
The Potential of Mesenchymal Stem/Stromal Cell Therapy in Mustard Keratopathy: Discovering New Roads to Combat Cellular Senescence

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Preparation of hBM-MSCs
2.2. Immunophenotyping of MSCs
2.3. NM Preparation
2.4. Animals
2.5. Study Arms
2.6. NM Exposure and MSC Injection
2.7. Clinical Assessments
2.8. Histopathological Assessments
2.9. Statistical Analysis
3. Results
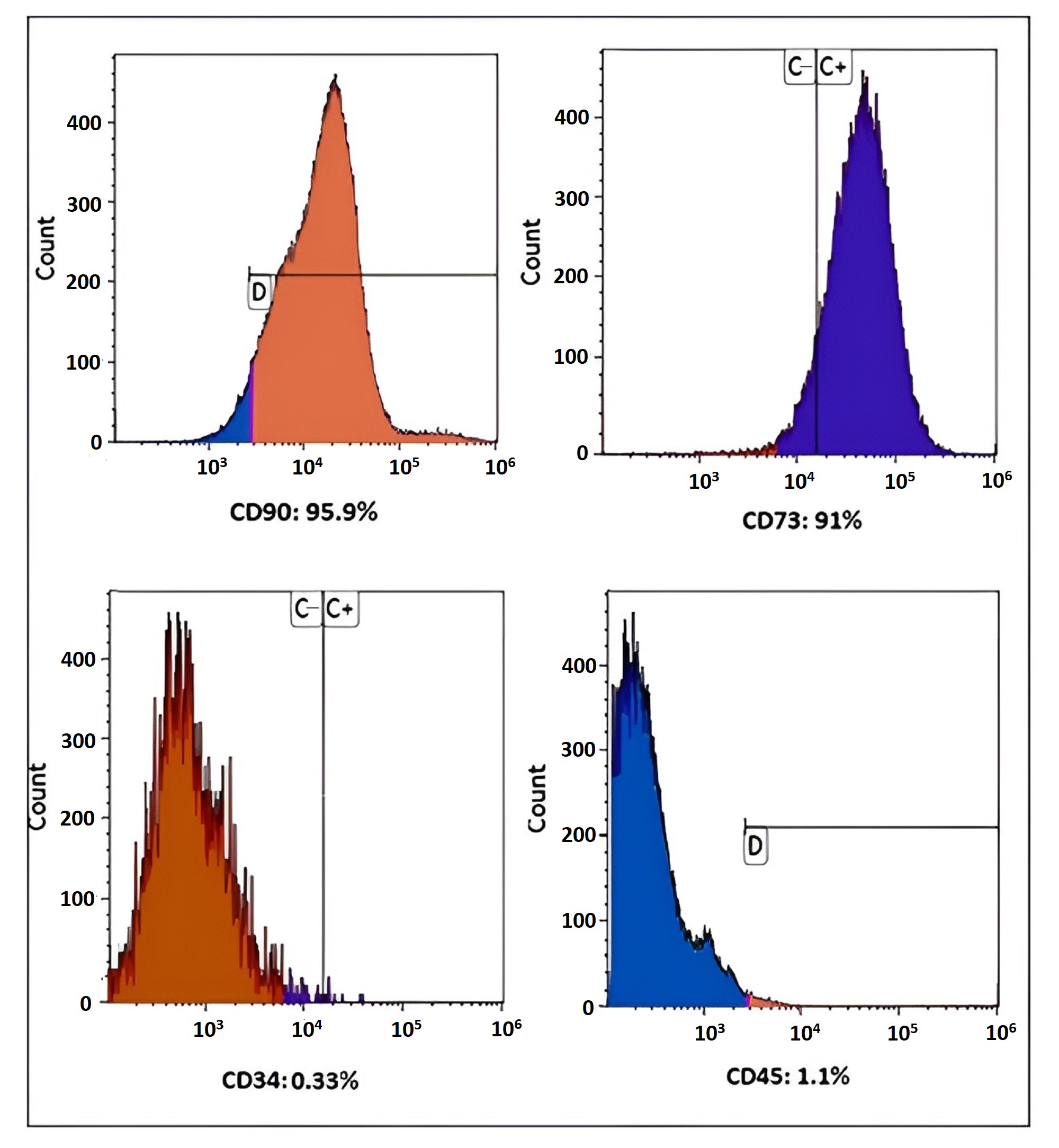
3.1. Immunophenotyping of MSCs
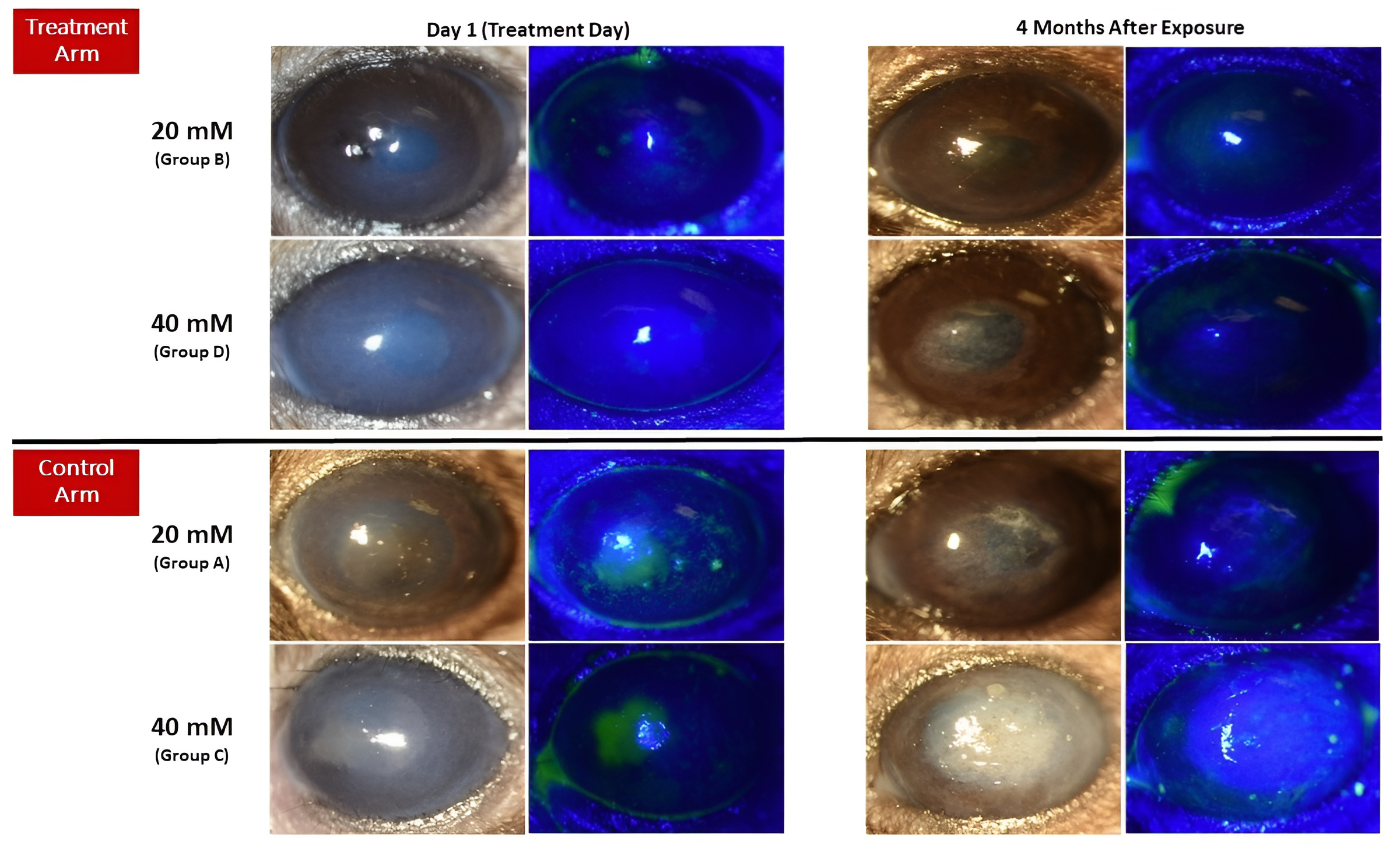
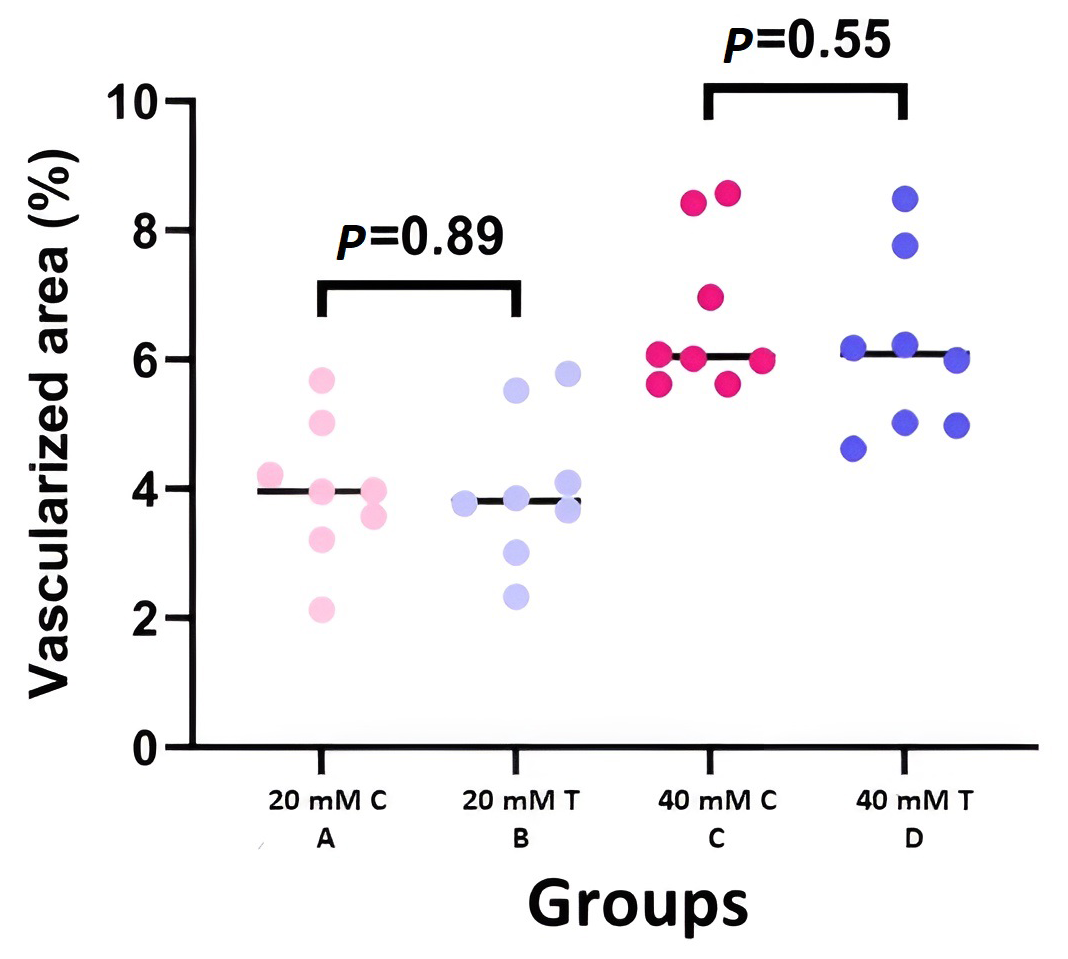
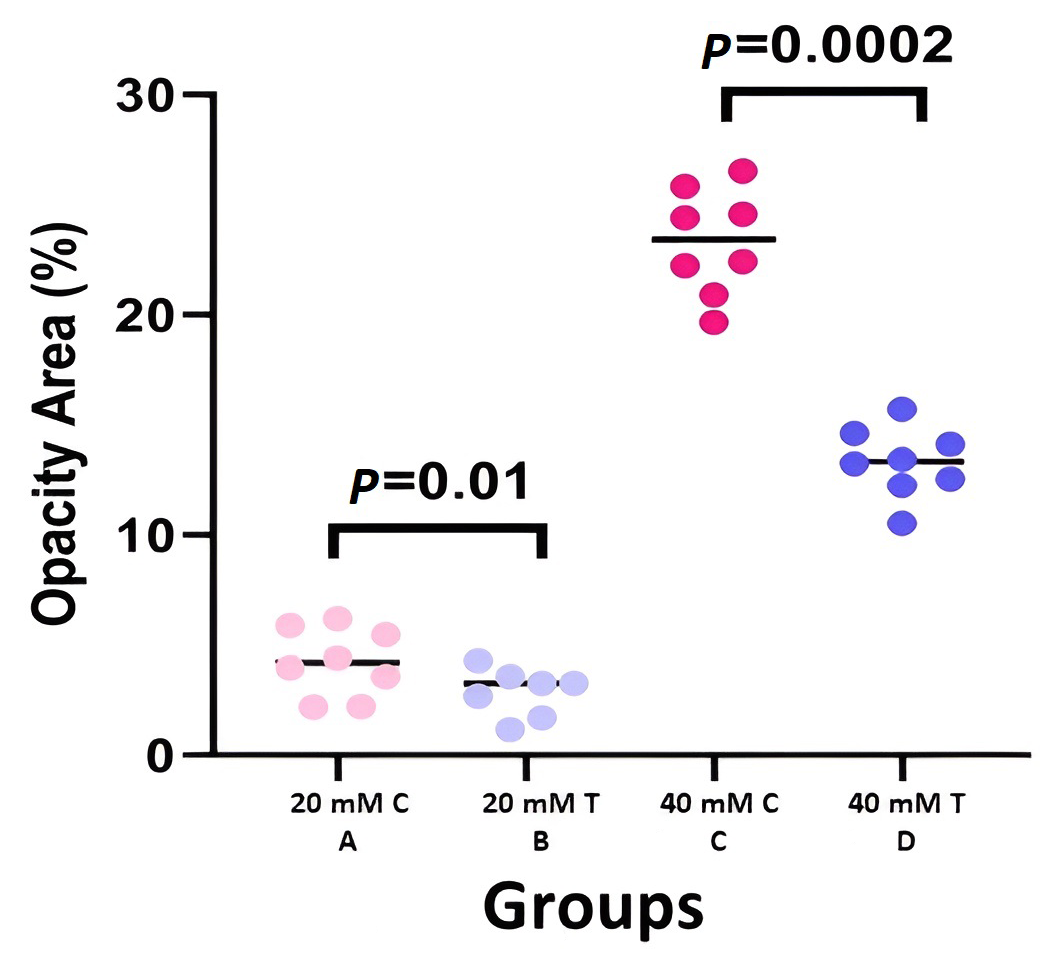
3.2. Clinical Results
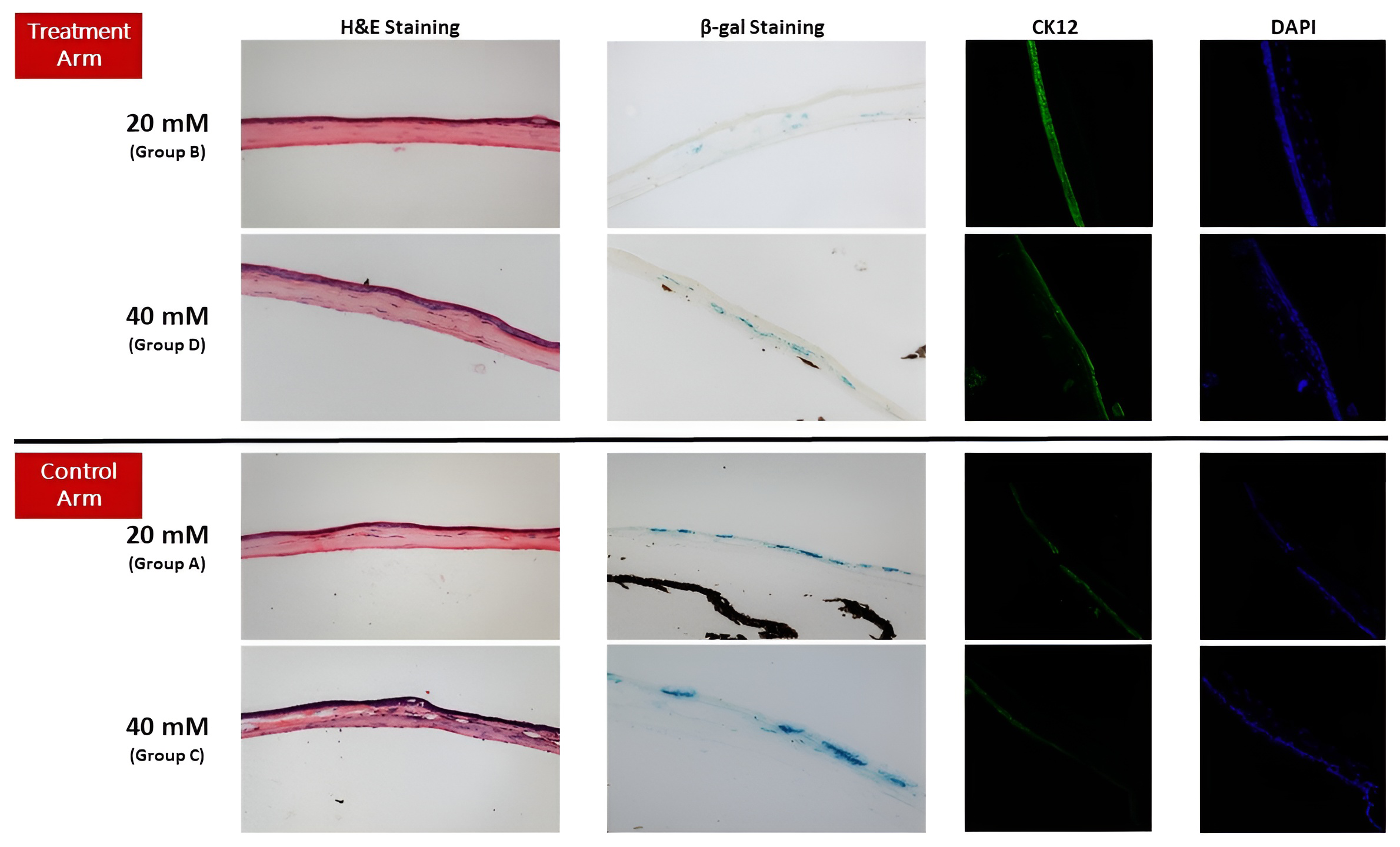
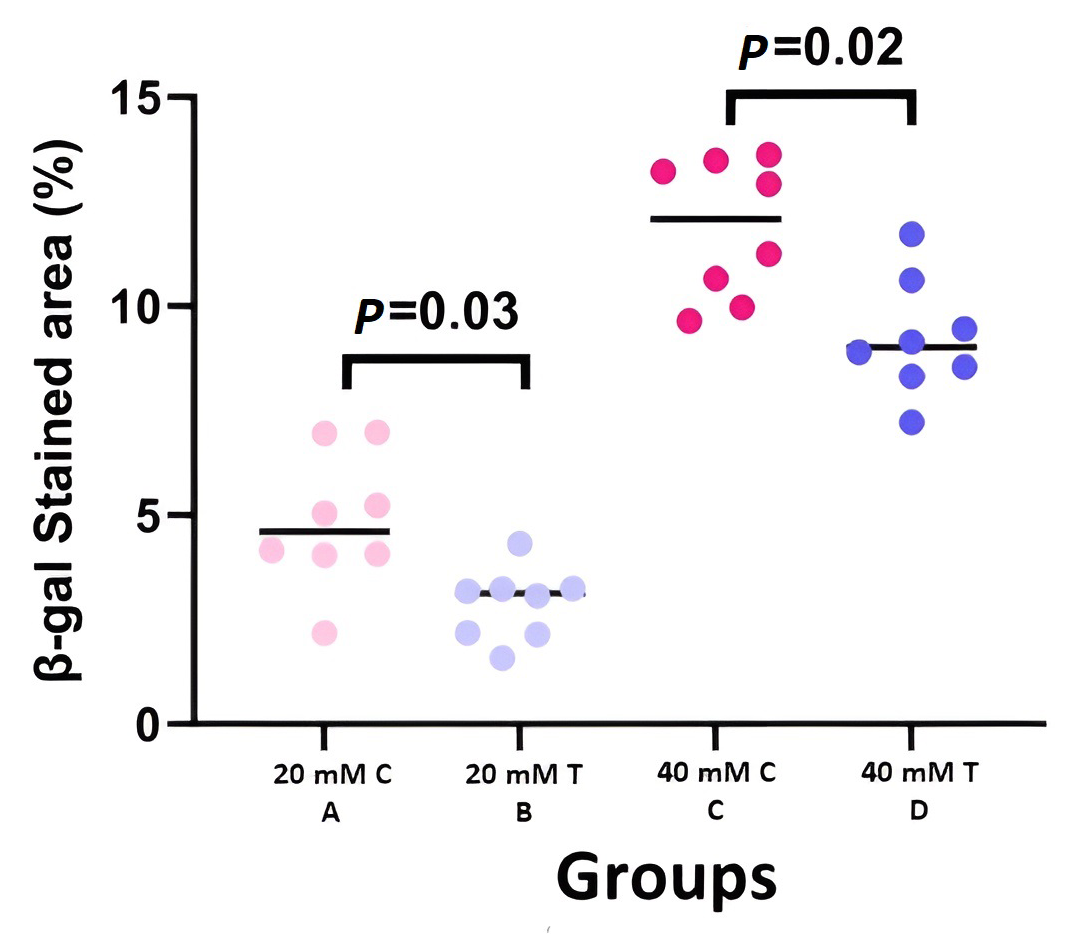
3.3. Histopathological Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Goswami, D.G.; Tewari-Singh, N.; Dhar, D.; Kumar, D.; Agarwal, C.; Ammar, D.A.; Kant, R.; Enzenauer, R.W.; Petrash, J.M.; Agarwal, R. Nitrogen mustard-induced corneal injury involves DNA damage and pathways related to inflammation, epithelial-stromal separation and neovascularization. Cornea 2016, 35, 257. [Google Scholar] [CrossRef]
- Ming, X.; Michaelson-Richie, E.D.; Groehler IV, A.S.; Villalta, P.W.; Campbell, C.; Tretyakova, N.Y. Cross-linking of the DNA repair protein O6-alkylguanine DNA alkyltransferase to DNA in the presence of cisplatin. DNA Repair 2020, 89, 102840. [Google Scholar] [CrossRef] [PubMed]
- Jan, Y.-H.; Heck, D.E.; Laskin, D.L.; Laskin, J.D. DNA damage signaling in the cellular responses to mustard vesicants. Toxicol. Lett. 2020, 326, 78–82. [Google Scholar] [CrossRef] [PubMed]
- Soleimani, M.; Baharnoori, S.M.; Cheraqpour, K.; Momenaei, B.; Mirshahi, R.; Chow, C.; Shahjahan, S.; Nguyen, T.; Ashraf, M.J.; Huang, X. Cellular senescence implication in mustard keratopathy. Exp. Eye Res. 2023, 233, 109565. [Google Scholar] [CrossRef] [PubMed]
- Kadar, T.; Dachir, S.; Cohen, L.; Sahar, R.; Fishbine, E.; Cohen, M.; Turetz, J.; Gutman, H.; Buch, H.; Brandeis, R. Ocular injuries following sulfur mustard exposure—Pathological mechanism and potential therapy. Toxicology 2009, 263, 59–69. [Google Scholar] [CrossRef]
- Charkoftaki, G.; Jester, J.V.; Thompson, D.C.; Vasiliou, V. Nitrogen mustard-induced corneal injury involves the sphingomyelin-ceramide pathway. Ocul. Surf. 2018, 16, 154–162. [Google Scholar] [CrossRef]
- Naderi, M.; Jadidi, K.; Falahati, F.; Alavi, S.A. The effect of sulfur mustard and nitrogen mustard on corneal collagen degradation induced by the enzyme collagenase. Cutan. Ocul. Toxicol. 2010, 29, 234–240. [Google Scholar] [CrossRef]
- Tewari-Singh, N.; Rana, S.; Gu, M.; Pal, A.; Orlicky, D.J.; White, C.W.; Agarwal, R. Inflammatory Biomarkers of Sulfur Mustard Analog 2-Chloroethyl Ethyl Sulfide–Induced Skin Injury in SKH-1 Hairless Mice. Toxicol. Sci. 2009, 108, 194–206. [Google Scholar] [CrossRef]
- Tewari-Singh, N.; Jain, A.K.; Inturi, S.; Ammar, D.A.; Agarwal, C.; Tyagi, P.; Kompella, U.B.; Enzenauer, R.W.; Petrash, J.M.; Agarwal, R. Silibinin, dexamethasone, and doxycycline as potential therapeutic agents for treating vesicant-inflicted ocular injuries. Toxicol. Appl. Pharmacol. 2012, 264, 23–31. [Google Scholar] [CrossRef]
- Kaluzhny, Y.; Kinuthia, M.W.; Lapointe, A.M.; Truong, T.; Klausner, M.; Hayden, P. Oxidative stress in corneal injuries of different origin: Utilization of 3D human corneal epithelial tissue model. Exp. Eye Res. 2020, 190, 107867. [Google Scholar] [CrossRef]
- Laskin, J.D.; Black, A.T.; Jan, Y.H.; Sinko, P.J.; Heindel, N.D.; Sunil, V.; Heck, D.E.; Laskin, D.L. Oxidants and antioxidants in sulfur mustard–induced injury. Ann. N. Y. Acad. Sci. 2010, 1203, 92–100. [Google Scholar] [CrossRef]
- Gu, S.; Xing, C.; Han, J.; Tso, M.O.; Hong, J. Differentiation of rabbit bone marrow mesenchymal stem cells into corneal epithelial cells in vivo and ex vivo. Mol. Vis. 2009, 15, 99. [Google Scholar]
- Nieto-Nicolau, N.; Martín-Antonio, B.; Müller-Sánchez, C.; Casaroli-Marano, R.P. In vitro potential of human mesenchymal stem cells for corneal epithelial regeneration. Regen. Med. 2020, 15, 1409–1426. [Google Scholar] [CrossRef] [PubMed]
- Stanko, P.; Kaiserova, K.; Altanerova, V.; Altaner, C. Comparison of human mesenchymal stem cells derived from dental pulp, bone marrow, adipose tissue, and umbilical cord tissue by gene expression. Biomed. Pap. Med. Fac. Univ. Palacky Olomouc Czech Repub. 2014, 158, 373–377. [Google Scholar] [CrossRef] [PubMed]
- Oh, J.Y.; Kim, M.K.; Shin, M.S.; Lee, H.J.; Ko, J.H.; Wee, W.R.; Lee, J.H. The anti-inflammatory and anti-angiogenic role of mesenchymal stem cells in corneal wound healing following chemical injury. Stem Cells 2008, 26, 1047–1055. [Google Scholar] [CrossRef] [PubMed]
- Hoogduijn, M.J.; Popp, F.; Verbeek, R.; Masoodi, M.; Nicolaou, A.; Baan, C.; Dahlke, M.-H. The immunomodulatory properties of mesenchymal stem cells and their use for immunotherapy. Int. Immunopharmacol. 2010, 10, 1496–1500. [Google Scholar] [CrossRef]
- Motegi, S.-I.; Sekiguchi, A.; Uchiyama, A.; Uehara, A.; Fujiwara, C.; Yamazaki, S.; Perera, B.; Nakamura, H.; Ogino, S.; Yokoyama, Y. Protective effect of mesenchymal stem cells on the pressure ulcer formation by the regulation of oxidative and endoplasmic reticulum stress. Sci. Rep. 2017, 7, 17186. [Google Scholar] [CrossRef]
- Tavakkoli, F.; Eleiwa, T.K.; Elhusseiny, A.M.; Damala, M.; Rai, A.K.; Cheraqpour, K.; Ansari, M.H.; Doroudian, M.; Keshel, S.H.; Soleimani, M. Corneal stem cells niche and homeostasis impacts in regenerative medicine; concise review. Eur. J. Ophthalmol. 2023, 33, 11206721221150065. [Google Scholar] [CrossRef] [PubMed]
- Soleimani, M.; Cheraqpour, K.; Koganti, R.; Baharnoori, S.M.; Djalilian, A.R. Concise Review: Bioengineering of Limbal Stem Cell Niche. Bioengineering 2023, 10, 111. [Google Scholar] [CrossRef]
- Soleimani, M.; Cheraqpour, K.; Koganti, R.; Djalilian, A.R. Cellular senescence and ophthalmic diseases: Narrative review. Graefe’s Arch. Clin. Exp. Ophthalmol. 2023, 261, 3067–3082. [Google Scholar] [CrossRef]
- Navas, A.; Magaña-Guerrero, F.S.; Domínguez-López, A.; Chávez-García, C.; Partido, G.; Graue-Hernández, E.O.; Sánchez-García, F.J.; Garfias, Y. Anti-inflammatory and anti-fibrotic effects of human amniotic membrane mesenchymal stem cells and their potential in corneal repair. Stem Cells Transl. Med. 2018, 7, 906–917. [Google Scholar] [CrossRef]
- Jabbehdari, S.; Yazdanpanah, G.; Kanu, L.N.; Chen, E.; Kang, K.; Anwar, K.N.; Ghassemi, M.; Hematti, P.; Rosenblatt, M.I.; Djalilian, A.R. Therapeutic effects of lyophilized conditioned-medium derived from corneal mesenchymal stromal cells on corneal epithelial wound healing. Curr. Eye Res. 2020, 45, 1490–1496. [Google Scholar] [CrossRef] [PubMed]
- Soleimani, M.; Masoumi, A.; Momenaei, B.; Cheraqpour, K.; Koganti, R.; Chang, A.Y.; Ghassemi, M.; Djalilian, A.R. Applications of mesenchymal stem cells in ocular surface diseases: Sources and routes of delivery. Expert Opin. Biol. Ther. 2023, 23, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Jiang, T.-S.; Cai, L.; Ji, W.-Y.; Hui, Y.-N.; Wang, Y.-S.; Hu, D.; Zhu, J. Reconstruction of the corneal epithelium with induced marrow mesenchymal stem cells in rats. Mol. Vis. 2010, 16, 1304. [Google Scholar] [PubMed]
- Margolis, M.; Jung, R.; Tu, G.; An, S.; Dana, R.; Jeng, B.H.; Basu, S.; Rosenblatt, M.; Hematti, P.; Mahmud, N. Phase I Study of the Safety of Locally Delivered Allogeneic Mesenchymal Stem Cells for Promoting Corneal Repair: Early Results. Investig. Ophthalmol. Vis. Sci. 2022, 63, 91-A0189. [Google Scholar]
- Ma, Y.; Xu, Y.; Xiao, Z.; Yang, W.; Zhang, C.; Song, E.; Du, Y.; Li, L. Reconstruction of chemically burned rat corneal surface by bone marrow–derived human mesenchymal stem cells. Stem Cells 2006, 24, 315–321. [Google Scholar] [CrossRef]
- Soleimani, M.; Mirshahi, R.; Cheraqpour, K.; Baharnoori, S.M.; Massoumi, H.; Chow, C.; Shahjahan, S.; Momenaei, B.; Ashraf, M.J.; Koganti, R. Intrastromal versus subconjunctival injection of mesenchymal stem/stromal cells for promoting corneal repair. Ocul. Surf. 2023, 30, 187–195. [Google Scholar] [CrossRef]
- Goswami, D.G.; Kumar, D.; Tewari-Singh, N.; Orlicky, D.J.; Jain, A.K.; Kant, R.; Rancourt, R.C.; Dhar, D.; Inturi, S.; Agarwal, C. Topical nitrogen mustard exposure causes systemic toxic effects in mice. Exp. Toxicol. Pathol. 2015, 67, 161–170. [Google Scholar] [CrossRef]
- Soleimani, M.; Momenaei, B.; Baradaran-Rafii, A.; Cheraqpour, K.; An, S.; Ashraf, M.J.; Abedi, F.; Javadi, M.A.; Djalilian, A.R. Mustard Gas–Induced Ocular Surface Disorders: An Update on the Pathogenesis, Clinical Manifestations, and Management. Cornea 2022, 42, 10–1097. [Google Scholar] [CrossRef]
- Shay, J.W.; Wright, W.E. Hayflick, his limit, and cellular ageing. Nat. Rev. Mol. Cell Biol. 2000, 1, 72–76. [Google Scholar] [CrossRef]
- Papaconstantinou, J. The role of signaling pathways of inflammation and oxidative stress in development of senescence and aging phenotypes in cardiovascular disease. Cells 2019, 8, 1383. [Google Scholar] [CrossRef]
- Abate, M.; Festa, A.; Falco, M.; Lombardi, A.; Luce, A.; Grimaldi, A.; Zappavigna, S.; Sperlongano, P.; Irace, C.; Caraglia, M. Mitochondria as playmakers of apoptosis, autophagy and senescence. In Seminars in Cell & Developmental Biology; Elsevier: Amsterdam, The Netherlands, 2020; pp. 139–153. [Google Scholar]
- Wang, X.; Qu, M.; Li, J.; Danielson, P.; Yang, L.; Zhou, Q. Induction of fibroblast senescence during mouse corneal wound healing. Investig. Ophthalmol. Vis. Sci. 2019, 60, 3669–3679. [Google Scholar] [CrossRef] [PubMed]
- Younis, L.T.; Hassan, M.I.; Ali, T.B.; Bustami, T.J. 3D TECA hydrogel reduces cellular senescence and enhances fibroblasts migration in wound healing. Asian J. Pharm. Sci. 2018, 13, 317–325. [Google Scholar] [CrossRef] [PubMed]
- Shukla, S.; Mittal, S.K.; Foulsham, W.; Elbasiony, E.; Singhania, D.; Sahu, S.K.; Chauhan, S.K. Therapeutic efficacy of different routes of mesenchymal stem cell administration in corneal injury. Ocul. Surf. 2019, 17, 729–736. [Google Scholar] [CrossRef]
- Kean, T.J.; Lin, P.; Caplan, A.I.; Dennis, J.E. MSCs: Delivery routes and engraftment, cell-targeting strategies, and immune modulation. Stem Cells Int. 2013, 2013, 732742. [Google Scholar] [CrossRef] [PubMed]
- Zhang, M.; Liu, D.; Li, S.; Chang, L.; Zhang, Y.; Liu, R.; Sun, F.; Duan, W.; Du, W.; Wu, Y.; et al. Bone marrow mesenchymal stem cell transplantation retards the natural senescence of rat hearts. Stem Cells Transl. Med. 2015, 4, 494–502. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, C.E.; Capcha, J.M.; de Bragança, A.C.; Sanches, T.R.; Gouveia, P.Q.; de Oliveira, P.A.; Malheiros, D.M.; Volpini, R.A.; Santinho, M.A.; Santana, B.A.; et al. Human umbilical cord-derived mesenchymal stromal cells protect against premature renal senescence resulting from oxidative stress in rats with acute kidney injury. Stem Cell Res. Ther. 2017, 8, 19. [Google Scholar] [CrossRef]
- Xiao, X.; Xu, M.; Yu, H.; Wang, L.; Li, X.; Rak, J.; Wang, S.; Zhao, R.C. Mesenchymal stem cell-derived small extracellular vesicles mitigate oxidative stress-induced senescence in endothelial cells via regulation of miR-146a/Src. Signal Transduct. Target. Ther. 2021, 6, 354. [Google Scholar] [CrossRef]
- Zhang, L.; Zhu, X.Y.; Zhao, Y.; Eirin, A.; Liu, L.; Ferguson, C.M.; Tang, H.; Lerman, A.; Lerman, L.O. Selective intrarenal delivery of mesenchymal stem cell-derived extracellular vesicles attenuates myocardial injury in experimental metabolic renovascular disease. Basic Res. Cardiol. 2020, 115, 16. [Google Scholar] [CrossRef]
- Huang, W.; Hickson, L.J.; Eirin, A.; Kirkland, J.L.; Lerman, L.O. Cellular senescence: The good, the bad and the unknown. Nat. Rev. Nephrol. 2022, 18, 611–627. [Google Scholar] [CrossRef]
- An, S.; Shen, X.; Anwar, K.; Ashraf, M.; Lee, H.; Koganti, R.; Ghassemi, M.; Djalilian, A.R. Therapeutic potential of mesenchymal stem cell-secreted factors on delay in corneal wound healing by nitrogen mustard. Int. J. Mol. Sci. 2022, 23, 11510. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Control Arm | Treatment Arm | |||
|---|---|---|---|---|
| 20 mM | 40 mM | 20 mM | 40 mM | |
| Grade 0 | 0 | 0 | 0 | 0 |
| Grade 1 | 1 | 0 | 4 | 1 |
| Grade 2 | 6 | 4 | 4 | 6 |
| Grade 3 | 1 | 4 | 0 | 1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Soleimani, M.; Mirzaei, A.; Cheraqpour, K.; Baharnoori, S.M.; Arabpour, Z.; Ashraf, M.J.; Ghassemi, M.; Djalilian, A.R. The Potential of Mesenchymal Stem/Stromal Cell Therapy in Mustard Keratopathy: Discovering New Roads to Combat Cellular Senescence. Cells 2023, 12, 2744. https://doi.org/10.3390/cells12232744
Soleimani M, Mirzaei A, Cheraqpour K, Baharnoori SM, Arabpour Z, Ashraf MJ, Ghassemi M, Djalilian AR. The Potential of Mesenchymal Stem/Stromal Cell Therapy in Mustard Keratopathy: Discovering New Roads to Combat Cellular Senescence. Cells. 2023; 12(23):2744. https://doi.org/10.3390/cells12232744
Chicago/Turabian StyleSoleimani, Mohammad, Arash Mirzaei, Kasra Cheraqpour, Seyed Mahbod Baharnoori, Zohreh Arabpour, Mohammad Javad Ashraf, Mahmood Ghassemi, and Ali R. Djalilian. 2023. "The Potential of Mesenchymal Stem/Stromal Cell Therapy in Mustard Keratopathy: Discovering New Roads to Combat Cellular Senescence" Cells 12, no. 23: 2744. https://doi.org/10.3390/cells12232744
APA StyleSoleimani, M., Mirzaei, A., Cheraqpour, K., Baharnoori, S. M., Arabpour, Z., Ashraf, M. J., Ghassemi, M., & Djalilian, A. R. (2023). The Potential of Mesenchymal Stem/Stromal Cell Therapy in Mustard Keratopathy: Discovering New Roads to Combat Cellular Senescence. Cells, 12(23), 2744. https://doi.org/10.3390/cells12232744