
Predictive Value of Flow Cytometry Quantification of BAL Lymphocytes and Neutrophils in ILD

 , , ,
, , ,  ,
,  and
and 
Abstract

1. Introduction
2. Materials and Methods
2.1. Patients and Samples
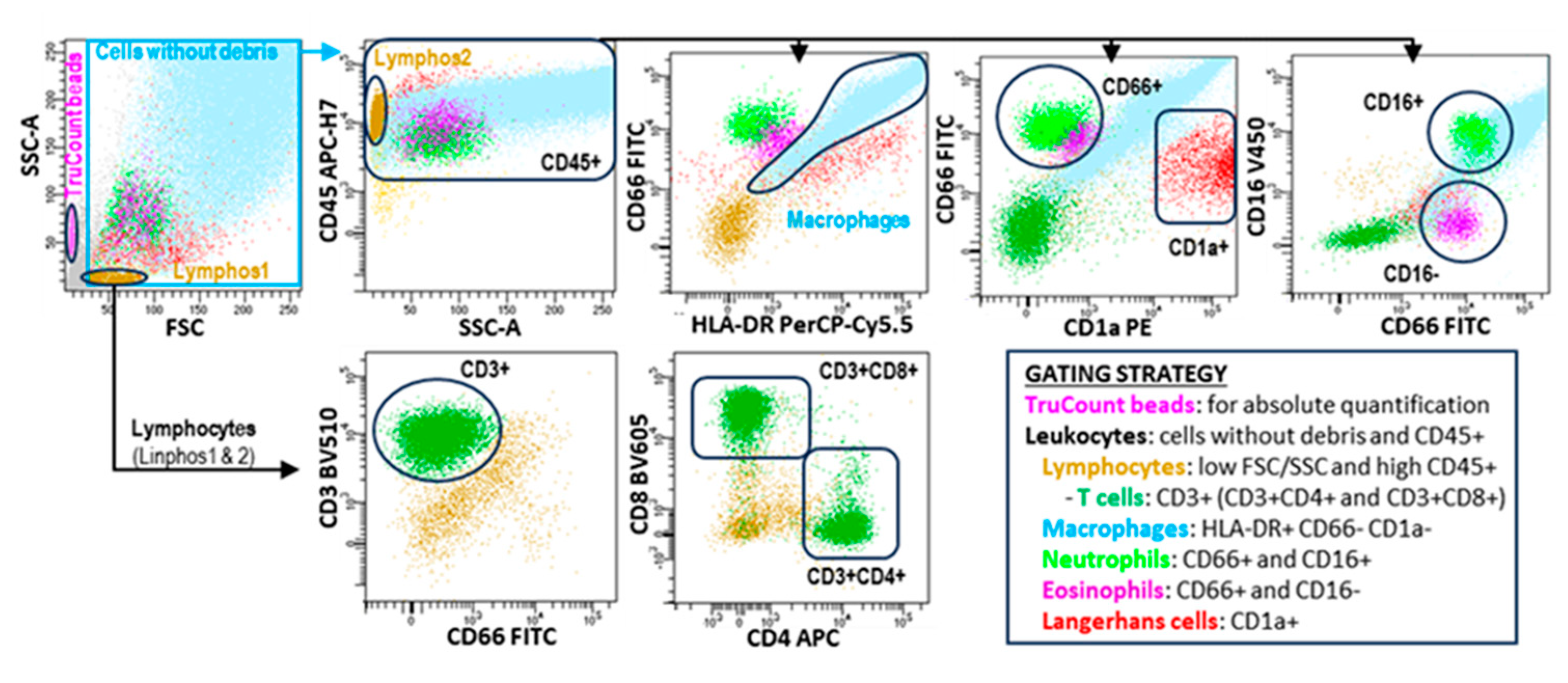
2.2. Immunophenotype Studies
2.3. Statistical Analysis
3. Results
3.1. Clinical, Biological, and Therapeutic Characteristics of Study Groups
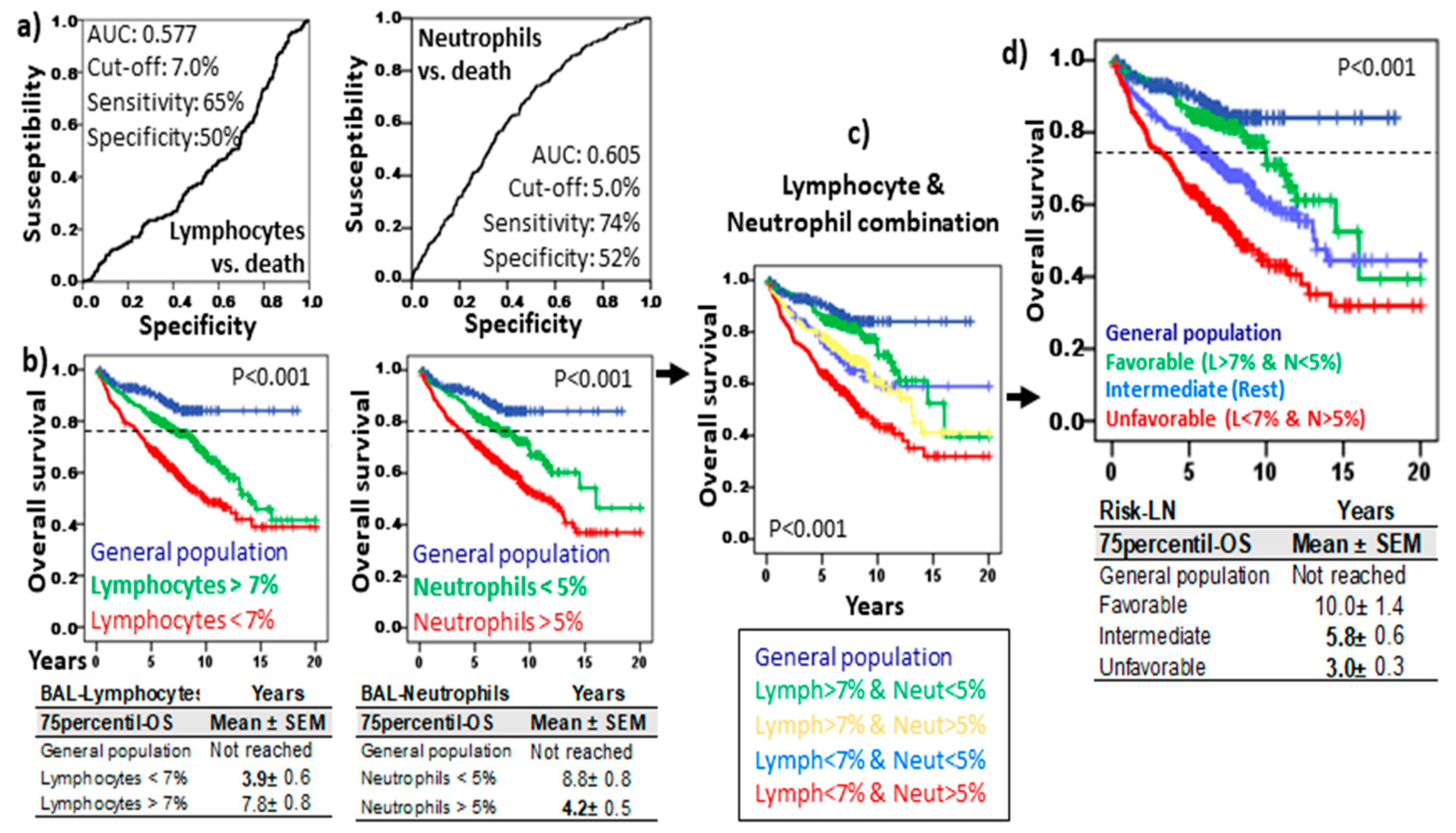
3.2. Risk Stratification of ILDs Based on Lymphocyte and Neutrophil Counts in BAL (Risk-LN)
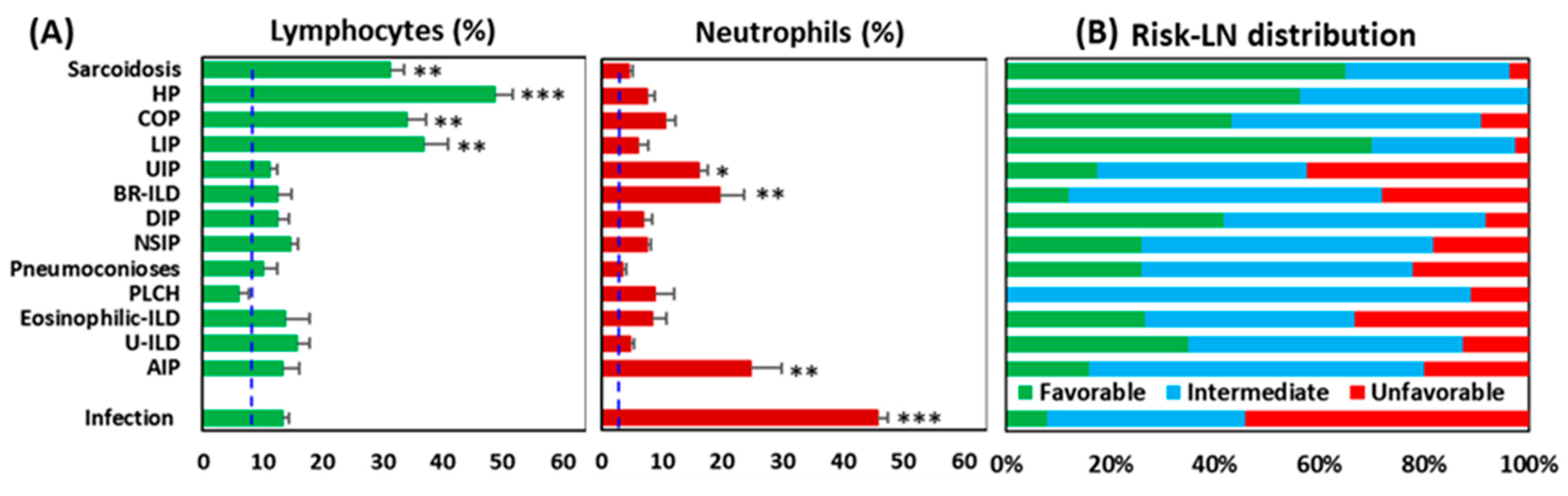
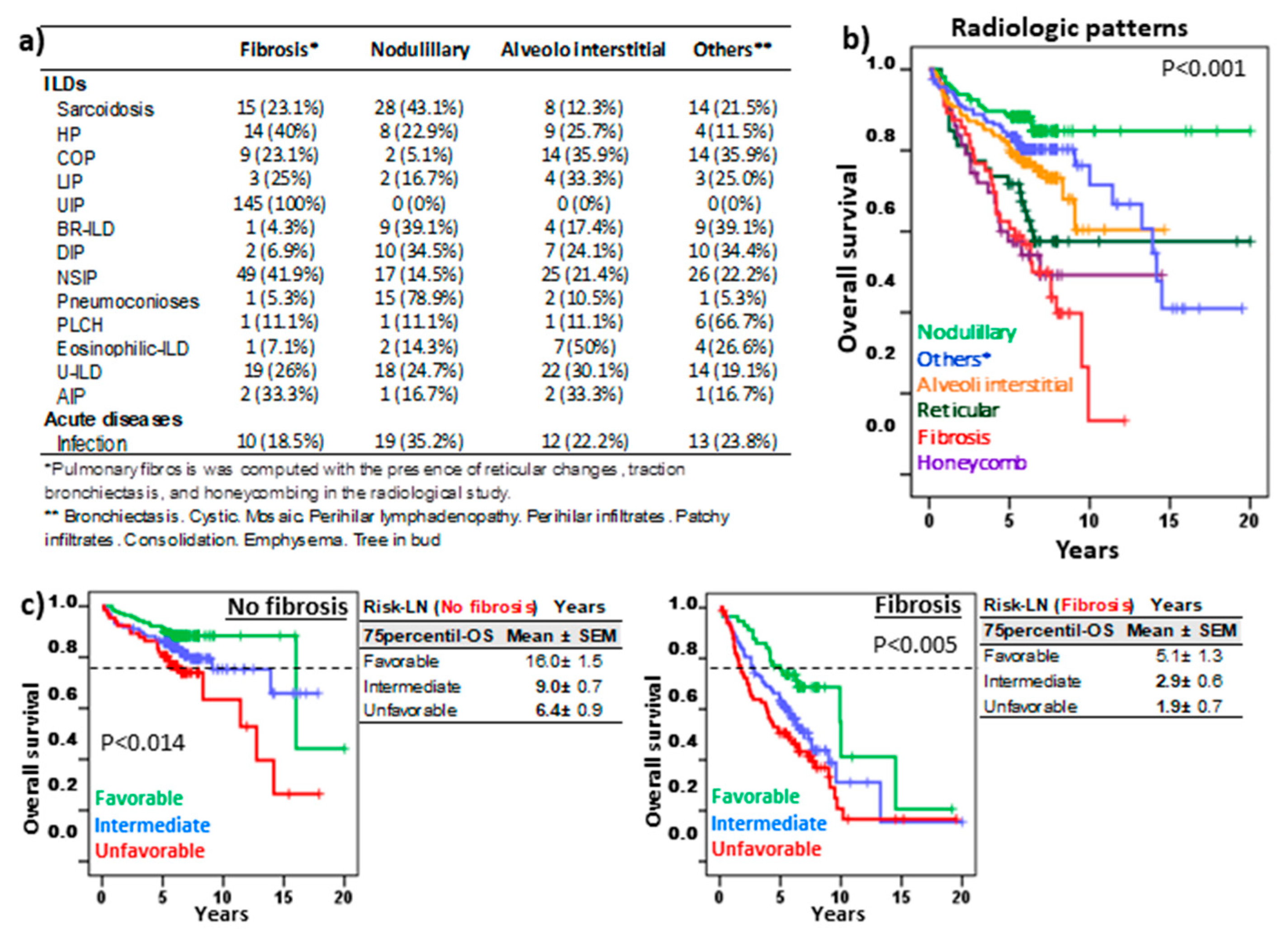
3.3. Uneven Distribution of Risk-LN Groups Among Pulmonary Pathologies
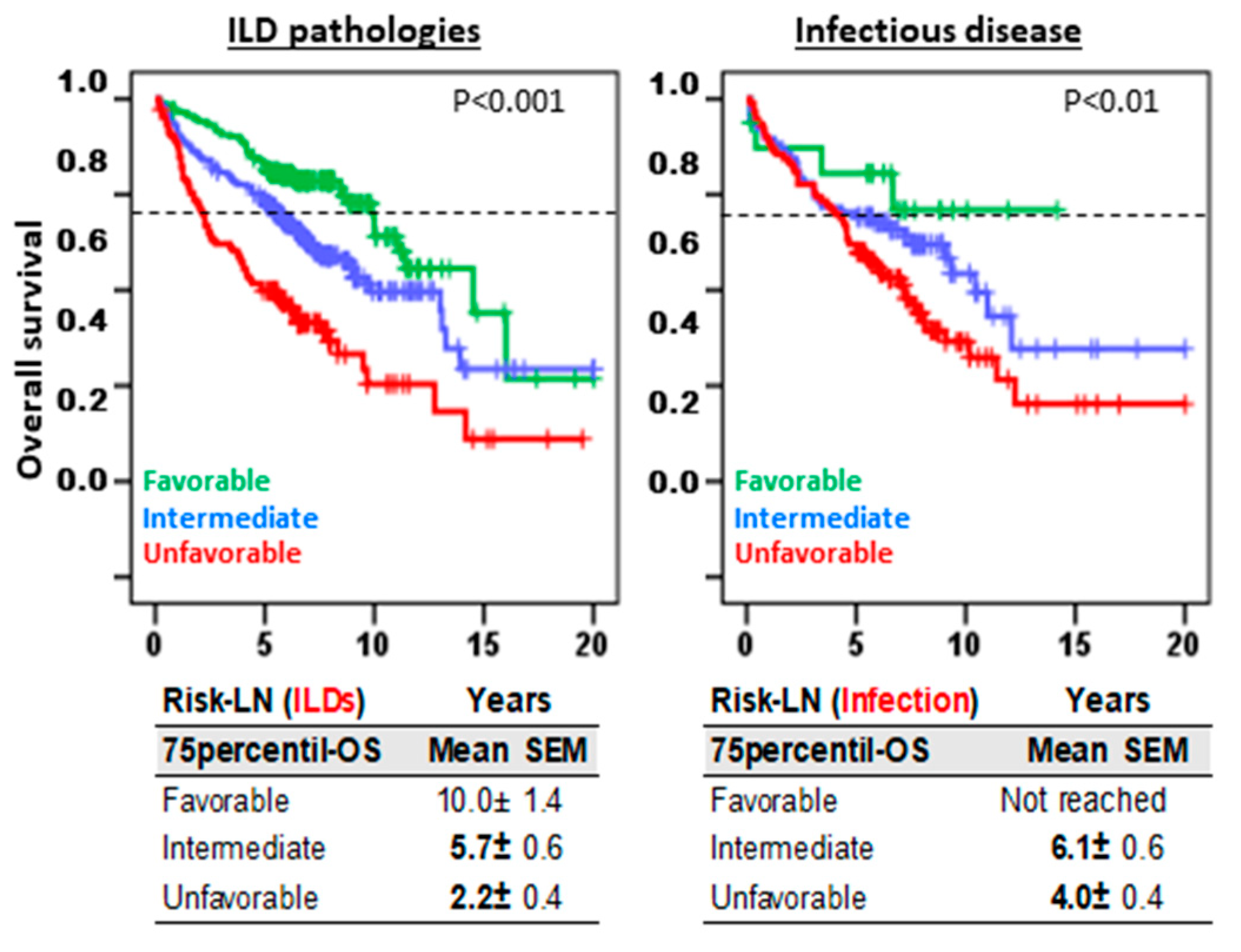
3.4. Risk-LN Stratification Preserves Its Predictive Value in Pathologies With or Without Pulmonary Fibrosis
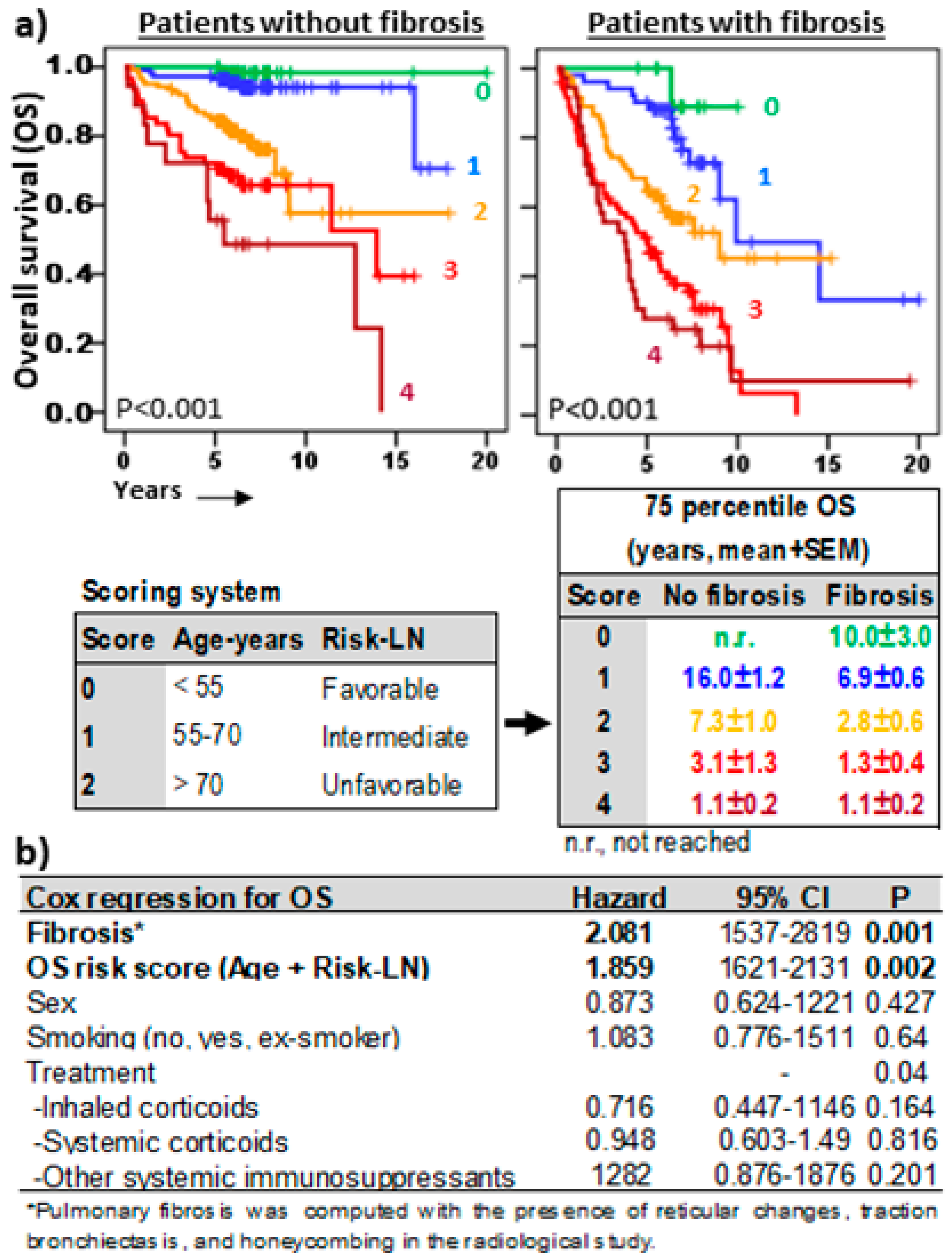
3.5. Risk-LN Predictive Capacity Was Independent of the Type of Treatment
3.6. Risk-LN, DLCO, and Fibrosis Are Independent and Complementary Predictive Factors in ILD
3.7. Risk-Scoring Model for Overall Survival Useful in Fibrotic and Non-Fibrotic ILDs
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bagnato, G.; Harari, S. Cellular interactions in the pathogenesis of interstitial lung diseases. Eur. Respir. Rev. 2015, 24, 102–114. [Google Scholar] [CrossRef]
- Moss, B.J.; Ryter, S.W.; Rosas, I.O. Pathogenic Mechanisms Underlying Idiopathic Pulmonary Fibrosis. Annu. Rev. Pathol. Mech. Dis. 2022, 17, 515–546. [Google Scholar] [CrossRef] [PubMed]
- Ley, B.; Ryerson, C.J.; Vittinghoff, E.; Ryu, J.; Tomassetti, S.; Lee, J.S.; Poletti, V.; Buccioli, M.; Elicker, B.M.; Jones, K.D.; et al. A multidimensional index and staging system for idiopathic pulmonary fibrosis. Ann. Intern. Med. 2012, 156, 684–691. [Google Scholar] [CrossRef] [PubMed]
- Salisbury, M.L.; Xia, M.; Zhou, Y.; Zhou, Y.; Murray, S.; Tayob, N.; Brown, K.K.; Wells, A.U.; Schmidt, S.L.; Martinez, F.J.; et al. Idiopathic Pulmonary Fibrosis: Gender-Age-Physiology Index Stage for Predicting Future Lung Function Decline. Chest 2016, 149, 491–498. [Google Scholar] [CrossRef] [PubMed]
- Ley, B.; Bradford, W.Z.; Weycker, D.; Vittinghoff, E.; du Bois, R.M.; Collard, H.R. Unified baseline and longitudinal mortality prediction in idiopathic pulmonary fibrosis. Eur. Respir. J. 2015, 45, 1374–1381. [Google Scholar] [CrossRef]
- Suzuki, Y.; Mori, K.; Aono, Y.; Kono, M.; Hasegawa, H.; Yokomura, K.; Naoi, H.; Hozumi, H.; Karayama, M.; Furuhashi, K.; et al. Combined assessment of the GAP index and body mass index at antifibrotic therapy initiation for prognosis of idiopathic pulmonary fibrosis. Sci. Rep. 2021, 11, 18579. [Google Scholar] [CrossRef] [PubMed]
- Chandel, A.; Pastre, J.; Valery, S.; King, C.S.; Nathan, S.D. Derivation and validation of a simple multidimensional index incorporating exercise capacity parameters for survival prediction in idiopathic pulmonary fibrosis. Thorax 2023, 78, 368–375. [Google Scholar] [CrossRef] [PubMed]
- Chandel, A.; King, C.S.; Ignacio, R.V.; Pastre, J.; Shlobin, O.A.; Khangoora, V.; Aryal, S.; Nyquist, A.; Singhal, A.; Flaherty, K.R.; et al. External validation and longitudinal application of the DO-GAP index to individualise survival prediction in idiopathic pulmonary fibrosis. ERJ Open Res. 2023, 9, 00124-2023. [Google Scholar] [CrossRef]
- Lee, J.H.; Jang, J.H.; Jang, H.-J.; Kim, S.Y.; Chung, M.P.; Yoo, H.; Jeong, S.H.; Song, J.W.; Lee, H.L.; Choi, S.M.; et al. New prognostic scoring system for mortality in idiopathic pulmonary fibrosis by modifying the gender, age, and physiology model with desaturation during the six-minute walk test. Front. Med. 2023, 10, 1052129. [Google Scholar] [CrossRef]
- Zhu, W.-W.; Li, H.; Li, Y.-D.; Sun, L.; Kong, L.; Ye, X.; Cai, Q.; Lv, X.-Z. Risk assessment in interstitial lung disease: The incremental prognostic value of cardiopulmonary ultrasound. BMC Pulm. Med. 2021, 21, 237. [Google Scholar] [CrossRef]
- Ryerson, C.J.; Vittinghoff, E.; Ley, B.; Lee, J.S.; Mooney, J.J.; Jones, K.D.; Elicker, B.M.; Wolters, P.J.; Koth, L.L.; King, T.E.; et al. Predicting survival across chronic interstitial lung disease: The ILD-GAP model. Chest 2014, 145, 723–728. [Google Scholar] [CrossRef] [PubMed]
- Almeida, L.M.; Fernandes, A.L.; Cardoso, C.G.; Lima, B.; Neves, I.; Novais-Bastos, H.; Mota, P.C.; Melo, N.; Moura, C.S.; Guimarães, S.; et al. Mortality risk prediction with ILD-GAP index in a fibrotic hypersensitivity pneumonitis cohort. Ther. Adv. Respir. Dis. 2022, 16, 17534666221135316. [Google Scholar] [CrossRef] [PubMed]
- Shi, S.; Chen, L.; Liu, X.; Yu, M.; Wu, C.; Xiao, Y. Development of a scoring system with multidimensional markers for fibrosing interstitial lung disease. Sci. Rep. 2022, 12, 14217. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Guo, J.; Yu, D.; Jie, B.; Zhou, Y. Predictors of Mortality in Progressive Fibrosing Interstitial Lung Diseases. Front. Pharmacol. 2021, 12, 754851. [Google Scholar] [CrossRef] [PubMed]
- Ruaro, B.; Baratella, E.; Confalonieri, P.; Wade, B.; Marrocchio, C.; Geri, P.; Busca, A.; Pozzan, R.; Andrisano, A.G.; Cova, M.A.; et al. High-Resolution Computed Tomography: Lights and Shadows in Improving Care for SSc-ILD Patients. Diagnostics 2021, 11, 1960. [Google Scholar] [CrossRef] [PubMed]
- Hughes, M.; Bruni, C.; Cuomo, G.; Sedie, A.D.; Gargani, L.; Gutierrez, M.; Lepri, G.; Ruaro, B.; Santiago, T.; Suliman, Y.; et al. The role of ultrasound in systemic sclerosis: On the cutting edge to foster clinical and research advancement. J. Scleroderma Relat. Disord. 2021, 6, 123–132. [Google Scholar] [CrossRef] [PubMed]
- Salonen, J.; Lampela, H.; Keskitalo, E.; Vähänikkilä, H.; Purokivi, M.; Kaarteenaho, R. Bronchoalveolar lavage differential cell count on prognostic assessment of patients with stable or acute interstitial lung disease: A retrospective real-life study. Clin. Immunol. 2020, 220, 108594. [Google Scholar] [CrossRef]
- Kinder, B.W.; Brown, K.K.; Schwarz, M.I.; Ix, J.H.; Kervitsky, A.; King, T.E. Baseline BAL neutrophilia predicts early mortality in idiopathic pulmonary fibrosis. Chest 2008, 133, 226–232. [Google Scholar] [CrossRef] [PubMed]
- Kono, M.; Miyashita, K.; Hirama, R.; Oshima, Y.; Takeda, K.; Mochizuka, Y.; Tsutsumi, A.; Miwa, H.; Miki, Y.; Hashimoto, D.; et al. Prognostic significance of bronchoalveolar lavage cellular analysis in patients with acute exacerbation of interstitial lung disease. Respir. Med. 2021, 186, 106534. [Google Scholar] [CrossRef] [PubMed]
- Hirasawa, Y.; Nakada, T.-A.; Shimazui, T.; Abe, M.; Isaka, Y.; Sakayori, M.; Suzuki, K.; Yoshioka, K.; Kawasaki, T.; Terada, J.; et al. Prognostic value of lymphocyte counts in bronchoalveolar lavage fluid in patients with acute respiratory failure: A retrospective cohort study. J. Intensiv. Care 2021, 9, 21. [Google Scholar] [CrossRef] [PubMed]
- Meyer, K.C.; Raghu, G.; Baughman, R.P.; Brown, K.K.; Costabel, U.; du Bois, R.M.; Drent, M.; Haslam, P.L.; Kim, D.S.; Nagai, S.; et al. An official American Thoracic Society clinical practice guideline: The clinical utility of bronchoalveolar lavage cellular analysis in interstitial lung disease. Am. J. Respir. Crit. Care Med. 2012, 185, 1004–1014. [Google Scholar] [CrossRef] [PubMed]
- Vasco-Mogorrón, M.A.; Campillo, J.A.; Periago, A.; Cabañas, V.; Berenguer, M.; García-Garay, M.C.; Gimeno, L.; Soto-Ramírez, M.F.; Martínez-Hernández, M.D.; Muro, M.; et al. Blood-based risk stratification for pre-malignant and symptomatic plasma cell neoplasms to improve patient management. Am. J. Cancer Res. 2021, 11, 2736–2753. [Google Scholar] [PubMed]
- Travis, W.D.; Costabel, U.; Hansell, D.M.; King, T.E., Jr.; Lynch, D.A.; Nicholson, A.G.; Ryerson, C.J.; Ryu, J.H.; Selman, M.; Wells, A.U.; et al. An official American Thoracic Society/European Respiratory Society statement: Update of the international multidisciplinary classification of the idiopathic interstitial pneumonias. Am. J. Respir. Crit. Care Med. 2013, 188, 733–748. [Google Scholar] [CrossRef] [PubMed]
- Bosch, L.v.D.; Luppi, F.; Ferrara, G.; Mura, M. Immunomodulatory treatment of interstitial lung disease. Ther. Adv. Respir. Dis. 2022, 16, 17534666221117002. [Google Scholar] [CrossRef]
- Novoa-Bolivar, E.M.; Ros, J.A.; Pérez-Fernández, S.; Campillo, J.A.; López-Hernández, R.; González-López, R.; Otalora-Alcaraz, A.; Ortuño-Hernández, C.; Gimeno, L.; Ruiz-Lorente, I.; et al. Neutrophils and Lymphocytes: Yin and Yang of Lung Fibrosis and Patient Outcome in Diffuse Interstitial Lung Diseases. Biomedicines 2024, 12, 2439. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Sánchez, M.V.; Fuster, J.L.; Campillo, J.A.; Galera, A.M.; Bermúdez-Cortés, M.; Llinares, M.E.; Ramos-Elbal, E.; Pascual-Gázquez, J.F.; Fita, A.M.; Martínez-Banaclocha, H.; et al. Expression of NK Cell Receptor Ligands on Leukemic Cells Is Associated with the Outcome of Childhood Acute Leukemia. Cancers 2021, 13, 2294. [Google Scholar] [CrossRef]
- Fujii, H.; Hara, Y.; Saigusa, Y.; Tagami, Y.; Murohashi, K.; Nagasawa, R.; Aoki, A.; Izawa, A.; Seki, K.; Watanabe, K.; et al. ILD-GAP Combined with the Charlson Comorbidity Index Score (ILD-GAPC) as a Prognostic Prediction Model in Patients with Interstitial Lung Disease. Can. Respir. J. 2023, 2023, 5088207. [Google Scholar] [CrossRef]
- Kanaoka, K.; Minami, S.; Ihara, S.; Komuta, K. High neutrophils and low lymphocytes percentages in bronchoalveolar lavage fluid are prognostic factors of higher in-hospital mortality in diffuse alveolar hemorrhage. BMC Pulm. Med. 2021, 21, 288. [Google Scholar] [CrossRef] [PubMed]
- D’Alessandro, M.; Bergantini, L.; Carleo, A.; Cameli, P.; Perrone, A.; Fossi, A.; Sestini, P.; Bargagli, E. Neutrophil-to-lymphocyte ratio in bronchoalveolar lavage from IPF patients: A novel prognostic biomarker? Minerva Med. 2022, 113, 526–531. [Google Scholar] [CrossRef]
- Ryu, W.K.; Moon, Y.; Park, M.H.; Lim, J.H.; Kim, Y.S.; Lee, K.-H.; Kwak, S.M.; Kim, C.; Nam, H.-S. A Preliminary Study on the Prognostic Impact of Neutrophil to Lymphocyte Ratio of the Bronchoalveolar Lavage Fluid in Patients with Lung Cancer. Diagnostics 2021, 11, 2201. [Google Scholar] [CrossRef]
- Crowley, L.E.; Stockley, R.A.; Thickett, D.R.; Dosanjh, D.; Scott, A.; Parekh, D. Neutrophil dynamics in pulmonary fibrosis: Pathophysiological and therapeutic perspectives. Eur. Respir. Rev. 2024, 33, 240139. [Google Scholar] [CrossRef] [PubMed]
- Achaiah, A.; Rathnapala, A.; Pereira, A.; Bothwell, H.; Dwivedi, K.; Barker, R.; Iotchkova, V.; Benamore, R.; Hoyles, R.K.; Ho, L.-P. Neutrophil lymphocyte ratio as an indicator for disease progression in Idiopathic Pulmonary Fibrosis. BMJ Open Respir. Res. 2022, 9, e001202. [Google Scholar] [CrossRef] [PubMed]
- Song, M.; Graubard, B.I.; Rabkin, C.S.; Engels, E.A. Neutrophil-to-lymphocyte ratio and mortality in the United States general population. Sci. Rep. 2021, 11, 464. [Google Scholar] [CrossRef]
- Lee, H.; Um, S.-J.; Kim, Y.S.; Kim, D.K.; Jang, A.S.; Choi, H.S.; Kim, Y.H.; Kim, T.E.; Yoo, K.H.; Jung, K.-S. Association of the Neutrophil-to-Lymphocyte Ratio with Lung Function and Exacerbations in Patients with Chronic Obstructive Pulmonary Disease. PLoS ONE 2016, 11, e0156511. [Google Scholar] [CrossRef]
- Pang, K.; Dong, S.; Zhu, Y.; Zhu, X.; Zhou, Q.; Gu, B.; Jin, W.; Zhang, R.; Fu, Y.; Yu, B.; et al. Advanced flow cytometry for biomedical applications. J. Biophotonics 2023, 16, e202300135. [Google Scholar] [CrossRef] [PubMed]
- Bratke, K.; Weise, M.; Stoll, P.; Virchow, J.C.; Lommatzsch, M. Flow Cytometry as an Alternative to Microscopy for the Differentiation of BAL Fluid Leukocytes. Chest 2024, 166, 793–801. [Google Scholar] [CrossRef]
- Inomata, T.; Konno, S.; Nagai, K.; Suzuki, M.; Nishimura, M. Neutrophil predominance in bronchoalveolar lavage fluid is associated with disease severity and progression of HRCT findings in pulmonary Mycobacterium avium infection. PLoS ONE 2018, 13, e0190189. [Google Scholar] [CrossRef]
- Collins, B.F.; Raghu, G. Antifibrotic therapy for fibrotic lung disease beyond idiopathic pulmonary fibrosis. Eur. Respir. Rev. 2019, 28, 190022. [Google Scholar] [CrossRef] [PubMed]
- Maher, T.M.; Strek, M.E. Antifibrotic therapy for idiopathic pulmonary fibrosis: Time to treat. Respir. Res. 2019, 20, 205. [Google Scholar] [CrossRef] [PubMed]
- Finnerty, J.P.; Ponnuswamy, A.; Dutta, P.; Abdelaziz, A.; Kamil, H. Efficacy of antifibrotic drugs, nintedanib and pirfenidone, in treatment of progressive pulmonary fibrosis in both idiopathic pulmonary fibrosis (IPF) and non-IPF: A systematic review and meta-analysis. BMC Pulm. Med. 2021, 21, 411. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patients | Sex | Age | Fibrosis 1 | Treatments (%) 2 | |||
|---|---|---|---|---|---|---|---|
| (N) | (% man) | (Mean ± SD) | (%) | NT | SC | Other | |
| Control groups | 355 | 53.2% | 61.2 ± 13.5 | - | |||
| General population 3 | 243 | 53.1% | 67.9 ± 12.3 | - | |||
| BAL control 4 | 112 | 53.3% | 53.5 ± 16.6 | 0% | |||
| Interstitial lung diseases (ILD) | 731 | 58.1% | 58.7 ± 16.4 | 38.2% | 32 | 32 | 18 |
| Sarcoidosis | 82 | 48.20% | 55.6 ± 14.8 | 19.5% | 34 | 38 | 15 |
| Hypersensitivity pneumonitis (HP) | 48 | 49.0% | 50.4 ± 17.6 | 29.1% | 13 | 46 | 13 |
| Organized cryptogenic pneumonia (COP) | 44 | 46.50% | 62.3 ± 17.4 | 18.1% | 18 | 52 | 21 |
| Lymphocytic interstitial pneumonia (LIP) | 37 | 69.20% | 53.2 ± 15.9 | 8.1% | 49 | 24 | 16 |
| Usual interstitial pneumonia (UIP) 5 | 145 | 71.70% | 65.8 ± 12.3 | 100% | 25 | 35 | 19 |
| Respiratory bronchiolitis ILD (RB-ILD) | 25 | 40.0% | 53.3 ± 22.8 | 8.0% | 36 | 36 | 8 |
| Desquamative interstitial pneumonitis (DIP) | 35 | 52.8% | 54.4 ± 20.8 | 5.7% | 46 | 23 | 17 |
| Nonspecific interstitial pneumonia (NSIP) | 156 | 48.1% | 59.3 ± 15.5 | 33.9% | 31 | 28 | 30 |
| Pneumoconiosis | 27 | 96.3% | 56.5 ± 16.0 | 18.5% | 42 | 23 | 4 |
| Pulmonary Langerhans cell histiocytosis (PLCH) | 9 | 66.7% | 36.7 ± 15.8 | 11.1% | 67 | 11 | 11 |
| Eosinophilic-ILD | 17 | 80.0% | 48.4 ± 22.7 | 5.9% | 0 | 76 | 6 |
| Unclassifiable-ILD (U-ILD) | 80 | 60.0% | 61.3 ± 12.4 | 25.0% | 49 | 15 | 10 |
| Acute interstitial pneumonia (AIP) | 26 | 56.0% | 57.5 ± 21.9 | 15.3% | 29 | 24 | 12 |
| Pulmonary infectious diseases | 231 | 59.0% | 62.1 ± 15.6 | 15.1% | 27 | 22 | 18 |
| BAL Control | ILD Without Fibrosis | ILD with Fibrosis | IPF | Infectious Diseases | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| (n = 112) | (n = 452) | (n = 279) | (n = 145) | (n = 231) | ||||||
| % | Cels/µL | % | Cels/µL | % | Cels/µL | % | Cels/µL | % | Cels/µL | |
| Lymphocytes | 6.3 ± 0.6 | 6.9 ± 0.7 | 22.4 ± 1.0 * | 24 ± 1.2 * | 20.8 ± 1.6 * | 22.7 ± 2.0 * | 10.5 ± 1.2 * | 11.1 ± 1.4 * | 13 ± 1.1 * | 14.6 ± 1.3 * |
| Macrophages | 89.8 ± 0.7 | 98.2 ± 4.6 | 65.9 ± 1.1 * | 70.1 ± 1.5 * | 67.1 ± 1.8 * | 72.9 ± 3.2 * | 69.1 ± 1.8 * | 71.8 ± 2.8 * | 37.9 ± 1.5 * | 44.5 ± 2.6 * |
| Neutrophils | 2.1 ± 0.2 | 2.5 ± 0.4 | 7.7 ± 0.5 * | 8.8 ± 1.0 * | 8.5 ± 0.8 * | 11.1 ± 2.4 * | 16.9 ± 1.5 * | 18.2 ± 1.8 * | 46.0 ± 1.8 * | 62.7 ± 7.1 * |
| Eosinophils | 0.4 ± 0.1 | 0.5 ± 0.2 | 1.6 ± 0.3 | 1.6 ± 0.3 | 1.3 ± 0.2 | 1.6 ± 0.4 | 1.1 ± 0.2 | 1.1 ± 0.2 | 0.9 ± 0.1 | 1.1 ± 0.2 |
| CD1a + D.C. | 0.5 ± 0.1 | 0.6 ± 0.1 | 0.7 ± 0.1 | 0.7 ± 0.1 | 0.7 ± 0.1 | 0.8 ± 0.1 | 0.9 ± 0.1 | 1.1 ± 0.1 | 0.5 ± 0.1 | 0.7 ± 0.1 |
| CD4 + Lymphs | 2.8 ± 0.3 | 3.0 ± 0.4 | 10.8 ± 0.6 | 11.5 ± 0.7 | 10.4 ± 1.0 | 11.0 ± 1.1 | 5.6 ± 0.8 | 5.9 ± 0.9 | 6.3 ± 0.7 | 7.1 ± 0.8 |
| CD8 + Lymphs | 2.5 ± 0.3 | 2.7 ± 0.3 | 8.8 ± 0.5 | 9.5 ± 0.7 | 7.7 ± 0.9 | 8.6 ± 1.1 | 3.5 ± 0.4 | 3.8 ± 0.6 | 4.7 ± 0.5 | 5.3 ± 0.6 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Novoa-Bolivar, E.M.; Ros, J.A.; Pérez-Fernández, S.; Campillo, J.A.; López-Hernández, R.; González-López, R.; Otálora-Alcaraz, A.; Ortuño-Hernández, C.; Gimeno, L.; Ruiz-Lorente, I.; et al. Predictive Value of Flow Cytometry Quantification of BAL Lymphocytes and Neutrophils in ILD. Cells 2024, 13, 2066. https://doi.org/10.3390/cells13242066
Novoa-Bolivar EM, Ros JA, Pérez-Fernández S, Campillo JA, López-Hernández R, González-López R, Otálora-Alcaraz A, Ortuño-Hernández C, Gimeno L, Ruiz-Lorente I, et al. Predictive Value of Flow Cytometry Quantification of BAL Lymphocytes and Neutrophils in ILD. Cells. 2024; 13(24):2066. https://doi.org/10.3390/cells13242066
Chicago/Turabian StyleNovoa-Bolivar, Erika M., José A. Ros, Sonia Pérez-Fernández, José A. Campillo, Ruth López-Hernández, Rosana González-López, Almudena Otálora-Alcaraz, Cristina Ortuño-Hernández, Lourdes Gimeno, Inmaculada Ruiz-Lorente, and et al. 2024. "Predictive Value of Flow Cytometry Quantification of BAL Lymphocytes and Neutrophils in ILD" Cells 13, no. 24: 2066. https://doi.org/10.3390/cells13242066
APA StyleNovoa-Bolivar, E. M., Ros, J. A., Pérez-Fernández, S., Campillo, J. A., López-Hernández, R., González-López, R., Otálora-Alcaraz, A., Ortuño-Hernández, C., Gimeno, L., Ruiz-Lorente, I., Ceballos-Francisco, D., Muro, M., Solana, E., Martinez-Camblor, P., & Minguela, A. (2024). Predictive Value of Flow Cytometry Quantification of BAL Lymphocytes and Neutrophils in ILD. Cells, 13(24), 2066. https://doi.org/10.3390/cells13242066