
Clinical, Histological, Cytogenetic and Molecular Analysis of Monozygous Twins with Wilms Tumor

 , , ,
, , , {kind=link}
{kind=link}
Abstract
1. Introduction
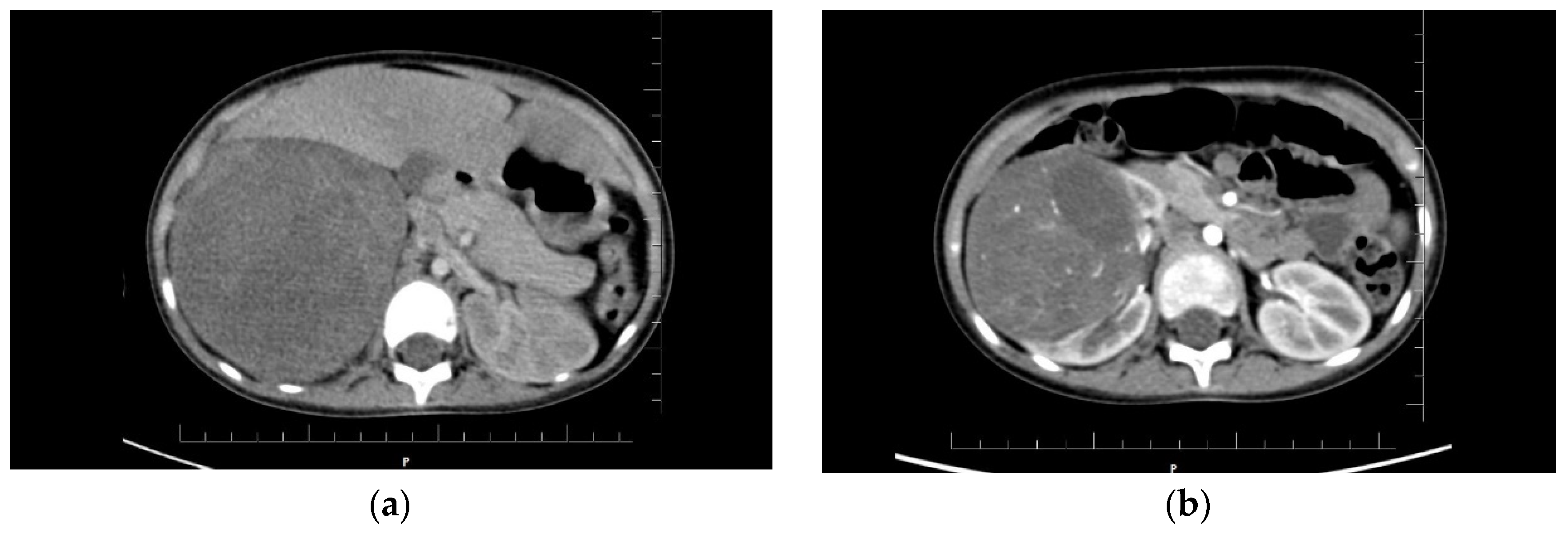
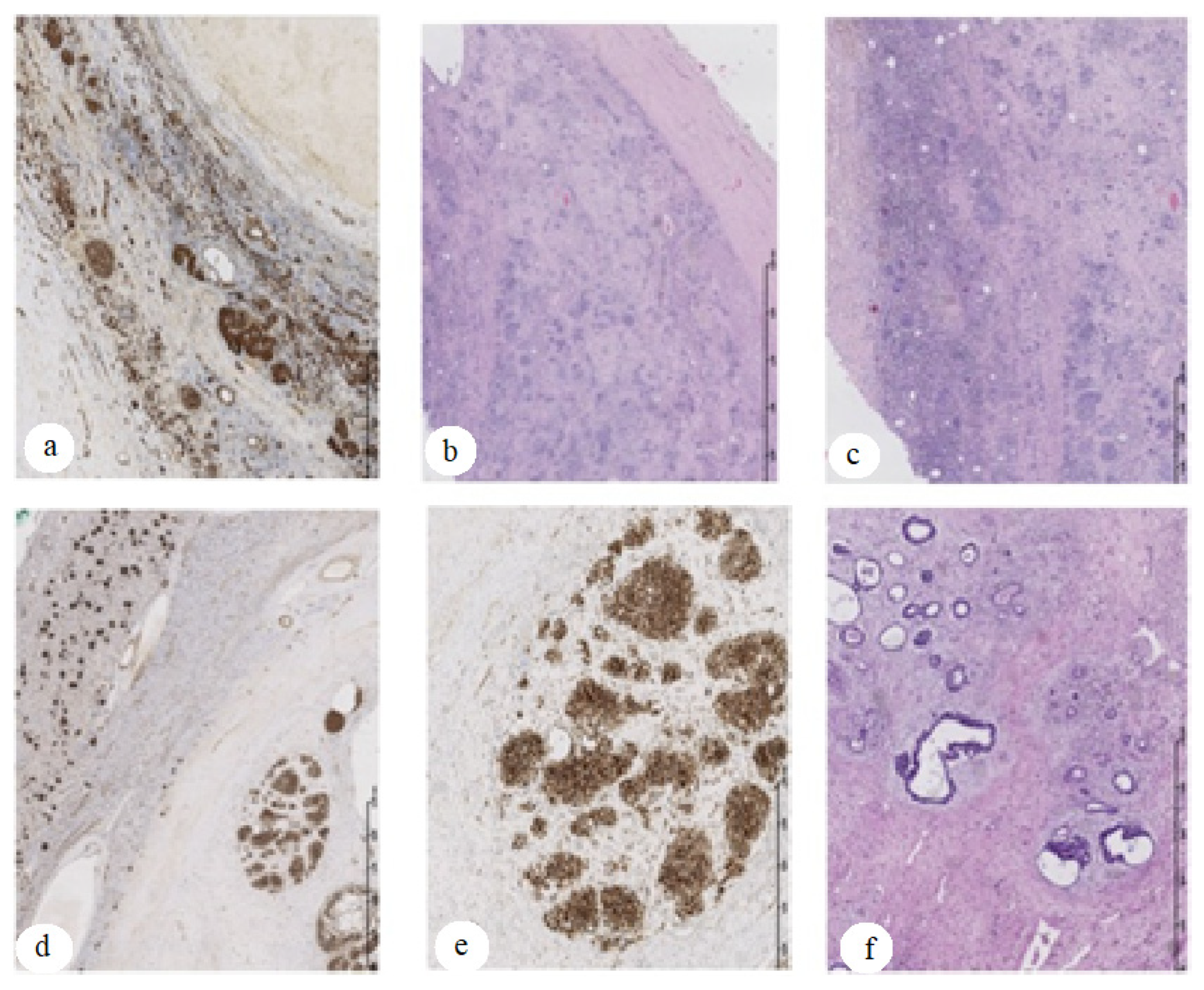
2. Case Report
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hewitt, D.; Lashof, J.C.; Stewart, A.M. Childhood cancers in twins. Cancer 1966, 19, 157–161. [Google Scholar] [CrossRef]
- Li, X.; Sun, N.; Huang, X.; Ju, X. Two pairs of monozygotic twins with concordant acute lymphoblastic leukemia (ALL): Case report. J. Pediatric Hematol. Oncol. 2014, 36, 299–303. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Kim, U.; Abraham, A.; Thirumalairaj, K.; Gaikwad, N.; Muthukkaruppan, V.; Reddy, A.G.; Thangaraj, K.; Vanniarajan, A. Retinoblastoma discordance in families with twins. Indian J. Ophthalmol. 2019, 67, 436–439. [Google Scholar] [CrossRef] [PubMed]
- Afshar, M.; Golden, C. Report of neuroblastoma in a set of monozygotic monochorionic twins. Pediatr. Hematol. Oncol. 2013, 30, 285–287. [Google Scholar] [CrossRef]
- Mahamdallie, S.; Yost, S.; Poyastro-Pearson, E.; Holt, E.; Zachariou, A.; Seal, S.; Elliott, A.; Clarke, M.; Warren-Perry, M.; Hanks, S.; et al. Identification of new Wilms tumor predisposition genes: An exome sequencing study. Lancet Child Adolesc. Health 2019, 3, 322–331. [Google Scholar] [CrossRef]
- Puumala, S.E.; Carozza, S.E.; Chow, E.; Fox, E.E.; Horel, S.; Johnson, K.J.; McLaughlin, C.; Mueller, B.A.; Reynolds, P.; Von Behren, J.; et al. Childhood cancer among twins and higher order multiples. Cancer Epidemiol. Biomark. Prev. 2009, 18, 162–168. [Google Scholar] [CrossRef]
- Gaulin, E. Simultaneous Wilms’ tumors in identical twins. J. Urol. 1951, 66, 547–550. [Google Scholar] [CrossRef]
- Svane, S. Simultaneous Wilms’ tumors in monozygotic twins: Case report and review of the literature. Scand. J. Urol. Nephrol. 1997, 31, 297–298. [Google Scholar] [CrossRef]
- Perotti, D.; De Vecchi, G.; Lualdi, E.; Testi, M.A.; Sozzi, G.; Collini, P.; Spreafico, F.; Terenziani, M.; Fossati-Bellani, F.; Radice, P. Wilms tumor in monozygous twins: Clinical, pathogical, cytogenetic and molecular case report. J. Pediatric Hematol. Oncol. 2005, 27, 521–525. [Google Scholar] [CrossRef]
- Cochran, W.; Frogatt, P. Bilateral nephroblastoma in two sisters. J. Urol. 1967, 97, 216–220. [Google Scholar] [CrossRef]
- Begum, Z.; Sharieff, S.; Attar, A. Familial occurance of nonsyndromic Wilms tumor—A report in two siblings. Indian J. Surg. 2013, 75, 99–102. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Dome, J.; Graf, N.; Geller, J.; Fernandez, C.; Mullen, E.; Spreafico, F.; van den Heuvel-Eibrink, M.; Pritchard-Jones, K. Advances in Wilms tumor treatment and biology: Progress through international collaboration. J. Clin. Oncol. 2015, 33, 2999–3007. [Google Scholar] [CrossRef] [PubMed]
- van den Heuvel-Eibrink, M.; Hol, J.; Pritchard-Jones, K.; van Tinteren, H.; Furtwängler, R.; Verschuur, A.C.; Vujanic, G.M.; Leuschner, I.; Brok, J.; Rübe, C.; et al. Rationale for the treatment of Wilms tumor in the UMBRELLA SIOP–RTSG 2016 protocol. Nat. Rev. Urol. 2017, 14, 743–752. [Google Scholar] [CrossRef]
- Juberg, R.C.; St Martin, E.C.; Hundley, J.R. Familial occurrence of Wilms’ tumor: Nephroblastoma in one of monozygous twins and in another sibling. Am. J. Hum. Genet. 1975, 27, 155–164. [Google Scholar] [PubMed]
- Olson, J.M.; Breslow, N.E.; Barce, J. Cancer in twins of Wilms’ tumor patients. Am. J. Med. Genet. 1993, 47, 91–94. [Google Scholar] [CrossRef] [PubMed]
- Maurer, H.S.; Pendergrass, T.W.; Borges, W.; Honig, G.R. The role of genetic factors in the etiology of Wilms’ tumor. Cancer 1979, 43, 205–208. [Google Scholar] [CrossRef]
- Royer-Pokora, B.; Beier, M.; Henzler, M.; Alam, R.; Weirich, A.; Huff, V. Twenty-four new cases of WT1 germline mutations and review of the literature: Genotype/phenotype correlations for Wilms tumor development. Am. J. Med. Genet. 2004, 127A, 249–257. [Google Scholar] [CrossRef]
- Little, S.E.; Hanks, S.P.; King-Underwood, L.; Jones, C.; Rapley, E.A.; Rahman, N.; Pritchard-Jones, K. Frequency and heritability of WT1 mutations in nonsyndromic Wilms’ tumor patients: A UK Children’s Cancer Study Group Study. J. Clin. Oncol. 2004, 22, 4140–4146. [Google Scholar] [CrossRef]
- Scott, R.; Stiller, C.; Walker, L.; Rahman, N. Syndromes and constitutional chromosomal abnormalities associated with Wilms tumor. J. Med. Genet. 2006, 43, 705–715. [Google Scholar] [CrossRef]
- Shatara, M.; Xavier, A.C.; Dombkowski, A.; Cukovic, D.; Poulik, J.M.; Altinok, D.; Ge, Y.; Taub, J.W. Monozygotic twin with neuroblastoma MS have a similar molecular profile: A case of twin-to-twin metastasis. Br. J. Cancer. 2019, 121, 890–893. [Google Scholar] [CrossRef]
- Tajiri, T.; Souzaki, R.; Kinoshita, Y.; Tanaka, S.; Koga, Y.; Suminoe, A.; Hara, T.; Kohashi, K.; Oda, Y.; Masumoto, K.; et al. Concordance for neuroblastoma in monozygotic twins: Case report and review of the literature. J. Pediatr. Surg. 2010, 45, 2312–2316. [Google Scholar] [CrossRef] [PubMed]
- Rios, P.; Bauer, H.; Schleiermacher, G.; Pasqualini, C.; Boulanger, C.; Thebaud, E.; Gandemer, V.; Pellier, I.; Verschuur, A.; Sudour-Bonnange, H.; et al. Environmental exposures related to parental habits in the perinatal period and the risk of Wilms’ tumor in children. Cancer Epidemiol. 2020, 66, 101706. [Google Scholar] [CrossRef] [PubMed]
- Cooney, M.A.; Daniels, J.L.; Ross, J.A.; Breslow, N.E.; Pollock, B.H.; Olshan, A.F. Household pesticides and the risk of Wilms tumor. Environ. Health Perspect. 2007, 115, 134–137. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Chu, A.; Heck, J.; Ribeiro, K.B.; Brennan, P.; Boffetta, P.; Buffler, P.; Hung, R.J. Wilms’ tumor: A systematic review of risk factors and meta-analysis. Paediatr. Perinat. Epidemiol. 2010, 24, 449–469. [Google Scholar] [CrossRef]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Iwańczyk, K.; Czachowski, B.; Sosnowska-Sienkiewicz, P.; Telman, G.; Ciążyńska, P.; Mańkowski, P.; Januszkiewicz-Lewandowska, D. Clinical, Histological, Cytogenetic and Molecular Analysis of Monozygous Twins with Wilms Tumor. Genes 2022, 13, 372. https://doi.org/10.3390/genes13020372
Iwańczyk K, Czachowski B, Sosnowska-Sienkiewicz P, Telman G, Ciążyńska P, Mańkowski P, Januszkiewicz-Lewandowska D. Clinical, Histological, Cytogenetic and Molecular Analysis of Monozygous Twins with Wilms Tumor. Genes. 2022; 13(2):372. https://doi.org/10.3390/genes13020372
Chicago/Turabian StyleIwańczyk, Katarzyna, Bartosz Czachowski, Patrycja Sosnowska-Sienkiewicz, Gabriela Telman, Paulina Ciążyńska, Przemysław Mańkowski, and Danuta Januszkiewicz-Lewandowska. 2022. "Clinical, Histological, Cytogenetic and Molecular Analysis of Monozygous Twins with Wilms Tumor" Genes 13, no. 2: 372. https://doi.org/10.3390/genes13020372
APA StyleIwańczyk, K., Czachowski, B., Sosnowska-Sienkiewicz, P., Telman, G., Ciążyńska, P., Mańkowski, P., & Januszkiewicz-Lewandowska, D. (2022). Clinical, Histological, Cytogenetic and Molecular Analysis of Monozygous Twins with Wilms Tumor. Genes, 13(2), 372. https://doi.org/10.3390/genes13020372