
Investigation of an Alternative Marker for Hypermutability Evaluation in Different Tumors


Abstract
1. Introduction
2. Materials and Methods
2.1. Patients and Samples
2.2. DNA Preparation
2.3. Evaluation of Microsatellite Instablity Stability and Short Tandem Repeats Alteration Status
2.4. Statistics Analysis
3. Results
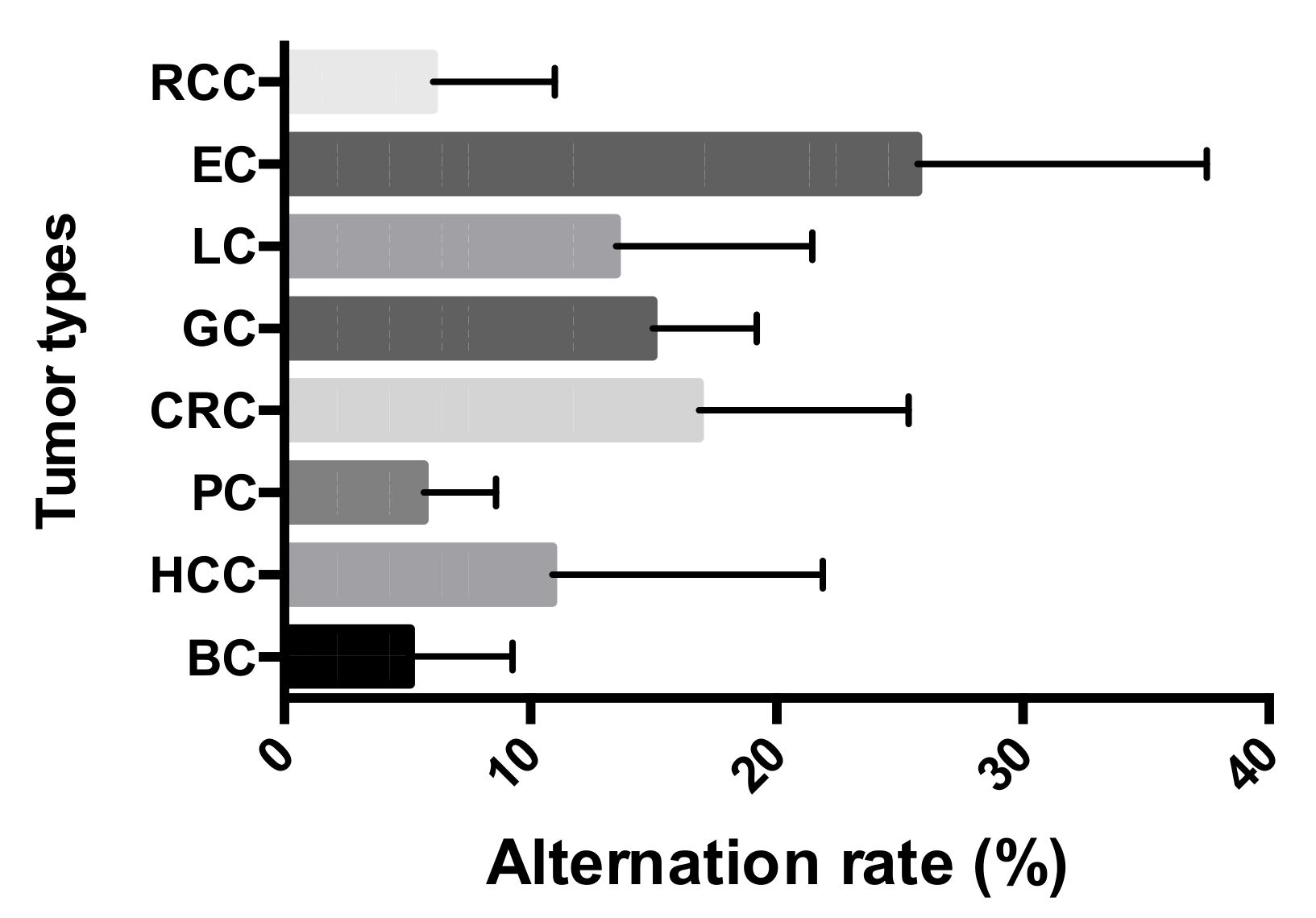
3.1. Widespread STR Alterations Observed across the Tumors
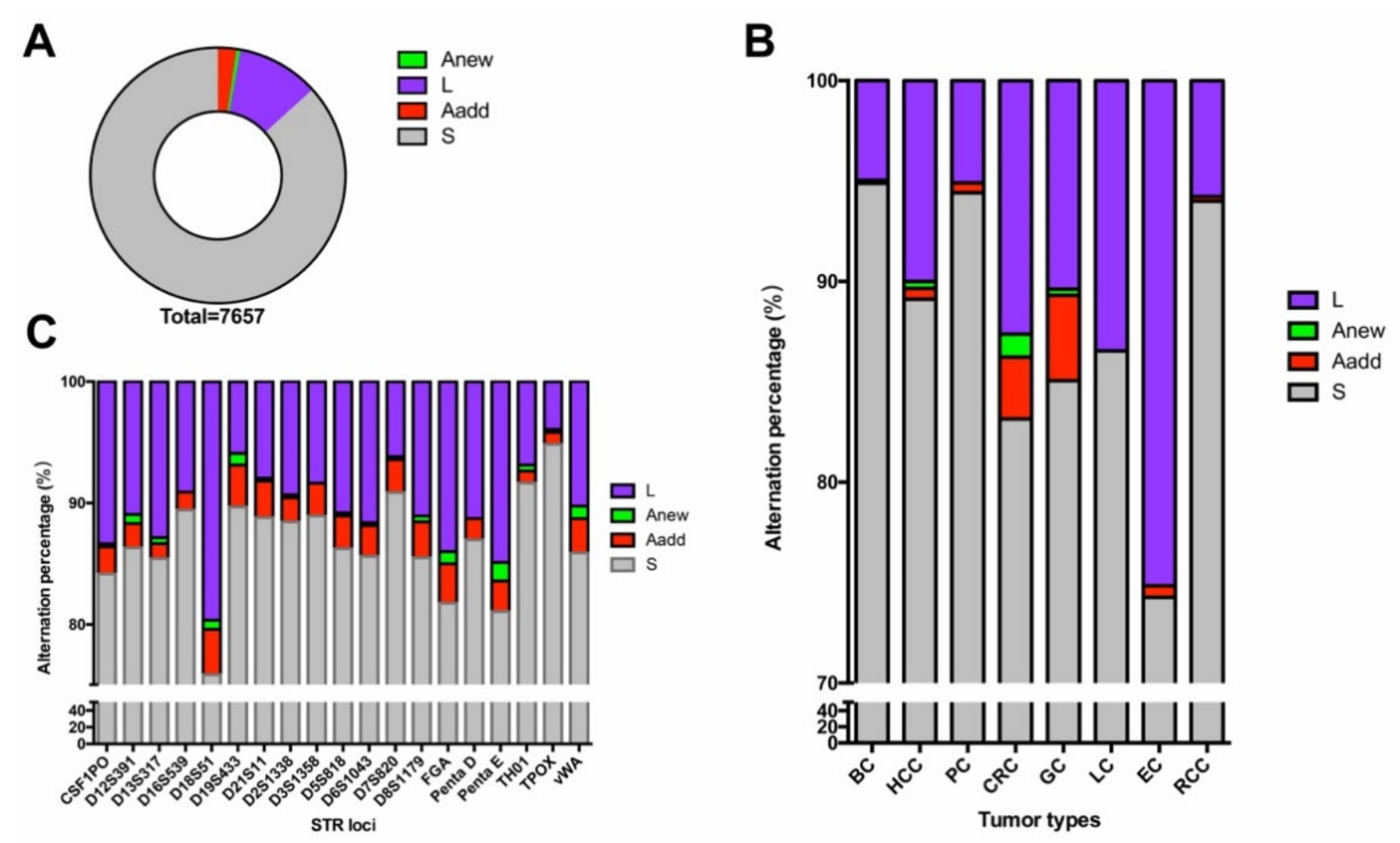
3.2. Loss of Heterozygosity Was the Most Commonly Observed Alteration in Eight Types of Tumor
3.3. Different Tumors Exhibited Varied Alteration Tendencies in the Loci
3.4. MSI Status Was Only Detected in Gastrointestinal Tumors
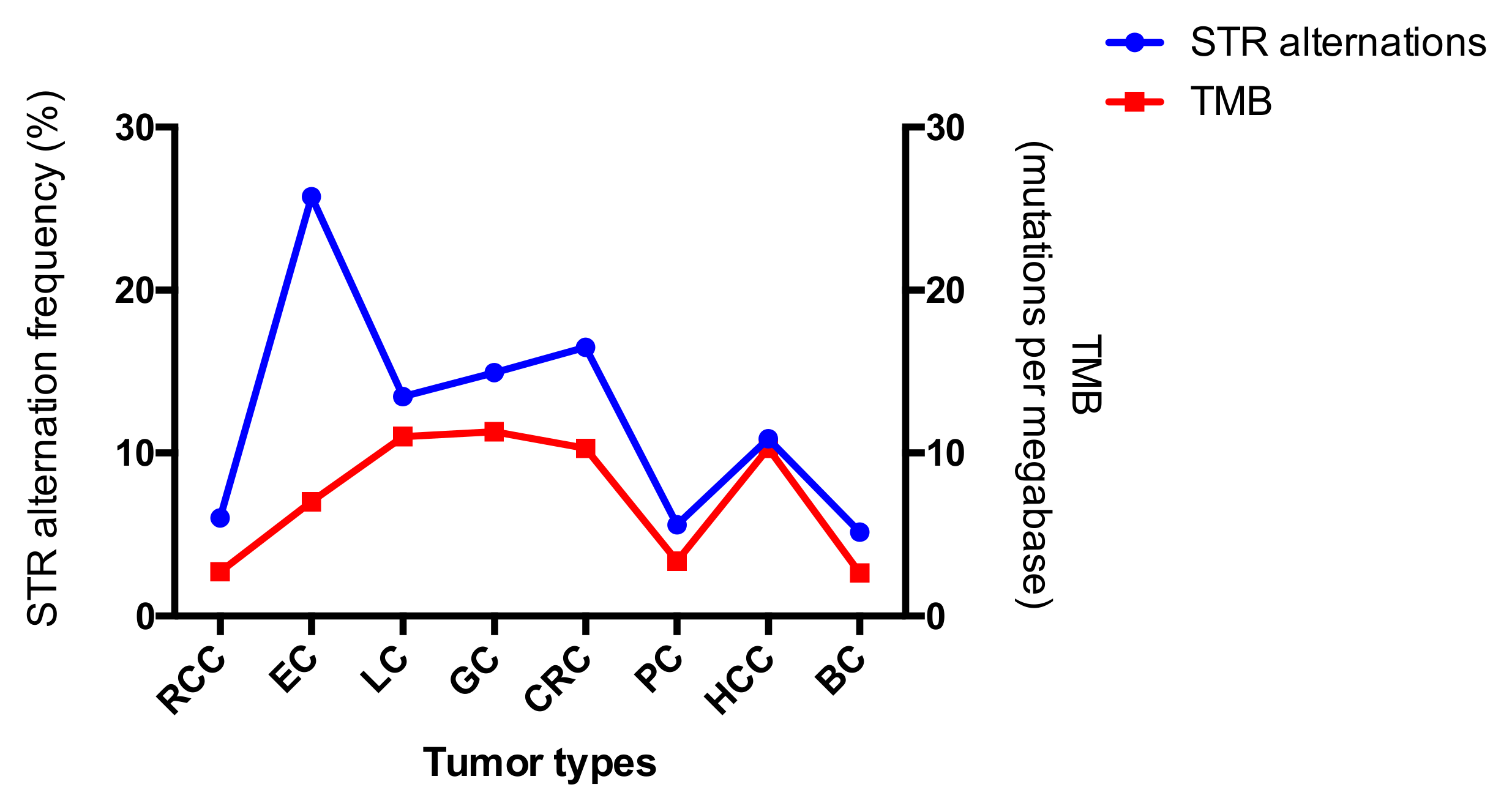
3.5. Comparison between the Alterations of STR and MSI
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lin, A.; Zhang, J.; Luo, P. Crosstalk between the MSI status and tumor microenvironment in colorectal cancer. Front. Immunol. 2020, 11, 2039. [Google Scholar] [CrossRef]
- Lemery, S.; Keegan, P.; Pazdur, R. First FDA approval agnostic of cancer site—When a biomarker defines the indication. N. Engl. J. Med. 2017, 377, 1409–1412. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.; Zheng, Z.C.; Luo, Y.H.; Piao, H.Z.; Zheng, G.L.; Shi, J.Y.; Zhang, T.; Zhang, J.J. Low-frequency microsatellite instability in genomic di-nucleotide sequences correlates with lymphatic invasion and poor prognosis in gastric cancer. Cell Biochem. Biophys. 2015, 71, 235–241. [Google Scholar] [CrossRef] [PubMed]
- Devaraj, B.; Lee, A.; Cabrera, B.L.; Miyai, K.; Luo, L.; Ramamoorthy, S.; Keku, T.; Sandler, R.S.; McGuire, K.L.; Carethers, J.M. Relationship of EMAST and microsatellite instability among patients with rectal cancer. Journal of gastrointestinal surgery. Off. J. Soc. Surg. Aliment. Tract. 2010, 14, 1521–1528. [Google Scholar]
- Torshizi Esfahani, A.; Seyedna, S.Y.; Nazemalhosseini, M.E.; Majd, A.; Asadzadeh, A.H. MSI-L/EMAST is a predictive biomarker for metastasis in colorectal cancer patients. J. Cell. Physiol. 2019, 234, 13128–13136. [Google Scholar] [CrossRef]
- Liu, X.; Meltzer, S.J. Gastric cancer in the era of precision medicine. Cell. Mol. Gastroenterol. Hepatol. 2017, 3, 348–358. [Google Scholar] [CrossRef] [PubMed]
- Taube, J.M.; Klein, A.; Brahmer, J.R.; Xu, H.; Pan, X.; Kim, J.H.; Chen, L.; Pardoll, D.M.; Topalian, S.L.; Anders, R.A. Association of PD-1, PD-1 ligands, and other features of the tumor immune microenvironment with response to anti-PD-1 therapy. Clin. Cancer Res. 2014, 20, 5064–5074. [Google Scholar] [CrossRef] [PubMed]
- Yarchoan, M.; Hopkins, A.; Jaffee, E.M. Tumor mutational burden and response rate to PD-1 inhibition. N. Engl. J. Med. 2017, 377, 2500–2501. [Google Scholar] [CrossRef]
- Chen, A.; Zhang, S.; Li, J.; Ji, C.; Chen, J.; Li, C. Detecting genetic hypermutability of gastrointestinal tumor by using a forensic STR kit. Front. Med. 2020, 14, 101–111. [Google Scholar] [CrossRef]
- Svrcek, M.; Lascols, O.; Cohen, R.; Collura, A.; Jonchère, V.; Fléjou, J.F.; Buhard, O.; Duval, A. MSI/MMR-deficient tumor diagnosis: Which standard for screening and for diagnosis? Diagnostic modalities for the colon and other sites: Differences between tumors. Bull. Cancer 2019, 106, 119–128. [Google Scholar] [CrossRef]
- Vilar, E.; Gruber, S.B. Microsatellite instability in colorectal cancer-the stable evidence. Nat. Rev. Clin. Oncol. 2010, 7, 153–162. [Google Scholar] [CrossRef] [PubMed]
- Schrock, A.B.; Ouyang, C.; Sandhu, J.; Sokol, E.; Jin, D.; Ross, J.S.; Miller, V.A.; Lim, D.; Amanam, I.; Chao, J.; et al. Tumor mutational burden is predictive of response to immune checkpoint inhibitors in MSI-high metastatic colorectal cancer. Ann. Oncol. 2019, 30, 1096–1103. [Google Scholar] [PubMed]
- Marabelle, A.; Le, D.T.; Ascierto, P.A.; Di Giacomo, A.M.; De Jesus-Acosta, A.; Delord, J.P.; Geva, R.; Gottfried, M.; Penel, N.; Hansen, A.R.; et al. Efficacy of pembrolizumab in patients with noncolorectal high microsatellite instability/mismatch repair-deficient cancer: Results from the phase II KEYNOTE-158 study. J. Clin. Oncol. 2020, 38, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Filoglu, G.; Bulbul, O.; Rayimoglu, G.; Yediay, F.E.; Zorlu, T.; Ongoren, S.; Altuncul, H. Evaluation of reliability on STR typing at leukemic patients used for forensic purposes. Mol. Biol. Rep. 2014, 41, 3961–3972. [Google Scholar] [CrossRef] [PubMed]
- Xiao, C.; Peng, Z.; Chen, F.; Yan, H.; Zhu, B.; Tai, Y.; Qiu, P.; Liu, C.; Song, X.; Wu, Z.; et al. Mutation analysis of 19 commonly used short tandem repeat loci in a Guangdong Han population. Leg. Med. 2018, 32, 92–97. [Google Scholar] [CrossRef]
- Wu, Y.; Xu, J.; Du, C.; Wu, Y.; Xia, D.; Lv, W.; Hu, J. The predictive value of tumor mutation burden on efficacy of immune checkpoint inhibitors in cancers: A systematic review and meta-analysis. Front. Oncol. 2019, 9, 1161. [Google Scholar] [CrossRef]
- Zhang, P.; Zhu, Y.; Li, Y.; Zhu, S.; Ma, R.; Zhao, M.; Li, J. Forensic evaluation of STR typing reliability in lung cancer. Leg. Med. 2018, 30, 38–41. [Google Scholar] [CrossRef]
- Pai, C.Y.; Hsieh, L.L.; Tsai, C.W.; Chiou, F.S.; Yang, C.H.; Hsu, B.D. Allelic alterations at the STR markers in the buccal tissue cells of oral cancer patients and the oral epithelial cells of healthy betel quid-chewers: An evaluation of forensic applicability. Forensic Sci. Int. 2002, 129, 158–167. [Google Scholar] [CrossRef]
- Tilanus, M.G. Short tandem repeat markers in diagnostics: What’s in a repeat? Leukemia 2006, 20, 1353–1355. [Google Scholar] [CrossRef]
- Chalmers, Z.R.; Connelly, C.F.; Fabrizio, D.; Gay, L.; Ali, S.M.; Ennis, R.; Schrock, A.; Campbell, B.; Shlien, A.; Chmielecki, J.; et al. Analysis of 100,000 human cancer genomes reveals the landscape of tumor mutational burden. Genome Med. 2017, 9, 34. [Google Scholar] [CrossRef]
- Barroso-Sousa, R.; Jain, E.; Cohen, O.; Kim, D.; Buendia-Buendia, J.; Winer, E.; Lin, N.; Tolaney, S.M.; Wagle, N. Prevalence and mutational determinants of high tumor mutation burden in breast cancer. Ann. Oncol. 2020, 31, 387–394. [Google Scholar] [CrossRef]
- Chen, P.; Zhang, C.; Meng, Z.; Zhang, X.; Ge, M.; Qin, H. Comparison of tumor mutational burden across eight types of human cancer. J. Clin. Oncol. 2020, 38, e15170. [Google Scholar] [CrossRef]
- Wang, W.; Zhou, B.; Ding, Y.; Li, G.; Zheng, X.; Huang, P.; Yan, S.; Li, J. 1541P The genomic features of Chinese pancreatic adenocarcinoma and the implications for therapy. Ann. Oncol. 2020, 31, S945–S946. [Google Scholar] [CrossRef]
- Ji, Y.; Wu, Y.; Fu, W.; Liu, L.; Tian, Z.; Wen, S.; Zhang, K.; Yao, M.; Liu, A.; Zhou, Y. Dynamic change in the distribution of cancer types in oncology phase I trials. Ann. Oncol. 2019, 30, i12–i14. [Google Scholar] [CrossRef]
- Riley, D.E.; Krieger, J.N. Short tandem repeat (STR) replacements in UTRs and introns suggest an important role for certain STRs in gene expression and disease. Gene 2005, 344, 203–211. [Google Scholar] [CrossRef] [PubMed]
- James, A.; Matchar, D.B.; Myers, E.R. Testing for von Willebrand disease in women with menorrhagia: A systematic review. Obstet. Gynecol. 2004, 104, 381–388. [Google Scholar] [CrossRef]
- Lynham, J.; Houry, W.A. The multiple functions of the PAQosome: An R2TP- and URI1 prefoldin-based chaperone complex. Adv. Exp. Med. Biol. 2018, 1106, 37–72. [Google Scholar]
- Chaves-Pérez, A.; Yilmaz, M.; Perna, C.; de la Rosa, S.; Djouder, N. URI is required to maintain intestinal architecture during ionizing radiation. Science 2019, 364, 6443. [Google Scholar]
- Wang, Y.; Garabedian, M.J.; Logan, S.K. URI1 amplification in uterine carcinosarcoma associates with chemo-resistance and poor prognosis. Am. J. Cancer Res. 2015, 5, 2320–2329. [Google Scholar]
- Ferrín, G.; Rodríguez-Perálvarez, M.; Aguilar-Melero, P.; Ranchal, I.; Llamoza, C.; Linares, C.I.; González-Rubio, S.; Muntané, J.; Briceño, J.; López-Cillero, P.; et al. Plasma protein biomarkers of hepatocellular carcinoma in HCV-infected alcoholic patients with cirrhosis. PLoS ONE 2015, 10, e0118527. [Google Scholar] [CrossRef]
- Abdel-Hamid, N.M. Premalignant variations in extracellular matrix composition in chemically induced hepatocellular carcinoma in rats. J. Membr. Biol. 2009, 230, 155–162. [Google Scholar] [CrossRef] [PubMed]
- Yang, G.; Zheng, R.Y.; Jin, Z.S. Correlations between microsatellite instability and the biological behaviour of tumours. J. Cancer Res. Clin. Oncol. 2019, 145, 2891–2899. [Google Scholar] [CrossRef]
- Sahin, I.H.; Akce, M.; Alese, O.; Shaib, W.; Lesinski, G.B.; El-Rayes, B.; Wu, C. Immune checkpoint inhibitors for the treatment of MSI-H/MMR-D colorectal cancer and a perspective on resistance mechanisms. Br. J. Cancer 2019, 121, 809–818. [Google Scholar] [CrossRef] [PubMed]
- Kono, K.; Nakajima, S.; Mimura, K. Current status of immune checkpoint inhibitors for gastric cancer. Gastric Cancer 2020, 23, 565–578. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.B.; Lee, S.Y.; Kim, J.H.; Sung, I.K.; Park, H.S.; Shim, C.S.; Han, H.S. Microsatellite instability of gastric and colorectal cancers as a predictor of synchronous gastric or colorectal neoplasms. Gut Liver 2016, 10, 220–227. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Boland, C.R.; Thibodeau, S.N.; Hamilton, S.R.; Sidransky, D.; Eshleman, J.R.; Burt, R.W.; Meltzer, S.J.; Rodriguez-Bigas, M.A.; Fodde, R.; Ranzani, G.N.; et al. A national cancer institute workshop on microsatellite instability for cancer detection and familial predisposition: Development of international criteria for the determination of microsatellite instability in colorectal cancer. Cancer Res. 1998, 58, 5248–5257. [Google Scholar]
- Kim, J.G.; Shin, S.; Park, J. Comparison between mononucleotide and dinucleotide marker panels in gastric cancer with loss of hMLH1 or hMSH2 expression. Int. J. Biol. Markers 2017, 32, e352–e356. [Google Scholar] [CrossRef]
- Egoavil, C.; Alenda, C.; Castillejo, A.; Paya, A.; Peiro, G.; Sánchez-Heras, A.B.; Castillejo, M.I.; Rojas, E.; Barberá, V.M.; Cigüenza, S.; et al. Prevalence of Lynch syndrome among patients with newly diagnosed endometrial cancers. PLoS ONE 2013, 8, e79737. [Google Scholar] [CrossRef]
- Liu, X.; Yang, Z.; Latchoumanin, O.; Qiao, L. Antagonizing programmed death-1 and programmed death ligand-1 as a therapeutic approach for gastric cancer. Ther. Adv. Gastroenterol. 2016, 9, 853–860. [Google Scholar] [CrossRef]
- Laiho, P.; Launonen, V.; Lahermo, P.; Esteller, M.; Guo, M.; Herman, J.G.; Mecklin, J.P.; Järvinen, H.; Sistonen, P.; Kim, K.M.; et al. Low-level microsatellite instability in most colorectal carcinomas. Cancer Res. 2002, 62, 1166–1170. [Google Scholar]
- Trabucco, S.E.; Gowen, K.; Maund, S.L.; Sanford, E.; Fabrizio, D.A.; Hall, M.J.; Yakirevich, E.; Gregg, J.P.; Stephens, P.J. Frampton GM et al: A novel next-generation sequencing approach to detecting microsatellite instability and pan-tumor characterization of 1000 microsatellite instability-high cases in 67,000 patient samples. J. Mol. Diagn. JMD 2019, 21, 1053–1066. [Google Scholar] [CrossRef] [PubMed]
- Ma, J.; Sun, D.; Wang, J.; Han, C.; Qian, Y.; Chen, G.; Li, X.; Zhang, J.; Cui, P.; Du, W.; et al. Immune checkpoint inhibitors combined with chemotherapy for the treatment of advanced pancreatic cancer patients. Cancer Immunol. Immunother. 2020, 69, 365–372. [Google Scholar] [PubMed]
- Wu, X.; Gu, Z.; Chen, Y.; Chen, B.; Chen, W.; Weng, L.; Liu, X. Application of PD-1 blockade in cancer immunotherapy. Comput. Struct. Biotechnol. J. 2019, 17, 661–674. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Zhang, X.; Ge, M.; Qin, H. Analysis of microsatellite instability differences in eight types of tumors. J. Clin. Oncol. 2020, 38 (Suppl. 15), e15174. [Google Scholar] [CrossRef]
- Lin, W.; Chen, R.; Yi, Y.; Lin, G.; Zhao, J.; Yuan, M.; Guan, Y.; Xia, X. P2.04-54 Characteristic of MSI-H lung cancer patients identified with targeted next-generation sequencing. J. Thorac. Oncol. 2019, 14 (Suppl. 10), S729. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Locus | Germline Mutation Frequency [14,15] | BC | HCC | PC | CRC | GC | LC | EC | RCC |
|---|---|---|---|---|---|---|---|---|---|
| D19S433 | 0.11% | 0.00% | 0.00% | 2.86% | 14.73% | 14.05% | 8.00% | 33.33% | 0.00% |
| D7S820 | 0.10% | 2.78% | 0.00% | 2.94% | 10.08% | 14.05% | 8.33% | 22.22% | 4.55% |
| D6S1043 | 0.14% | 2.78% | 26.67% | 7.14% | 13.18% | 17.50% | 8.33% | 33.33% | 15.00% |
| CSF1PO | 0.16% | 2.78% | 3.33% | 6.25% | 23.26% | 21.49% | 12.00% | 11.11% | 0.00% |
| D5S818 | 0.11% | 0.00% | 0.00% | 8.57% | 24.81% | 12.40% | 20.00% | 11.11% | 0.00% |
| FGA | 0.28% | 2.78% | 30.00% | 6.45% | 24.03% | 19.33% | 12.50% | 33.33% | 4.55% |
| D3S1358 | 0.12% | 5.56% | 10.00% | 5.71% | 9.30% | 12.40% | 16.00% | 44.44% | 13.64% |
| D2S1338 | 0.12% | 2.78% | 6.67% | 2.86% | 13.18% | 15.70% | 16.00% | 22.22% | 4.55% |
| TPOX | 0.01% | 2.78% | 3.33% | 0.00% | 7.75% | 5.79% | 4.00% | 11.11% | 0.00% |
| D21S11 | 0.19% | 0.00% | 3.33% | 6.45% | 14.73% | 10.74% | 20.83% | 33.33% | 9.09% |
| Penta D | 0.14% | 0.00% | 3.33% | 6.45% | 15.50% | 16.81% | 16.67% | 22.22% | 13.64% |
| D18S51 | 0.22% | 5.56% | 6.67% | 9.38% | 43.41% | 21.85% | 16.00% | 22.22% | 9.09% |
| D16S539 | 0.11% | 11.11% | 23.33% | 2.86% | 9.30% | 14.88% | 4.00% | 0.00% | 0.00% |
| Penta E | 0.16% | 11.11% | 6.67% | 7.14% | 26.56% | 19.33% | 20.83% | 33.33% | 9.09% |
| D13S317 | 0.14% | 11.11% | 36.67% | 2.94% | 13.28% | 9.92% | 36.00% | 44.44% | 4.55% |
| D12S391 | 0.24% | 8.33% | 13.33% | 9.68% | 13.95% | 16.53% | 16.67% | 22.22% | 4.55% |
| Vwa | 0.17% | 8.33% | 13.33% | 11.43% | 16.67% | 16.81% | 4.00% | 33.33% | 4.55% |
| TH01 | 0.01% | 8.33% | 3.33% | 2.86% | 10.08% | 9.09% | 4.00% | 22.22% | 9.09% |
| D8S1179 | 0.14% | 11.11% | 16.67% | 5.71% | 16.28% | 15.70% | 12.00% | 33.33% | 9.09% |
| Average | ☐ | 5.12% | 10.88% | 5.67% | 16.85% | 14.97% | 13.48% | 25.73% | 6.05% |
| Standard deviation | ☐ | 4.06% | 10.70% | 2.87% | 8.28% | 4.11% | 7.76% | 11.43% | 4.80% |
| Tumor Type | No. of Loci | MSI Loci | MSI Status | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| NR21 | BAT26 | NR27 | BAT25 | NR24 | MONO27 | MSS | MSI-L | MSI-H | ||
| BC | S | 36 | 36 | 36 | 36 | 36 | 36 | 36 (100%) | 0 (0%) | 0 (0%) |
| I | 0 | 0 | 0 | 0 | 0 | 0 | ||||
| HCC | S | 30 | 30 | 30 | 30 | 30 | 30 | 30 (100%) | 0 (0%) | 0 (0%) |
| I | 0 | 0 | 0 | 0 | 0 | 0 | ||||
| PC | S | 35 | 35 | 35 | 35 | 35 | 35 | 35 (100%) | 0 (0%) | 0 (0%) |
| I | 0 | 0 | 0 | 0 | 0 | 0 | ||||
| CRC | S | 124 | 123 | 123 | 122 | 124 | 125 | 122 (94.57%) | 1 (0.78%) | 6 (4.65%) |
| I | 5 | 6 | 6 | 7 | 5 | 4 | ||||
| GC | S | 113 | 113 | 113 | 110 | 114 | 112 | 109 (90.08%) | 3 (2.48%) | 9 (7.44%) |
| I | 8 | 8 | 8 | 11 | 7 | 9 | ||||
| LC | S | 25 | 25 | 25 | 25 | 25 | 25 | 25 (100%) | 0 (0%) | 0 (0%) |
| I | 0 | 0 | 0 | 0 | 0 | 0 | ||||
| EC | S | 9 | 9 | 9 | 9 | 9 | 9 | 9 (100%) | 0 (0%) | 0 (0%) |
| I | 0 | 0 | 0 | 0 | 0 | 0 | ||||
| RCC | S | 22 | 22 | 22 | 22 | 22 | 22 | 22 (100%) | 0 (0%) | 0 (0%) |
| I | 0 | 0 | 0 | 0 | 0 | 0 | ||||
| Sample ID | Tumor Type | Alteration (%) | Status | |
|---|---|---|---|---|
| STR | MSI | |||
| 138 | CRC | 84.21% | 100.00% | MSI-H |
| 166 | CRC | 55.56% | 83.33% | MSI-H |
| 180 | CRC | 68.42% | 100.00% | MSI-H |
| 200 | CRC | 31.58% | 16.67% | MSI-L |
| 214 | CRC | 52.63% | 83.33% | MSI-H |
| 220 | CRC | 78.95% | 100.00% | MSI-H |
| 230 | CRC | 42.11% | 66.67% | MSI-H |
| 237 | GC | 78.95% | 100.00% | MSI-H |
| 244 | GC | 26.32% | 33.33% | MSI-H |
| 245 | GC | 47.37% | 16.67% | MSI-L |
| 247 | GC | 36.84% | 100.00% | MSI-H |
| 272 | GC | 73.68% | 100.00% | MSI-H |
| 286 | GC | 52.63% | 100.00% | MSI-H |
| 300 | GC | 68.42% | 100.00% | MSI-H |
| 302 | GC | 52.63% | 16.67% | MSI-L |
| 307 | GC | 36.84% | 100.00% | MSI-H |
| 312 | GC | 73.68% | 16.67% | MSI-L |
| 328 | GC | 31.58% | 83.33% | MSI-H |
| 337 | GC | 68.42% | 100.00% | MSI-H |
| Tumor Type | No. of Total Samples | Cutoff of STR Alterations | ORR with Anti-PD1 or Anti-PD-L1 [7] | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ≥5.26% (1 Out of 19) | ≥10.53% (2 Out of 19) | ≥15.79% (3 Out of 19) | ≥21.05% (4 Out of 19) | ≥26.32% (5 Out of 19) | ≥31.58% (6 Out of 19) | |||||||||
| Sample No. | Perc. | Sample No. | Perc. | Sample No. | Perc. | Sample No. | Perc. | Sample No. | Perc. | Sample No. | Perc. | |||
| BC | 36 | 13 | 36.11% | 5 | 13.89% | 4 | 11.11% | 4 | 11.11% | 4 | 11.11% | 1 | 2.78% | ~5% |
| HCC | 30 | 19 | 63.33% | 15 | 50.00% | 11 | 36.67% | 8 | 26.67% | 6 | 20.00% | 3 | 10.00% | ~17% |
| PC | 35 | 9 | 25.71% | 5 | 14.29% | 3 | 8.57% | 3 | 8.57% | 3 | 8.57% | 2 | 5.71% | ~0% |
| CRC | 129 | 90 | 69.77% | 80 | 62.02% | 67 | 51.94% | 51 | 39.53% | 44 | 34.11% | 24 | 18.60% | ~30% |
| GC | 121 | 66 | 54.55% | 48 | 39.67% | 42 | 34.71% | 37 | 30.58% | 36 | 29.75% | 30 | 24.79% | ~30% |
| LC | 25 | 12 | 48.00% | 12 | 48.00% | 10 | 40.00% | 8 | 32.00% | 6 | 24.00% | 6 | 24.00% | ~21% |
| EC | 9 | 7 | 77.78% | 7 | 77.78% | 5 | 55.56% | 5 | 55.56% | 4 | 44.44% | 4 | 44.44% | 22–23.5% |
| RCC | 22 | 9 | 40.91% | 4 | 18.18% | 3 | 13.64% | 2 | 9.09% | 2 | 9.09% | 1 | 4.55% | ~25% |
| Tumor Type | No. of Total Samples | Cutoff of STR Alterations | ORR with Anti-PD1 or Anti-PD-L1 [7] | |||||||||||
| ≥36.84% (7 Out of 19) | ≥42.11% (8 Out of 19) | ≥47.37% (9 Out of 19) | ≥52.63% (10 Out of 19) | ≥57.89% (11 Out of 19) | ☐ | |||||||||
| Sample No. | Perc. | Sample No. | Perc. | Sample No. | Perc. | Sample No. | Perc. | Sample No. | Perc. | ☐ | ☐ | |||
| BC | 36 | 1 | 2.78% | 1 | 2.78% | 1 | 2.78% | 1 | 2.78% | 0 | 0.00% | ☐ | ☐ | ~5% |
| HCC | 30 | 0 | 0.00% | 0 | 0.00% | 0 | 0.00% | 0 | 0.00% | 0 | 0.00% | ☐ | ☐ | ~17% |
| PC | 35 | 2 | 5.71% | 2 | 5.71% | 2 | 5.71% | 2 | 5.71% | 1 | 2.86% | ☐ | ☐ | ~0% |
| CRC | 129 | 17 | 13.18% | 11 | 8.53% | 8 | 6.20% | 5 | 3.88% | 3 | 2.33% | ☐ | ☐ | ~30% |
| GC | 121 | 21 | 17.36% | 17 | 14.05% | 13 | 10.74% | 9 | 7.44% | 7 | 5.79% | ☐ | ☐ | ~30% |
| LC | 25 | 4 | 16.00% | 2 | 8.00% | 2 | 8.00% | 1 | 4.00% | 1 | 4.00% | ☐ | ☐ | ~21% |
| EC | 9 | 4 | 44.44% | 3 | 33.33% | 2 | 22.22% | 2 | 22.22% | 1 | 11.11% | ☐ | ☐ | 22–23.5% |
| RCC | 22 | 1 | 4.55% | 1 | 4.55% | 1 | 4.55% | 1 | 4.55% | 0 | 0.00% | ☐ | ☐ | ~25% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, A.; Zhang, S.; Xiong, L.; Xi, S.; Tao, R.; Chen, C.; Li, J.; Chen, J.; Li, C. Investigation of an Alternative Marker for Hypermutability Evaluation in Different Tumors. Genes 2021, 12, 197. https://doi.org/10.3390/genes12020197
Chen A, Zhang S, Xiong L, Xi S, Tao R, Chen C, Li J, Chen J, Li C. Investigation of an Alternative Marker for Hypermutability Evaluation in Different Tumors. Genes. 2021; 12(2):197. https://doi.org/10.3390/genes12020197
Chicago/Turabian StyleChen, Anqi, Suhua Zhang, Lei Xiong, Shihan Xi, Ruiyang Tao, Chong Chen, Jixi Li, Jinzhong Chen, and Chengtao Li. 2021. "Investigation of an Alternative Marker for Hypermutability Evaluation in Different Tumors" Genes 12, no. 2: 197. https://doi.org/10.3390/genes12020197
APA StyleChen, A., Zhang, S., Xiong, L., Xi, S., Tao, R., Chen, C., Li, J., Chen, J., & Li, C. (2021). Investigation of an Alternative Marker for Hypermutability Evaluation in Different Tumors. Genes, 12(2), 197. https://doi.org/10.3390/genes12020197