
Adiponectin Gene Polymorphism (rs17300539) Has No Influence on the Occurrence of Metabolic Syndrome in Women with Polycystic Ovary Syndrome

 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
- (a)
- Waist circumference >= 80 cm;
- (b)
- Fasting glucose > 100 mg/dL or treatment of type 2 diabetes;
- (c)
- Triglyceride concentration >= 150 mg/dL;
- (d)
- HDL cholesterol < 50 mg/dL;
- (e)
- Elevated blood pressure: systolic >= 130 mmHg and or diastolic >= 85 mmHg or treatment of previously diagnosed arterial hypertension. The study included patients who were not treated pharmacologically due to chronic diseases, following a normal diet. The characteristics of the study group are presented in the table below (Table 1).
2.2. Gynecologic Examination and Anthropometry
2.3. Laboratory Tests
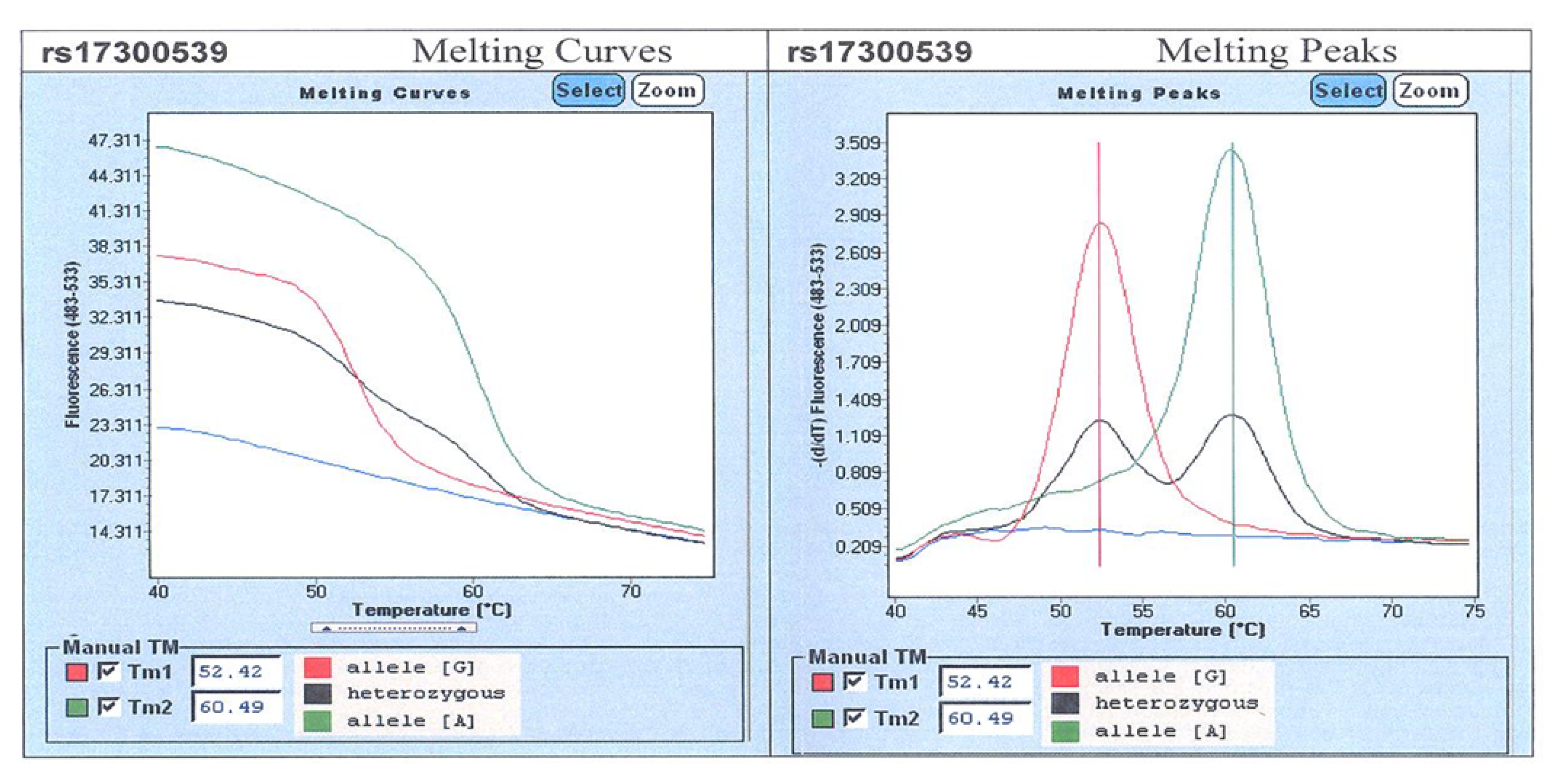
2.4. Genetic Testing
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- National Institutes of Health. Evidence-Based Methodology Workshop on Polycystic Ovary Syndrome. Final Report. Available online: https://prevention.nih.gov/docs/programs/pcos/FinalReport.pdf (accessed on 16 December 2016).
- Fauser, B.C.; Tarlatzis, B.C.; Rebar, R.W.; Legro, R.; Balen, A.H.; Lobo, R.; Carmina, E.; Chang, J.; Yildiz, B.O.; Laven, J.S.; et al. Consensus on women’s health aspects of polycystic ovary syndrome (PCOS): The Amsterdam ESHRE/ASRM-Sponsored 3rd PCOS Consensus Workshop Group. Fertil. Steril. 2012, 97, 28–38.e25. [Google Scholar] [CrossRef]
- Szczuko, M.; Kikut, J.; Szczuko, U.; Szydłowska, I.; Nawrocka-Rutkowska, J.; Ziętek, M.; Verbanac, D.; Saso, L. Nutrition Strategy and Life Style in Polycystic Ovary Syndrome—Narrative Review. Nutrients 2021, 13, 2452. [Google Scholar] [CrossRef] [PubMed]
- Speroff, L.; Fritz, M. Clinical Gynecologic Endocrinology and Infertility, 8th ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2010. [Google Scholar]
- Skałba, P. Diagnostics and Treatment of Endocrine Disorders in Gynecology, 1st ed.; Medycyna Praktyczna: Krakow, Poland, 2014. [Google Scholar]
- Szczuko, M.; Zapałowska-Chwyć, M.; Maciejewska, D.; Drozd, A.; Starczewski, A.; Stachowska, E. High glycemic index diet in PCOS patients. The analysis of IGF I and TNF-α pathways in metabolic disorders. Med. Hypotheses 2016, 96, 42–47. [Google Scholar] [CrossRef]
- Szczuko, M.; Zapałowska-Chwyć, M.; Drozd, A.; Maciejewska, D.; Starczewski, A.; Stachowska, E. Effect of IGF-I and TNF-α on intensification of steroid pathways in women with PCOS phenotypes are not identical. Enhancement of progesterone pathway in women with PCOS increases the concentration of TNF-α. Gynecol. Endocrinol. 2016, 32, 714–717. [Google Scholar] [CrossRef]
- Hutley, L.; Prins, J.B. Fat as an Endocrine Organ: Relationship to the Metabolic Syndrome. Am. J. Med. Sci. 2005, 330, 280–289. [Google Scholar] [CrossRef]
- Fang, H.; Judd, R.L. Adiponectin Regulation and Function. Compr. Physiol. 2011, 8, 1031–1063. [Google Scholar]
- Achari, A.E.; Jain, S.K. Adiponectin, a Therapeutic Target for Obesity, Diabetes, and Endothelial Dysfunction. Int. J. Mol. Sci. 2017, 18, 1321. [Google Scholar] [CrossRef] [Green Version]
- Howlader, M.; Sultana, M.I.; Akter, F.; Hossain, M. Adiponectin gene polymorphisms associated with diabetes mellitus: A descriptive review. Heliyon 2021, 7, e07851. [Google Scholar] [CrossRef]
- Hou, H.; Ge, S.; Zhao, L.; Wang, C.; Wang, W.; Zhao, X.; Sun, Z. An Updated Systematic Review and Meta-analysis of Association Between Adiponectin Gene Polymorphisms and Coronary Artery Disease. OMICS J. Integr. Biol. 2017, 21, 340–351. [Google Scholar] [CrossRef]
- Garcia-Garcia, M.R.; Morales-Lanuza, M.A.; Campos-Perez, W.Y.; Ruiz-Madrigal, B.; Maldonado-Gonzalez, M.; Vizmanos, B.; Hernandez-Cañaveral, I.; Yañez-Sanchez, I.; Roman, S.; Panduro, A.; et al. Effect of the ADIPOQ Gene—11391 G/A Polymorphism Is Modulated by Lifestyle Factors in Mexican Subjects. J. Nutr. Nutr. 2014, 7, 212–224. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Wu, Q.H.; Jiao, M.L.; Fan, X.H.; Hu, Q.; Hao, Y.H.; Liu, R.H.; Zhang, W.; Cui, Y.; Han, L.Y. Gene-environment interaction between adiponectin gene polymorphisms and environmental factors on the risk of diabetic retinopathy. J. Diabetes Investig. 2015, 6, 56–66. [Google Scholar] [CrossRef]
- Han, L.Y.; Wu, Q.H.; Jiao, M.L.; Hao, Y.H.; Liang, L.B.; Gao, L.J.; Legge, D.G.; Quan, H.; Zhao, M.M.; Ning, N.; et al. Associations between single-nucleotide polymorphisms (+45T>G, +276G>T, −11377C>G, −11391G>A) of adiponectin gene and type 2 diabetes mellitus: A systematic review and meta-analysis. Diabetologia 2011, 54, 2303–2314. [Google Scholar] [CrossRef] [Green Version]
- Rotterdam Criteria from 2003”, “Modified Criteria of the International Diabetes Federation (IDF) from 2009” and “Korotkoff Method”. Available online: https://doi.org/10.1093/humrep/deh098 (accessed on 16 September 2021).
- Madani, T.; Hosseini, R.; Ramezanali, F.; Khalili, G.; Jahangiri, N.; Ahmadi, J.; Rastegar, F.; Zolfaghari, Z. Metabolic syndrome in infertile women with polycystic ovarian syndrome. Arch. Endocrinol. Metab. 2016, 60, 199–204. [Google Scholar] [CrossRef] [Green Version]
- Moran, L.; Teede, H. Metabolic features of the reproductive phenotypes of polycystic ovary syndrome. Hum. Reprod. Updat. 2009, 15, 477–488. [Google Scholar] [CrossRef] [PubMed]
- Tabrizi, F.P.F.; Alipour, B.; Sadaghiani, M.M.; Ostadrahimi, A.; Mahdavi, A.M. Metabolic Syndrome and Its Characteristics among Reproductive-Aged Women with Polycystic Ovary Syndrome: A Cross-sectional Study in Northwest Iran. Int. J. Fertil. Steril. 2013, 6, 244–249. [Google Scholar]
- Cussons, A.J.; Watts, G.F.; Burke, V.; Shaw, J.E.; Zimmet, P.Z.; Stuckey, B.G. Cardiometabolic risk in polycystic ovary syndrome: A comparison of different approaches to defining the metabolic syndrome. Hum. Reprod. 2008, 23, 2352–2358. [Google Scholar] [CrossRef] [Green Version]
- Ehrmann, D.A.; Liljenquist, D.R.; Kasza, K.; Azziz, R.; Legro, R.S.; Ghazzi, M.N. Prevalence and Predictors of the Metabolic Syndrome in Women with Polycystic Ovary Syndrome. J. Clin. Endocrinol. Metab. 2006, 91, 48–53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carmina, E.; Napoli, N.; Longo, R.A.; Rini, G.B.; Lobo, R.A. Metabolic syndrome in polycystic ovary syndrome (PCOS): Lower prevalence in southern Italy than in the USA and the influence of criteria for the diagnosis of PCOS. Eur. J. Endocrinol. 2006, 154, 141–145. [Google Scholar] [CrossRef]
- Park, H.R.; Choi, Y.; Lee, H.J.; Oh, J.Y.; Hong, Y.S.; Sung, Y.A. The metabolic syndrome in young Korean women with polycystic ovary syndrome. Diabetes Res. Clin. Pract. 2007, 77, 3. [Google Scholar] [CrossRef] [PubMed]
- Soares, E.M.M.; Azevedo, G.D.; Gadelha, R.G.N.; Lemos, T.M.A.M.; Maranhão, T.M.O. Prevalence of the metabolic syndrome and its components in Brazilian women with polycystic ovary syndrome. Fertil. Steril. 2008, 89, 649–655. [Google Scholar] [CrossRef] [Green Version]
- Bhattacharya, S.M. Prevalence of metabolic syndrome in women with polycystic ovary syndrome, using two proposed definitions. Gynecol. Endocrinol. 2010, 26, 516–520. [Google Scholar] [CrossRef] [PubMed]
- Glueck, C.J.; Papanna, R.; Wang, P.; Goldenberg, N.; Sieve-Smith, L. Incidence and treatment of metabolic syndrome in newly referred women with confirmed polycystic ovarian syndrome. Metabolism 2003, 52, 908–915. [Google Scholar] [CrossRef]
- Szczuko, M.; Zapałowska-Chwyć, M.; Drozd, A.; Maciejewska, D.; Starczewski, A.; Stachowska, E. Metabolic pathways of oleic and palmitic acid are intensified in PCOS patients with normal androgen levels. Prostaglandins Leukot. Essent. Fat. Acids 2017, 126, 105–111. [Google Scholar] [CrossRef]
- Szczuko, M.; Splinter, J.; Zapałowska-Chwyć, M.; Ziętek, M.; Maciejewska, D. Fluorine may intensify the mechanisms of polycystic ovary syndrome (PCOS) development via increased insulin resistance and disturbed thyroid-stimulating hormone (TSH) synthesis even at reference levels. Med. Hypotheses 2019, 128, 58–63. [Google Scholar] [CrossRef] [PubMed]
- Szczuko, M.; Zapalowska-Chwyć, M.; Drozd, R. A Low Glycemic Index Decreases Inflammation by Increasing the Concentration of Uric Acid and the Activity of Glutathione Peroxidase (GPx3) in Patients with Polycystic Ovary Syndrome (PCOS). Molecules 2019, 24, 1508. [Google Scholar] [CrossRef] [Green Version]
- Kyrkou, G.; Trakakis, E.; Attilakos, A.; Panagopoulos, P.; Chrelias, C.; Papadimitriou, A.; Vaggopoulos, V.; Alexiou, E.; Mastorakos, G.; Lykeridou, A.; et al. Metabolic syndrome in Greek women with polycystic ovary syndrome: Prevalence, characteristics and associations with body mass index. A prospective controlled study. Arch. Gynecol. Obstet. 2016, 293, 915–923. [Google Scholar] [CrossRef]
- Kahsar-Miller, M.D.; Nixon, C.; Boots, L.R.; Go, R.C.; Azziz, R. Prevalence of polycystic ovary syndrome (PCOS) in first-degree relatives of patients with PCOS. Fertil. Steril. 2001, 75, 53–58. [Google Scholar] [CrossRef]
- Trottier, A.; Battista, M.-C.; Geller, D.H.; Moreau, B.; Carpentier, A.C.; Simoneau-Roy, J.; Baillargeon, J.-P. Adipose tissue insulin resistance in peripubertal girls with first-degree family history of polycystic ovary syndrome. Fertil. Steril. 2012, 98, 1627–1634. [Google Scholar] [CrossRef] [Green Version]
- Sir-Petermann, T.; Codner, E.; Perez, V.; Echiburu, B.; Maliqueo, M.; Ladron de Guevara, A.; Preisler, J.; Crisosto, N.; Sanchez, F.; Cassorla, F.; et al. Metabolic and reproductive features before and during puberty in daughters of women with polycystic ovary syndrome. J. Clin. Endocrinol. Metab. 2009, 94, 1923–1930. [Google Scholar] [CrossRef] [Green Version]
- Sun, X.; Wu, X.; Duan, Y.; Liu, G.; Yu, X.; Zhang, W. Family-Based Association Study of rs17300539 and rs12495941 Polymorphism in Adiponectin Gene and Polycystic Ovary Syndrome in a Chinese Population. Med. Sci. Monit. 2017, 23, 78–84. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fumeron, F.; Aubert, R.; Siddiq, A.; Betoulle, D.; Péan, F.; Hadjadj, S.; Tichet, J.; Wilpart, E.; Chesnier, M.-C.; Balkau, B.; et al. Adiponectin Gene Polymorphisms and Adiponectin Levels Are Independently Associated with the Development of Hyperglycemia During a 3-Year Period: The Epidemiologic Data on the Insulin Resistance Syndrome Prospective Study. Diabetes 2004, 53, 1150–1157. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hasani-Ranjbar, S.; Amoli, M.M.; Tabatabaei-Malazy, O.; Rumi, Y.; Tavakkoly-Bazzaz, J.; Samimi, H.; Abbasifarid, E. Effect of adiponectin gene polymorphisms on waist circumference in patients with diabetes. J. Diabetes Metab. Disord. 2012, 11, 14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karmelić, I.; Lovrić, J.; Božina, T.; Ljubić, H.; Vogrinc, Ž.; Božina, N.; Sertić, J. Adiponectin Level and Gene Variability Are Obesity and Metabolic Syndrome Markers in a Young Population. Arch. Med. Res. 2012, 43, 145–153. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jang, Y.; Chae, J.S.; Koh, S.J.; Hyun, Y.J.; Kim, J.Y.; Jeong, Y.J.; Park, S.; Ahn, C.-M.; Lee, J.H. The influence of the adiponectin gene on adiponectin concentrations and parameters of metabolic syndrome in non-diabetic Korean women. Clin. Chim. Acta 2008, 391, 85–90. [Google Scholar] [CrossRef]


{kind=link}
| C (n = 50) Mean ± SD | B1 (n = 81) Mean ± SD | B2 (n = 70) Mean ± SD | P C vs. B1 | P C vs. B2 | P B1 vs. B2 | |
|---|---|---|---|---|---|---|
| Age (year) | 28.48 ± 3.88 | 27.17 ± 4.14 | 28.39 ± 4.91 | 0.655 | 0.991 | 0.125 |
| BMI (kg/m2) | 21.81 ± 1.63 | 22.52 ± 4.08 | 31.52 ± 6.46 | 0.068 | 0.000 | 0.000 |
| WC (cm) | 73.26 ± 5.33 | 76.10 ± 9.98 | 94.64 ± 12.71 | 0.079 | 0.000 | 0.000 |
| GLU (mg/dL) | 88.89 ± 8.26 | 89.74 ± 8.55 | 94.34 ± 10.43 | 0.151 | 0.000 | 0.000 |
| TGL (mg/dL) | 112.89 ± 20.81 | 75.26 ± 29.27 | 145.61 ± 63.21 | 0.000 | 0.000 | 0.000 |
| HDL (mg/dL) | 58.51 ± 8.94 | 66.67 ± 22.84 | 47.82 ± 12.67 | 0.000 | 0.000 | 0.000 |
| SBP (mmHg) | 115.60 ± 8.60 | 112.85 ± 11.42 | 136.00 ± 10.70 | 0.980 | 0.000 | 0.000 |
| DBP (mmHg) | 72.22 ± 7.31 | 70.60 ± 9.66 | 85.54 ± 8.80 | 0.315 | 0.000 | 0.000 |
| Genotype | K (n = 50) | B1 (n = 81) | B2 (n = 70) | Overall |
|---|---|---|---|---|
| GG | n = 45 (90.00%) | n = 71 (87.65%) | n = 62 (88.57%) | n = 178 |
| GA | n = 5 (10.00%) | n = 10 (12.35%) | n = 7 (10.00%) | n = 22 |
| AA | n = 0 (0.00%) | n = 0 (0.00%) | n = 1 (1.43%) | n = 1 |
| Chi-square | 2.13 | df = 4 | p = 0.71118 |
| Groups | Genotype | OR | 95%CI | p |
|---|---|---|---|---|
| B1 vs. K | GG | 0.79 | 0.25–2.46 | 0.683 |
| B1 vs. K | GA | 1.27 | 0.41–3.95 | 0.683 |
| B2 vs. K | GG | 0.86 | 0.26–2.81 | 0.804 |
| B2 vs. K | GA | 1.00 | 0.30–3.35 | 1.000 |
| B2 vs. B1 | GG | 1.09 | 0.41–2.94 | 0.862 |
| B2 vs. B1 | GA | 0.79 | 0.28–2.20 | 0.650 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nowak, I.; Ciećwież, S.; Łój, B.; Brodowski, J.; Brodowska, A. Adiponectin Gene Polymorphism (rs17300539) Has No Influence on the Occurrence of Metabolic Syndrome in Women with Polycystic Ovary Syndrome. Genes 2021, 12, 1902. https://doi.org/10.3390/genes12121902
Nowak I, Ciećwież S, Łój B, Brodowski J, Brodowska A. Adiponectin Gene Polymorphism (rs17300539) Has No Influence on the Occurrence of Metabolic Syndrome in Women with Polycystic Ovary Syndrome. Genes. 2021; 12(12):1902. https://doi.org/10.3390/genes12121902
Chicago/Turabian StyleNowak, Izabela, Sylwester Ciećwież, Beata Łój, Jacek Brodowski, and Agnieszka Brodowska. 2021. "Adiponectin Gene Polymorphism (rs17300539) Has No Influence on the Occurrence of Metabolic Syndrome in Women with Polycystic Ovary Syndrome" Genes 12, no. 12: 1902. https://doi.org/10.3390/genes12121902
APA StyleNowak, I., Ciećwież, S., Łój, B., Brodowski, J., & Brodowska, A. (2021). Adiponectin Gene Polymorphism (rs17300539) Has No Influence on the Occurrence of Metabolic Syndrome in Women with Polycystic Ovary Syndrome. Genes, 12(12), 1902. https://doi.org/10.3390/genes12121902