Total Tumor Load of mRNA Cytokeratin 19 in the Sentinel Lymph Node as a Predictive Value of Axillary Lymphadenectomy in Patients with Neoadjuvant Breast Cancer

 and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Sentinel Lymph Node Sampling
2.2. One-Step Nucleic Acid Amplification Assay
2.3. Statistical Analysis
3. Results
3.1. Patient Characteristics and Pathological Findings
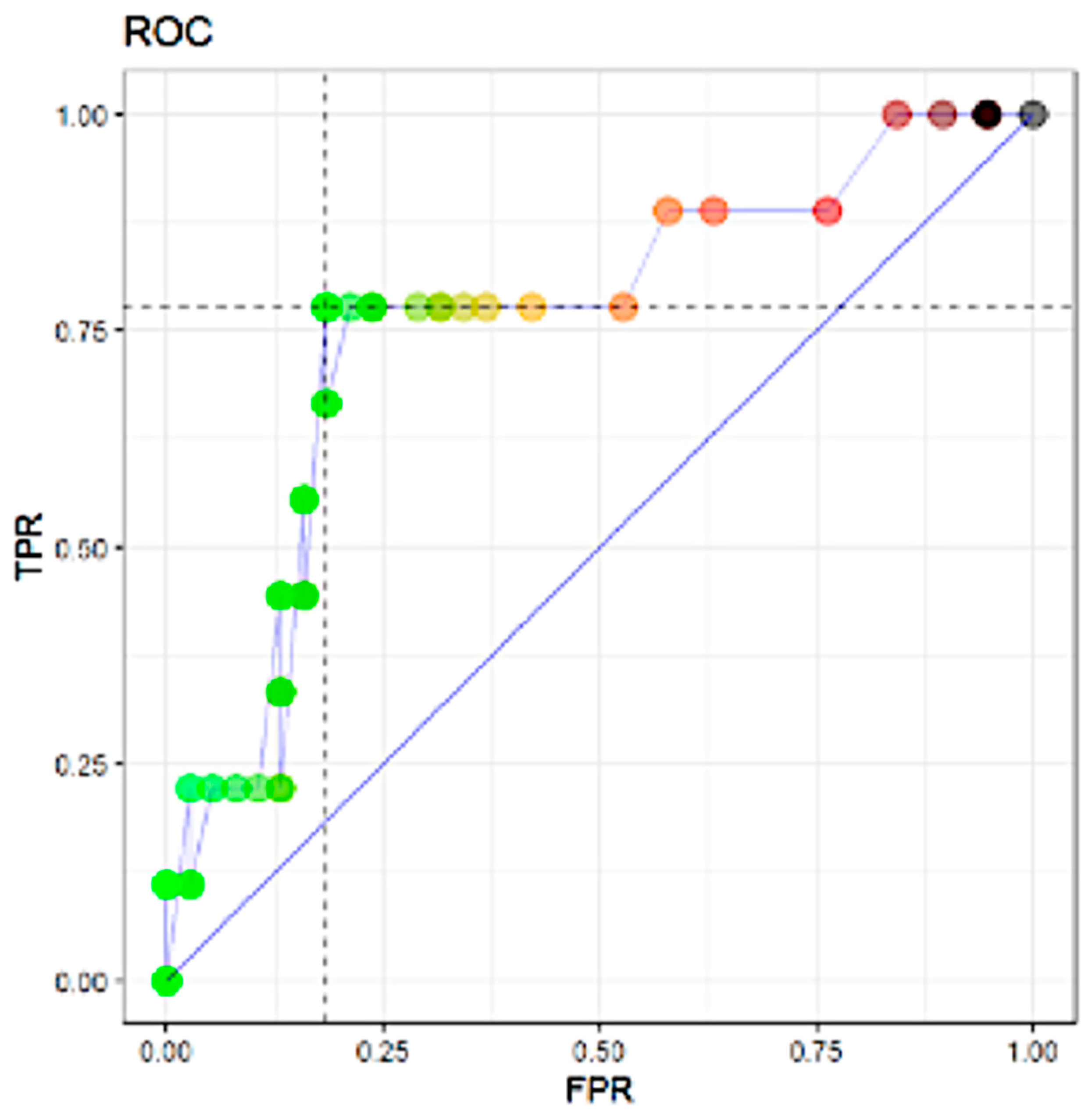
3.2. ROC Analysis
3.3. Correlation between Total Tumor Load and Positive Lymph Nodes in Axillar Lymphadenectomy
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lyman, G.H.; Somerfield, M.R.; Bosserman, L.D.; Perkins, C.L.; Weaver, D.L.; Giuliano, A.E. Sentinel Lymph Node Biopsy for Patients with Early-Stage Breast Cancer: American Society of Clinical Oncology Clinical Practice Guideline Update. J. Clin. Oncol. 2017, 35, 561–564. [Google Scholar] [CrossRef] [PubMed]
- Manca, G.; Rubello, D.; Tardelli, E.; Giammarile, F.; Mazzarri, S.; Boni, G.; Chondrogiannis, S.; Marzola, M.C.; Chiacchio, S.; Ghilli, M.; et al. Sentinel Lymph Node Biopsy in Breast Cancer: Indications, Contraindications, and Controversies. Clin. Nucl. Med. 2016, 41, 126–133. [Google Scholar] [CrossRef] [PubMed]
- Wong, W.; Rubenchik, I.; Nofech-Mozes, S.; Slodkowska, E.; Parra-Herran, C.; Hanna, W.M.; Lu, F.-I. Intraoperative Assessment of Sentinel Lymph Nodes in Breast Cancer Patients Post-Neoadjuvant Therapy. Technol. Cancer Res. Treat. 2019, 18, 1533033818821104. [Google Scholar] [CrossRef] [PubMed]
- Giuliano, A.E.; Ballman, K.V.; McCall, L.; Beitsch, P.; Brennan, M.B.; Kelemen, P.R.; Ollila, D.W.; Hansen, N.M.; Whitworth, P.; Blumencranz, P.W.; et al. Effect of Axillary Dissection vs No Axillary Dissection on 10-Year Overall Survival Among Women With Invasive Breast Cancer and Sentinel Node Metastasis: The ACOSOG Z0011 (Alliance) Randomized Clinical Trial. JAMA 2017, 318, 918–926. [Google Scholar] [CrossRef]
- Mieog, J.S.D.; Van Der Hage, J.A.; Van De Velde, C.J.H. Neoadjuvant chemotherapy for operable breast cancer. BJS 2007, 94, 1189–1200. [Google Scholar] [CrossRef]
- Van Der Hage, J.H.; Van De Velde, C.C.; Mieog, S.J. Preoperative chemotherapy for women with operable breast cancer. Cochrane Database Syst. Rev. 2007, 2007, CD005002. [Google Scholar] [CrossRef]
- Li, X.; Wang, M.; Wang, M.; Yu, X.; Guo, J.; Sun, T.; Yao, L.; Zhang, Q.; Xu, Y. Predictive and Prognostic Roles of Pathological Indicators for Patients with Breast Cancer on Neoadjuvant Chemotherapy. J. Breast Cancer 2018, 22, 497–521. [Google Scholar] [CrossRef]
- De Barros, A.C.S.D.; Paulo, M.H.B.P.D.S.; De Andrade, D.A. Extended Sentinel Node Biopsy in Breast Cancer Patients who Achieve Complete Nodal Response with Neoadjuvant Chemotherapy. Eur. J. Breast Health 2020, 16, 99–105. [Google Scholar] [CrossRef]
- Ogston, K.N.; Miller, I.D.; Payne, S.; Hutcheon, A.W.; Sarkar, T.K.; Smith, I.; Schofield, A.; Heys, S.D. A new histological grading system to assess response of breast cancers to primary chemotherapy: Prognostic significance and survival. Breast 2003, 12, 320–327. [Google Scholar] [CrossRef]
- Byrd, D.R.; Carducci, M.A.; Compton, C.C.; Fritz, A.G.; Greene, F.L. (Eds.) AJCC Cancer Staging Manual, 8th ed.; Springer: New York, NY, USA, 2017. [Google Scholar]
- Tsujimoto, M.; Nakabayashi, K.; Yoshidome, K.; Kaneko, T.; Iwase, T.; Akiyama, F.; Kato, Y.; Tsuda, H.; Ueda, S.; Sato, K.; et al. One-step Nucleic Acid Amplification for Intraoperative Detection of Lymph Node Metastasis in Breast Cancer Patients. Clin. Cancer Res. 2007, 13, 4807–4816. [Google Scholar] [CrossRef]
- Mansel, R.E.; Fallowfield, L.; Kissin, M.; Goyal, A.; Newcombe, R.G.; Dixon, J.M.; Yiangou, C.; Horgan, K.; Bundred, N.; Monypenny, I.; et al. Randomized Multicenter Trial of Sentinel Node Biopsy Versus Standard Axillary Treatment in Operable Breast Cancer: The ALMANAC Trial. J. Natl. Cancer Inst. 2006, 98, 599–609. [Google Scholar] [CrossRef] [PubMed]
- Purushotham, A.D.; Upponi, S.; Klevesath, M.B.; Bobrow, L.; Millar, K.; Myles, J.P.; Duffy, S.W. Morbidity After Sentinel Lymph Node Biopsy in Primary Breast Cancer: Results from a Randomized Controlled Trial. J. Clin. Oncol. 2005, 23, 4312–4321. [Google Scholar] [CrossRef] [PubMed]
- Bleiweiss, I.J. Sentinel lymph nodes in breast cancer after 10 years: Rethinking basic principles. Lancet Oncol. 2006, 7, 686–692. [Google Scholar] [CrossRef]
- Benson, J.R.; Jatoi, I. Sentinel lymph node biopsy and neoadjuvant chemotherapy in breast cancer patients. Future Oncol. 2014, 10, 577–586. [Google Scholar] [CrossRef] [PubMed]
- Kuehn, T.; Bauerfeind, I.; Fehm, T.; Fleige, B.; Hausschild, M.; Helms, G.; Lebeau, A.; Liedtke, C.; Von Minckwitz, G.; Nekljudova, V.; et al. Sentinel-lymph-node biopsy in patients with breast cancer before and after neoadjuvant chemotherapy (SENTINA): A prospective, multicentre cohort study. Lancet Oncol. 2013, 14, 609–618. [Google Scholar] [CrossRef]
- Fisher, B.; Brown, A.; Mamounas, E.; Wieand, S.; Robidoux, A.; Margolese, R.G.; Cruz, A.B.; Fisher, E.R.; Wickerham, D.L.; Wolmark, N.; et al. Effect of preoperative chemotherapy on local-regional disease in women with operable breast cancer: Findings from National Surgical Adjuvant Breast and Bowel Project B-18. J. Clin. Oncol. 1997, 15, 2483–2493. [Google Scholar] [CrossRef]
- Gianni, L.; Baselga, J.; Eiermann, W.; Porta, V.G.; Semiglazov, V.F.; Lluch, A.; Zambetti, M.; Sabadell, D.; Raab, G.; Cussac, A.L.; et al. Phase III Trial Evaluating the Addition of Paclitaxel to Doxorubicin Followed by Cyclophosphamide, Methotrexate, and Fluorouracil, As Adjuvant or Primary Systemic Therapy: European Cooperative Trial in Operable Breast Cancer. J. Clin. Oncol. 2009, 27, 2474–2481. [Google Scholar] [CrossRef]
- Mamounas, E.P.; Brown, A.; Anderson, S.; Smith, R.; Julian, T.; Miller, B.; Bear, H.D.; Caldwell, C.B.; Walker, A.P.; Mikkelson, W.M.; et al. Sentinel Node Biopsy After Neoadjuvant Chemotherapy in Breast Cancer: Results From National Surgical Adjuvant Breast and Bowel Project Protocol B-27. J. Clin. Oncol. 2005, 23, 2694–2702. [Google Scholar] [CrossRef]
- Nason, K.S.; Anderson, B.O.; Byrd, D.R.; Dunnwald, L.K.; Eary, J.F.; Mankoff, D.A.; Livingston, R.; Schmidt, R.A.; Jewell, K.D.; Yeung, R.S.; et al. Increased false negative sentinel node biopsy rates after preoperative chemotherapy for invasive breast carcinoma. Cancer 2000, 89, 2187–2194. [Google Scholar] [CrossRef]
- Tafra, L.; Verbanac, K.M.; Lannin, D.R. Preoperative chemotherapy and sentinel lymphadenectomy for breast cancer. Am. J. Surg. 2001, 182, 312–315. [Google Scholar] [CrossRef]
- Parada, D.; Peña, K.B.; Riu, F.F.; Aguilar, A.E.; Cohan, S. Intraoperative molecular analysis of sentinel lymph nodes following neoadjuvant chemotherapy in patients with clinical node negative breast cancer: An institutional study. Mol. Clin. Oncol. 2016, 5, 507–510. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Geng, C.; Chen, X.; Pan, X.; Li, J. The Feasibility and Accuracy of Sentinel Lymph Node Biopsy in Initially Clinically Node-Negative Breast Cancer after Neoadjuvant Chemotherapy: A Systematic Review and Meta-Analysis. PLoS ONE 2016, 11, e0162605. [Google Scholar] [CrossRef]
- Buchholz, T.A.; Lehman, C.D.; Harris, J.R.; Pockaj, B.A.; Khouri, N.; Hylton, N.F.; Miller, M.J.; Whelan, T.; Pierce, L.J.; Esserman, L.J.; et al. Statement of the Science Concerning Locoregional Treatments After Preoperative Chemotherapy for Breast Cancer: A National Cancer Institute Conference. J. Clin. Oncol. 2008, 26, 791–797. [Google Scholar] [CrossRef] [PubMed]
- Ohi, Y.; Umekita, Y.; Rai, Y.; Yotsumoto, D.; Matsukata, A.; Baba, S.; Tamada, S.; Matsuyama, Y.; Ando, M.; Sasaki, M.; et al. Whole sentinel lymph node analysis by a molecular assay predicts axillary node status in breast cancer. Br. J. Cancer 2012, 107, 1239–1243. [Google Scholar] [CrossRef] [PubMed]
- Peg‡, V.; Espinosa-Bravo, M.; Vieites, B.; Vilardell, F.; Antúnez, J.R.; De Salas, M.S.; Delgado-Sánchez, J.J.; Pinto, W.; Gozalbo, F.; Petit, A.; et al. Intraoperative molecular analysis of total tumor load in sentinel lymph node: A new predictor of axillary status in early breast cancer patients. Breast Cancer Res. Treat. 2013, 139, 87–93. [Google Scholar] [CrossRef] [PubMed]
- Rubio, I.T.; Espinosa-Bravo, M.; Rodrigo, M.; Diaz, M.A.V.; Hardisson, D.; Sagasta, A.; Dueñas, B.; Peg, V. Nomogram including the total tumoral load in the sentinel nodes assessed by one-step nucleic acid amplification as a new factor for predicting nonsentinel lymph node metastasis in breast cancer patients. Breast Cancer Res. Treat. 2014, 147, 371–380. [Google Scholar] [CrossRef]
- Piñero-Madrona, A.; Ripoll-Orts, F.; Sánchez-Méndez, J.I.; Chaves-Benito, A.; La Bárcena, M.R.G.-D.; Calatrava-Fons, A.; Menjón-Beltrán, S.; Peg-Cámara, V. External validation of a prognostic model based on total tumor load of sentinel lymph node for early breast cancer patients. Breast Cancer Res. Treat. 2020, 181, 339–345. [Google Scholar] [CrossRef]
- Cuffolo, G.; Msc, H.K.G.; Smith, B. One-step nucleic acid amplification CK19 copy number for sentinel node biopsy in breast cancer: Identification of new cutoffs to predict nonsentinel axillary node involvement. Breast J. 2020, 26, 2002–2005. [Google Scholar] [CrossRef]
- Sansano, I.; Vieites, B.; De Salas, M.S.; García, C.; Amendoeira, I.; Bernet, L.; Pérez-García, J.M.; Espinosa-Bravo, M.; Rubio, I.T.; Cajal, S.R.Y.; et al. Axillary staging based on molecular analysis: Results of the B-CLOSER-II study. Pathol.-Res. Prat. 2020, 216, 153197. [Google Scholar] [CrossRef]
- Fougo, J.L.; Amendoeira, I.; Brito, M.J.; Correia, A.P.; Gonçalves, A.; Honavar, M.; Machado, A.; Magalhães, A.; Marta, S.; Nogueira, M.; et al. Sentinel node total tumour load as a predictive factor for non-sentinel node status in early breast cancer patients –The porttle study. Surg. Oncol. 2020, 32, 108–114. [Google Scholar] [CrossRef]
- Qiu, P.-F.; Zhao, R.-R.; Wang, W.; Sun, X.; Chen, P.; Liu, Y.-B.; Liu, Z.-G.; Wang, Y.-S. Internal Mammary Sentinel Lymph Node Biopsy in Clinically Axillary Lymph Node-Positive Breast Cancer: Diagnosis and Implications for Patient Management. Ann. Surg. Oncol. 2019, 27, 375–383. [Google Scholar] [CrossRef] [PubMed]
- Manca, G.; Volterrani, D.; Mazzarri, S.; Duce, V.; Svirydenka, A.; Giuliano, A.; Mariani, G. Sentinel lymph node mapping in breast cancer: A critical reappraisal of the internal mammary chain issue. Q. J. Nucl. Med. Mol. Imaging 2014, 58, 114–126. [Google Scholar] [PubMed]
- Paredes, P.; Vidal-Sicart, S.; Zanón, G.; Pahisa, J.; Fernandez, P.L.; Velasco, M.; Santamaría, G.; Ortín, J.; Duch, J.; Pons, F. Clinical relevance of sentinel lymph nodes in the internal mammary chain in breast cancer patients. Eur. J. Nucl. Med. Mol. Imaging 2005, 32, 1283–1287. [Google Scholar] [CrossRef]
- Colomer, R.; Saura, C.; Sánchez-Rovira, P.; Pascual, T.; Rubio, I.T.; Burgués, O.; Marcos, L.; Rodríguez, C.A.; Martín, M.; Lluch, A. Neoadjuvant Management of Early Breast Cancer: A Clinical and Investigational Position Statement. Oncology 2019, 24, 603–611. [Google Scholar] [CrossRef]
- Classe, J.-M.; Loaec, C.; Gimbergues, P.; Alran, S.; De Lara, C.T.; Dupre, P.F.; Rouzier, R.; Faure, C.; Paillocher, N.; Chauvet, M.P.; et al. Sentinel lymph node biopsy without axillary lymphadenectomy after neoadjuvant chemotherapy is accurate and safe for selected patients: The GANEA 2 study. Breast Cancer Res. Treat. 2019, 173, 343–352. [Google Scholar] [CrossRef]
- Mathelin, C.; Lodi, M. Narrative review of sentinel lymph node biopsy in breast cancer: A technique in constant evolution with still numerous unresolved questions. Chin. Clin. Oncol. 2020, 9, 5. [Google Scholar] [CrossRef]
- Qiu, S.-Q.; Zhang, G.; Jansen, L.; De Vries, J.; Schröder, C.P.; De Vries, E.G.; Van Dam, G.M. Evolution in sentinel lymph node biopsy in breast cancer. Crit. Rev. Oncol. 2018, 123, 83–94. [Google Scholar] [CrossRef]


{kind=link}
| Characteristics | No. |
|---|---|
| Age (years) ** | 57 (29.5–84.5) |
| Histological type | |
| No special type | 104 (93.7%) |
| Special type | 7 (6.3%) |
| Nuclear Grade | |
| 2 | 44 (39.6%) |
| 3 | 67 (60.4%) |
| ICC-4 type | |
| Luminal A | 5 (4.5%) |
| Luminal B | 70 (63.1%) |
| HER2 positive | 16 (14.4%) |
| Triple negative | 20 (18%) |
| Pathological T classification (pT) | |
| pT2 | 91 (81.98%) |
| pT3 | 20 (18.02%) |
| Estrogen receptors ** | 70 (0–97) |
| Progesterone receptors ** | 6 (0–80) |
| HER-2 expression | |
| Negative | 65 (58.6%) |
| Positive | 46 (41.4%) |
| Ki-67 ** | 43 (26.5–64.5) |
| Pathological response to chemotherapy | |
| No response | 6 (5.4%) |
| Partial | 67 (60.4%) |
| Complete | 38 (34.2%) |
| Luminal A | Luminal B | HER2 Expression | Triple Negative | |
|---|---|---|---|---|
| n | 5 | 70 | 16 | 20 |
| SLN | ||||
| Positive | 2 | 41 | 7 | 5 |
| Negative | 3 | 29 | 9 | 15 |
| SLN positive | ||||
| ITC | 0 | 7 | 1 | 1 |
| Micrometastases | 2 | 19 | 6 | 3 |
| Macrometastases | 0 | 15 | 0 | 1 |
| ALD | ||||
| Positive | 0 | 8 | 0 | 1 |
| Negative | 2 | 33 | 7 | 4 |
| Pathological response | ||||
| No response | 0 | 3 | 0 | 3 |
| Partial response | 4 | 52 | 3 | 8 |
| Complete response | 1 | 15 | 13 | 9 |
| ALD Negative | ALD Positive | ||||||
|---|---|---|---|---|---|---|---|
| Mean | CI lower | CI upper | Mean | CI lower | CI upper | p value | |
| Diagnostic age | 48.66 | 45.39 | 55.35 | 44.15 | 40.57 | 51.40 | 0.439 |
| Miller–Payne | 4 | 3 | 5 | 3 | 2 | 3 | 0.080 |
| Tumor diameter previous treatment (mm) | 33 | 22.25 | 39.75 | 43.5 | 34.5 | 59.5 | 0.181 |
| Tumor diameter after treatment (mm) | 5 | 0 | 0.15 | 30 | 12 | 34 | 0.026 |
| Total Tumor Load | 680,000 | 352,500 | 3,875,000 | 27,410,000 | 11,530,000 | 3,000,000 | 0.043 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Peña, K.B.; Kepa, A.; Cochs, A.; Riu, F.; Parada, D.; Gumà, J. Total Tumor Load of mRNA Cytokeratin 19 in the Sentinel Lymph Node as a Predictive Value of Axillary Lymphadenectomy in Patients with Neoadjuvant Breast Cancer. Genes 2021, 12, 77. https://doi.org/10.3390/genes12010077
Peña KB, Kepa A, Cochs A, Riu F, Parada D, Gumà J. Total Tumor Load of mRNA Cytokeratin 19 in the Sentinel Lymph Node as a Predictive Value of Axillary Lymphadenectomy in Patients with Neoadjuvant Breast Cancer. Genes. 2021; 12(1):77. https://doi.org/10.3390/genes12010077
Chicago/Turabian StylePeña, Karla B., Amillano Kepa, Alba Cochs, Francesc Riu, David Parada, and Josep Gumà. 2021. "Total Tumor Load of mRNA Cytokeratin 19 in the Sentinel Lymph Node as a Predictive Value of Axillary Lymphadenectomy in Patients with Neoadjuvant Breast Cancer" Genes 12, no. 1: 77. https://doi.org/10.3390/genes12010077
APA StylePeña, K. B., Kepa, A., Cochs, A., Riu, F., Parada, D., & Gumà, J. (2021). Total Tumor Load of mRNA Cytokeratin 19 in the Sentinel Lymph Node as a Predictive Value of Axillary Lymphadenectomy in Patients with Neoadjuvant Breast Cancer. Genes, 12(1), 77. https://doi.org/10.3390/genes12010077