
Cytogenetic Investigation of Infertile Patients in Hungary: A 10-Year Retrospective Study


Abstract
1. Introduction
2. Materials and Methods
3. Results
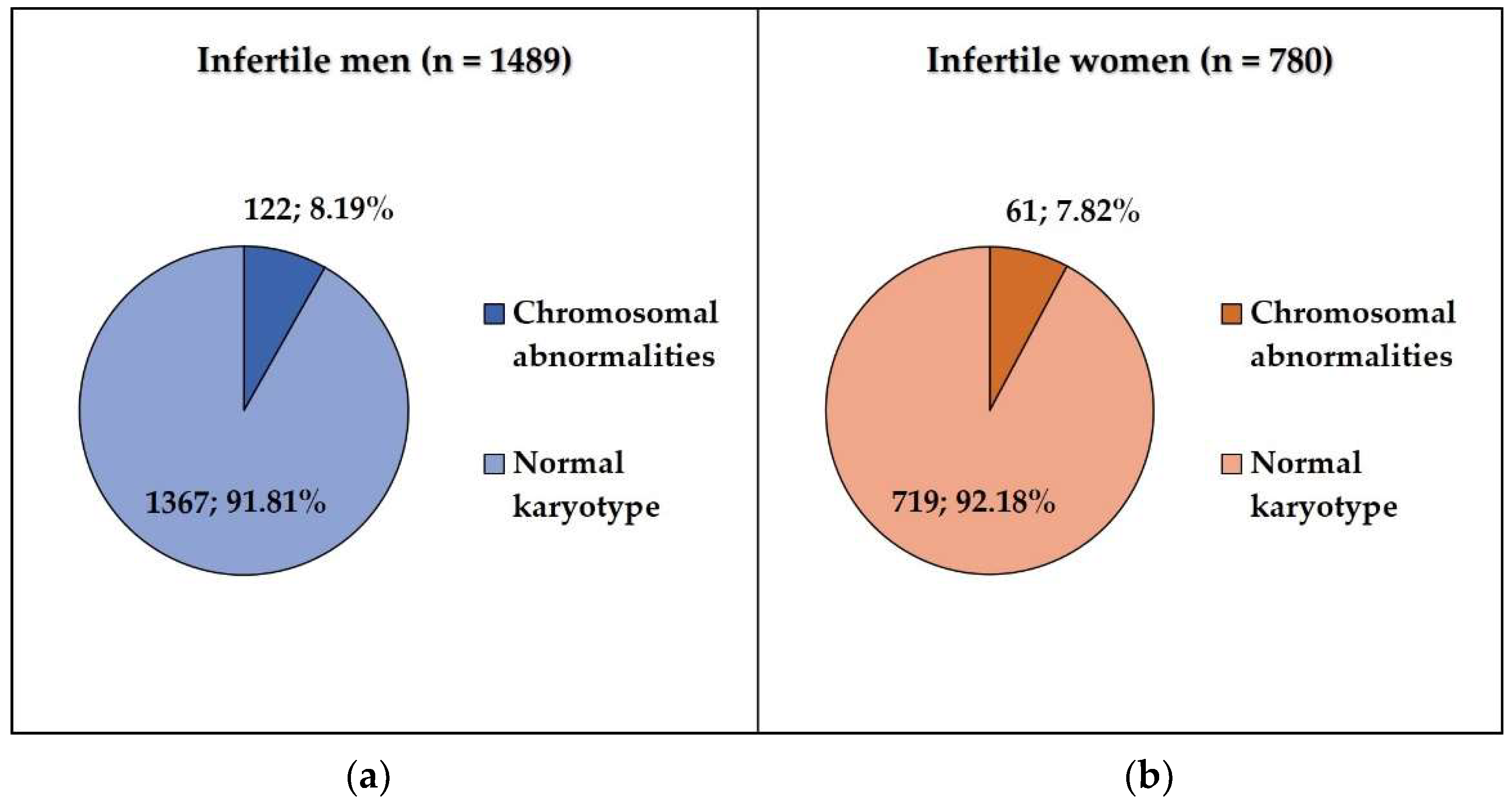
3.1. Infertile Men vs. Control Patients
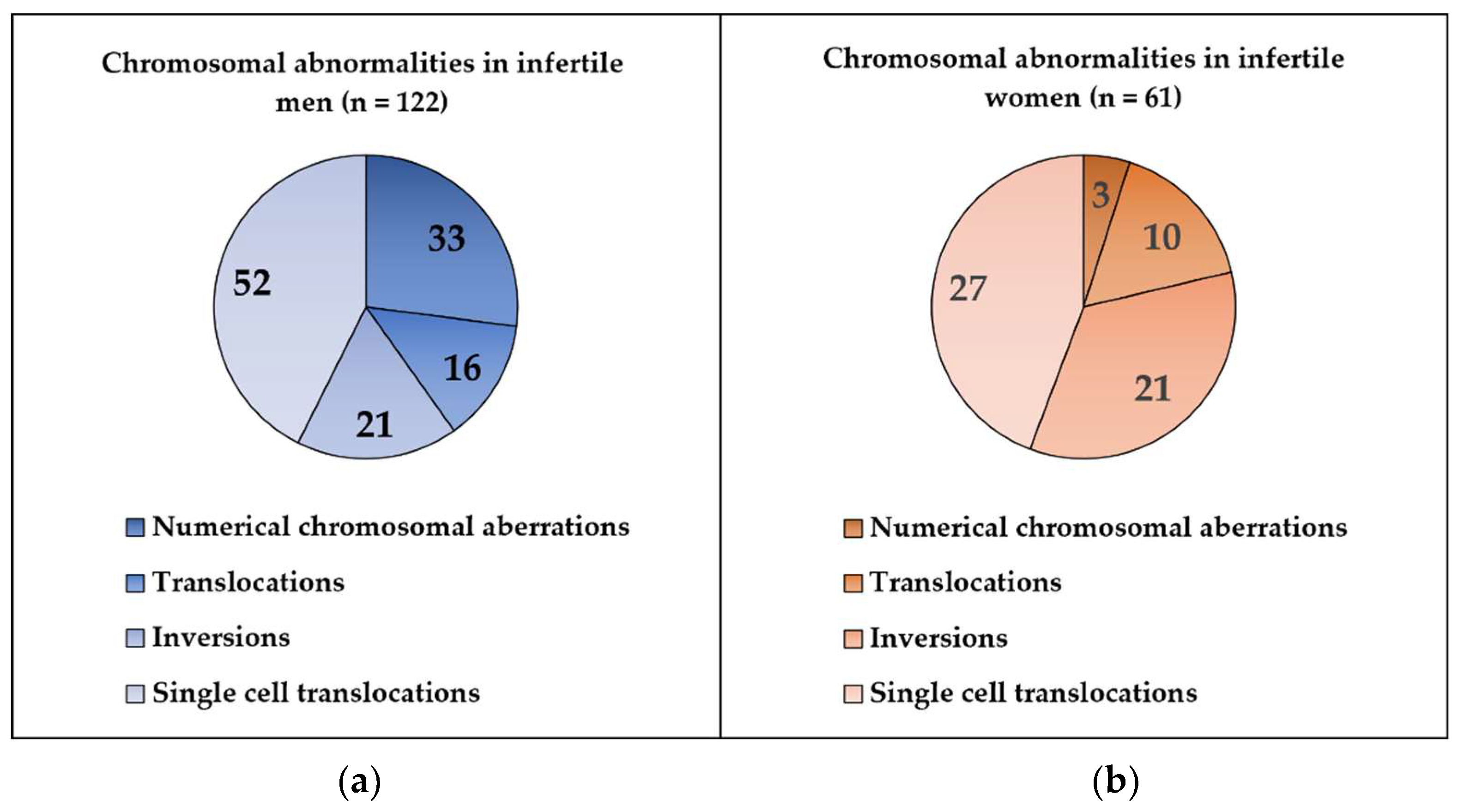
3.1.1. Numerical Chromosomal Aberrations
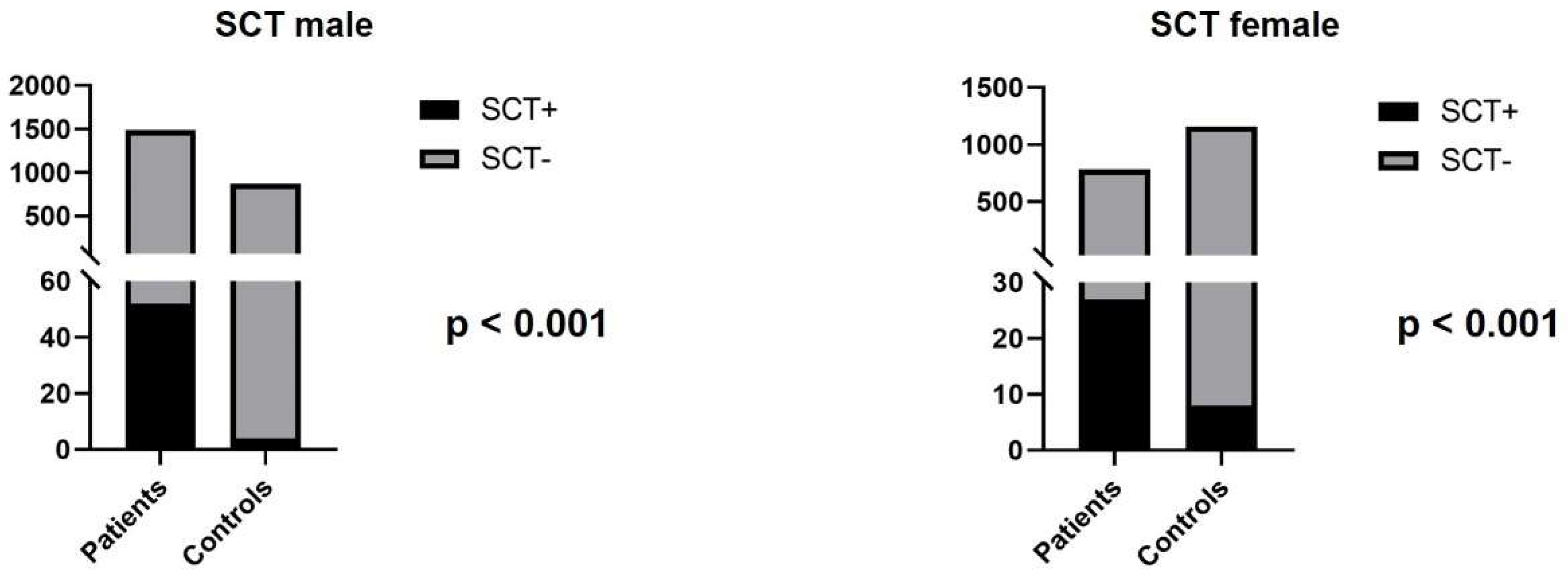
3.1.2. Structural Chromosomal Aberrations
3.2. Infertile vs. Control Women
3.2.1. Numerical Chromosomal Aberrations
3.2.2. Structural Chromosomal Aberrations
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kamel, R.M. Management of the infertile couple: An evidence-based protocol. Reprod. Biol. Endocrinol. 2010, 8, 21. [Google Scholar] [CrossRef] [PubMed]
- Dohle, G.R.; Colpi, G.M.; Hargreave, T.B.; Papp, G.K.; Jungwirth, A.; Weidner, W. EAU guidelines on male infertility. Eur. Urol. 2005, 48, 703–711. [Google Scholar] [CrossRef] [PubMed]
- Shah, K.; Sivapalan, G.; Gibbons, N.; Tempest, H.; Griffin, D.K. The genetic basis of infertility. Reproduction 2003, 126, 13–25. [Google Scholar] [CrossRef]
- Carson, S.A.; Kallen, A.N. Diagnosis and Management of Infertility. JAMA 2021, 326, 65–76. [Google Scholar] [CrossRef] [PubMed]
- Serapinas, D.; Valantinavičienė, E.; Machtejevienė, E.; Bartkevičiūtė, A.; Bartkevičienė, D. Evaluation of Chromosomal Structural Anomalies in Fertility Disorders. Medicina 2021, 57, 37. [Google Scholar] [CrossRef] [PubMed]
- Foresta, C.; Ferlin, A.; Gianaroli, L.; Dallapiccola, B. Guidelines for the appropriate use of genetic tests in infertile couples. Eur. J. Hum. Genet. 2002, 10, 303–312. [Google Scholar] [CrossRef]
- Bonomi, M.; Rochira, V.; Pasquali, D.; Balercia, G.; Jannini, E.A.; Ferlin, A. Klinefelter syndrome (KS): Genetics, clinical phenotype and hypogonadism. J. Endocrinol. Investig. 2017, 40, 123–134. [Google Scholar] [CrossRef]
- Park, S.-J.; Min, J.-Y.; Kang, J.-S.; Yang, B.-G.; Hwang, S.-Y.; Han, S.-H. Chromosomal abnormalities of 19,000 couples with recurrent spontaneous abortions: A multicenter study. Fertil. Steril. 2022, 117, 1015–1025. [Google Scholar] [CrossRef]
- Ferlin, A.; Raicu, F.; Gatta, V.; Zuccarello, D.; Palka, G.; Foresta, C. Male infertility: Role of genetic background. Reprod. Biomed. Online 2007, 14, 734–745. [Google Scholar] [CrossRef]
- Mozdarani, H.; Meybodi, A.M.; Karimi, H. Impact of pericentric inversion of Chromosome 9 [inv (9) (p11q12)] on infertility. Indian J. Hum. Genet. 2007, 13, 26–29. [Google Scholar] [CrossRef][Green Version]
- Elkarhat, Z.; Kindil, Z.; Zarouf, L.; Razoki, L.; Aboulfaraj, J.; Elbakay, C.; Nassereddine, S.; Nasser, B.; Barakat, A.; Rouba, H. Chromosomal abnormalities in couples with recurrent spontaneous miscarriage: A 21-year retrospective study, a report of a novel insertion, and a literature review. J. Assist. Reprod. Genet. 2019, 36, 499–507. [Google Scholar] [CrossRef] [PubMed]
- Šípek, A.; Mihalová, R.; Panczak, A.; Hrčková, L.; Janashia, M.; Kaspříková, N.; Kohoutová, M. Heterochromatin variants in human karyotypes: A possible association with reproductive failure. Reprod. Biomed. Online 2014, 29, 245–250. [Google Scholar] [CrossRef] [PubMed]
- Šípek, A.; Panczak, A.; Mihalová, R.; Hrčková, L.; Suttrová, E.; Sobotka, V.; Lonský, P.; Kaspříková, N.; Gregor, V. Pericentric Inversion of Human Chromosome 9 Epidemiology Study in Czech Males and Females. Folia Biol. 2015, 61, 140–146. [Google Scholar]
- Dana, M.; Stoian, V. Association of Pericentric Inversion of Chromosome 9 and Infertility in Romanian Population. Maedica 2012, 7, 25–29. [Google Scholar] [PubMed]
- Merrion, K.; Maisenbacher, M. Pericentric inversion (Inv) 9 variant-reproductive risk factor or benign finding? J. Assist. Reprod. Genet. 2019, 36, 2557–2561. [Google Scholar] [CrossRef]
- Sheth, F.; Pani, J.; Desai, M.; Mehta, S.; Sheth, J. Single Cell Abnormality in Couples with Bad Obstetric History and Repeated Fetal Loss: Occurrence and Clinical Outcome. Int. J. Hum. Genet. 2011, 11, 271–276. [Google Scholar] [CrossRef]
- Higgins, M.D.; Palmer, C.G. Single cell translocations in couples with multiple spontaneous abortions. Hum. Genet. 1987, 75, 24–27. [Google Scholar] [CrossRef]
- Velissariou, V.; Lyberatou, E.; Antonopoulou, E.; Polymilis, C. Chromosome breakage in individuals with single-cell structural aberrations and habitual abortions. Gynecol. Obstet. Investig. 1993, 36, 71–74. [Google Scholar] [CrossRef]
- Peschka, B.; Leygraaf, J.; Van Der Ven, K.; Montag, M.; Schartmann, B.; Schubert, R.; Van Der Ven, H.; Schwanitz, G. Type and frequency of chromosome aberrations in 781 couples undergoing intracytoplasmic sperm injection. Hum. Reprod. 1999, 14, 2257–2263. [Google Scholar] [CrossRef]
- Tarlatzis, B.C.; Toncheva, D.I.; Vatev, I.T. Significance of chromosomal aberrations for the unsuccessful procedures of assisted reproduction. Eur. J. Obstet. Gynecol. Reprod. Biol. 2000, 88, 181–187. [Google Scholar] [CrossRef]
- Devi, R.; Sayee, R. Isolated cell translocations: Are they significant? Indian J. Hum. Genet. 2015, 11, 105–107. [Google Scholar] [CrossRef][Green Version]
- Silva, M.; de Leeuw, N.; Mann, K.; Schuring-Blom, H.; Morgan, S.; Giardino, D.; Rack, K.; Hastings, R. European guidelines for constitutional cytogenomic analysis. Eur. J. Hum. Genet. 2019, 27, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Hook, E.B. Exclusion of chromosomal mosaicism: Tables of 90%, 95% and 99% confidence limits and comments on use. Am. J. Hum. Genet. 1977, 29, 94–97. [Google Scholar] [PubMed]
- Nakamura, Y.; Kitamura, M.; Nishimura, K.; Koga, M.; Kondoh, N.; Takeyama, M.; Matsumiya, K.; Okuyama, A. Chromosomal variants among 1790 infertile men. Int. J. Urol. 2001, 8, 49–52. [Google Scholar] [CrossRef]
- Poornima, S.; Daram, S.; Devaki, R.K.; Qurratulain, H. Chromosomal Abnormalities in Couples with Primary and Secondary Infertility: Genetic Counseling for Assisted Reproductive Techniques (ART). J. Reprod. Infertil. 2020, 21, 269–274. [Google Scholar] [CrossRef]
- Saxena, S.G.; Desai, K.; Shewale, L.; Ranjan, P.; Saranath, D. Chromosomal aberrations in 2000 couples of Indian ethnicity with reproductive failure. Reprod. Biomed. Online 2012, 25, 209–218. [Google Scholar] [CrossRef]
- Mackic-Djurovic, M.; Hasic, S.; Kiseljakovic, E.; Rukavina, D.; Ibrulj, S. Cytogenetic Abnormalities Found in Patients with Reproductive Problems. Med. Arch. 2017, 71, 396–399. [Google Scholar] [CrossRef]
- Pal, A.K.; Ambulkar, P.S.; Waghmare, J.E.; Wankhede, V.; Shende, M.R.; Tarnekar, A.M. Chromosomal Aberrations in Couples with Pregnancy Loss: A Retrospective Study. J. Hum. Reprod. Sci. 2018, 11, 247–253. [Google Scholar] [CrossRef]
- Gekas, J.; Thepot, F.; Turleau, C.; Siffroi, J.; Dadoune, J.; Briault, S.; Rio, M.; Bourouillou, G.; Carré-Pigeon, F.; Wasels, R.; et al. Chromosomal factors of infertility in candidate couples for ICSI: An equal risk of constitutional aberrations in women and men. Hum. Reprod. 2001, 16, 82–90. [Google Scholar] [CrossRef]
- Zachaki, S.; Kouvidi, E.; Pantou, A.; Tsarouha, H.; Mitrakos, A.; Tounta, G.; Charalampous, I.; Manola, K.N.; Kanavakis, E.; Mavrou, A. Low-level X Chromosome Mosaicism: A Common Finding in Women Undergoing IVF. In Vivo 2020, 34, 1433–1437. [Google Scholar] [CrossRef]
- Madan, K.; Lundberg, E. Low grade mosaicism for X aneuploidy in women referred for recurrent abortions. Eur. Cytogenet. Assoc. Newsl. 2015, 35, 9–12. [Google Scholar]
- Yue, F.; Zhang, H.; Xi, Q.; Jiang, Y.; Li, L.; Liu, R.; Wang, R. Molecular cytogenetic analysis and genetic counseling: A case report of eight 46,XX males and a literature review. Mol. Cytogenet. 2019, 12, 44. [Google Scholar] [CrossRef] [PubMed]
- Feuk, L. Inversion variants in the human genome: Role in disease and genome architecture. Genome Med. 2010, 2, 11. [Google Scholar] [CrossRef] [PubMed]
- Morel, F.; Laudier, B.; Guérif, F.; Couet, M.; Royère, D.; Roux, C.; Bresson, J.; Amice, V.; De Braekeleer, M.; Douet-Guilbert, N. Meiotic segregation analysis in spermatozoa of pericentric inversion carriers using fluorescence in-situ hybridization. Hum. Reprod. 2007, 22, 136–141. [Google Scholar] [CrossRef]
- Anton, E.; Garcia-Guixé, E.; Ramos-Muntada, M.; Godo, A.; Sandalinas, M.; Blanco, J. Chromosome heteromorphisms: Do they entail a reproductive risk for male carriers? Asian J. Androl. 2020, 22, 544–546. [Google Scholar] [CrossRef]
- Liehr, T.; Weise, A.; Mrasek, K.; Ziegler, M.; Padutsch, N.; Wilhelm, K.; Al-Rikabi, A. Recombinant Chromosomes Resulting From Parental Pericentric Inversions-Two New Cases and a Review of the Literature. Front. Genet. 2019, 10, 1165. [Google Scholar] [CrossRef]
- Young, D.; Klepacka, D.; McGarvey, M.; Schoolcraft, W.B.; Katz-Jaffe, M.G. Infertility patients with chromosome inversions are not susceptible to an inter-chromosomal effect. J. Assist. Reprod. Genet. 2019, 36, 509–516. [Google Scholar] [CrossRef]
- Mohsen-Pour, N.; Talebi, T.; Naderi, N.; Moghadam, M.H.; Maleki, M.; Kalayinia, S. Chromosome 9 Inversion: Pathogenic or Benign? A Comprehensive Systematic Review of all Clinical Reports. Curr. Mol. Med. 2022, 22, 385–400. [Google Scholar] [CrossRef]
- Garzo, M.; Catusi, I.; Colombo, D.M.; De Grada, L.; Recalcati, M.P.; Rodeschini, O.; Barone, C.; Beltrami, N.; Busuito, R.; Cappellani, S.; et al. Ten new cases of Balanced Reciprocal Translocation Mosaicism (BRTM): Reproductive implications, frequency and mechanism. Eur. J. Med. Genet. 2020, 63, 103639. [Google Scholar] [CrossRef]
- Arlt, M.F.; Durkin, S.G.; Ragland, R.L.; Glover, T.W. Common fragile sites as targets for chromosome rearrangements. DNA Repair 2006, 5, 1126–1135. [Google Scholar] [CrossRef]
- Manvelyan, M.; Schreyer, I.; Höls-Herpertz, I.; Köhler, S.; Niemann, R.; Hehr, U.; Belitz, B.; Bartels, I.; Götz, J.; Huhle, D.; et al. Forty-eight new cases with infertility due to balanced chromosomal rearrangements: Detailed molecular cytogenetic analysis of the 90 involved breakpoints. Int. J. Mol. Med. 2007, 19, 855–864. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Zech, L.; Haglund, U. A recurrent structural aberration, t(7;14), in phytohemagglutinin-stimulated lymphocytes. Hereditas 1978, 89, 69–73. [Google Scholar] [CrossRef] [PubMed]
- Wallace, C.; Bernstein, R.; Pinto, M.R. Non-random in vitro 7;14 translocations detected in a routine cytogenetic series. 12 examples and their possible significance. Hum. Genet. 1984, 66, 157–161. [Google Scholar] [CrossRef] [PubMed]
- Dewald, G.W.; Noonan, K.J.; Spurbeck, J.L.; Johnson, D.D. T-lymphocytes with 7;14 translocations: Frequency of occurrence, breakpoints, and clinical and biological significance. Am. J. Hum. Genet. 1986, 38, 520–532. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Type of Aberrations | Karyotype | No. of Cases | % | |
|---|---|---|---|---|
| Infertile Patients (n = 1489) | ||||
| DSD (46,XX male) | 46,XX | 1 | 0.07 | |
| Numerical chromosomal aberrations | 47,XXY | 28 | 1.88 | |
| 47,XXY[3]/46,XY[12] (n = 1); 47,XXY[10]/46,XY[5] (n = 1); 47,XXY[14]/46,XY[1] (n = 1) | 3 | 0.21 | ||
| 48,XXXY[1]/47,XXY[14] | 1 | 0.07 | ||
| Structural chromosomal aberrations | Translocations (n = 16; 1.07%) | 45,XY,rob(13;14)(q10;q10) | 4 | 0.28 |
| 45,XY,rob(14;21)(q10;q10) | 1 | 0.07 | ||
| 46,XY,t(2;5)(p21?;q31) | 1 | 0.07 | ||
| 46,XY,t(3;6)(q21;q23) | 1 | 0.07 | ||
| 46,XY,t(5;14)(q31;q11.2) | 1 | 0.07 | ||
| 46,XY,t(7;20)(p15;p13) | 1 | 0.07 | ||
| 46,XY,t(8;15)(p21;q26) | 1 | 0.07 | ||
| 46,XY,t(10;22)(q26;q13) | 1 | 0.07 | ||
| 46,XY,t(11;22)(q23;q11) | 1 | 0.07 | ||
| 46,Y,t(X;3)(p1?1.2;q2?7) | 1 | 0.07 | ||
| 46,XY,t(Y;3)(q12;q22?) | 1 | 0.07 | ||
| 46,XY,t(11;22)(q23.3;q11.2)[8]/46,XY[7] | 1 | 0.07 | ||
| 46,XY,t(14;19)(q24;q13)[5]/46,XY[10] | 1 | 0.07 | ||
| Inversions (n = 21; 1.41%) | 46,XY,inv(9)(p13q21) (n = 10); 46,XY,inv(9)(p12q13) (n = 6) | 16 | 1.07 | |
| 46,XY,inv(5)(q13q35) (n = 1); 46,XY,inv(5)(q31q33) (n = 1) | 2 | 0.14 | ||
| 46,XY,inv(16)(q11.2q22) | 1 | 0.07 | ||
| 46,XY,inv(10)(p11.2q21.2) | 1 | 0.07 | ||
| 46,XY,inv(12)(p13q12) | 1 | 0.07 | ||
| Single cell translocations | (Table 3.) | 52 | 3.5 | |
| Control group (n = 869) | ||||
| Structural chromosomal aberrations | Inversions | 46,XY,inv(9)(p12q13) (n = 12); 46,XY,inv(9)(p13q21) (n = 11) | 23 | 2.65 |
| Single cell translocations | (Table 3.) | 4 | 0.46 | |
| Type of Aberrations | Karyotype | No. of Cases | % | |
|---|---|---|---|---|
| Infertile Patients (n = 780) | ||||
| DSD (46,XY female) | 46,XY | 1 | 0.13 | |
| Numerical chromosomal aberrations | 45,X[2]/46,XX[13] (n = 1); 45,X[1]/46,XX[14] (n = 1) | 2 | 0.26 | |
| Structural chromosomal aberrations | Translocations (n = 10; 1.28%) | 45,XX,rob(13;14)(q10;q10) | 1 | 0.13 |
| 45,XX,rob(13;22)(q10;q10) | 1 | 0.13 | ||
| 45,XX,rob(14;15)(q10;q10) | 1 | 0.13 | ||
| 45,XX,rob(14;21)(q10;q10) | 1 | 0.13 | ||
| 46,XX,t(1;4)(q?;q?) | 1 | 0.13 | ||
| 46,XX,t(1;16)(p36;p13)? | 1 | 0.13 | ||
| 46,XX,t(2;6)(p2?3;q2?1) | 1 | 0.13 | ||
| 46,XX,t(2;10)(p11?;p11?) | 1 | 0.13 | ||
| 46,XX,t(3;11)(p2?3;q23) | 1 | 0.13 | ||
| 46,XX,t(9;20)(p?;p?) | 1 | 0.13 | ||
| Inversions (n = 21; 2.69%) | 46,XX,inv(9)(p12q13) (n = 12); 46,XX,inv(9)(p13q21) (n = 7) | 19 | 2.44 | |
| 46,XX,inv(10)(p11q21) | 2 | 0.26 | ||
| Single cell translocations | (Table 3.) | 27 | 3.46 | |
| Control group (n = 1160) | ||||
| Structural chromosomal aberrations | Inversions (n = 31; 2.67%) | 46,XX,inv(9)(p13q21) (n = 15); 46,XX,inv(9)(p12q13) (n = 11); | 26 | 2.24 |
| 46,XX,inv(10)(p11.2q22.1) | 2 | 0.17 | ||
| 46,XX,inv(1)(p13q21) | 1 | 0.09 | ||
| 46,XX,inv(5)(q11.2q22) | 1 | 0.09 | ||
| 46,XX,inv(13)(q12q14.?1) | 1 | 0.09 | ||
| Single cell translocations | (Table 3.) | 8 | 0.7 | |
| Infertile Patients (n = 2269) | |||
|---|---|---|---|
| t(7;14)(q34;q11.2) (n = 8; 0.35%) | t(5;9)(p15;p11) (n = 1; 0.04%) | t(2;8)(q33;q22) (n = 1; 0.04%) | t(7;17)(q32;q21) (n = 1; 0.04%) |
| t(7;14)(q34;q11.2)/t(1;17)(q42;q25) (n = 1; 0.04%) | t(5;9)(q35;q13) (n = 1; 0.04%) | t(3,5)(q21;q35) (n = 1; 0.04%) | t(7;18)(p22;q21) (n = 1; 0.04%) |
| t(7;14)(p15.3;q13) (n = 2; 0.09%) | t(6;6)(q21;p21) (n = 1; 0.04%) | t(3;7)(q12;p15) (n = 1; 0.04%) | t(7;22)(?;?) (n = 1; 0.04%) |
| t(7;14)(q10;q10) (n = 1; 0.04%) | t(6;6)(q21;p25) (n = 1; 0.04%) | t(3;7)(q23;q22) (n = 1; 0.04%) | t(8;11)(p23.3;p15.5) (n = 1; 0.04%) |
| t(7;14)(q11;p11) (n = 1; 0.04%) | t(7;12)(p15;q13) (n = 1; 0.04%) | t(3;10)(p13;q26) (n = 1; 0.04%) | t(8;14)(q24;q24) (n = 1; 0.04%) |
| t(7,14)(q32;q32) (n = 1; 0.04%) | t(7;12)(q36;q22) (n = 1; 0.04%) | t(3;13)(q27;q14) (n = 1; 0.04%) | t(9;13)(p13;q22) (n = 1; 0.04%) |
| t(7;14)(q3?5;q11) (n = 1; 0.04%) | t(8;16)(p12;q24) (n = 1; 0.04%) | t(4;6)(q27;q23) (n = 1; 0.04%) | t(9;20)(?;?) (n = 1; 0.04%) |
| t(7;14)(q3?6;q13) (n = 1; 0.04%) | t(8;16)(p21;q13) (n = 1; 0.04%) | t(4;8)(p14;q22) (n = 1; 0.04%) | t(10;12)(q22;q13) (n = 1; 0.04%) |
| t(7;14)(q3?6;q13) (n = 1; 0.04%) | t(10;11)(p13;q25) (n = 1; 0.04%) | t(4;11)(p16;q13) (n = 1; 0.04%) | t(10;16)(q22;q22) (n = 1; 0.04%) |
| t(7;14)(p13;q11) (n = 1; 0.04%) | t(10;11)(q22;p15) (n = 1; 0.04%) | t(4;12)(q21;p13) (n = 1; 0.04%) | t(10;18)(q24;q23) (n = 1; 0.04%) |
| t(1;2)(p22;p13) (n = 1; 0.04%) | t(1;6)(p22;p21) (n = 1; 0.04%) | t(4;17)(q24;q21) (n = 1; 0.04%) | t(11;12)(q21;q13) (n = 1; 0.04%) |
| t(1;2)(p22;p21) (n = 1; 0.04%) | t(1;7)(p32;q32) (n = 1; 0.04%) | t(5;12)(q31;q13) (n = 1; 0.04%) | t(11;13)(q13;q21) (n = 1; 0.04%) |
| t(1;5)(q32;p15.2) (n = 1; 0.04%) | t(1;10)(p36;p11) (n = 1; 0.04%) | t(6;12)(q27;q13.1) (n = 1; 0.04%) | t(14;16)(q24;q24) (n = 1; 0.04%) |
| t(1;5)(p22;q31) (n = 1; 0.04%) | t(1;11)(p32;q23) (n = 1; 0.04%) | t(6;13)(p11;q21.2) (n = 1; 0.04%) | t(14;20)(p11;p11) (n = 1; 0.04%) |
| t(2;7)(q35;p22) (n = 1; 0.04%) | t(1;13)(q32;q22) (n = 1; 0.04%) | t(6;20)(q13;q13) (n = 1; 0.04%) | t(X;1)(q32;p22) (n = 1; 0.04%) |
| t(2;7)(q33;q33)/t(2;12)(q33;q13.1) (n = 1; 0.04%) | t(1;14)(p36;q13)/t(15;18)(q13;q11) (n = 1; 0.04%) | t(7;8)(q32;q24) (n = 1; 0.04%) | t(X;11)(q13;p15) (n = 1; 0.04%) |
| t(2;11)(p21?;p15?) (n = 1; 0.04%) | t(1;18)(q32;q11) (n = 1; 0.04%) | t(7;10)(p13;q11) (n = 1; 0.04%) | t(Y;16)(q12;q13.3) (n = 1; 0.04%) |
| t(2;11)(p25;p11) (n = 1; 0.04%) | t(1;22)(q23;q13) (n = 1; 0.04%) | t(7;16)(q11;q12) (n = 1; 0.04%) | |
| Control patients (n = 2029) | |||
| t(7;14)(q11;p11) (n = 1; 0.05%) | t(7;14)(q34;q11) (n = 1; 0.05%) | t(14;19)(q11;q13) (n = 1; 0.05%) | t(7;20)(?;?) (n = 1; 0.05%) |
| t(7;14)(q11.2;p11) (n = 1; 0.05%) | t(7;14)(q34;q11)/t(3;10)(q27;q21) (n = 1; 0.05%) | t(14;19)(q11;p13) (n = 1; 0.05%) | t(7;22)(p32;q11) (n = 1; 0.05%) |
| t(7;14)(p21;q22) (n = 1; 0.05%) | t(7;14)(q36;q13) (n = 1; 0.05%) | t(7;10)(q36;q11) (n = 1; 0.05%) | t(9;12)(?;?) (n = 1; 0.05%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Andó, S.; Koczok, K.; Bessenyei, B.; Balogh, I.; Ujfalusi, A. Cytogenetic Investigation of Infertile Patients in Hungary: A 10-Year Retrospective Study. Genes 2022, 13, 2086. https://doi.org/10.3390/genes13112086
Andó S, Koczok K, Bessenyei B, Balogh I, Ujfalusi A. Cytogenetic Investigation of Infertile Patients in Hungary: A 10-Year Retrospective Study. Genes. 2022; 13(11):2086. https://doi.org/10.3390/genes13112086
Chicago/Turabian StyleAndó, Szilvia, Katalin Koczok, Beáta Bessenyei, István Balogh, and Anikó Ujfalusi. 2022. "Cytogenetic Investigation of Infertile Patients in Hungary: A 10-Year Retrospective Study" Genes 13, no. 11: 2086. https://doi.org/10.3390/genes13112086
APA StyleAndó, S., Koczok, K., Bessenyei, B., Balogh, I., & Ujfalusi, A. (2022). Cytogenetic Investigation of Infertile Patients in Hungary: A 10-Year Retrospective Study. Genes, 13(11), 2086. https://doi.org/10.3390/genes13112086