
Early Markers of Cardiovascular Disease Associated with Clinical Data and Autosomal Ancestry in Patients with Type 1 Diabetes: A Cross-Sectional Study in an Admixed Brazilian Population

 , , ,
, , ,  , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Sample
2.2. Anthropometric and Laboratory Data
2.3. Ophthalmological Evaluation
2.4. Analysis of Early CVD Markers
2.5. Autosomal Ancestry Proportions
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ABI | ankle–brachial index |
| AIM-Indels | autosomal informational insertion/deletion ancestry markers |
| ALT | alanine aminotransferase |
| AST | aspartate aminotransferase |
| BMI | body mass index |
| BP | blood pressure |
| CACS | coronary artery calcium score |
| CMIT | carotid intima-media thickness |
| CVD | cardiovascular disease |
| CVR | cardiovascular risk |
| HDL | high-density lipoprotein |
| hs-CRP | high sensitivity C-reactive protein |
| HU-UFMA | University Hospital of the Federal University of Maranhão |
| LDL | low-density lipoprotein cholesterol |
| PAD | peripheral arterial disease |
| PCR | polymerase chain reaction |
| ±sd | standard deviation |
| T1D | type 1 diabetes |
References
- Schofield, J.; Ho, J.; Soran, H. Cardiovascular Risk in Type 1 Diabetes Mellitus. Diabetes Ther. 2019, 10, 773–789. [Google Scholar] [CrossRef] [PubMed]
- Dahl-Jørgensen, K.; Larsen, J.R.; Hanssen, K.F. Atherosclerosis in childhood and adolescent type 1 diabetes: Early disease, early treatment? Diabetologia 2005, 48, 1445–1453. [Google Scholar] [CrossRef] [PubMed]
- Kupfer, R.; Larrúbia, M.R.; Bussade, I.; Pereira, J.R.D.; Epifanio, M.A.; Schettino, C.D.S.; Momesso, D.P.; Lima, G.A.B. Predictors of subclinical atherosclerosis evaluated by carotid intima-media thickness in asymptomatic young women with type 1 diabetes mellitus. Arch. Endocrinol. Metab. 2017, 61, 115–121. [Google Scholar] [CrossRef] [PubMed]
- Bjornstad, P.; Donaghue, K.C.; Maahs, D.M. Macrovascular disease and risk factors in youth with type 1 diabetes: Time to be more attentive to treatment? Lancet Diabetes Endocrinol. 2018, 6, 809–820. [Google Scholar] [CrossRef]
- Pease, A.; Earnest, A.; Ranasinha, S.; Nanayakkara, N.; Liew, D.; Wischer, N.; Andrikopoulos, S.; Zoungas, S. Burden of cardiovascular risk factors and disease among patients with type 1 diabetes: Results of the Australian National Diabetes Audit (ANDA). Cardiovasc. Diabetol. 2018, 17, 77. [Google Scholar] [CrossRef] [PubMed]
- Bertoluci, M.C.; Moreira, R.O.; Faludi, A.; Izar, M.C.; Schaan, B.D.; Valerio, C.M.; Bertolami, M.C.; Chacra, A.P.; Malachias, M.V.B.; Vencio, S.; et al. Brazilian guidelines on prevention of cardiovascular disease in patients with diabetes: A position statement from the Brazilian Diabetes Society (SBD), the Brazilian Cardiology Society (SBC) and the Brazilian Endocrinology and Metabolism Society (SBEM). Diabetol. Metab. Syndr. 2017, 9, 53. [Google Scholar] [CrossRef] [PubMed]
- Jellinger, P.S.; Handelsman, Y.; Rosenblit, P.D.; Bloomgarden, Z.T.; Fonseca, V.A.; Garber, A.J.; Grunberger, G.; Guerin, C.K.; Bell, D.S.H.; Mechanick, J.I.; et al. American Association of Clinical Endocrinologists and American College of Endocrinology Guidelines for Management of Dyslipidemia and Prevention of Cardiovascular Disease. Endocr. Pr. 2017, 23, 1–87. [Google Scholar] [CrossRef]
- Sarwar, K.N.; Cliff, P.; Saravanan, P.; Khunti, K.; Nirantharakumar, K.; Narendran, P. Comorbidities, complications and mortality in people of South Asian ethnicity with type 1 diabetes compared with other ethnic groups: A systematic review. BMJ Open 2017, 7, e015005. [Google Scholar] [CrossRef]
- Cardena, M.M.S.G.; Ribeiro-Dos-Santos, Â.; Santos, S.; Mansur, A.J.; Pereira, A.C.; Fridman, C. Assessment of the Relationship between Self-Declared Ethnicity, Mitochondrial Haplogroups and Genomic Ancestry in Brazilian Individuals. PLoS ONE 2013, 8, e62005. [Google Scholar] [CrossRef]
- De Souza, A.M.; Resende, S.S.; De Sousa, T.N.; De Brito, C.F.A. A systematic scoping review of the genetic ancestry of the Brazilian population. Genet. Mol. Biol. 2019, 42, 495–508. [Google Scholar] [CrossRef]
- Knopfholz, J.; Disserol, C.C.D.; Pierin, A.J.; Schirr, F.L.; Streisky, L.; Takito, L.L.; Ledesma, P.M.; Faria-Neto, J.R.; Olandoski, M.; Da Cunha, C.L.P.; et al. Validation of the Friedewald Formula in Patients with Metabolic Syndrome. Cholesterol 2014, 2014, 261878. [Google Scholar] [CrossRef] [PubMed]
- Infeld, D.A.; O’Shea, J.G. Diabetic retinopathy. Postgrad. Med. J. 1998, 74, 129–133. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Hirsch, A.T.; Haskal, Z.J.; Hertzer, N.R.; Bakal, C.W.; Creager, M.A.; Halperin, J.L.; Hiratzka, L.F.; Murphy, W.R.; Olin, J.W.; Puschett, J.B.; et al. ACC/AHA 2005 Practice Guidelines for the Management of Patients With Peripheral Arterial Disease (Lower Extremity, Renal, Mesenteric, and Abdominal Aortic). Circulation 2006, 113, e463–e654. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, S.; Morgan, T.; Herrington, D.M.; Xu, J.; Cox, A.J.; Freedman, B.I.; Carr, J.J.; Bowden, N.W. Coronary Calcium Score and Prediction of All-Cause Mortality in Diabetes: The Diabetes Heart Study. Diabetes Care 2011, 34, 1219–1224. [Google Scholar] [CrossRef] [PubMed]
- Stein, J.H.; Korcarz, C.; Hurst, R.T.; Lonn, E.; Kendall, C.B.; Mohler, E.R.; Najjar, S.S.; Rembold, C.; Post, W.S. Use of Carotid Ultrasound to Identify Subclinical Vascular Disease and Evaluate Cardiovascular Disease Risk: A Consensus Statement from the American Society of Echocardiography Carotid Intima-Media Thickness Task Force Endorsed by the Society for Vascular Medicine. J. Am. Soc. Echocardiogr. 2008, 21, 93–111. [Google Scholar] [CrossRef] [PubMed]
- Pereira, R.; Phillips, C.; Pinto, N.; Santos, C.; dos Santos, S.E.B.; Amorim, A.; Carracedo, Á.; Gusmão, L. Straightforward Inference of Ancestry and Admixture Proportions through Ancestry-Informative Insertion Deletion Multiplexing. PLoS ONE 2012, 7, e29684. [Google Scholar] [CrossRef] [PubMed]
- Manta, F.S.D.N.; Pereira, R.; Vianna, R.; De Araújo, A.R.B.; Gitaí, D.; Silva, D.; Wolfgramm, E.D.V.; Pontes, I.D.M.; Aguiar, J.I.; Moraes, M.O.; et al. Revisiting the Genetic Ancestry of Brazilians Using Autosomal AIM-Indels. PLoS ONE 2013, 8, e75145. [Google Scholar] [CrossRef]
- American Diabetes Association. 10. Cardiovascular Disease and Risk Management: Standards of Medical Care in Diabetes—2021. Diabetes Care 2020, 44, S125–S150. [Google Scholar] [CrossRef]
- Cosentino, F.; Grant, P.J.; Aboyans, V.; Bailey, C.J.; Ceriello, A.; Delgado, V.; Federici, M.; Filippatos, G.; Grobbee, D.E.; Hansen, T.B.; et al. 2019 ESC Guidelines on diabetes, pre-diabetes, and cardiovascular diseases developed in collaboration with the EASD. Eur. Heart J. 2020, 41, 255–323. [Google Scholar] [CrossRef]
- Detrano, R.; Guerci, A.D.; Carr, J.J.; Bild, D.E.; Burke, G.L.; Folsom, A.R.; Liu, K.; Shea, S.; Szklo, M.; Bluemke, D.A.; et al. Coronary Calcium as a Predictor of Coronary Events in Four Racial or Ethnic Groups. N. Engl. J. Med. 2008, 358, 1336–1345. [Google Scholar] [CrossRef]
- Felício, J.S.; Koury, C.C.; Zahalan, N.A.; Resende, F.D.S.; de Lemos, M.N.; Pinto, R.J.D.M.C.; Neto, N.J.K.D.S.; de Franco, I.I.F.; de Oliveira, M.C.N.I.; de Alcântara, A.L.; et al. Ankle-brachial index and peripheral arterial disease: An evaluation including a type 2 diabetes mellitus drug-naïve patients cohort. Diabetes Vasc. Dis. Res. 2019, 16, 344–350. [Google Scholar] [CrossRef] [PubMed]
- Chevtchouk, L.; Da Silva, M.H.S.; Nascimento, O.J.M.D. Ankle-brachial index and diabetic neuropathy: Study of 225 patients. Arq. Neuro-Psiquiatr. 2017, 75, 533–538. [Google Scholar] [CrossRef] [PubMed]
- Nattero-Chávez, L.; López, S.R.; Díaz, S.A.; Ureña, M.G.; Fernández-Durán, E.; Escobar-Morreale, H.F.; Luque-Ramírez, M. The peripheral atherosclerotic profile in patients with type 1 diabetes warrants a thorough vascular assessment of asymptomatic patients. Diabetes/Metab. Res. Rev. 2018, 35, e3088. [Google Scholar] [CrossRef] [PubMed]
- Wang, F.M.; Yang, C.; Ballew, S.H.; Kalbaugh, C.A.; Meyer, M.L.; Tanaka, H.; Heiss, G.; Allison, M.; Salameh, M.; Coresh, J.; et al. Ankle-brachial index and subsequent risk of incident and recurrent cardiovascular events in older adults: The Atherosclerosis Risk in Communities (ARIC) study. Atherosclerosis 2021, 336, 39–47. [Google Scholar] [CrossRef]
- Giannopoulou, E.Z.; Doundoulakis, I.; Antza, C.; Christoforidis, A.; Haidich, A.B.; Kotsis, V.; Stabouli, S. Subclinical arterial damage in children and adolescents with type 1 diabetes: A systematic review and meta-analysis. Pediatr. Diabetes 2019, 20, 668–677. [Google Scholar] [CrossRef]
- Wang, P.; Xu, Y.-Y.; Lv, T.-T.; Guan, S.-Y.; Li, X.-M.; Li, X.-P.; Pan, H.-F. Subclinical Atherosclerosis in Patients With Type 1 Diabetes Mellitus: A Systematic Review and Meta-Analysis. Angiology 2018, 70, 141–159. [Google Scholar] [CrossRef]
- De Andrade, C.R.M.; Silva, E.L.C.; Matta, M.D.F.B.D.; Castier, M.B.; Rosa, M.L.G.; Gomes, M.D.B. Influence of a family history of type 2 diabetes, demographic and clinical data on carotid intima-media thickness in patients with type 1 diabetes: A cross-sectional study. Cardiovasc. Diabetol. 2014, 13, 87. [Google Scholar] [CrossRef]
- Burge, M.R.; Eaton, R.P.; Schade, D.S. The Role of a Coronary Artery Calcium Scan in Type 1 Diabetes. Diabetes Technol. Ther. 2016, 18, 594–603. [Google Scholar] [CrossRef]
- Aguilera, E.; Serra-Planas, E.; Granada, M.L.; Alonso, N.; Pellitero, S.; Pizarro, E.; Reverter, J.L.; Salinas, I.; Soldevila, B.; Mauricio, D.; et al. Low Prevalence of Subclinical Atherosclerosis in Asymptomatic Patients With Type 1 Diabetes in a European Mediterranean Population. Diabetes Care 2014, 37, 814–820. [Google Scholar] [CrossRef][Green Version]
- Mortensen, M.B.; Gaur, S.; Frimmer, A.; Bøtker, H.E.; Sørensen, H.T.; Kragholm, K.H.; Peter, S.R.N.; Steffensen, F.H.; Jensen, R.V.; Mæng, M.; et al. Association of Age With the Diagnostic Value of Coronary Artery Calcium Score for Ruling Out Coronary Stenosis in Symptomatic Patients. JAMA Cardiol. 2021. [Google Scholar] [CrossRef]
- Costacou, T.; Edmundowicz, D.; Prince, C.; Conway, B.; Orchard, T.J. Progression of Coronary Artery Calcium in Type 1 Diabetes Mellitus. Am. J. Cardiol. 2007, 100, 1543–1547. [Google Scholar] [CrossRef] [PubMed]
- Diabetes Control and Complications Trial Research Group; Nathan, D.M.; Genuth, S.; Lachin, J.; Cleary, P.; Crofford, O.; Davis, M.; Rand, L.; Siebert, C. The effect of intesive treatment of diabetes on the development and progression od long term complications in insulin-dependent diabetes mellitus. N. Engl. J. Med. 1993, 329, 977–986. [Google Scholar] [PubMed]
- Nathan, D.M.; Cleary, P.A.; Backlund, J.-Y.C.; Genuth, S.M.; Lachin, J.; Orchard, T.; Raskin, P.; Zinman, B.; Diabetes Control and Complications Trial/Epidemiology of Diabetes Interventions and Complications (DCCT/EDIC) Study Research Group. Intensive Diabetes Treatment and Cardiovascular Disease in Patients with Type 1 Diabetes. N. Engl. J. Med. 2005, 353, 2643–2653. [Google Scholar] [CrossRef] [PubMed]
- Azulay, R.S.D.S.; Porto, L.C.; Silva, D.A.; Tavares, M.D.G.; Reis, R.M.D.F.; Nascimento, G.C.; Damianse, S.D.S.P.; Rocha, V.C.D.C.; Magalhães, M.; Rodrigues, V.; et al. Genetic ancestry inferred from autosomal and Y chromosome markers and HLA genotypes in Type 1 Diabetes from an admixed Brazilian population. Sci. Rep. 2021, 11, 14157. [Google Scholar] [CrossRef]
- Santos, D.C.; De Melo, L.G.N.; Pizarro, M.H.; Barros, B.S.V.; Negrato, C.A.; Porto, L.C.; Silva, D.A.; Drummond, K.R.G.; Muniz, L.H.; Mattos, T.C.L.; et al. Genomic ancestry as a risk factor for dia-betic retinopathy in patients with type 1 diabetes from an admixed population: A nested case–control study in Brazil. Acta Diabetol 2020, 57, 937–945. [Google Scholar] [CrossRef]
- Gaillard, T. Consequences of Abdominal Adiposity within the Metabolic Syndrome Paradigm in Black People of African An-cestry. J. Clin. Med. 2014, 3, 897–912. [Google Scholar] [CrossRef]
- Bidulescu, A.; Choudhry, S.; Musani, S.K.; Buxbaum, S.G.; Liu, J.; Rotimi, C.N.; Wilson, J.G.; Taylor, H.A.; Gibbons, G.H. Associations of adiponectin with individual European ancestry in African Americans: The Jackson Heart Study. Front. Genet. 2014, 5, 22. [Google Scholar] [CrossRef]
- Barros, B.S.V.; Santos, D.C.; Melo, L.G.N.; Pizarro, M.H.; Muniz, L.H.; Silva, D.A.; Porto, L.C.; Gomes, M.B. Genomic ancestry and metabolic syndrome in individuals with type 1 diabetes from an admixed population: A multicentre, cross-sectional study in Brazil. Diabet. Med. 2020, 38, e14400. [Google Scholar] [CrossRef]
- Gomes, M.B.; Calliari, L.E.; Santos, D.C.; Muniz, L.H.; Porto, L.C.; Silva, D.A.; Negrato, C.A. Genomic ancestry and glycemic control in adolescents with type 1 diabetes: A multicenter study in Brazil. Pediatr. Diabetes 2020, 21, 727–734. [Google Scholar] [CrossRef]
- Pizarro, M.H.; Santos, D.C.; Melo, L.G.N.; Barros, B.S.V.; Muniz, L.H.; Porto, L.C.; Silva, D.A.; Gomes, M. Influence of genomic ancestry and self-reported color-race in CKD in a nationwide admixed sample of Brazilian patients with type 1 diabetes. Diabetes Metab. Syndr. Obes. Targets Ther. 2019, 12, 1831–1840. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | n (%) | Mean ± sd |
|---|---|---|
| Age (in years) | 27.6 ± 10.2 | |
| Sex | ||
| Female | 56 (55.6) | |
| Male | 43 (43.4) | |
| Anthropometric data | ||
| Body mass index (kg/m2) | 22.5 ± 3.8 | |
| Abdominal circumference in female group (cm) | 82.1 ± 13.8 | |
| Abdominal circumference in male group (cm) | 89.1 ± 8.5 | |
| Autosomal ancestry proportions | ||
| Amerindian | 24.7 ± 9.4 | |
| European | 47.3 ± 14.1 | |
| African | 28.0 ± 12.6 | |
| Arterial pressure | ||
| Systolic blood pressure (mmHg) | 116.4 ± 15.5 | |
| Diastolic blood pressure (mmHg) | 74.1 ± 10.4 | |
| Diabetes data | ||
| Age at T1D Diagnosis (years) | 14.4 ± 8.4 | |
| Duration of diabetes (years) | 13.2 ± 8.3 | |
| Fasting glucose (mg/dL) | 188.3 ± 108.1 | |
| HbA1c (%) | 8.9 ± 2.2 | |
| Microalbuminuria | ||
| <30 mg/dL | 81 (81.8) | |
| ≥30 mg/dL | 17 (17.2) | |
| No data | 1 (1.0) | |
| Retinopathy | ||
| Absent | 72 (72.7) | |
| Present | 27 (27.3) | |
| Creatinine clearance | ||
| ≥60 mL/min | 95 (95.9) | |
| <60 mL/min | 4 (4.1) | |
| Serum data | ||
| LDL cholesterol (mg/dL) | 96.9 ± 31.7 | |
| HDL cholesterol (mg/dL) | 54.0 ± 13.5 | |
| Triglyceride (mg/dL) | 104.6 ± 65.7 | |
| Creatinine (mg/dL) | 0.86 ± 0.64 | |
| Urea (mg/dL) | 28.8 ± 13.2 | |
| hs-CRP (mg/L) | 0.25 ± 0.38 |
| Variables | n | (%) |
|---|---|---|
| Coronary artery calcium score | ||
| Normal | 92 | (92.9) |
| Abnormal | 4 | (4.1) |
| No data | 3 | (3.0) |
| Carotid Doppler sonography | ||
| Normal | 88 | (88.9) |
| Abnormal | 5 | (5.0) |
| No data | 6 | (6.1) |
| Ankle–brachial index | ||
| Normal | 60 | (60.6) |
| Abnormal | 19 | (19.2) |
| No data | 20 | (20.2) |
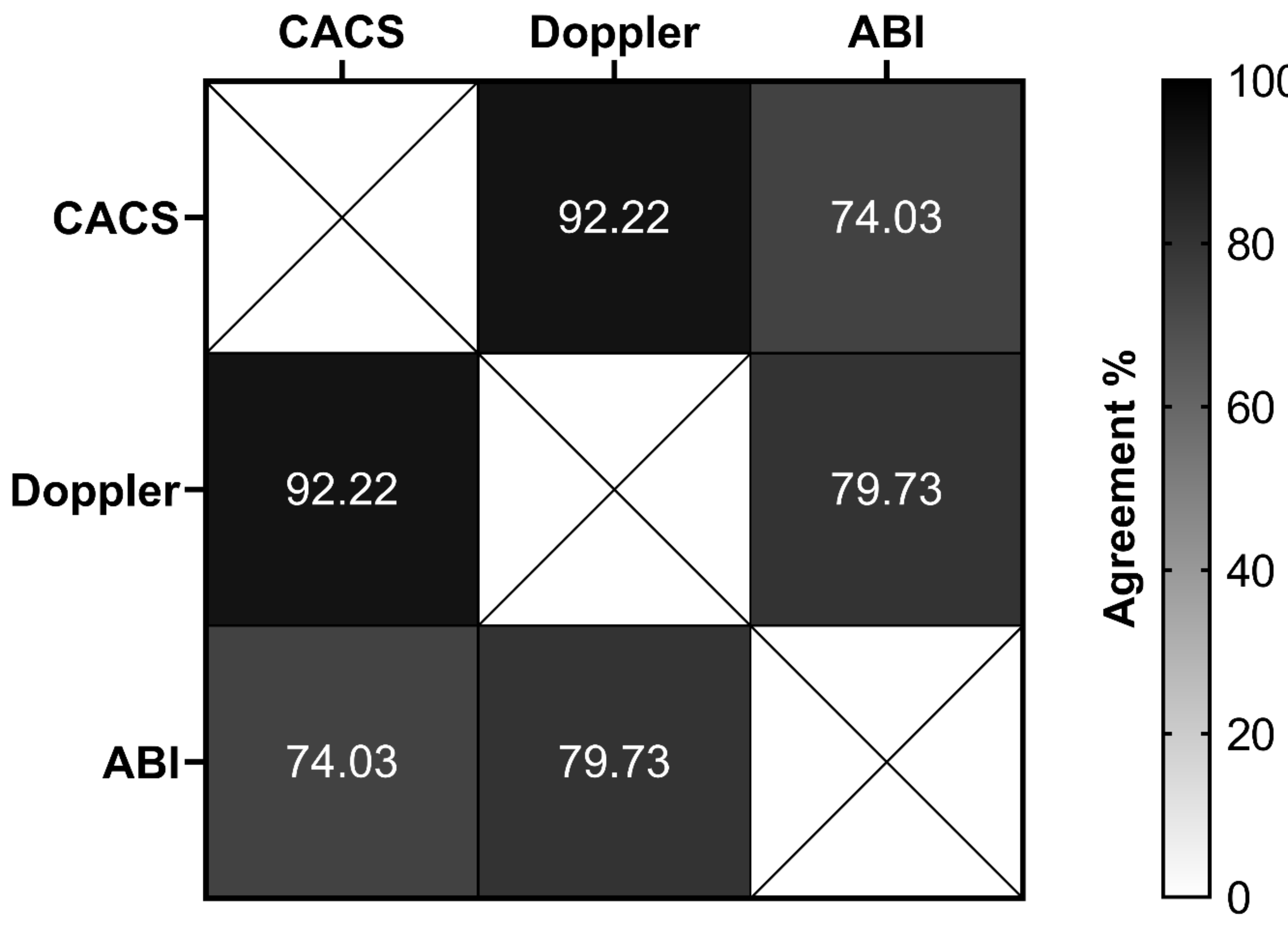
| Variables | Cardiovascular Abnormalities Detected by | |||||
|---|---|---|---|---|---|---|
| CACS | p Value | Doppler | p Value | ABI | p Value | |
| % | % | % | ||||
| Gender (Sex) | 1.000 | 0.373 | 0.116 | |||
| Female | 3.8 | 7.8 | 30.4 | |||
| Male | 4.7 | 2.4 | 15.2 | |||
| Microalbuminuria | 0.017 * | 0.540 | 1.000 | |||
| <30 mg/dL | 1.3 | 3.9 | 23.4 | |||
| ≥30 mg/dL | 17.7 | 6.3 | 21.4 | |||
| Retinopathy | 1.000 | 0.020 * | 0.786 | |||
| Absent | 4.3 | 1.5 | 23.2 | |||
| Present | 3.7 | 15.4 | 26.1 | |||
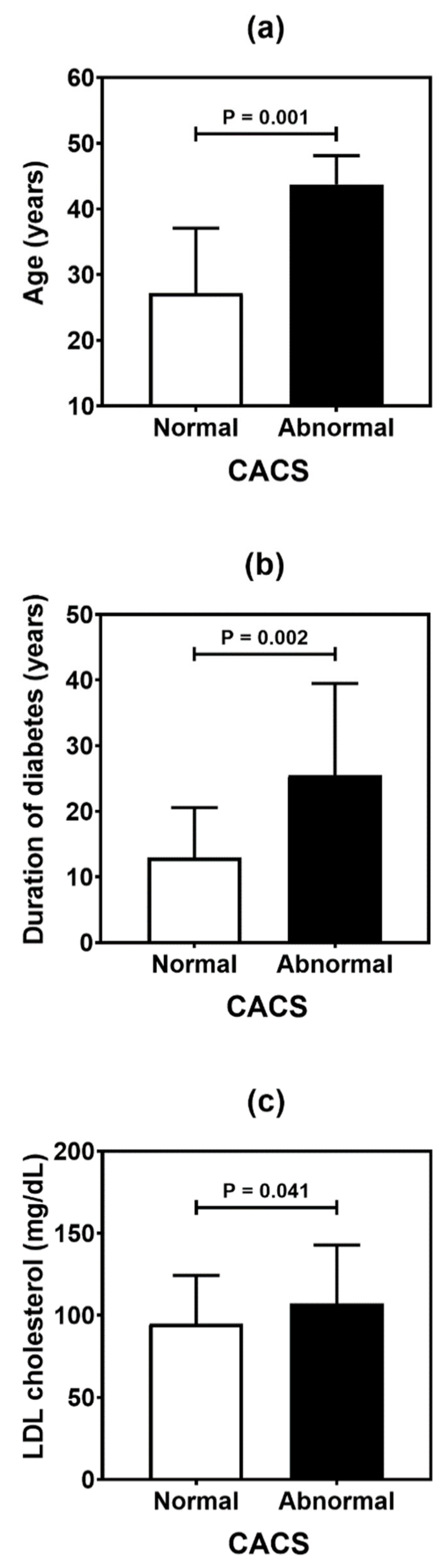
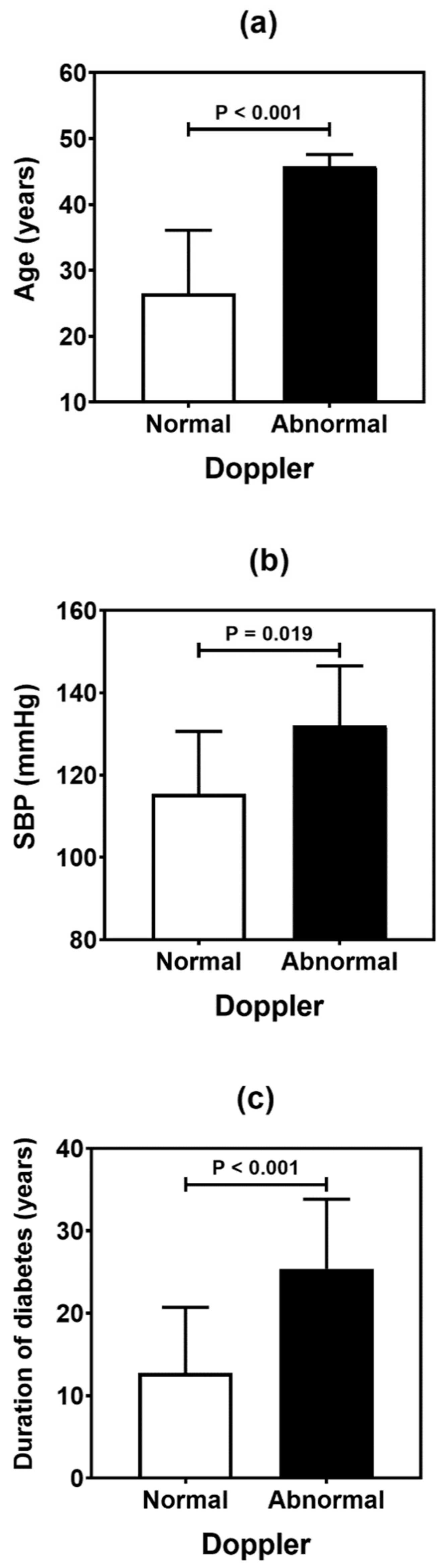
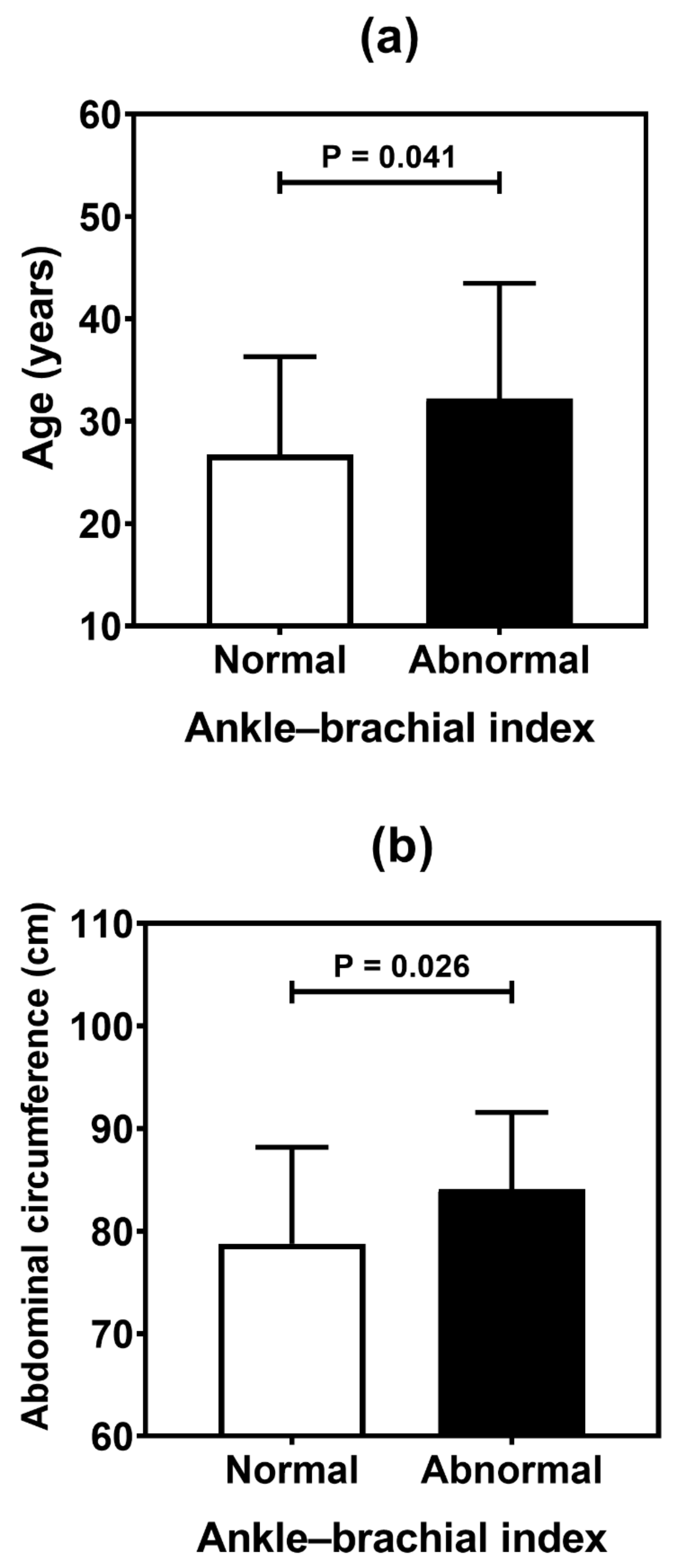
| Variables | Cardiovascular Abnormalities | ||
|---|---|---|---|
| CACS | Doppler | ABI | |
| p Value | p Value | p Value | |
| Age | 0.001 * | <0.001 * | 0.041 * |
| Anthropometric data | |||
| Body mass index | 0.268 | 0.154 | 0.518 |
| Abdominal circumference | 0.256 | 0.052 | 0.026 * |
| Arterial pressure | |||
| Systolic blood pressure | 0.160 | 0.019 * | 0.570 |
| Diastolic blood pressure | 0.351 | 0.164 | 0.629 |
| Diabetes data | |||
| Age at T1D diagnosis | 0.299 | 0.111 | 0.145 |
| Duration of diabetes | 0.002 * | <0.001 * | 0.172 |
| Fasting glucose | 0.278 | 0.916 | 0.571 |
| HbA1c (%) | 0.637 | 0.608 | 0.716 |
| Serum data | |||
| LDL cholesterol | 0.041 * | 0.222 | 0.639 |
| HDL cholesterol | 0.948 | 0.557 | 0.138 |
| Triglyceride | 0.750 | 0.979 | 0.976 |
| Creatinine | 0.873 | 0.553 | 0.395 |
| Urea | 0.729 | 0.361 | 0.989 |
| hs-CRP | 0.516 | 0.648 | 0.426 |
| Variables | Cardiovascular Abnormalities | ||
|---|---|---|---|
| CACS | Doppler | ABI | |
| p Value | p Value | p Value | |
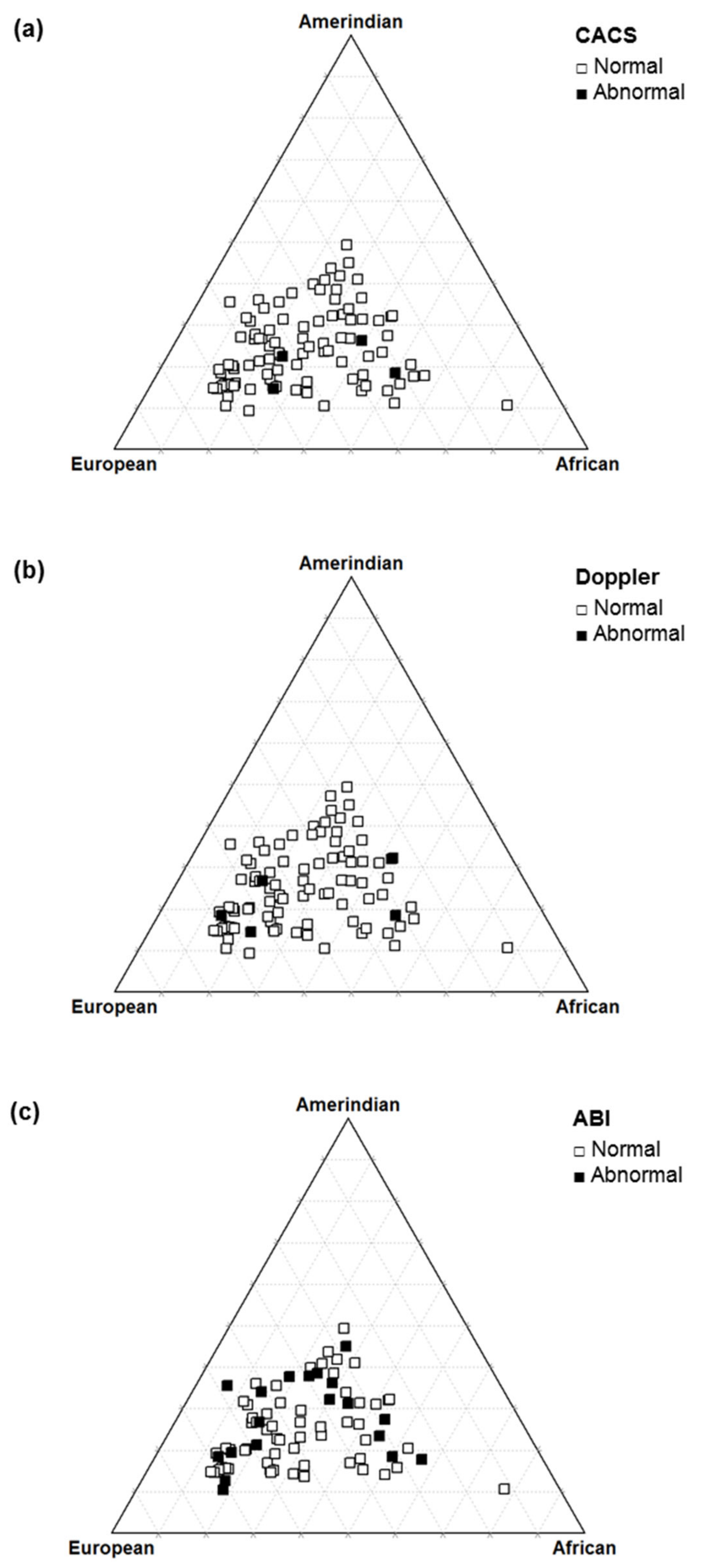
| Autosomal ancestry | |||
| Amerindian | 0.222 | 0.795 | 0.765 |
| European | 0.383 | 0.481 | 0.234 |
| African | 0.688 | 0.801 | 0.636 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Reis, R.M.D.F.; Azulay, R.S.d.S.; Tavares, M.d.G.; Nascimento, G.C.; Damianse, S.d.S.P.; Rocha, V.C.d.C.; Almeida, A.G.; Lago, D.C.F.; Rodrigues, V.; Magalhães, M.; et al. Early Markers of Cardiovascular Disease Associated with Clinical Data and Autosomal Ancestry in Patients with Type 1 Diabetes: A Cross-Sectional Study in an Admixed Brazilian Population. Genes 2022, 13, 389. https://doi.org/10.3390/genes13020389
Reis RMDF, Azulay RSdS, Tavares MdG, Nascimento GC, Damianse SdSP, Rocha VCdC, Almeida AG, Lago DCF, Rodrigues V, Magalhães M, et al. Early Markers of Cardiovascular Disease Associated with Clinical Data and Autosomal Ancestry in Patients with Type 1 Diabetes: A Cross-Sectional Study in an Admixed Brazilian Population. Genes. 2022; 13(2):389. https://doi.org/10.3390/genes13020389
Chicago/Turabian StyleReis, Roberta Maria Duailibe Ferreira, Rossana Santiago de Sousa Azulay, Maria da Glória Tavares, Gilvan Cortês Nascimento, Sabrina da Silva Pereira Damianse, Viviane Chaves de Carvalho Rocha, Ana Gregória Almeida, Débora Cristina Ferreira Lago, Vandilson Rodrigues, Marcelo Magalhães, and et al. 2022. "Early Markers of Cardiovascular Disease Associated with Clinical Data and Autosomal Ancestry in Patients with Type 1 Diabetes: A Cross-Sectional Study in an Admixed Brazilian Population" Genes 13, no. 2: 389. https://doi.org/10.3390/genes13020389
APA StyleReis, R. M. D. F., Azulay, R. S. d. S., Tavares, M. d. G., Nascimento, G. C., Damianse, S. d. S. P., Rocha, V. C. d. C., Almeida, A. G., Lago, D. C. F., Rodrigues, V., Magalhães, M., Sobral, C. S., Parente, C., França, J., Ribeiro, J., Ferraz, P. C. D., Junior, C. A. A., Silva, D. A., Gomes, M. B., & Faria, M. d. S. (2022). Early Markers of Cardiovascular Disease Associated with Clinical Data and Autosomal Ancestry in Patients with Type 1 Diabetes: A Cross-Sectional Study in an Admixed Brazilian Population. Genes, 13(2), 389. https://doi.org/10.3390/genes13020389