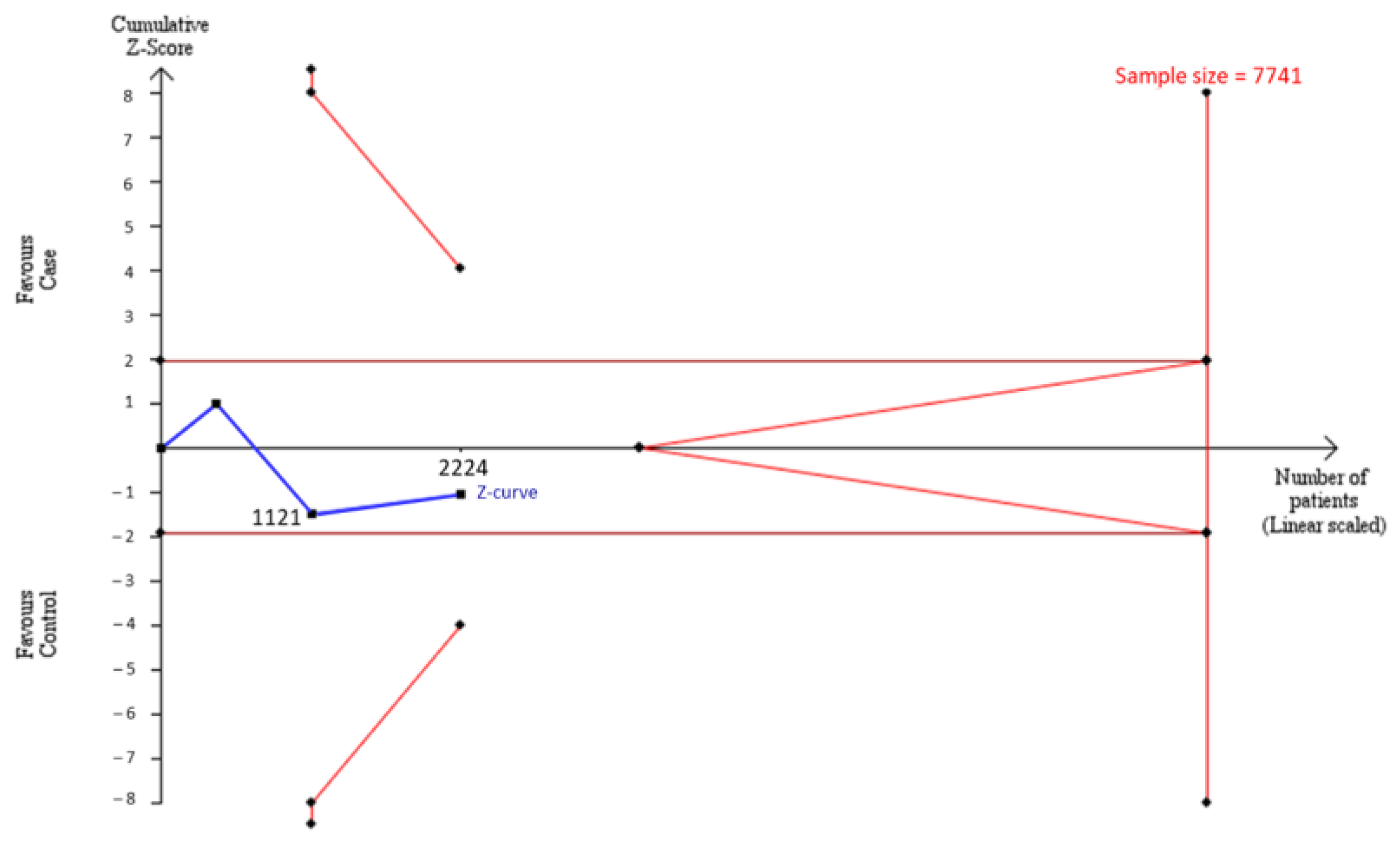
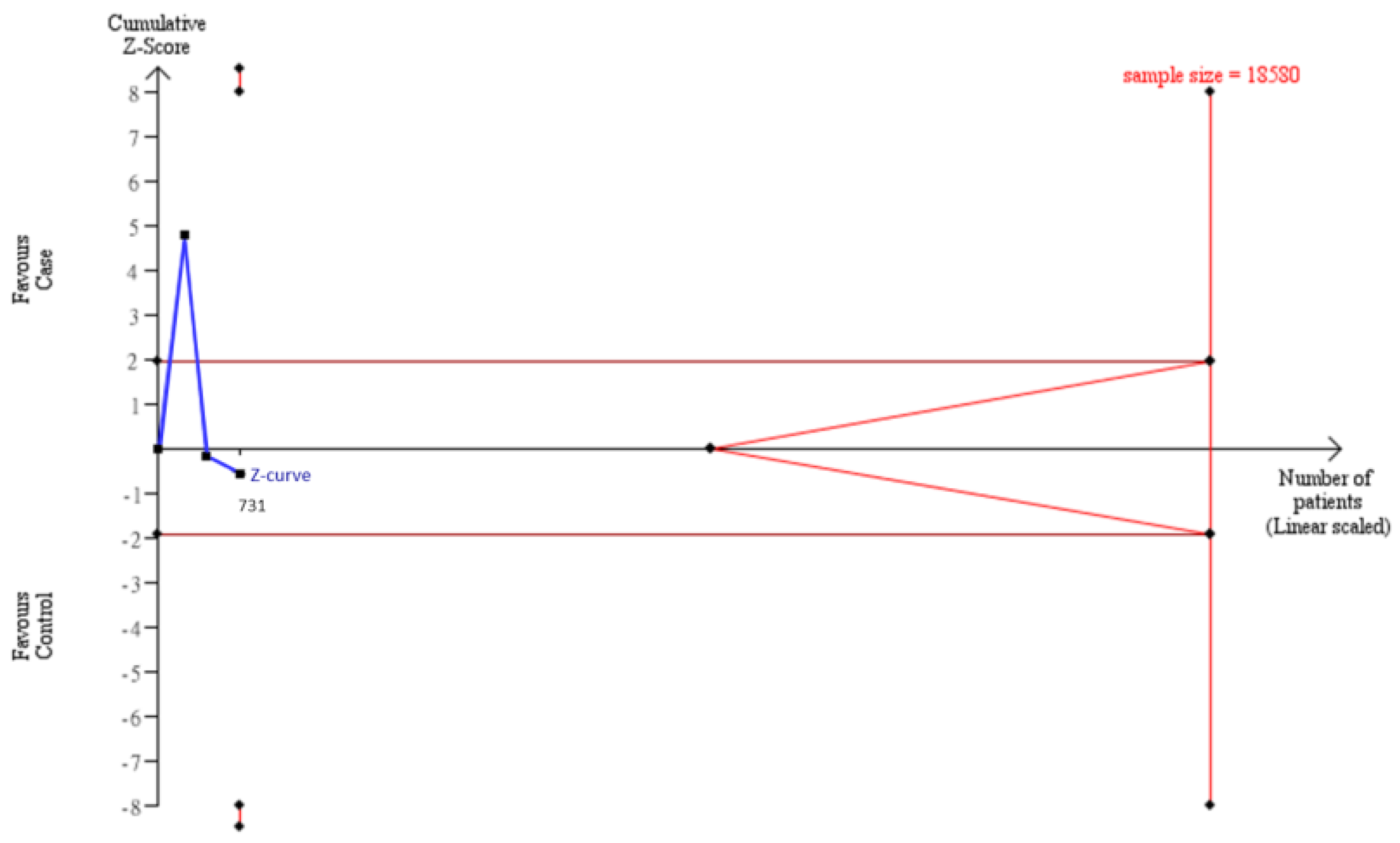
3.3. TSA Evaluation
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Damen, J.; Van Rijn, R.M.; Emans, P.J.; Hilberdink, W.K.H.A.; Wesseling, J.; Oei, E.H.G.; Bierma-Zeinstra, S.M.A. Prevalence and development of hip and knee osteoarthritis according to American College of Rheumatology criteria in the CHECK cohort. Arthritis Res. Ther. 2019, 21, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spector, T.D.; Cicuttini, F.; Baker, J.; Loughlin, J.; Hart, D. Genetic influences on osteoarthritis in women: A twin study. BMJ 1996, 312, 940–943. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reginato, A.M.; Olsen, B.R. The role of structural genes in the pathogenesis of osteoarthritic disorders. Arthritis Res. Ther. 2002, 4, 337–345. [Google Scholar] [CrossRef] [PubMed]
- Arakaki, P.A.; Marques, M.R.; Santos, M.C.L.G. MMP-1 polymorphism and its relationship to pathological processes. J. Biosci. 2009, 34, 313–320. [Google Scholar] [CrossRef]
- Burrage, P.S.; Mix, K.S.; Brinckerhoff, C.E. Matrix Metalloproteinases: Role In Arthritis. Front. Biosci. 2006, 11, 529–543. [Google Scholar] [CrossRef] [Green Version]
- Kaspiris, A.; Khaldi, L.; Grivas, T.; Vasiliadis, E.; Kouvaras, I.; Dagkas, S.; Chronopoulos, E.; Papadimitriou, E. Subchondral cyst development and MMP-1 expression during progression of osteoarthritis: An immunohistochemical study. Orthop. Traumatol. Surg. Res. 2013, 99, 523–529. [Google Scholar] [CrossRef] [Green Version]
- Rutter, J.; I Mitchell, T.; Buttice’, G.; Meyers, J.; Gusella, J.F.; Ozelius, L.J.; E Brinckerhoff, C. A single nucleotide polymorphism in the matrix metalloproteinase-1 promoter creates an Ets binding site and augments transcription. Cancer Res. 1998, 58, 5321–5325. [Google Scholar]
- Song, Y.-Q.; Ho, D.W.; Karppinen, J.; Kao, P.Y.; Fan, B.-J.; Luk, K.D.; Yip, S.-P.; Leong, J.C.; Cheah, K.S.; Sham, P.; et al. Association between promoter -1607 polymorphism of MMP1 and Lumbar Disc Disease in Southern Chinese. BMC Med. Genet. 2008, 9, 38. [Google Scholar] [CrossRef] [Green Version]
- Tetlow, L.C.; Adlam, D.J.; Woolley, D.E. Matrix metalloproteinase and proinflammatory cytokine production by chondrocytes of human osteoarthritic cartilage: Associations with degenerative changes. Arthritis Rheum. 2001, 44, 585–594. [Google Scholar] [CrossRef]
- Barlas, I.; Sezgin, M.; Erdal, M.E.; Sahin, G.; Ankarali, H.C.; Altintas, Z.M.; Türkmen, E. Association of (−1607) 1G/2G polymorphism of matrix metalloproteinase-1 gene with knee osteoarthritis in the Turkish population (knee osteoarthritis and MMPs gene polymorphisms). Rheumatol. Int. 2009, 29, 383–388. [Google Scholar] [CrossRef]
- Abd-Allah, S.H.; Shalaby, S.M.; Pasha, H.F.; El-Shal, A.S.; El-Saoud, A.M.A. Variation of Matrix Metalloproteinase 1 and 3 Haplotypes and Their Serum Levels in Patients with Rheumatoid Arthritis and Osteoarthritis. Genet. Test. Mol. Biomark. 2012, 16, 15–20. [Google Scholar] [CrossRef]
- Lepetsos, P.; Pampanos, A.; Kanavakis, E.; Tzetis, M.; Korres, D.; Papavassiliou, A.G.; Efstathopoulos, N. Association of MMP-1 -1607 1G/2G (rs1799750) polymorphism with primary knee osteoarthritis in the Greek population. J. Orthop. Res. 2014, 32, 1155–1160. [Google Scholar] [CrossRef] [PubMed]
- Yang, H.; Chuang, S.; Fang, W.; Huang, G.; Wang, C.; Huang, Y.; Chu, M.; Lin, C.; Su, W.; Chen, C.; et al. Effect of RAGE polymorphisms on susceptibility to and severity of osteoarthritis in a Han Chinese population: A case-control study. Genet. Mol. Res. 2015, 14, 11362–11370. [Google Scholar] [CrossRef] [PubMed]
- Geng, R.; Xu, Y.; Hu, W.; Zhao, H. The association between MMP-1 gene rs1799750 polymorphism and knee osteoarthritis risk. Biosci. Rep. 2018, 38, BSR20181257. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Møller, A.M.; Myles, P. What makes a good systematic review and meta-analysis? Br. J. Anaesth. 2016, 117, 428–430. [Google Scholar] [CrossRef] [Green Version]
- Thorlund, K.; Engstrøm, J.; Wetterslev, J.; Brok, J.; Imberger, G.; Gluud, C. User Manual for Trial Sequential Analysis (TSA); Copenhagen Trial Unit, Centre for Clinical Intervention Research: Copenhagen, Denmark, 2011; pp. 1–115. Available online: www.ctu.dk/tsa.2012 (accessed on 18 July 2021).
- Wetterslev, J.; Jakobsen, J.C.; Gluud, C. Trial Sequential Analysis in systematic reviews with meta-analysis. BMC Med. Res. Methodol. 2017, 17, 1–18. [Google Scholar] [CrossRef] [Green Version]
- Kellgren, J.H.; Lawrence, J.S. Radiological Assessment of Osteo-Arthrosis. Ann. Rheum. Dis. 1957, 16, 494–502. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Viechtbauer, W. Conducting Meta-Analyses in R with themetaforPackage. J. Stat. Softw. 2010, 36, 1–48. [Google Scholar] [CrossRef] [Green Version]
- Schwarzer, G.; Carpenter, J.R.; Rücker, G. Meta-Analysis with R; Springer: Berlin/Heidelberg, Germany, 2015; Volume 4784. [Google Scholar]
- Xu, B.; Xing, R.-L.; Zhang, L.; Huang, Z.-Q.; Zhang, N.-S.; Mao, J. Effects of MMP-1 1G/2G polymorphism on osteoarthritis: A meta-analysis study. Acta Orthop. Traumatol. Turc. 2019, 53, 129–133. [Google Scholar] [CrossRef]
- Peng, L.; Bin, J.; Ou, Y.-C.; Zhu, L.L.; Lu, J.J. Lack of association between matrix metalloproteinase-1 gene rs1799750 polymorphism and osteoarthritis susceptibility: A meta-analysis. Biosci. Rep. 2019, 39, BSR20181960. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Wang, G.; Peng, Z. Association between the MMP-1-1607 1G/2G Polymorphism and Osteoarthritis Risk: A Systematic Review and Meta-Analysis. BioMed Res. Int. 2020, 2020, 5190587. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.C.; Sutton, A.J.; Ioannidis, J.P.A.; Terrin, N.; Jones, D.R.; Lau, J.; Carpenter, J.; Rücker, G.; Harbord, R.M.; Schmid, C.H.; et al. Recommendations for examining and interpreting funnel plot asymmetry in meta-analyses of randomised controlled trials. BMJ 2011, 343, d4002. [Google Scholar] [CrossRef] [Green Version]
- Lin, C.; Chu, C.; Lin, J.; Yang, H.-Y.; Su, S.-L. Gene-Gene and Gene-Environment Interactions in Meta-Analysis of Genetic Association Studies. PLoS ONE 2015, 10, e0124967. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Knee OA Group (n = 569) | Control Group (n = 534) | p Value | |
|---|---|---|---|
| Gender (%) | <0.001 * | ||
| Male | 204 (35.9%) | 263 (49.3%) | |
| Female | 365 (64.1%) | 271 (50.7%) | |
| Age (mean ± SD) | 73.55 ± 7.27 | 71.60 ± 6.86 | <0.001 * |
| BMI (mean ± SD) | 24.63 ± 3.61 | 24.12 ± 3.33 | 0.018 * |
| 25th percentiles | 22.33 | 21.78 | |
| Median | 24.38 | 23.92 | |
| 75th percentiles | 26.73 | 25.88 | |
| KL Grade (%) | <0.001 * | ||
| 0 | 0 | 22 (4.1%) | |
| 1 | 0 | 512 (95.9%) | |
| 2 | 420 (73.8%) | 0 | |
| 3 | 79 (13.9%) | 0 | |
| 4 | 70 (12.3%) | 0 |
| Knee OA Group (n = 569) | Control Group (n = 534) | Crude-OR (95% CI) | p Value | Adj-OR a (95% CI) | p Value | |
|---|---|---|---|---|---|---|
| Genotype | ||||||
| 1G1G | 63(11.1%) | 61(11.4%) | 1.00 | 1.00 | ||
| 1G2G | 262(46.0%) | 242(45.3%) | 1.05 (0.71–1.55) | 0.814 | 1.07 (0.71–1.63) | 0.734 |
| 2G2G | 244(42.9%) | 231(43.3%) | 1.02 (0.69–1.52) | 0.911 | 1.02 (0.67–1.55) | 0.930 |
| Allele Model | ||||||
| 1G | 388(34.1%) | 364(34.1%) | 1.00 | 1.00 | ||
| 2G | 750(65.9%) | 704(65.9%) | 1.00 (0.84–1.19) | 0.995 | 0.96 (0.75–1.24) | 0.762 |
| Dominant Model | ||||||
| 1G1G | 63(11.1%) | 61(11.4%) | 1.00 | 1.00 | ||
| 1G2G + 2G2G | 506(88.9%) | 473(88.6%) | 1.04 (0.71–1.51) | 0.854 | 1.05 (0.71–1.55) | 0.818 |
| Recessive Model | ||||||
| 1G1G + 1G2G | 325(57.1%) | 303(56.7%) | 1.00 | 1.00 | ||
| 2G2G | 244(42.9%) | 231(43.3%) | 0.98 (0.78–1.25) | 0.900 | 0.96 (0.75–1.24) | 0.762 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kao, C.-C.; Hsu, H.-E.; Lai, J.-C.; Chen, H.-C.; Chuang, S.-W.; Lee, M.-C. Strategy to Estimate Sample Sizes to Justify the Association between MMP1 SNP and Osteoarthritis. Genes 2022, 13, 1084. https://doi.org/10.3390/genes13061084
Kao C-C, Hsu H-E, Lai J-C, Chen H-C, Chuang S-W, Lee M-C. Strategy to Estimate Sample Sizes to Justify the Association between MMP1 SNP and Osteoarthritis. Genes. 2022; 13(6):1084. https://doi.org/10.3390/genes13061084
Chicago/Turabian StyleKao, Chung-Cheng, Hsiang-En Hsu, Jen-Chieh Lai, Hsiang-Cheng Chen, Su-Wen Chuang, and Meng-Chang Lee. 2022. "Strategy to Estimate Sample Sizes to Justify the Association between MMP1 SNP and Osteoarthritis" Genes 13, no. 6: 1084. https://doi.org/10.3390/genes13061084
APA StyleKao, C.-C., Hsu, H.-E., Lai, J.-C., Chen, H.-C., Chuang, S.-W., & Lee, M.-C. (2022). Strategy to Estimate Sample Sizes to Justify the Association between MMP1 SNP and Osteoarthritis. Genes, 13(6), 1084. https://doi.org/10.3390/genes13061084