
A Comprehensive Exploration of the Biological Effects of Adipose-Derived Stem Cells in the Treatment of Systemic Sclerosis

 ,
,  , , ,
, , ,  , , ,
, , ,  and
and
Abstract
1. Introduction
2. Systemic Sclerosis (SSc)
2.1. Pathogenetic Mechanisms
2.2. Clinical Manifestations
3. ADSCs
3.1. Possible Biological Mechanisms Underlying ADSC Effects in SSc
3.1.1. Regulation of Inflammatory and Immune Responses
3.1.2. Reduction in Fibrosis
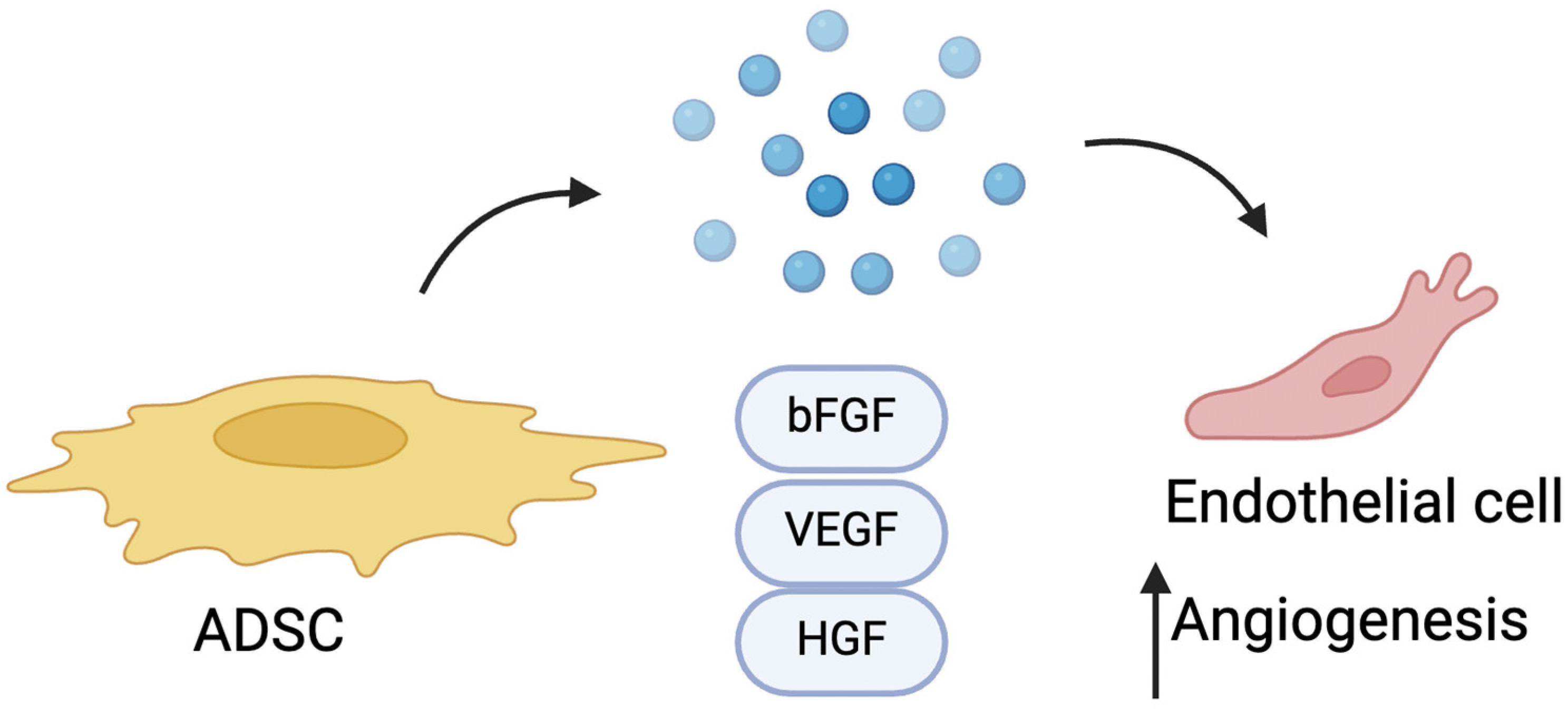
3.1.3. Pro-Angiogenic Effect of ADSCs
3.1.4. ADSC-Derived Extracellular Vesicles
3.2. Possible Effects of SSc on ADSCs
4. Clinical Applications of ADSCs in SSc Treatment
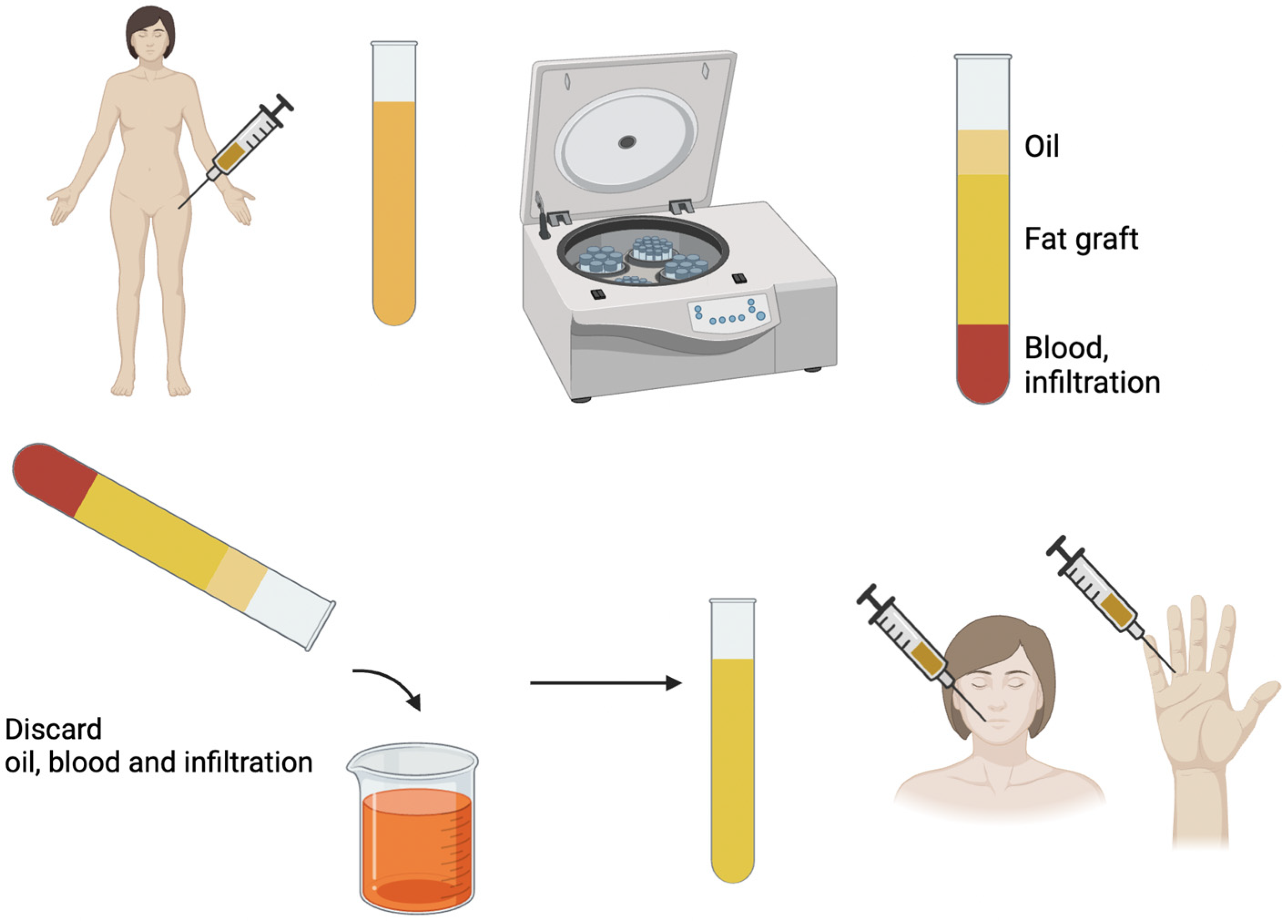
4.1. Lipofilling and Expanded ADSCs
4.2. Fat Grafting Enrichment
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bergamasco, A.; Hartmann, N.; Wallace, L.; Verpillat, P. Epidemiology of Systemic Sclerosis and Systemic Sclerosis-Associated Interstitial Lung Disease. Clin. Epidemiol. 2019, 11, 257–273. [Google Scholar] [CrossRef] [PubMed]
- Maria, A.T.J.; Maumus, M.; Le Quellec, A.; Jorgensen, C.; Noël, D.; Guilpain, P. Adipose-Derived Mesenchymal Stem Cells in Autoimmune Disorders: State of the Art and Perspectives for Systemic Sclerosis. Clin. Rev. Allergy Immunol. 2017, 52, 234–259. [Google Scholar] [CrossRef] [PubMed]
- Foti, R.; Storti, G.; Palmesano, M.; Scioli, M.G.; Fiorelli, E.; Terriaca, S.; Cervelli, G.; Kim, B.S.; Orlandi, A.; Cervelli, V. Senescence in Adipose-Derived Stem Cells: Biological Mechanisms and Therapeutic Challenges. Int. J. Mol. Sci. 2024, 25, 8390. [Google Scholar] [CrossRef]
- Ruhl, T.; Storti, G.; Pallua, N. Proliferation, Metabolic Activity, and Adipogenic Differentiation of Human Preadipocytes Exposed to 2 Surfactants In Vitro. J. Pharm. Sci. 2018, 107, 1408–1415. [Google Scholar] [CrossRef]
- Storti, G.; Scioli, M.G.; Kim, B.-S.; Terriaca, S.; Fiorelli, E.; Orlandi, A.; Cervelli, V. Mesenchymal Stem Cells in Adipose Tissue and Extracellular Vesicles in Ovarian Cancer Patients: A Bridge toward Metastatic Diffusion or a New Therapeutic Opportunity? Cells 2021, 10, 2117. [Google Scholar] [CrossRef] [PubMed]
- Scioli, M.G.; Storti, G.; Bielli, A.; Sanchez, M.; Scimeca, M.; Gimble, J.M.; Cervelli, V.; Orlandi, A. CD146 Expression Regulates Osteochondrogenic Differentiation of Human Adipose-Derived Stem Cells. J. Cell. Physiol. 2022, 237, 589–602. [Google Scholar] [CrossRef]
- Strong, A.L.; Peter Rubin, J.; Kozlow, J.H.; Cederna, P.S. Fat Grafting for the Treatment of Scleroderma. Plast. Reconstr. Surg. 2019, 144, 1498–1507. [Google Scholar] [CrossRef]
- Storti, G.; Favi, E.; Albanesi, F.; Kim, B.-S.; Cervelli, V. Adipose-Derived Stem/Stromal Cells in Kidney Transplantation: Status Quo and Future Perspectives. Int. J. Mol. Sci. 2021, 22, 1188. [Google Scholar] [CrossRef]
- Araújo, R.S.D.; Mussalem, M.G.V.B.; Carrijo, G.S.; Bani, J.V.d.F.; Ferreira, L.M. Adipose Tissue Derivatives in Peripheral Nerve Regeneration after Transection: A Systematic Review. Bioengineering 2024, 11, 697. [Google Scholar] [CrossRef]
- Tang, H.; He, Y.; Liang, Z.; Li, J.; Dong, Z.; Liao, Y. The Therapeutic Effect of Adipose-Derived Stem Cells on Soft Tissue Injury after Radiotherapy and Their Value for Breast Reconstruction. Stem Cell Res. Ther. 2022, 13, 493. [Google Scholar] [CrossRef]
- Surowiecka, A.; Chrapusta, A.; Klimeczek-Chrapusta, M.; Korzeniowski, T.; Drukała, J.; Strużyna, J. Mesenchymal Stem Cells in Burn Wound Management. Int. J. Mol. Sci. 2022, 23, 5339. [Google Scholar] [CrossRef]
- Zayed, M.A.; Sultan, S.; Alsaab, H.O.; Yousof, S.M.; Alrefaei, G.I.; Alsubhi, N.H.; Alkarim, S.; Al Ghamdi, K.S.; Bagabir, S.A.; Jana, A.; et al. Stem-Cell-Based Therapy: The Celestial Weapon against Neurological Disorders. Cells 2022, 11, 3476. [Google Scholar] [CrossRef] [PubMed]
- Coulange Zavarro, A.; Velier, M.; Arcani, R.; Abellan Lopez, M.; Simoncini, S.; Benyamine, A.; Gomes De Pinho, Q.; Coatmeur, R.; Wang, J.; Xia, J.; et al. Adipose Tissue and Adipose-Tissue-Derived Cell Therapies for the Treatment of the Face and Hands of Patients Suffering from Systemic Sclerosis. Biomedicines 2023, 11, 348. [Google Scholar] [CrossRef] [PubMed]
- Denton, C.P.; Khanna, D. Systemic Sclerosis. Lancet 2017, 390, 1685–1699. [Google Scholar] [CrossRef] [PubMed]
- Ciaffi, J.; Morabito, M.F.; Ruscitti, P.; D’Angelo, S.; Mancarella, L.; Brusi, V.; Abignano, G.; Pucino, V.; Giacomelli, R.; Meliconi, R.; et al. Incidence, Prevalence and Mortality of Systemic Sclerosis in Italy: A Nationwide Population-Based Study Using Administrative Health Data. Rheumatol. Int. 2021, 41, 129–137. [Google Scholar] [CrossRef]
- Lepri, G.; Di Battista, M.; Codullo, V.; Bonomi, F.; Sulis, A.; Guiducci, S.; Rossa, A. Della Systemic Sclerosis: One Year in Review 2024. Clin. Exp. Rheumatol. 2024, 42, 1517–1528. [Google Scholar] [CrossRef]
- Furue, M.; Mitoma, C.; Mitoma, H.; Tsuji, G.; Chiba, T.; Nakahara, T.; Uchi, H.; Kadono, T. Pathogenesis of Systemic Sclerosis-Current Concept and Emerging Treatments. Immunol. Res. 2017, 65, 790–797. [Google Scholar] [CrossRef]
- Rosendahl, A.H.; Schönborn, K.; Krieg, T. Pathophysiology of Systemic Sclerosis (Scleroderma). Kaohsiung J. Med. Sci. 2022, 38, 187–195. [Google Scholar] [CrossRef]
- Zurawski, G.; de Vries, J.E. Interleukin 13, an Interleukin 4-like Cytokine That Acts on Monocytes and B Cells, but Not on T Cells. Immunol. Today 1994, 15, 19–26. [Google Scholar] [CrossRef]
- Doucet, C.; Brouty-Boyé, D.; Pottin-Clemenceau, C.; Jasmin, C.; Canonica, G.W.; Azzarone, B. IL-4 and IL-13 Specifically Increase Adhesion Molecule and Inflammatory Cytokine Expression in Human Lung Fibroblasts. Int. Immunol. 1998, 10, 1421–1433. [Google Scholar] [CrossRef]
- Massagué, J. TGFβ Signalling in Context. Nat. Rev. Mol. Cell Biol. 2012, 13, 616–630. [Google Scholar] [CrossRef]
- Knipper, J.A.; Willenborg, S.; Brinckmann, J.; Bloch, W.; Maaß, T.; Wagener, R.; Krieg, T.; Sutherland, T.; Munitz, A.; Rothenberg, M.E.; et al. Interleukin-4 Receptor α Signaling in Myeloid Cells Controls Collagen Fibril Assembly in Skin Repair. Immunity 2015, 43, 803–816. [Google Scholar] [CrossRef]
- Tecchio, C.; Micheletti, A.; Cassatella, M.A. Neutrophil-Derived Cytokines: Facts beyond Expression. Front. Immunol. 2014, 5, 508. [Google Scholar] [CrossRef] [PubMed]
- Kozikowska, M.; Luboń, W.; Kucharz, E.J.; Mrukwa-Kominek, E. Ocular Manifestations in Patients with Systemic Sclerosis. Reumatologia 2020, 58, 401–406. [Google Scholar] [CrossRef] [PubMed]
- Gagliano, C.; Visalli, E.; Toro, M.D.; Amato, R.; Panta, G.; Scollo, D.; Scandura, G.; Ficili, S.; Amato, G.; Benenati, A.; et al. Dry Eye in Systemic Sclerosis Patients: Novel Methods to Monitor Disease Activity. Diagnostics 2020, 10, 404. [Google Scholar] [CrossRef]
- Foti, R.; Zeppieri, M.; Foti, R.; Visalli, E.; Amato, G.; Amato, R.; Dammino, E.; D’Esposito, F.; Gagliano, C. Retinal Vascular Abnormalities and Clinical Parameters in Systemic Sclerosis. J. Clin. Med. 2024, 13, 2738. [Google Scholar] [CrossRef]
- Volkmann, E.R.; Andréasson, K.; Smith, V. Systemic Sclerosis. Lancet 2023, 401, 304–318. [Google Scholar] [CrossRef]
- Jerjen, R.; Nikpour, M.; Krieg, T.; Denton, C.P.; Saracino, A.M. Systemic Sclerosis in Adults. Part II: Management and Therapeutics. J. Am. Acad. Dermatol. 2022, 87, 957–978. [Google Scholar] [CrossRef] [PubMed]
- Hughes, M.; Allanore, Y.; Chung, L.; Pauling, J.D.; Denton, C.P.; Matucci-Cerinic, M. Raynaud Phenomenon and Digital Ulcers in Systemic Sclerosis. Nat. Rev. Rheumatol. 2020, 16, 208–221. [Google Scholar] [CrossRef]
- Hughes, M.; Bruni, C.; Ruaro, B.; Confalonieri, M.; Matucci-Cerinic, M.; Bellando-Randone, S. Digital Ulcers in Systemic Sclerosis. Presse Med. 2021, 50, 104064. [Google Scholar] [CrossRef]
- Morrisroe, K.; Stevens, W.; Sahhar, J.; Ngian, G.S.; Ferdowsi, N.; Hill, C.L.; Roddy, J.; Walker, J.; Proudman, S.; Nikpour, M. Digital Ulcers in Systemic Sclerosis: Their Epidemiology, Clinical Characteristics, and Associated Clinical and Economic Burden. Arthritis Res. Ther. 2019, 21, 299. [Google Scholar] [CrossRef] [PubMed]
- Varga, J.; Trojanowska, M.; Kuwana, M. Pathogenesis of Systemic Sclerosis: Recent Insights of Molecular and Cellular Mechanisms and Therapeutic Opportunities. J. Scleroderma Relat. Disord. 2017, 2, 137–152. [Google Scholar] [CrossRef]
- Cutolo, M.; Herrick, A.L.; Distler, O.; Becker, M.O.; Beltran, E.; Carpentier, P.; Ferri, C.; Inanç, M.; Vlachoyiannopoulos, P.; Chadha-Boreham, H.; et al. Nailfold Videocapillaroscopic Features and Other Clinical Risk Factors for Digital Ulcers in Systemic Sclerosis: A Multicenter, Prospective Cohort Study. Arthritis Rheumatol. 2016, 68, 2527–2539. [Google Scholar] [CrossRef]
- Trombetta, A.C.; Pizzorni, C.; Ruaro, B.; Paolino, S.; Sulli, A.; Smith, V.; Cutolo, M. Effects of Longterm Treatment with Bosentan and Iloprost on Nailfold Absolute Capillary Number, Fingertip Blood Perfusion, and Clinical Status in Systemic Sclerosis. J. Rheumatol. 2016, 43, 2033–2041. [Google Scholar] [CrossRef] [PubMed]
- Bhat, Y.; Bashir, Y.; Latif, I.; Daing, A.; Devi, R.; Shah, I.; Akhtar, S.; Rather, S.; Nabi, N.; Saqib, N. Efficacy of Fractional CO2 Laser for Improvement of Limited Mouth Opening in Systemic Sclerosis. J. Cutan. Aesthet. Surg. 2022, 15, 387–393. [Google Scholar] [CrossRef]
- Jeon, F.H.K.; Griffin, M.; Denton, C.P.; Butler, P.E.M. Feasibility Study of Stem-Cell Enriched Autologous Lipotransfer to Treat Oro-Facial Fibrosis in Systemic Sclerosis (Sys-Stem): Protocol for Open-Label Randomised Controlled Trial. Int. J. Surg. Protoc. 2020, 23, 6–10. [Google Scholar] [CrossRef]
- Denton, C.P.; Black, C.M.; Abraham, D.J. Mechanisms and Consequences of Fibrosis in Systemic Sclerosis. Nat. Clin. Pract. Rheumatol. 2006, 2, 134–144. [Google Scholar] [CrossRef] [PubMed]
- Veale, B.J.; Jablonski, R.Y.; Frech, T.M.; Pauling, J.D. Orofacial Manifestations of Systemic Sclerosis. Br. Dent. J. 2016, 221, 305–310. [Google Scholar] [CrossRef]
- Strong, A.L.; Adidharma, W.; Brown, O.H.; Cederna, P.S. Fat Grafting Subjectively Improves Facial Skin Elasticity and Hand Function of Scleroderma Patients. Plast. Reconstr. Surg. Glob. Open 2021, 9, E3373. [Google Scholar] [CrossRef]
- Jeon, F.H.K.; Griffin, M.; Varghese, J.; Butler, P.E.M. Oro-Facial Fibrosis in Systemic Sclerosis: A Reconstructive Journey. BMJ Case Rep. 2020, 13, e236663. [Google Scholar] [CrossRef]
- Kumar, R.; Griffin, M.; Adigbli, G.; Kalavrezos, N.; Butler, P.E.M. Lipotransfer for Radiation-Induced Skin Fibrosis. Br. J. Surg. 2016, 103, 950–961. [Google Scholar] [CrossRef]
- Daumas, A.; Magalon, J.; Delaunay, F.; Abellan, M.; Philandrianos, C.; Sabatier, F.; Granel, B.; Magalon, G. Fat Grafting for Treatment of Facial Scleroderma. Clin. Plast. Surg. 2020, 47, 155–163. [Google Scholar] [CrossRef] [PubMed]
- Sautereau, N.; Daumas, A.; Truillet, R.; Jouve, E.; Magalon, J.; Veran, J.; Casanova, D.; Frances, Y.; Magalon, G.; Granel, B. Efficacy of Autologous Microfat Graft on Facial Handicap in Systemic Sclerosis Patients. Plast. Reconstr. Surg. Glob. Open 2016, 4, e660. [Google Scholar] [CrossRef]
- Iglesias, M.; Torre-Villalvazo, I.; Butrón-Gandarillas, P.; Rodríguez-Reyna, T.S.; Torre-Anaya, E.A.; Guevara-Cruz, M.; Flores-Cháirez, M.A.; López-Contreras, D.B.; López-Sánchez, J.Y.; Ruiz-Betanzos, Á.J.; et al. Adipose Derived Stromal Vascular Fraction and Fat Graft for Treating the Hands of Patients with Systemic Sclerosis. A Randomized Clinical Trial. PLoS ONE 2023, 18, e0289594. [Google Scholar] [CrossRef]
- Herrick, A.L.; Shukla, R.; Watson, R.E.B. Frontiers in Translational Systemic Sclerosis Research: A Focus on the Unmet “cutaneous” Clinical Needs (Viewpoint). Exp. Dermatol. 2020, 29, 1144–1153. [Google Scholar] [CrossRef] [PubMed]
- Mouthon, L. L’atteinte de La Main Dans La Sclérodermie Systémique. Presse Med. 2013, 42, 1616–1626. [Google Scholar] [CrossRef] [PubMed]
- Zuk, P.A.; Zhu, M.; Mizuno, H.; Huang, J.; Futrell, J.W.; Katz, A.J.; Benhaim, P.; Lorenz, H.P.; Hedrick, M.H. Multilineage Cells from Human Adipose Tissue: Implications for Cell-Based Therapies. Tissue Eng. 2001, 7, 211–228. [Google Scholar] [CrossRef]
- Gimble, J.M.; Katz, A.J.; Bunnell, B.A. Adipose-Derived Stem Cells for Regenerative Medicine. Circ. Res. 2007, 100, 1249–1260. [Google Scholar] [CrossRef]
- Bourin, P.; Bunnell, B.A.; Casteilla, L.; Dominici, M.; Katz, A.J.; March, K.L.; Redl, H.; Rubin, J.P.; Yoshimura, K.; Gimble, J.M. Stromal Cells from the Adipose Tissue-Derived Stromal Vascular Fraction and Culture Expanded Adipose Tissue-Derived Stromal/Stem Cells: A Joint Statement of the International Federation for Adipose Therapeutics and Science (IFATS) and the International Society for Cellular Therapy (ISCT). Cytotherapy 2013, 15, 641–648. [Google Scholar] [CrossRef]
- Ullah, I.; Subbarao, R.B.; Rho, G.J. Human Mesenchymal Stem Cells—Current Trends and Future Prospective. Biosci. Rep. 2015, 35, e00191. [Google Scholar] [CrossRef]
- Laloze, J.; Fiévet, L.; Desmoulière, A. Adipose-Derived Mesenchymal Stromal Cells in Regenerative Medicine: State of Play, Current Clinical Trials, and Future Prospects. Adv. Wound Care 2021, 10, 24–48. [Google Scholar] [CrossRef] [PubMed]
- Raposio, E.; Simonacci, F.; Perrotta, R.E. Adipose-Derived Stem Cells: Comparison between Two Methods of Isolation for Clinical Applications. Ann. Med. Surg. 2017, 20, 87. [Google Scholar] [CrossRef] [PubMed]
- Mazini, L.; Ezzoubi, M.; Malka, G. Overview of Current Adipose-Derived Stem Cell (ADSCs) Processing Involved in Therapeutic Advancements: Flow Chart and Regulation Updates before and after COVID-19. Stem Cell Res. Ther. 2021, 12, 1. [Google Scholar] [CrossRef]
- Storti, G.; Scioli, M.G.; Kim, B.S.; Orlandi, A.; Cervelli, V.; De Francesco, F. Adipose-Derived Stem Cells in Bone Tissue Engineering: Useful Tools with New Applications. Stem Cells Int. 2019, 2019, 3673857. [Google Scholar] [CrossRef]
- Jia, Q.; Zhao, H.; Wang, Y.; Cen, Y.; Zhang, Z. Mechanisms and Applications of Adipose-Derived Stem Cell-Extracellular Vesicles in the Inflammation of Wound Healing. Front. Immunol. 2023, 14, 1214757. [Google Scholar] [CrossRef]
- Higginbotham, S.; Workman, V.L.; Giblin, A.V.; Green, N.H.; Lambert, D.W.; Hearnden, V. Inhibition and Reversal of a TGF-Β1 Induced Myofibroblast Phenotype by Adipose Tissue-Derived Paracrine Factors. Stem Cell Res. Ther. 2024, 15, 166. [Google Scholar] [CrossRef]
- Naderi, N.; Combellack, E.J.; Griffin, M.; Sedaghati, T.; Javed, M.; Findlay, M.W.; Wallace, C.G.; Mosahebi, A.; Butler, P.E.M.; Seifalian, A.M.; et al. The Regenerative Role of Adipose-Derived Stem Cells (ADSC) in Plastic and Reconstructive Surgery. Int. Wound J. 2017, 14, 112–124. [Google Scholar] [CrossRef]
- Rozier, P.; Maumus, M.; Maria, A.T.J.; Toupet, K.; Lai-Kee-Him, J.; Jorgensen, C.; Guilpain, P.; Noël, D. Mesenchymal Stromal Cells-Derived Extracellular Vesicles Alleviate Systemic Sclerosis via MiR-29a-3p. J. Autoimmun. 2021, 121, 102660. [Google Scholar] [CrossRef] [PubMed]
- Mohammedsaleh, Z.M. The Use of Patient-Specific Stem Cells in Different Autoimmune Diseases. Saudi J. Biol. Sci. 2022, 29, 3338–3346. [Google Scholar] [CrossRef]
- Kornicka, K.; Śmieszek, A.; Węgrzyn, A.S.; Röcken, M.; Marycz, K. Immunomodulatory Properties of Adipose-Derived Stem Cells Treated with 5-Azacytydine and Resveratrol on Peripheral Blood Mononuclear Cells and Macrophages in Metabolic Syndrome Animals. J. Clin. Med. 2018, 7, 383. [Google Scholar] [CrossRef]
- Zargarani, S.; Tavaf, M.J.; Soltanmohammadi, A.; Yazdanpanah, E.; Baharlou, R.; Yousefi, B.; Sadighimoghaddam, B.; Esmaeili, S.A.; Haghmorad, D. Adipose-Derived Mesenchymal Stem Cells Ameliorates Experimental Autoimmune Encephalomyelitis via Modulation of Th1/Th17 and Expansion of Th2/Treg Responses. Cell Biol. Int. 2024, 48, 1124–1137. [Google Scholar] [CrossRef] [PubMed]
- Kuca-Warnawin, E.; Janicka, I.; Szczęsny, P.; Olesińska, M.; Bonek, K.; Głuszko, P.; Kontny, E. Modulation of T-Cell Activation Markers Expression by the Adipose Tissue-Derived Mesenchymal Stem Cells of Patients with Rheumatic Diseases. Cell Transplant. 2020, 29, 963689720945682. [Google Scholar] [CrossRef] [PubMed]
- Kuca-Warnawin, E.; Olesińska, M.; Szczȩsny, P.; Kontny, E. Impact and Possible Mechanism(s) of Adipose Tissue-Derived Mesenchymal Stem Cells on T-Cell Proliferation in Patients with Rheumatic Disease. Front. Physiol. 2022, 12, 749481. [Google Scholar] [CrossRef]
- Okamura, A.; Matsushita, T.; Komuro, A.; Kobayashi, T.; Maeda, S.; Hamaguchi, Y.; Takehara, K. Adipose-Derived Stromal/Stem Cells Successfully Attenuate the Fibrosis of Scleroderma Mouse Models. Int. J. Rheum. Dis. 2020, 23, 216–225. [Google Scholar] [CrossRef] [PubMed]
- Almadori, A.; Griffin, M.; Ryan, C.M.; Hunt, D.F.; Hansen, E.; Kumar, R.; Abraham, D.J.; Denton, C.P.; Butler, P.E.M. Stem Cell Enriched Lipotransfer Reverses the Effects of Fibrosis in Systemic Sclerosis. PLoS ONE 2019, 14, e0218068. [Google Scholar] [CrossRef]
- Tanaka, K.; Ogino, R.; Yamakawa, S.; Suda, S.; Hayashida, K. Role and Function of Mesenchymal Stem Cells on Fibroblast in Cutaneous Wound Healing. Biomedicines 2022, 10, 1391. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Maria, A.T.J.; Toupet, K.; Maumus, M.; Fonteneau, G.; Le Quellec, A.; Jorgensen, C.; Guilpain, P.; Noël, D. Human Adipose Mesenchymal Stem Cells as Potent Anti-Fibrosis Therapy for Systemic Sclerosis. J. Autoimmun. 2016, 70, 31–39. [Google Scholar] [CrossRef]
- Oh, C.K.; Lee, J.; Jang, B.S.; Kang, Y.S.; Bae, Y.C.; Kwon, K.S.; Jang, H.S. Treatment of Atrophies Secondary to Trilinear Scleroderma En Coup de Sabre by Autologous Tissue Cocktail Injection. Dermatol. Surg. 2003, 29, 1073–1075. [Google Scholar] [CrossRef]
- Chen, W.; Xia, Z.K.; Zhang, M.H.; Ding, G.C.; Zhang, X.Y.; Wang, Z.X.; Yang, R.Y. Adipose Tissue-Derived Stem Cells Ameliorates Dermal Fibrosis in a Mouse Model of Scleroderma. Asian Pac. J. Trop. Med. 2017, 10, 52–56. [Google Scholar] [CrossRef]
- Suzuka, T.; Kotani, T.; Saito, T.; Matsuda, S.; Sato, T.; Takeuchi, T. Therapeutic Effects of Adipose-Derived Mesenchymal Stem/Stromal Cells with Enhanced Migration Ability and Hepatocyte Growth Factor Secretion by Low-Molecular-Weight Heparin Treatment in Bleomycin-Induced Mouse Models of Systemic Sclerosis. Arthritis Res. Ther. 2022, 24, 228. [Google Scholar] [CrossRef]
- Guillaume-Jugnot, P.; Daumas, A.; Magalon, J.; Sautereau, N.; Veran, J.; Magalon, G.; Sabatier, F.; Granel, B. State of the Art. Autologous Fat Graft and Adipose Tissue-Derived Stromal Vascular Fraction Injection for Hand Therapy in Systemic Sclerosis Patients. Curr. Res. Transl. Med. 2016, 64, 35–42. [Google Scholar] [CrossRef]
- Frommer, M.L.; Langridge, B.J.; Awad, L.; Jasionowska, S.; Denton, C.P.; Abraham, D.J.; Abu-Hanna, J.; Butler, P.E.M. Single-Cell Analysis of ADSC Interactions with Fibroblasts and Endothelial Cells in Scleroderma Skin. Cells 2023, 12, 1784. [Google Scholar] [CrossRef]
- Wu, S.C.; Kuo, P.J.; Rau, C.S.; Huang, L.H.; Lin, C.W.; Wu, Y.C.; Wu, C.J.; Tsai, C.W.; Hsieh, T.M.; Liu, H.T.; et al. Increased Angiogenesis by Exosomes Secreted by Adipose-Derived Stem Cells upon Lipopolysaccharide Stimulation. Int. J. Mol. Sci. 2021, 22, 8877. [Google Scholar] [CrossRef]
- Velier, M.; Simoncini, S.; Abellan, M.; Francois, P.; Eap, S.; Lagrange, A.; Bertrand, B.; Daumas, A.; Granel, B.; Delorme, B.; et al. Adipose-Derived Stem Cells from Systemic Sclerosis Patients Maintain Pro-Angiogenic and Antifibrotic Paracrine Effects In Vitro. J. Clin. Med. 2019, 8, 1979. [Google Scholar] [CrossRef]
- Rozier, P.; Maumus, M.; Bony, C.; Maria, A.T.J.; Sabatier, F.; Jorgensen, C.; Guilpain, P.; Noël, D. Extracellular Vesicles Are More Potent than Adipose Mesenchymal Stromal Cells to Exert an Anti-Fibrotic Effect in an In Vitro Model of Systemic Sclerosis. Int. J. Mol. Sci. 2021, 22, 6837. [Google Scholar] [CrossRef]
- Fang, S.; Xu, C.; Zhang, Y.; Xue, C.; Yang, C.; Bi, H.; Qian, X.; Wu, M.; Ji, K.; Zhao, Y.; et al. Umbilical Cord-Derived Mesenchymal Stem Cell-Derived Exosomal MicroRNAs Suppress Myofibroblast Differentiation by Inhibiting the Transforming Growth Factor-β/SMAD2 Pathway During Wound Healing. Stem Cells Transl. Med. 2016, 5, 1425–1439. [Google Scholar] [CrossRef]
- Shao, L.; Zhang, Y.; Lan, B.; Wang, J.; Zhang, Z.; Zhang, L.; Xiao, P.; Meng, Q.; Geng, Y.J.; Yu, X.Y.; et al. MiRNA-Sequence Indicates That Mesenchymal Stem Cells and Exosomes Have Similar Mechanism to Enhance Cardiac Repair. Biomed. Res. Int. 2017, 2017, 4150705. [Google Scholar] [CrossRef]
- Capelli, C.; Zaccara, E.; Cipriani, P.; Di Benedetto, P.; Maglione, W.; Andracco, R.; Di Luca, G.; Pignataro, F.; Giacomelli, R.; Introna, M.; et al. Phenotypical and Functional Characteristics of in Vitro-Expanded Adipose-Derived Mesenchymal Stromal Cells from Patients with Systematic Sclerosis. Cell Transplant. 2017, 26, 841. [Google Scholar] [CrossRef]
- Rosa, I.; Romano, E.; Fioretto, B.S.; Matucci-Cerinic, M.; Manetti, M. Adipose-Derived Stem Cells: Pathophysiologic Implications vs Therapeutic Potential in Systemic Sclerosis. World J. Stem Cells 2021, 13, 30. [Google Scholar] [CrossRef]
- Manetti, M.; Romano, E.; Rosa, I.; Fioretto, B.S.; Praino, E.; Guiducci, S.; Iannone, F.; Ibba-Manneschi, L.; Matucci-Cerinic, M. Systemic Sclerosis Serum Steers the Differentiation of Adipose-Derived Stem Cells Toward Profibrotic Myofibroblasts: Pathophysiologic Implications. J. Clin. Med. 2019, 8, 1256. [Google Scholar] [CrossRef]
- Taki, Z.; Gostjeva, E.; Thilly, W.; Yaseen, B.; Lopez, H.; Mirza, M.; Hassuji, Z.; Vigneswaran, S.; Ahmed Abdi, B.; Hart, A.; et al. Pathogenic Activation of Mesenchymal Stem Cells Is Induced by the Disease Microenvironment in Systemic Sclerosis. Arthritis Rheumatol. 2020, 72, 1361–1374. [Google Scholar] [CrossRef]
- Di Benedetto, P.; Panzera, N.; Cipriani, P.; Mastroiaco, V.; Tessitore, A.; Liakouli, V.; Ruscitti, P.; Berardicurti, O.; Carubbi, F.; Guggino, G.; et al. Mesenchymal Stem Cells of Systemic Sclerosis Patients, Derived from Different Sources, Show a Profibrotic MicroRNA Profiling. Sci. Rep. 2019, 9, 7144. [Google Scholar] [CrossRef]
- Ra, J.C.; Kang, S.K.; Shin, I.S.; Park, H.G.; Joo, S.A.; Kim, J.G.; Kang, B.C.; Lee, Y.S.; Nakama, K.; Piao, M.; et al. Stem Cell Treatment for Patients with Autoimmune Disease by Systemic Infusion of Culture-Expanded Autologous Adipose Tissue Derived Mesenchymal Stem Cells. J. Transl. Med. 2011, 9, 181. [Google Scholar] [CrossRef]
- Griffin, M.; Ryan, C.M.; Pathan, O.; Abraham, D.; Denton, C.P.; Butler, P.E.M. Characteristics of Human Adipose Derived Stem Cells in Scleroderma in Comparison to Sex and Age Matched Normal Controls: Implications for Regenerative Medicine. Stem Cell Res. Ther. 2017, 8, 23. [Google Scholar] [CrossRef]
- Gheisari, M.; Ahmadzadeh, A.; Nobari, N.; Iranmanesh, B.; Mozafari, N. Autologous Fat Grafting in the Treatment of Facial Scleroderma. Dermatol. Res. Pract. 2018, 2018, 6568016. [Google Scholar] [CrossRef]
- Griffin, M.F.; Almadori, A.; Butler, P.E. Use of Lipotransfer in Scleroderma. Aesthet. Surg. J. 2017, 37, S33–S37. [Google Scholar] [CrossRef]
- Dudek, D.W.; Walczuk, E.; Wajda, A.; Paradowska-Gorycka, A. Mesenchymal Stem Cells in Systemic Sclerosis Therapy. Reumatologia 2020, 58, 324–330. [Google Scholar] [CrossRef]
- Scuderi, N.; Ceccarelli, S.; Onesti, M.G.; Fioramonti, P.; Guidi, C.; Romano, F.; Frati, L.; Angeloni, A.; Marchese, C. Human Adipose-Derived Stromal Cells for Cell-Based Therapies in the Treatment of Systemic Sclerosis. Cell Transplant. 2013, 22, 779–795. [Google Scholar] [CrossRef]
- Del Papa, N.; Di Luca, G.; Andracco, R.; Zaccara, E.; Maglione, W.; Pignataro, F.; Minniti, A.; Vitali, C. Regional Grafting of Autologous Adipose Tissue Is Effective in Inducing Prompt Healing of Indolent Digital Ulcers in Patients with Systemic Sclerosis: Results of a Monocentric Randomized Controlled Study. Arthritis Res. Ther. 2019, 21, 7. [Google Scholar] [CrossRef]
- Virzì, F.; Bianca, P.; Giammona, A.; Apuzzo, T.; Di Franco, S.; Mangiapane, L.R.; Colorito, M.L.; Catalano, D.; Scavo, E.; Nicotra, A.; et al. Combined Platelet-Rich Plasma and Lipofilling Treatment Provides Great Improvement in Facial Skin-Induced Lesion Regeneration for Scleroderma Patients. Stem Cell Res. Ther. 2017, 8, 236. [Google Scholar] [CrossRef]
- Wang, C.; Long, X.; Si, L.; Chen, B.; Zhang, Y.; Sun, T.; Zhang, X.; Zhao, R.C.; Wang, X. A Pilot Study On Ex Vivo Expanded Autologous Adipose-Derived Stem Cells of Improving Fat Retention in Localized Scleroderma Patients. Stem Cells Transl. Med. 2021, 10, 1148–1156. [Google Scholar] [CrossRef] [PubMed]
- Cervelli, V.; Storti, G. Novel Strategies to Improve Graft Survival and Retention. In Plastic and Aesthetic Regenerative Surgery and Fat Grafting: Clinical Application and Operative Techniques; Springer: Cham, Switzerland, 2022; pp. 165–182. [Google Scholar] [CrossRef]
- Onesti, M.G.; Fioramonti, P.; Carella, S.; Fino, P.; Marchese, C.; Scuderi, N. Improvement of Mouth Functional Disability in Systemic Sclerosis Patients over One Year in a Trial of Fat Transplantation versus Adipose-Derived Stromal Cells. Stem Cells Int. 2016, 2016, 2416192. [Google Scholar] [CrossRef] [PubMed]
- Cao, Y.; Kan, H.; Ma, X.; Zhang, Y.; Huang, J.; Long, X. Autologous Fat or Adipose-Derived Stem Cell Grafting in Systemic Sclerosis Treatment: A Systematic Review and Meta-Analysis. Clin. Exp. Rheumatol. 2023, 41, 1659–1669. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Authors and Year of Publication | Effects of ADSCs | Experimental Settings | Experimental Model | Reference |
|---|---|---|---|---|
| Higginbotham S. et al., 2024 | Inhibit myofibroblast activation and reduce collagen production by downregulating the TGF-β/Smad pathway | In vitro | TGFβ1-induced model of myofibroblast differentiation was used to test the effect of conditioned media from adipose tissues, ADSCs, or lipids on the proportion of fibroblasts and myofibroblasts. | [56] |
| Rozier P. et al., 2021 | Inhibit profibrotic pathways | In vitro | Extracellular vesicles were injected in the HOCl-induced SSc model. | [58] |
| Kornicka K. et al., 2018 | Reduce T lymphocyte proliferation | In vitro | Azacitidine/Resveratrol-treated ADSC isolated from metabolic syndrome horses. | [60] |
| Kuca-Warnawin E. et al., 2022 | Decrease T-cell proliferation | In vitro | PBMC and purified CD4+ T cells of healthy donors were activated and co-cultured with untreated or cytokine licensed ASCs, then analyzed by flow cytometry. | [63] |
| Okamura A. et al., 2020 | Decrease the infiltration of CD4+ and CD8+ T cells and macrophages into the skin | Animal model (mouse) | ADSCs were intravenously administered to a scleroderma model. | [64] |
| Maria A.T. et al., 2016 | Increase in the MMP1/TIMP1 ratio | Animal model (mouse) | Scleroderma mice received intravenous injection of BM-MSC from syngeneic BALB/c or allogeneic C57BL/6 mice and xenogeneic hBM-MSC or hADSC. | [67] |
| Chen W. et al., 2017 | Reduced skin thickness and hydroxyproline content | Animal model (mouse) | ADSCs were subcutaneously injected into the dorsal area in the model treatment mice group. | [69] |
| Suzuka T. et al., 2022 | Reduced skin fibrosis | Animal model | ADSCs activated with LMWH in the treatment of fibrosis. | [70] |
| Velier M. et al., 2019 | SSc-ADSCs maintain pro-angiogenic and anti-fibrotic paracrine effects | In vitro | ADSCs were co-cultured in transwell inserts with HMVEC-dA. | [74] |
| Rozier P. et al., 2021 | EVs have been shown to be more effective than the cells themselves in exerting anti-fibrotic effects | In vitro | ADSCs and EVs on TGFβ1-activated fibroblasts. | [75] |
| Rozier P. et al., 2021 | EVs alleviate systemic sclerosis via miR-29a-3p | Animal model | EVs were injected in the HOCl-induced SSc murine model. | [58] |
| Authors and Year of Publication | Role of ADSC | Type of Study | Study Design | Study Results | Reference |
|---|---|---|---|---|---|
| Scuderi N. et al., 2013 | Reduction in skin tightness and enhanced elasticity in treated areas | Prospective cohort study | Autologous ADSCs were transplanted into patients with scleroderma using a hyaluronic acid solution as the delivery medium | ADSC in hyaluronic acid solution determined a significant improvement in tightening of the skin without complications | [88] |
| Gheisari M. et al., 2018 | Reduced microstomia, improving oral function and reducing stiffness | Open-label study | Autologous ADSCs were transplanted | Improvement in mouth opening capacity 3 months after autologous fat transfer | [85] |
| Almadori A. et al., 2019 | Reductions in MHISS scores and enhanced esthetic outcomes | Open cohort study | Autologous ADSC-enriched lipotransfer treatment | Improvement of mouth function and facial volumetric appearance with improved psychological outcome | [65] |
| Del Papa N. et al., 2019 | To alleviate pain and to increase capillary density | Case–control study | Adipose tissue grafting consisted of injection, at the base of the finger with the ischemic digital ulcer, of 0.5–1 mL of adipose tissue after centrifugation of fat aspirate | Ischemic digital ulcer healing and pain reduction were observed | [89] |
| Daumas A. et al., 2020 | Enhanced skin flexibility, greater mouth opening, and improved facial contour | Case report | Microfat was mixed with PRP in an 80/20 proportion using two 10 mL syringes connected | Improvement in MHISS score | [42] |
| Virzì F. et al., 2017 | New blood vessel formation and collagen remodeling | Prospective cohort study | ADSC and PRP | Improved buccal’s rhyme, skin elasticity, and vascularization | [90] |
| Jeon F.H.K. et al., 2020 | Fat grafts appear to enhance capillary networks in the fibrotic areas | Case report | Autologous fat grafting and z plasty | Maximal mouth opening increase | [40] |
| Wang C. et al., 2021 | Superiority of ADSC-assisted fat grafting over traditional fat grafting and SVF-assisted grafting in treating facial atrophy | Pilot study | ADSC-assisted fat grafting, fat grafting, and SVF-assisted grafting | Improvement of facial atrophy caused by LoS | [91] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Storti, G.; Foti, R.; Foti, R.; Palmesano, M.; Patacchiola, M.; Incognito, D.; Cervelli, G.; Longo, B.; Scioli, M.G.; Fiorelli, E.; et al. A Comprehensive Exploration of the Biological Effects of Adipose-Derived Stem Cells in the Treatment of Systemic Sclerosis. Cells 2025, 14, 458. https://doi.org/10.3390/cells14060458
Storti G, Foti R, Foti R, Palmesano M, Patacchiola M, Incognito D, Cervelli G, Longo B, Scioli MG, Fiorelli E, et al. A Comprehensive Exploration of the Biological Effects of Adipose-Derived Stem Cells in the Treatment of Systemic Sclerosis. Cells. 2025; 14(6):458. https://doi.org/10.3390/cells14060458
Chicago/Turabian StyleStorti, Gabriele, Riccardo Foti, Roberta Foti, Marco Palmesano, Martina Patacchiola, Dalila Incognito, Giulio Cervelli, Benedetto Longo, Maria Giovanna Scioli, Elena Fiorelli, and et al. 2025. "A Comprehensive Exploration of the Biological Effects of Adipose-Derived Stem Cells in the Treatment of Systemic Sclerosis" Cells 14, no. 6: 458. https://doi.org/10.3390/cells14060458
APA StyleStorti, G., Foti, R., Foti, R., Palmesano, M., Patacchiola, M., Incognito, D., Cervelli, G., Longo, B., Scioli, M. G., Fiorelli, E., Terriaca, S., Lisa, A., Kim, B. S., Orlandi, A., & Cervelli, V. (2025). A Comprehensive Exploration of the Biological Effects of Adipose-Derived Stem Cells in the Treatment of Systemic Sclerosis. Cells, 14(6), 458. https://doi.org/10.3390/cells14060458