
Diagnostic Yield and Economic Implications of Whole-Exome Sequencing for ASD Diagnosis in Israel

 ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Sample and Statistical Analysis
2.2. Whole-Exome Sequencing
2.3. Identification of Candidate ASD Genetic Variants
2.4. Cost-Effectiveness Analysis
3. Results
3.1. Genetic Findings
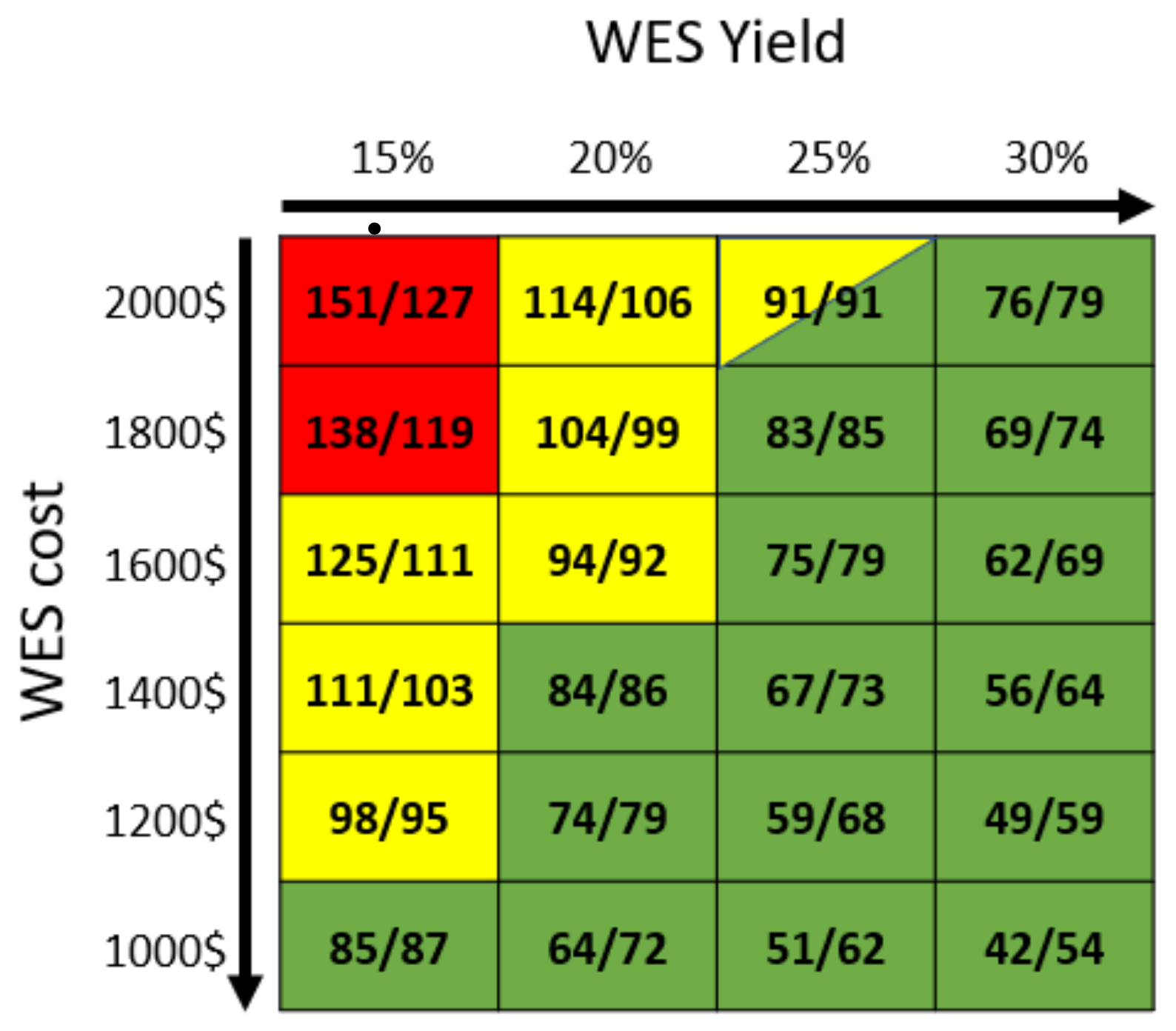
3.2. Cost-Effectiveness Analysis
4. Discussion
4.1. Whole-Exome Sequencing Yield
4.2. Ethnic Differences in Whole-Exome Sequencing Yield
4.3. Cost Effectiveness of Whole-Exome Sequencing for Children with ASD in the Israeli Health System
4.4. Additional Implications of Whole-Exome Sequencing for Children with ASD
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sharma, S.R.; Gonda, X.; Tarazi, F.I. Autism Spectrum Disorder: Classification, diagnosis and therapy. Pharmacol. Ther. 2018, 190, 91–104. [Google Scholar] [CrossRef] [PubMed]
- Muhle, R.; Trentacoste, S.V.; Rapin, I. The Genetics of Autism. Pediatrics 2004, 113, 472–486. [Google Scholar] [CrossRef]
- Hansen, S.N.; Schendel, D.E.; Francis, R.W.; Windham, G.C.; Bresnahan, M.; Levine, S.Z.; Reichenberg, A.; Gissler, M.; Kodesh, A.; Bai, D.; et al. Recurrence Risk of Autism in Siblings and Cousins: A Multinational, Population-Based Study. J. Am. Acad. Child Adolesc. Psychiatry 2019, 58, 866–875. [Google Scholar] [CrossRef]
- Conti, S.L.; Eisenberg, M.L. Paternal aging and increased risk of congenital disease, psychiatric disorders, and cancer. Asian J. Androl. 2016, 18, 420–424. [Google Scholar]
- Miller, D.T.; Adam, M.P.; Aradhya, S.; Biesecker, L.G.; Brothman, A.R.; Carter, N.P.; Church, D.M.; Crolla, J.A.; Eichler, E.E.; Epstein, C.J.; et al. Consensus Statement: Chromosomal Microarray Is a First-Tier Clinical Diagnostic Test for Individuals with Developmental Disabilities or Congenital Anomalies. Am. J. Hum. Genet. 2010, 86, 749–764. [Google Scholar] [CrossRef] [PubMed]
- Lu, X.-Y.; Phung, M.T.; Shaw, C.A.; Pham, K.; Neil, S.E.; Patel, A.; Sahoo, T.; Bacino, C.A.; Stankiewicz, P.; Kang, S.-H.L.; et al. Genomic Imbalances in Neonates With Birth Defects: High Detection Rates by Using Chromosomal Microarray Analysis. Pediatrics 2008, 122, 1310–1318. [Google Scholar] [CrossRef] [PubMed]
- Bai, D.; Yip, B.H.K.; Windham, G.C.; Sourander, A.; Francis, R.; Yoffe, R.; Glasson, E.; Mahjani, B.; Suominen, A.; Leonard, H.; et al. Association of Genetic and Environmental Factors With Autism in a 5-Country Cohort. JAMA Psychiatry 2019, 76, 1035–1043. [Google Scholar] [CrossRef]
- Devlin, B.; Scherer, S.W. Genetic architecture in autism spectrum disorder. Curr. Opin. Genet. Dev. 2012, 22, 229–237. [Google Scholar] [CrossRef] [PubMed]
- Girirajan, S.; Dennis, M.Y.; Baker, C.; Malig, M.; Coe, B.P.; Campbell, C.D.; Mark, K.; Vu, T.H.; Alkan, C.; Cheng, Z.; et al. Refinement and Discovery of New Hotspots of Copy-Number Variation Associated with Autism Spectrum Disorder. Am. J. Hum. Genet. 2013, 92, 221–237. [Google Scholar] [CrossRef] [PubMed]
- Sebat, J.; Lakshmi, B.; Malhotra, D.; Troge, J.; Lese-Martin, C.; Walsh, T.; Yamrom, B.; Yoon, S.; Krasnitz, A.; Kendall, J.; et al. Strong Association of De Novo Copy Number Mutations with Autism. Science 2007, 316, 445–449. [Google Scholar] [CrossRef]
- Vicari, S.; Napoli, E.; Cordeddu, V.; Menghini, D.; Alesi, V.; Loddo, S.; Novelli, A.; Tartaglia, M. Copy number variants in autism spectrum disorders. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2019, 92, 421–427. [Google Scholar] [CrossRef]
- Woodbury-Smith, M.; Zarrei, M.; Wei, J.; Thiruvahindrapuram, B.; O’Connor, I.; Paterson, A.D.; Yuen, R.K.C.; Dastan, J.; Stavropoulos, D.J.; Howe, J.L.; et al. Segregating patterns of copy number variations in extended autism spectrum disorder (ASD) pedigrees. Am. J. Med Genet. B Neuropsychiatr. Genet. 2020, 183, 268–276. [Google Scholar] [CrossRef]
- Kanduri, C.; Kantojärvi, K.; Salo, P.M.; Vanhala, R.; Buck, G.; Blancher, C.; Lähdesmäki, H.; Järvelä, I. The landscape of copy number variations in Finnish families with autism spectrum disorders. Autism Res. 2015, 9, 9–16. [Google Scholar] [CrossRef] [PubMed]
- Shendure, J.; Fisher, S.; Bernier, R.; Nickerson, D.; Rieder, M.; Baker, C.; Ng, S.; Mackenzie, A.; Karakoc, E.; Girirajan, S.; et al. Exome sequencing in sporadic autism spectrum disorders identifies severe de novo mutations. Nat. Genet. 2011, 43, 585. [Google Scholar]
- Grove, J.; Ripke, S.; Als, T.D.; Mattheisen, M.; Walters, R.K.; Won, H.; Pallesen, J.; Agerbo, E.; Andreassen, O.A.; Anney, R.; et al. Identification of common genetic risk variants for autism spectrum disorder. Nat. Genet. 2019, 51, 431–444. [Google Scholar] [CrossRef] [PubMed]
- Yuen, R.K.C.; Merico, D.; Bookman, M.; Howe, J.L.; Thiruvahindrapuram, B.; Patel, R.V.; Whitney, J.; Deflaux, N.; Bingham, J.; Wang, Z.; et al. Whole genome sequencing resource identifies 18 new candidate genes for autism spectrum disorder. Nat. Neurosci. 2017, 20, 602–611. [Google Scholar] [CrossRef] [PubMed]
- Geschwind, D.H. Genetics of autism spectrum disorders. Trends Cogn. Sci. 2011, 15, 409–416. [Google Scholar] [CrossRef]
- Rylaarsdam, L.E.; Guemez-Gamboa, A. Genetic Causes and Modifiers of Autism Spectrum Disorder. Front. Cell. Neurosci. 2019, 13, 385. [Google Scholar] [CrossRef] [PubMed]
- Wiśniowiecka-Kowalnik, B.; Nowakowska, B.A. Genetics and epigenetics of autism spectrum disorder—current evidence in the field. J. Appl. Genet. 2019, 60, 37–47. [Google Scholar] [CrossRef]
- Woodbury-Smith, M.; Scherer, S.W. Progress in the genetics of autism spectrum disorder. Dev. Med. Child Neurol. 2018, 60, 445–451. [Google Scholar] [CrossRef]
- Jeste, S.S.; Geschwind, D.H. Disentangling the heterogeneity of autism spectrum disorder through genetic findings. Nat. Rev. Neurol. 2014, 10, 74–81. [Google Scholar] [CrossRef] [PubMed]
- Wallace, S.E.; Bean, L.J.H. Educational Materials—Genetic Testing: Current Approaches; University of Washington: Seattle, WA, USA, 2018. [Google Scholar]
- Arteche-López, A.; Gómez Rodríguez, M.J.; Sánchez Calvin, M.T.; Quesada-Espinosa, J.F.; Lezana Rosales, J.M.; Palma Milla, C.; Gómez-Manjón, I.; Hidalgo Mayoral, I.; Pérez de la Fuente, R.; Díaz de Bustamante, A.; et al. Towards a Change in the Diagnostic Algorithm of Autism Spectrum Disorders: Evidence Supporting Whole Exome Sequencing as a First-Tier Test. Genes 2021, 12, 560. [Google Scholar] [CrossRef]
- Israel Ministry of Health. Circular letter: Autism Spectrum Disorder Diagnosis. 2013. Available online: https://www.health.govt.nz/publication/health-and-independence-report-2013 (accessed on 14 September 2021).
- Israel Ministry of Health. Circular Letter: Genetic Tests Including Next Generation Sequencing. 2018. Available online: https://www.health.gov.il/English/Topics/Genetics/checks/Pages/exome.aspx (accessed on 14 September 2021).
- Cappe, E.; Poirier, N.; Sankey, C.; Belzil, A.; Dionne, C. Quality of life of French Canadian parents raising a child with autism spectrum disorder and effects of psychosocial factors. Qual. Life Res. 2017, 27, 955–967. [Google Scholar] [CrossRef]
- van Tongerloo, M.A.M.M.P.; van Wijngaarden, J.M.; van der Gaag, R.J.; Lagro-Janssen, A.L.M. Raising a child with an Autism Spectrum Disorder: ‘If this were a partner relationship, I would have quit ages ago. Fam. Pract. 2015, 32, 88–93. [Google Scholar] [CrossRef][Green Version]
- Dieleman, L.M.; Moyson, T.; De Pauw, S.S.; Prinzie, P.; Soenens, B. Parents’ Need-related Experiences and Behaviors When Raising a Child With Autism Spectrum Disorder. J. Pediatr. Nurs. 2018, 42, e26–e37. [Google Scholar] [CrossRef]
- Horlin, C.; Falkmer, M.; Parsons, R.; Albrecht, M.; Falkmer, T. The Cost of Autism Spectrum Disorders. PLoS ONE 2014, 9, e106552. [Google Scholar] [CrossRef] [PubMed]
- Buescher, A.V.S.; Cidav, Z.; Knapp, M.; Mandell, D.S. Costs of Autism Spectrum Disorders in the United Kingdom and the United States. JAMA Pediatr. 2014, 168, 721–728. [Google Scholar] [CrossRef]
- National Insurance Institute of Israel. ASD—Autistic Spectrum Disorder—Eligibility (Based on Disabilities and Medical Conditions) [Hebrew]. 2019. Available online: https://www.btl.gov.il/benefits/Disabled_Child/likuilist/Pages/autism.aspx (accessed on 6 July 2019).
- ALUT—The Israeli Society for Children and Adults with Autism, General Disability Allowance. 2021. Available online: https://alut.org.il/?page_id=322 (accessed on 6 November 2021).
- ALUT—The Israeli Society for Children and Adults with Autism, Special Services Allowance. 2021. Available online: https://alut.org.il/?page_id=324 (accessed on 6 November 2021).
- WHO. Cost-Effectiveness Analysis for Health Interventions; World Health Organization: Geneva, Switzerland, 2010; p. 1. Available online: https://www.who.int/heli/economics/costeffanalysis/en/ (accessed on 14 September 2021).
- Yuen, T.; Carter, M.T.; Szatmari, P.; and Ungar, W.J. Cost-effectiveness of Genome and Exome Sequencing in Children Di-agnosed with Autism Spectrum Disorder. Appl. Health Econ. Health Policy 2018, 16, 481–493. [Google Scholar] [CrossRef] [PubMed]
- Meiri, G.; Dinstein, I.; Michaelowski, A.; Flusser, H.; Ilan, M.; Faroy, M.; Bar-Sinai, A.; Manelis, L.; Stolowicz, D.; Yosef, L.L.; et al. Brief Report: The Negev Hospital-University-Based (HUB) Autism Database. J. Autism Dev. Disord. 2017, 47, 2918–2926. [Google Scholar] [CrossRef]
- Dinstein, I.; Arazi, A.; Golan, H.M.; Koller, J.; Elliott, E.; Gozes, I.; Shulman, C.; Shifman, S.; Raz, R.; Davidovitch, N.; et al. The National Autism Database of Israel: A Resource for Studying Autism Risk Factors, Biomarkers, Outcome Measures, and Treatment Efficacy. J. Mol. Neurosci. 2020, 70, 1303–1312. [Google Scholar] [CrossRef] [PubMed]
- Buxbaum, J.D.; Daly, M.J.; Devlin, B.; Lehner, T.; Roeder, K.; State, M.W.; Autism Sequencing Consortium. NeuroView The Autism Sequencing Consortium: Large-Scale, High-Throughput Sequencing in Autism Spectrum Disorders. Neuron 2012, 76, 1052–1056. [Google Scholar] [CrossRef] [PubMed]
- Abrahams, B.S.; Arking, D.E.; Campbell, D.B.; Mefford, H.C.; Morrow, E.M.; Weiss, L.A.; Menashe, I.; Wadkins, T.; Banerjee-Basu, S.; Packer, A. SFARI Gene 2.0: A community-driven knowledgebase for the autism spectrum disorders (ASDs). Mol. Autism 2013, 4, 36. [Google Scholar] [CrossRef] [PubMed]
- McKenna, A.; Hanna, M.; Banks, E.; Sivachenko, A.; Cibulskis, K.; Kernytsky, A.; Garimella, K.; Altshuler, D.; Gabriel, S.; Daly, M.; et al. The Genome Analysis Toolkit: A MapReduce framework for analyzing next-generation DNA sequencing data. Genome Res. 2010, 20, 1297–1303. [Google Scholar] [CrossRef]
- McLaren, W.; Gil, L.; Hunt, S.E.; Riat, H.S.; Ritchie, G.R.S.; Thormann, A.; Flicek, P.; Cunningham, F. The Ensembl Variant Effect Predictor. Genome Biol. 2016, 17, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Ng, P.C.; Henikoff, S. SIFT: Predicting amino acid changes that affect protein function. Nucleic Acids Res. 2003, 31, 3812–3814. [Google Scholar] [CrossRef] [PubMed]
- Adzhubei, I.; Jordan, D.; Sunyaev, S.R. Predicting Functional Effect of Human Missense Mutations Using PolyPhen-2. Curr. Protoc. Hum. Genet. 2013, 76, 7.20.1–7.20.41. [Google Scholar] [CrossRef]
- Robinson, J.T.; Thorvaldsdóttir, H.; Winckler, W.; Guttman, M.; Lander, E.S.; Getz, G.; Mesirov, J.P. Integrative genomics viewer. Nat. Biotechnol. 2011, 29, 24–26. [Google Scholar] [CrossRef]
- Bambha, K.; Kim, W.R. Cost-effectiveness analysis and incremental cost-effectiveness ratios: Uses and pitfalls. Eur. J. Gastroenterol. Hepatol. 2004, 16, 519–526. [Google Scholar] [CrossRef]
- Barzilai University Medical Center. Common Services and Codes Price List. 2019. Available online: http://www.bmc.gov.il/?CategoryID=859&ArticleID=3665 (accessed on 23 March 2020).
- Hadassah University Medical Center. Hadassah Medical Center Exome Sequencing Lab. Available online: https://www.hadassah.org.il/en/exome_sequencing_lab/ (accessed on 14 September 2021).
- The National Insurance Property Development Company Limited, Ministry of Health Pharmaceutical Price List. 2021. Available online: https://nipdec.com/pharmaceutical/ (accessed on 14 September 2021).
- National Insurance Institute of Israel. Average Wages According to Sections 1 and 2 of the National Insurance Law. Available online: https://www.btl.gov.il/Mediniyut/GeneralData/Pages/%D7%A9%D7%9B%D7%A8%20%D7%9E%D7%9E%D7%95%D7%A6%D7%A2.aspx (accessed on 23 March 2020).
- Clark, M.M.; Stark, Z.; Farnaes, L.; Tan, T.Y.; White, S.M.; Dimmock, D.; Kingsmore, S.F. Meta-analysis of the diagnostic and clinical utility of genome and exome sequencing and chromosomal microarray in children with suspected genetic diseases. NPJ Genom. Med. 2018, 3, 16. [Google Scholar] [CrossRef]
- Richards, S.; Aziz, N.; Bale, S.; Bick, D.; Das, S.; Gastier-Foster, J.; Grody, W.W.; Hegde, M.; Lyon, E.; Spector, E.; et al. Standards and guidelines for the interpretation of sequence variants: A joint consensus recommendation of the American College of Medical Genetics and Genomics and the Association for Molecular Pathology. Genet. Med. 2015, 17, 405–424. [Google Scholar] [CrossRef]
- Bahcall, O.G. Genetic testing: ACMG guides on the interpretation of sequence variants. Nat. Rev. Genet. 2015, 16, 256–257. [Google Scholar] [CrossRef]
- DiCicco-Bloom, E.; Lord, C.; Zwaigenbaum, L.; Courchesne, E.; Dager, S.R.; Schmitz, C.; Schultz, R.T.; Crawley, J.; Young, L.J. The Developmental Neurobiology of Autism Spectrum Disorder. J. Neurosci. 2006, 26, 6897–6906. [Google Scholar] [CrossRef] [PubMed]
- Zlotogora, J. Genetics and genomic medicine in Israel. Mol. Genet. Genom. Med. 2014, 2, 85–94. [Google Scholar] [CrossRef] [PubMed]
- The Knesset. Bedouins in the State of Israel. Available online: https://www.knesset.gov.il/lexicon/eng/bedouim_eng.htm (accessed on 14 October 2020).
- Na’Amnih, W.; Romano-Zelekha, O.; Kabaha, A.; Rubin, L.P.; Bilenko, N.; Jaber, L.; Honovich, M.; Shohat, T. Prevalence of consanguineous marriages and associated factors among Israeli Bedouins. J. Community Genet. 2014, 5, 395–398. [Google Scholar] [CrossRef]
- Levaot, Y.; Meiri, G.; Dinstein, I.; Menashe, I.; Shoham-Vardi, I. Autism Prevalence and Severity in Bedouin-Arab and Jewish Communities in Southern Israel. Community Ment. Heal. J. 2018, 55, 156–160. [Google Scholar] [CrossRef]
- Kerub, O.; Haas, E.J.; Meiri, G.; Bilenko, N.; Flusser, H.; Michaelovski, A.; Dinstein, I.; Davidovitch, N.; Menashe, I. Ethnic Disparities in the Diagnosis of Autism in Southern Israel. Autism Res. 2020, 14, 193–201. [Google Scholar] [CrossRef] [PubMed]
- Zaresani, A.; Emery, H.; Dutton, D. Why Adults with Autism Spectrum Disorder Have Lower Labor Supply than the Other Disability Groups? 2018. Available online: https://azaresani.com/wp-content/uploads/Autism-and-labor.pdf (accessed on 14 September 2021).
- Hendel, Y.; Meiri, G.; Flusser, H.; Michaelovski, A.; Dinstein, I.; Menashe, I. Factors Affecting Family Compliance with Genetic Testing of Children Diagnosed with Autism Spectrum Disorder. J. Autism Dev. Disord. 2021, 51, 1201–1209. [Google Scholar] [CrossRef]
- Kostic, A.; Buxbaum, J.D. The promise of precision medicine in autism. Neuron 2021, 109, 2212–2215. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variable | Children with Exome (N = 182) | Children without Exome (N = 690) | p-Value | |
|---|---|---|---|---|
| Gender (Male) | 139 (76.4%) | 555 (80.4%) | 0.2844 a | |
| Ethnicity (Bedouin) | 47 (25.8%) | 165 (23.9%) | 0.5512 a | |
| Diagnosis age (years; mean, SD) | 3.01 (1.43) | 3.35 (1.37) | 0.0004 b | |
| IQ (mean, SD) | 72.71 (18.79) | 75.37 (17.89) | 0.1516 b | |
| ADOS module (N = 705) | Toddler | 57 (39.3%) | 150 (26.8%) | 0.0165 c |
| 1 | 57 (39.3%) | 239 (42.7%) | ||
| 2 | 18 (12.4%) | 111 (19.8%) | ||
| 3 | 13 (9.0%) | 60 (10.7%) | ||
| ADOS comparison score (mean, SD) | 7.47 (2.3) | 6.65 (2.3) | <0.0001 b | |
| DSM-5 severity level (A) # (N = 782) | 1 | 12 (7.6%) | 112 (17.9%) | 0.0014 c |
| 2 | 68 (43.0%) | 266 (42.6%) | ||
| 3 | 78 (49.4%) | 246 (39.4%) | ||
| DSM-5 severity level (B) # (N = 782) | 1 | 15 (9.5%) | 145 (23.2%) | <0.0001 c |
| 2 | 83 (52.5%) | 310 (49.7%) | ||
| 3 | 60 (38.0%) | 169 (27.0%) | ||
| Variable | Children with Positive WES Findings (N = 28) | Children with Negative WES Findings (N = 154) | p-Value | |
|---|---|---|---|---|
| Gender (Male) | 20 (71.4%) | 119 (77.3%) | 0.503 a | |
| Ethnicity (Bedouin) | 13 (46.4%) | 34 (22.1%) | 0.036 a | |
| Diagnosis age (years; mean, SD) | 2.62, 0.90 | 3.08, 1.50 | 0.114 b | |
| IQ (mean, SD) | 69.6, 18.42 | 73.2, 18.89 | 0.38 b | |
| ADOS module (N = 145) | Toddler | 12 (50%) | 45 (37.2%) | 0.162 c |
| 1 | 9 (37.5%) | 48 (39.7%) | ||
| 2 | 2 (8.3%) | 16 (13.2%) | ||
| 3 | 1 (4.2%) | 12 (9.9%) | ||
| ADOS comparison score (mean, SD) | 8.04, 2.44 | 7.36, 2.252 | 0.073 b | |
| DSM-5 severity level (A) # (N = 158) | 1 | 3 (11.5%) | 9 (6.8%) | 0.33 c |
| 2 | 12 (46.2%) | 56 (42.4%) | ||
| 3 | 11 (42.3%) | 67 (50.8%) | ||
| DSM-5 severity level (B) # (N = 158) | 1 | 2 (7.7%) | 13 (9.8%) | 0.412 c |
| 2 | 17 (65.4%) | 66 (50%) | ||
| 3 | 7 (26.9%) | 53 (40.2%) | ||
| Strategy | Total Cost (USD) | Outcome–Diagnostic Yield by Each Strategy (%) | Incremental Cost-Effectiveness Ratio (ICER) |
|---|---|---|---|
| CMA | 1170 | 10 | 117.0 |
| WES | 2270 | 15.4 | 147.4 |
| CMA + WES | 3170 | 25.4 | 124.8 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tal-Ben Ishay, R.; Shil, A.; Solomon, S.; Sadigurschi, N.; Abu-Kaf, H.; Meiri, G.; Flusser, H.; Michaelovski, A.; Dinstein, I.; Golan, H.; et al. Diagnostic Yield and Economic Implications of Whole-Exome Sequencing for ASD Diagnosis in Israel. Genes 2022, 13, 36. https://doi.org/10.3390/genes13010036
Tal-Ben Ishay R, Shil A, Solomon S, Sadigurschi N, Abu-Kaf H, Meiri G, Flusser H, Michaelovski A, Dinstein I, Golan H, et al. Diagnostic Yield and Economic Implications of Whole-Exome Sequencing for ASD Diagnosis in Israel. Genes. 2022; 13(1):36. https://doi.org/10.3390/genes13010036
Chicago/Turabian StyleTal-Ben Ishay, Rotem, Apurba Shil, Shirley Solomon, Noa Sadigurschi, Hadeel Abu-Kaf, Gal Meiri, Hagit Flusser, Analya Michaelovski, Ilan Dinstein, Hava Golan, and et al. 2022. "Diagnostic Yield and Economic Implications of Whole-Exome Sequencing for ASD Diagnosis in Israel" Genes 13, no. 1: 36. https://doi.org/10.3390/genes13010036
APA StyleTal-Ben Ishay, R., Shil, A., Solomon, S., Sadigurschi, N., Abu-Kaf, H., Meiri, G., Flusser, H., Michaelovski, A., Dinstein, I., Golan, H., Davidovitch, N., & Menashe, I. (2022). Diagnostic Yield and Economic Implications of Whole-Exome Sequencing for ASD Diagnosis in Israel. Genes, 13(1), 36. https://doi.org/10.3390/genes13010036