Peripheral Blood Eosinophilia Is Associated with Poor Outcome Post-Lung Transplantation

 , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Inclusion
2.2. Definitions
2.3. Statistical Analyses
3. Results
3.1. Patient Characteristics
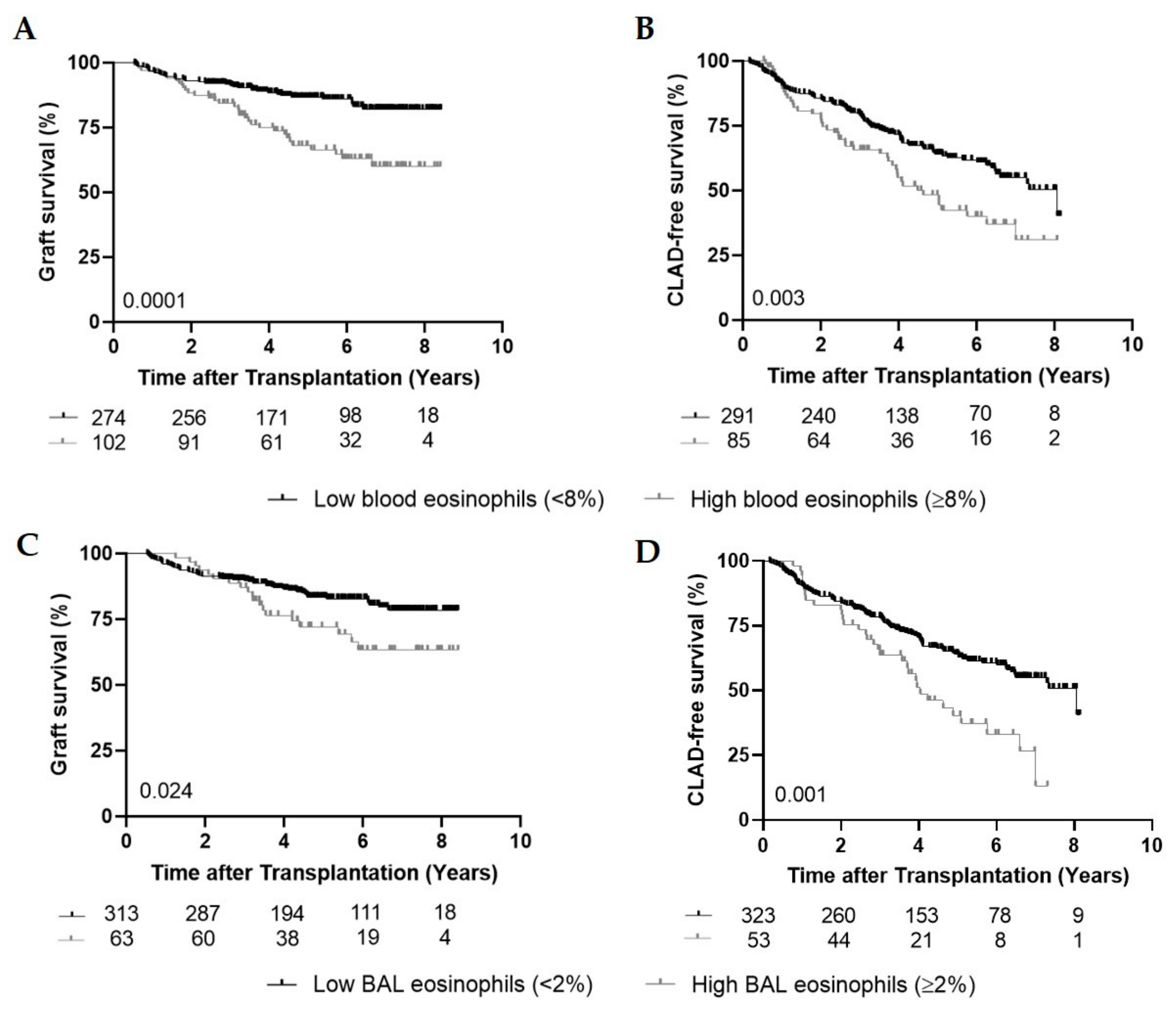
3.2. High Peripheral Blood Eosinophils and Graft Survival
3.3. High Peripheral Blood Eosinophils and CLAD-Free Survival
3.4. Role of Infection and Meropenem at Peak Peripheral Blood Eosinophilia
3.5. High BAL Eosinophils, Graft and CLAD-Free Survival
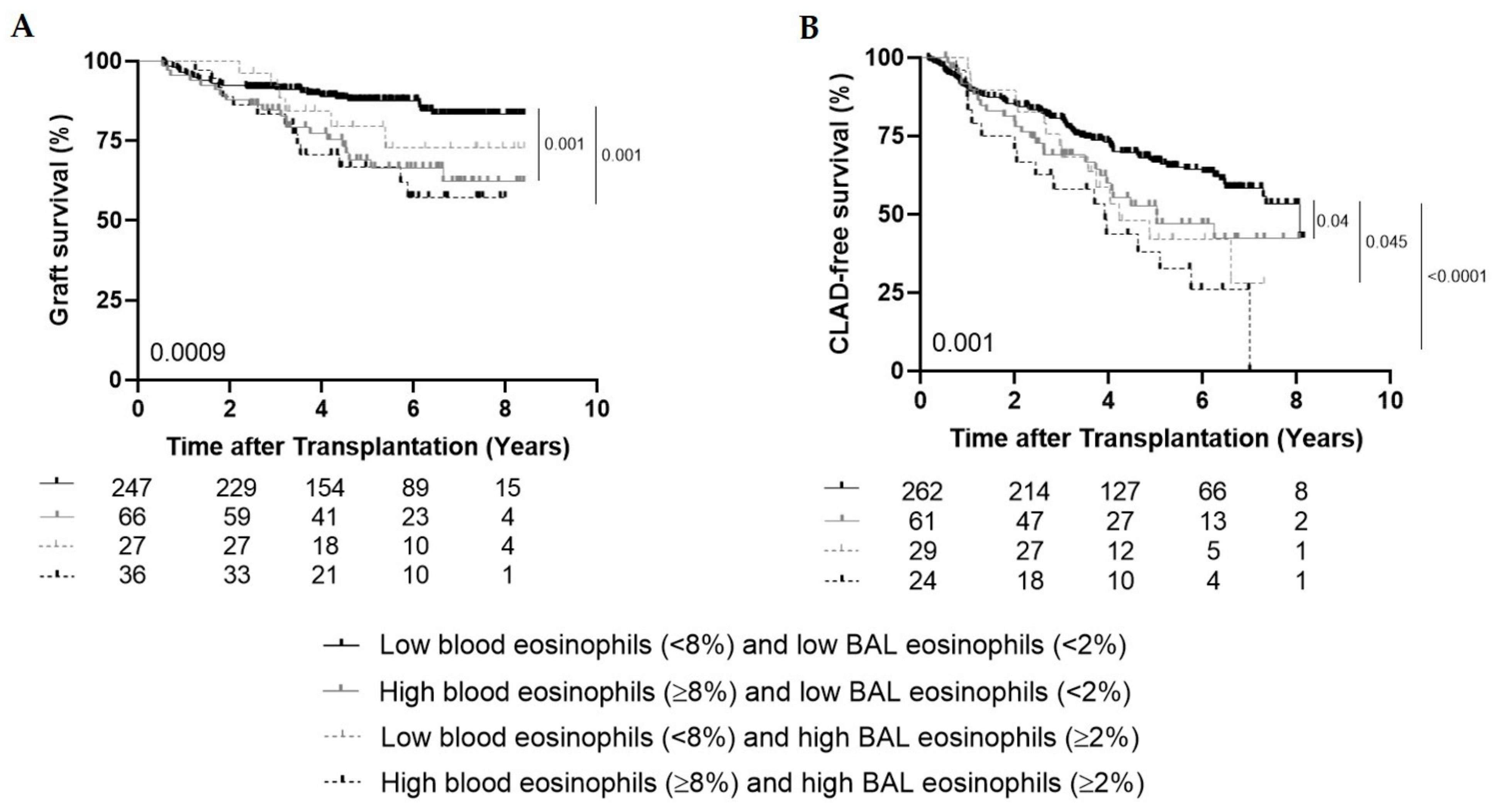
3.6. High Peripheral Blood Eosinophils and High BAL Eosinophils
3.7. Histological Findings in Explant Lungs of Retransplantations
3.8. Multivariate Analyses
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Low Blood Eosinophils | High Blood Eosinophils | |
|---|---|---|
| Infection, n (%) | 69/274 (25%) | 49/102 (48%) |
| Pulmonary | 45 (65.2%) | 34 (69.4%) |
| Bacterial | 20 (44.4%) | 9 (26.5%) |
| Viral | 12 (26.7%) | 6 (17.6%) |
| Fungal | 6 (13.3%) | 7 (20.6%) |
| Multiple pathogens | 7 (15.6%) | 12 (35.3%) |
| Extrapulmonary | 7 (10.2%) | 4 (8.2%) |
| Unknown | 17 (24.6%) | 11 (22.4%) |
References
- Bos, S.; Vos, R.; Van Raemdonck, D.E.; Verleden, G.M. Survival in adult lung transplantation. Curr. Opin. Organ Transplant. 2020, 25, 268–273. [Google Scholar] [CrossRef] [PubMed]
- Kulkarni, H.S.; Cherikh, W.S.; Chambers, D.C.; Garcia, V.C.; Hachem, R.R.; Kreisel, D.E.; Puri, V.; Kozower, B.D.; Byers, D.E.; Witt, C.A.; et al. Bronchiolitis obliterans syndrome–free survival after lung transplantation: An International Society for Heart and Lung Transplantation Thoracic Transplant Registry analysis. J. Heart Lung Transplant. 2019, 38, 5–16. [Google Scholar] [CrossRef] [PubMed]
- Verleden, S.E.; Ruttens, D.; Vandermeulen, E.; Vaneylen, A.; Van Raemdonck, D.; Dupont, L.J.; Vanaudenaerde, B.M.; Verleden, G.M.; Vos, R. Bronchiolitis Obliterans Syndrome and Restrictive Allograft Syndrome: Do Specific Risk Factors Differ? J. Heart Lung Transplant. 2013, 32, S60. [Google Scholar] [CrossRef]
- Verleden, S.E.; Vanaudenaerde, B.M.; Emonds, M.-P.; Van Raemdonck, D.E.; Neyrinck, A.P.; Verleden, G.M.; Vos, R. Donor-specific and -nonspecific HLA antibodies and outcome post lung transplantation. Eur. Respir. J. 2017, 50, 1701248. [Google Scholar] [CrossRef] [PubMed]
- D’Ovidio, F.; Mura, M.; Tsang, M.E.; Waddell, T.K.; Hutcheon, M.A.; Singer, L.G.; Hadjiliadis, D.; Chaparro, C.; Gutiérrez, C.; Pierre, A.; et al. Bile acid aspiration and the development of bronchiolitis obliterans after lung transplantation. J. Thorac. Cardiovasc. Surg. 2005, 129, 1144–1152. [Google Scholar] [CrossRef]
- Ruttens, D.; Verleden, S.E.; Bijnens, E.M.; Winckelmans, E.; Gottlieb, J.; Warnecke, G.; Meloni, F.; Morosini, M.; Van Der Bij, W.; Verschuuren, E.A.; et al. An association of particulate air pollution and traffic exposure with mortality after lung transplantation in Europe. Eur. Respir. J. 2016, 49, 1600484. [Google Scholar] [CrossRef]
- Verleden, S.E.; Ruttens, D.; Vandermeulen, E.; Van Raemdonck, D.E.; Vanaudenaerde, B.M.; Verleden, G.M.; Vos, R. Elevated Bronchoalveolar Lavage Eosinophilia Correlates with Poor Outcome After Lung Transplantation. Transplant. 2014, 97, 83–89. [Google Scholar] [CrossRef]
- Possa, S.S.; Leick, E.A.; Prado, C.M.; Martins, M.A.; Tibério, I.D.F.L.C. Eosinophilic Inflammation in Allergic Asthma. Front. Pharmacol. 2013, 4, 46. [Google Scholar] [CrossRef]
- Trull, A.; Steel, L.; Cornelissen, J.; Smith, T.; Sharples, L.; Cary, N.; Stewart, S.; Large, S.; Wallwork, J. Association between blood eosinophil counts and acute cardiac and pulmonary allograft rejection. J. Heart Lung Transplant. 1998, 17, 517–524. [Google Scholar]
- Vos, R.; Vanaudenaerde, B.M.; Verleden, S.E.; De Vleeschauwer, S.I.; Willems-Widyastuti, A.; Van Raemdonck, D.E.; Dupont, L.J.; Nawrot, T.S.; Verbeken, E.K.; Verleden, G.M. Bronchoalveolar lavage neutrophilia in acute lung allograft rejection and lymphocytic bronchiolitis. J. Heart Lung Transplant. 2010, 29, 1259–1269. [Google Scholar] [CrossRef]
- LeMessurier, K.S.; Samarasinghe, A.E. Eosinophils: Nemeses of Pulmonary Pathogens? Curr. Allergy Asthma Rep. 2019, 19, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Verleden, G.M.; Glanville, A.R.; Lease, E.D.; Fisher, A.J.; Calabrese, F.; Corris, P.A.; Ensor, C.R.; Gottlieb, J.; Hachem, R.R.; Lama, V.; et al. Chronic lung allograft dysfunction: Definition, diagnostic criteria, and approaches to treatment―A consensus report from the Pulmonary Council of the ISHLT. J. Heart Lung Transplant. 2019, 38, 493–503. [Google Scholar] [CrossRef] [PubMed]
- Glanville, A.R.; Verleden, G.M.; Todd, J.L.; Benden, C.; Calabrese, F.; Gottlieb, J.; Hachem, R.R.; Levine, D.; Meloni, F.; Palmer, S.M.; et al. Chronic lung allograft dysfunction: Definition and update of restrictive allograft syndrome―A consensus report from the Pulmonary Council of the ISHLT. J. Heart Lung Transplant. 2019, 38, 483–492. [Google Scholar] [CrossRef] [PubMed]
- Stewart, S.; Fishbein, M.C.; Snell, G.I.; Berry, G.J.; Boehler, A.; Burke, M.M.; Glanville, A.; Gould, F.K.; Magro, C.; Marboe, C.C.; et al. Revision of the 1996 Working Formulation for the Standardization of Nomenclature in the Diagnosis of Lung Rejection. J. Heart Lung Transplant. 2007, 26, 1229–1242. [Google Scholar] [CrossRef]
- Hatem, N.A.; Campbell, S.; Rubio, E.; Loschner, A.L. Meropenem: A possible new culprit in eosinophilic lung diseases. Lung India Off. Organ Indian Chest Soc. 2017, 34, 461–464. [Google Scholar]
- Peterson, M.W.; Monick, M.; Hunninghake, G.W. Prognostic Role of Eosinophils in Pulmonary Fibrosis. Chest 1987, 92, 51–56. [Google Scholar] [CrossRef]
- Vedel-Krogh, S.; Nielsen, S.F.; Lange, P.; Vestbo, J.; Nordestgaard, B.G. Blood Eosinophils and Exacerbations in Chronic Obstructive Pulmonary Disease. The Copenhagen General Population Study. Am. J. Respir. Crit. Care Med. 2016, 193, 965–974. [Google Scholar] [CrossRef]
- Ravin, K.A.; Loy, M. The Eosinophil in Infection. Clin. Rev. Allergy Immunol. 2016, 50, 214–227. [Google Scholar] [CrossRef]
- Vandermeulen, E.; Lammertyn, E.; Verleden, S.E.; Ruttens, D.; Bellon, H.; Ricciardi, M.; Somers, J.; Bracke, K.R.; Eynde, K.V.D.; Tousseyn, T.; et al. Immunological diversity in phenotypes of chronic lung allograft dysfunction: A comprehensive immunohistochemical analysis. Transpl. Int. 2016, 30, 134–143. [Google Scholar] [CrossRef]
- Darley, D.R.; Ma, J.; Huszti, E.; Fiset, P.; Levy, L.; Hwang, D.M.; Pal, P.; Klement, W.; Zamel, R.; Keshavjee, S.; et al. Eosinophils in transbronchial biopsies: A predictor of chronic lung allograft dysfunction and reduced survival after lung transplantation—A retrospective single-center cohort study. Transpl. Int. 2020. Online ahead of print. [Google Scholar] [CrossRef]
- Vanstapel, A.; Verleden, S.E.; Weynand, B.; Verbeken, E.; De Sadeleer, L.J.; Vanaudenaerde, B.M.; Verleden, G.M.; Vos, R. Late-onset “acute fibrinous and organising pneumonia” impairs long-term lung allograft function and survival. Eur. Respir. J. 2020, 56, 1902292. [Google Scholar] [CrossRef] [PubMed]
- Goldman, M.; Le Moine, A.; Braun, M.; Flamand, V.; Abramowicz, D. A role for eosinophils in transplant rejection. Trends Immunol. 2001, 22, 247–251. [Google Scholar] [CrossRef]
- Sacreas, A.; Von Der Thüsen, J.H.; Bosch, T.P.V.D.; Weynand, B.; Verbeken, E.K.; Debbaut, C.; Van Raemdonck, D.E.; Vos, R.; Verleden, S.E. The pleural mesothelium and transforming growth factor-β1 pathways in restrictive allograft syndrome: A pre-clinical investigation. J. Heart Lung Transplant. 2019, 38, 570–579. [Google Scholar] [CrossRef]
- Lee, J.J.; Jacobsen, E.A.; McGarry, M.P.; Schleimer, R.P.; Lee, N.A. Eosinophils in health and disease: The LIAR hypothesis. Clin. Exp. Allergy 2010, 40, 563–575. [Google Scholar] [CrossRef] [PubMed]
- Vos, R.; Eynde, R.V.; Ruttens, D.; Verleden, S.E.; Vanaudenaerde, B.M.; Dupont, L.J.; Yserbyt, J.; Verbeken, E.K.; Neyrinck, A.P.; Van Raemdonck, D.E.; et al. Montelukast in chronic lung allograft dysfunction after lung transplantation. J. Heart Lung Transplant. 2019, 38, 516–527. [Google Scholar] [CrossRef]
- Speck, N.E.; Schuurmans, M.M.; Murer, C.; Benden, C.; Huber, L.C. Diagnostic value of plasma and bronchoalveolar lavage samples in acute lung allograft rejection: Differential cytology. Respir. Res. 2016, 17, 1–12. [Google Scholar] [CrossRef] [PubMed]


| Low Blood Eosinophils (<8%) | High Blood Eosinophils (≥8%) | p-Value | |
|---|---|---|---|
| Number of patients, n (%) | 274 (72.9%) | 102 (27.1%) | |
| Gender female, n (%) | 122 (44.5%) | 64 (62.7%) | 0.002 |
| Age, years, median (IQR) | 57 (47–61) | 55 (34.5–61) | 0.18 |
| Native disease, n (%) | 0.014 | ||
| Emphysema. α-1ATD | 153 (55.8%) | 50 (49%) | |
| CF/Bronchiectasis | 36 (13.2%) | 24 (23.5%) | |
| Pulmonary fibrosis | 56 (20.4%) | 15 (14.7%) | |
| PPH | 12 (4.4%) | 1 (1%) | |
| Other | 17 (6.2%) | 12 (11.8%) | |
| Type Tx, n (%) | 0.30 | ||
| SSL | 267 (97.4%) | 96 (94.1%) | |
| SSL + liver | 3 (1.1%) | 3 (2.9%) | |
| SSL + kidney | 1 (0.4%) | 0 | |
| HL | 3 (1.1%) | 3 (2.9%) | |
| Outcome, n (%) | 0.0002 | ||
| Alive | 236 (86.1%) | 69 (67.6%) | |
| Death | 33 (12.1%) | 28 (27.5%) | |
| Retransplantation | 5 (1.8%) | 5 (4.9%) | |
| Cause of death or retransplantation, n (%) | 0.048 | ||
| CLAD | 12 (31.6%) | 21 (63.6%) | |
| BOS | 7 (58%) | 7 (33.4%) | |
| RAS | 5 (42%) | 14 (66.6%) | |
| Infection | 11 (28.9%) | 3 (9.1%) | |
| Multifactorial | 6 (15.8%) | 4 (12.1%) | |
| Other (e.g., cancer) | 9 (23.7%) | 5 (15.2%) | |
| Number of biopsies per patient, median (IQR) | 6 (6–7) | 7 (6–8) | 0.0047 |
| Ever AR, n (%) | 82 (29.9%) | 38 (37.3%) | 0.21 |
| Ever severe AR (≥A2), n (%) | 37 (13.5%) | 21 (20.6%) | 0.11 |
| Mean AR score (St dev) | 0.077 (±0.14) | 0.11 (±0.21) | 0.15 |
| Ever LB, n (%) | 97 (35.4%) | 51 (50%) | 0.012 |
| Ever severe LB (≥B2), n (%) | 40 (14.6%) | 25 (24.5%) | 0.031 |
| Mean LB score (St dev) | 0.12 (±0.22) | 0.17 (±0.24) | 0.008 |
| Presence of DSAs, n (%) | 18 (6.6%) | 15 (14.7%) | 0.022 |
| Infection at peak eosinophilia, n (%) | 69 (25%) | 49 (48%) | <0.0001 |
| Meropenem at peak eosinophilia, n (%) | 19 (6.9%) | 33 (32.4%) | <0.0001 |
| WBC count at peak eosinophilia, median (IQR) | 5.58 (4.31–6.89) | 6.28 (3.56–7.84) | 0.65 |
| Abnormal WBC count at peak eosinophilia (<4 × 109/L), n (%) | 54 (20%) | 29 (28%) | 0.09 |
| Time to CLAD, median (IQR) | 2.6 years (1.0–4.0) | 2.1 years (1.0–3.8) | 0.51 |
| Time of follow-up, median (IQR) | 4.7 years (3.2–6.6) | 4.5 years (3.0–6.5) | 0.29 |
| Total | CLAD | BOS | RAS | |
|---|---|---|---|---|
| Low blood eosinophils | 274 (72.9%) | 83 (30.3%) | 75 (27.4%) | 8 (3%) |
| High blood eosinophils | 102 (27.1%) | 62 (60.8%) | 38 (37.3%) | 24 (23.5%) |
| Low BAL eosinophils | 313 (83.2%) | 103 (32.9%) | 89 (28.4%) | 14 (4.5%) |
| High BAL eosinophils | 63 (16.8%) | 42 (66.7%) | 24 (38.1%) | 18 (28.6%) |
| Univariate Analyses | Multivariate Analyses | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Death | CLAD | Death | CLAD | |||||||||
| HR | (CI) | p-Value | HR | (CI) | p-Value | HR | (CI) | p-Value | HR | (CI) | p-Value | |
| Age | 1.02 | (0.99–1.04) | 0.1 | 1.01 | (1.00–1.03) | 0.03 | 1.02 | (0.99–1.05) | 0.31 | 0.99 | (0.97–1.01) | 0.44 |
| Gender (female) | 0.92 | (0.58–1.46) | 0.72 | 1.16 | (0.83–1.60) | 0.39 | 0.75 | (0.46–1.23) | 0.26 | 1.02 | (0.72–1.44) | 0.92 |
| Native disease: | ||||||||||||
| Emphysema | 1.26 | (0.78–2.02) | 0.34 | 1.49 | (1.06–2.08) | 0.02 | REF | |||||
| CF/Bronchiectasis | 0.66 | (0.32–1.38) | 0.27 | 0.46 | (0.26–0.81) | 0.008 | 0.82 | (0.25–2.69) | 0.74 | 0.26 | (0.11–0.64) | 0.003 |
| Pulmonary fibrosis | 1.19 | (0.67–2.10) | 0.56 | 1.14 | (0.75–1.72) | 0.55 | 0.84 | (0.44–1.59) | 0.59 | 0.7 | (0.44–1.01) | 0.12 |
| PPH | 0.67 | (0.16–2.74) | 0.58 | 0.40 | (0.13–1.26) | 0.12 | 1.13 | (0.23–5.53) | 0.88 | 0.35 | (0.09–1.21) | 0.09 |
| Other | 0.71 | (0.26–1.95) | 0.51 | 1.00 | (0.55–1.81) | 0.99 | 0.71 | (0.21–2.38) | 0.58 | 0.41 | (0.19–0.91) | 0.03 |
| Any AR | 1.44 | (0.90–2.31) | 0.13 | 1.51 | (1.08–2.10) | 0.016 | 1.48 | (0.91–2.40) | 0.11 | 1.48 | (1.06–2.09) | 0.024 |
| Any LB | 0.69 | (0.43–1.13) | 0.14 | 1.00 | (0.72–1.39) | 0.99 | 0.74 | (0.45–1.24) | 0.26 | 0.99 | (0.71–1.40) | 0.98 |
| Presence of DSA | 2.36 | (1.29–4.30) | 0.005 | 2.12 | (1.33–3.37) | 0.002 | 1.63 | (0.85–3.13) | 0.15 | 1.82 | (1.13–2.91) | 0.013 |
| Infection at peak blood eosinophils | 2.46 | (1.54–3.92) | <0.0001 | 1.66 | (1.18–2.36) | 0.004 | 1.66 | (0.92–2.97) | 0.09 | 1.81 | (1.21–2.72) | 0.004 |
| Meropenem at peak blood eosinophils | 3.54 | (2.15–5.82) | <0.0001 | 1.18 | (0.72–1.94) | 0.5 | 1.95 | (1.00–3.8) | 0.05 | 0.57 | (0.32–1.04) | 0.065 |
| High BAL eosinophils (≥2%) | 1.82 | (1.08–3.08) | 0.026 | 1.90 | (1.28–2.82) | 0.001 | 1.36 | (0.77–2.4) | 0.28 | 1.89 | (1.24–2.87) | 0.003 |
| High blood eosinophils (≥8%) | 2.44 | (1.53–3.89) | <0.0001 | 1.70 | (1.19–2.41) | 0.003 | 1.81 | (1.04–3.16) | 0.036 | 1.67 | (1.11–2.5) | 0.013 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kaes, J.; Van der Borght, E.; Vanstapel, A.; Van Herck, A.; Sacreas, A.; Heigl, T.; Vanaudenaerde, B.M.; Godinas, L.; Van Raemdonck, D.E.; Ceulemans, L.J.; et al. Peripheral Blood Eosinophilia Is Associated with Poor Outcome Post-Lung Transplantation. Cells 2020, 9, 2516. https://doi.org/10.3390/cells9112516
Kaes J, Van der Borght E, Vanstapel A, Van Herck A, Sacreas A, Heigl T, Vanaudenaerde BM, Godinas L, Van Raemdonck DE, Ceulemans LJ, et al. Peripheral Blood Eosinophilia Is Associated with Poor Outcome Post-Lung Transplantation. Cells. 2020; 9(11):2516. https://doi.org/10.3390/cells9112516
Chicago/Turabian StyleKaes, Janne, Elise Van der Borght, Arno Vanstapel, Anke Van Herck, Annelore Sacreas, Tobias Heigl, Bart M. Vanaudenaerde, Laurent Godinas, Dirk E. Van Raemdonck, Laurens J. Ceulemans, and et al. 2020. "Peripheral Blood Eosinophilia Is Associated with Poor Outcome Post-Lung Transplantation" Cells 9, no. 11: 2516. https://doi.org/10.3390/cells9112516
APA StyleKaes, J., Van der Borght, E., Vanstapel, A., Van Herck, A., Sacreas, A., Heigl, T., Vanaudenaerde, B. M., Godinas, L., Van Raemdonck, D. E., Ceulemans, L. J., Neyrinck, A. P., Vos, R., Verleden, G. M., Verleden, S. E., & Group the Leuven Lung Transplant. (2020). Peripheral Blood Eosinophilia Is Associated with Poor Outcome Post-Lung Transplantation. Cells, 9(11), 2516. https://doi.org/10.3390/cells9112516