
Findings and Graduation of Sarcoidosis-Related Uveitis: A Single-Center Study



Abstract
:
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Ocular Classification
2.3. Statistical Analysis
3. Results
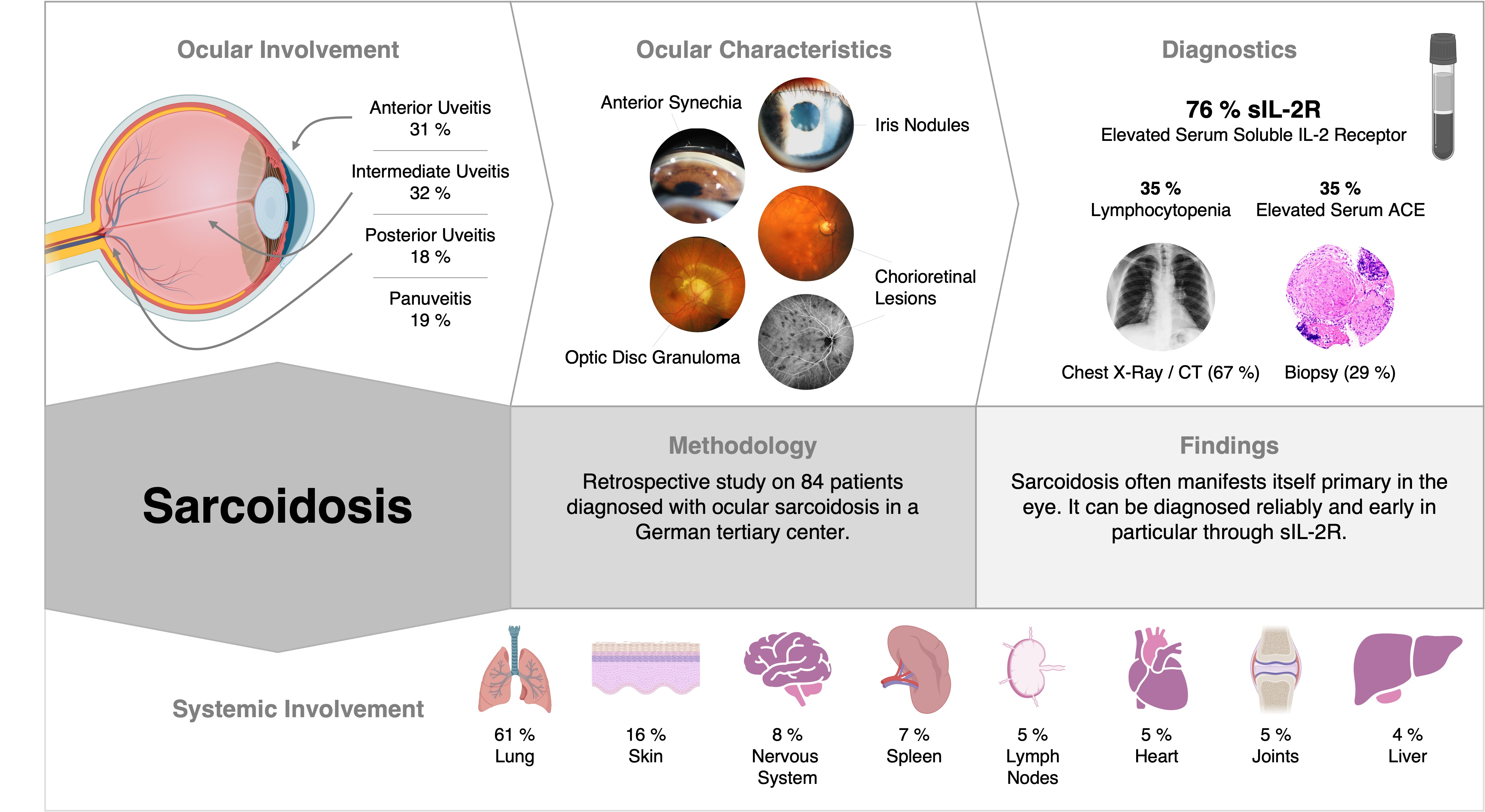
3.1. Clinical Manifestation
3.1.1. Patient Characteristics
3.1.2. Systemic Involvement
3.2. Ocular Findings
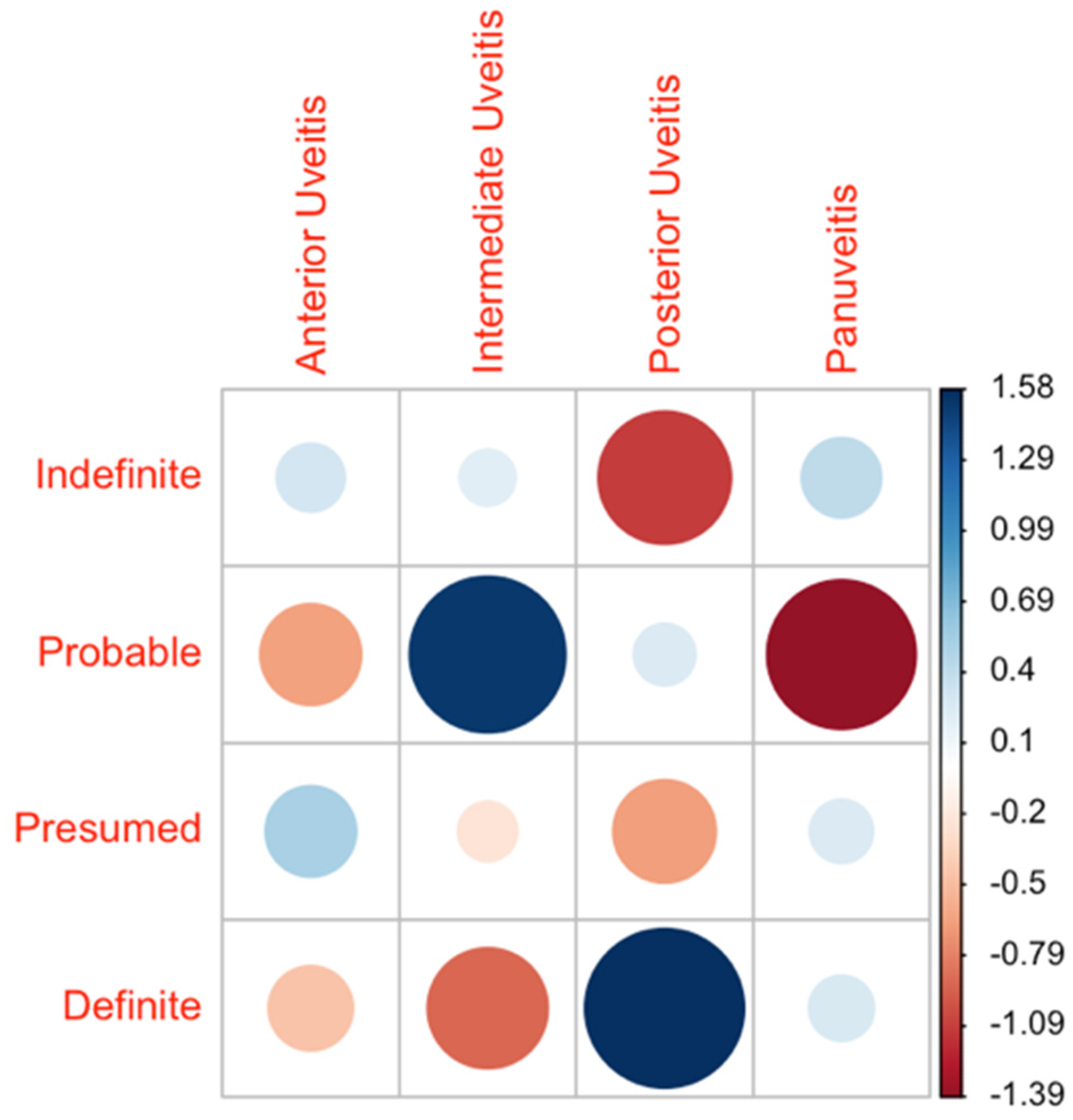
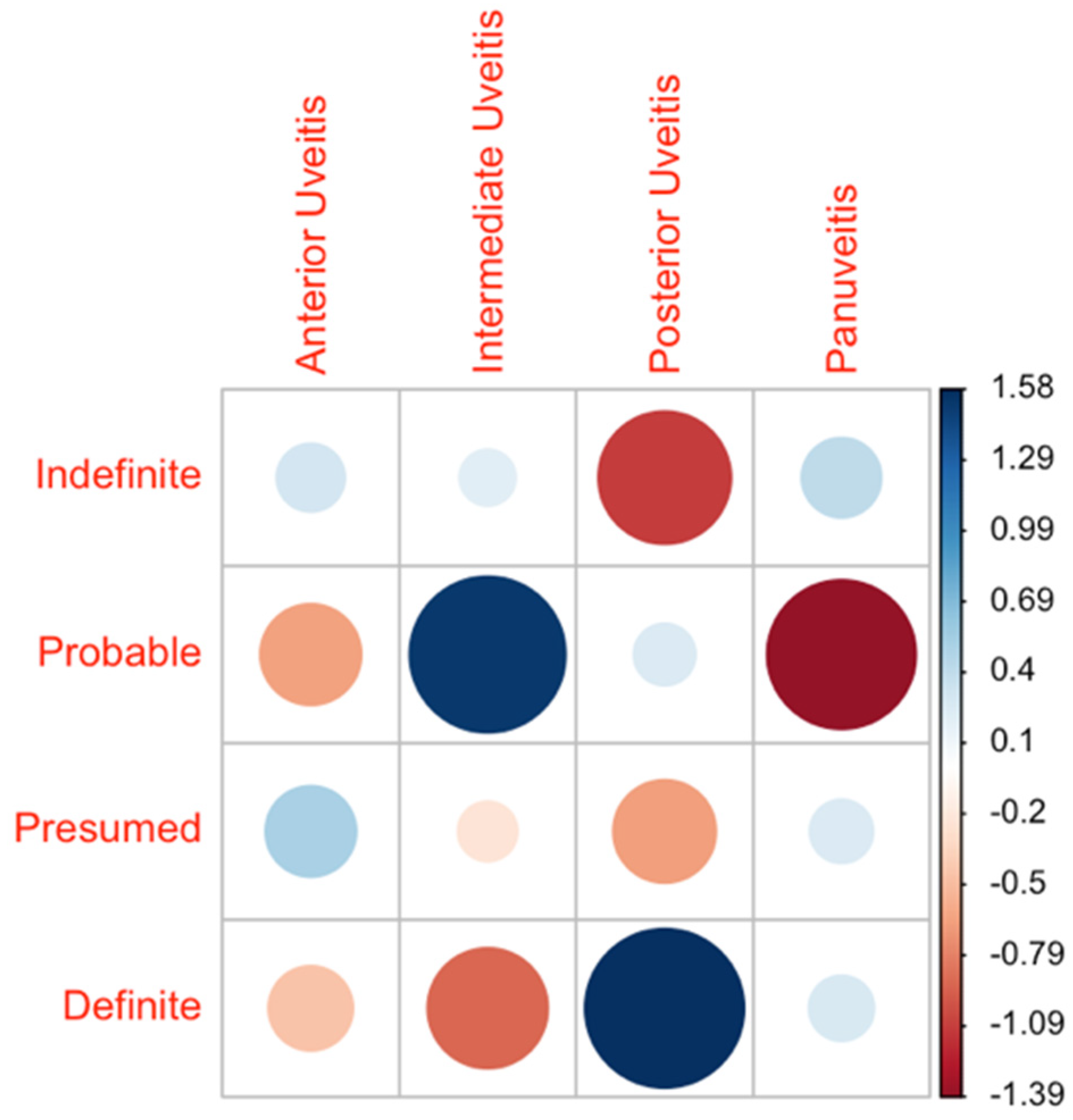
3.2.1. IWOS Classification and Uveitis Subtypes
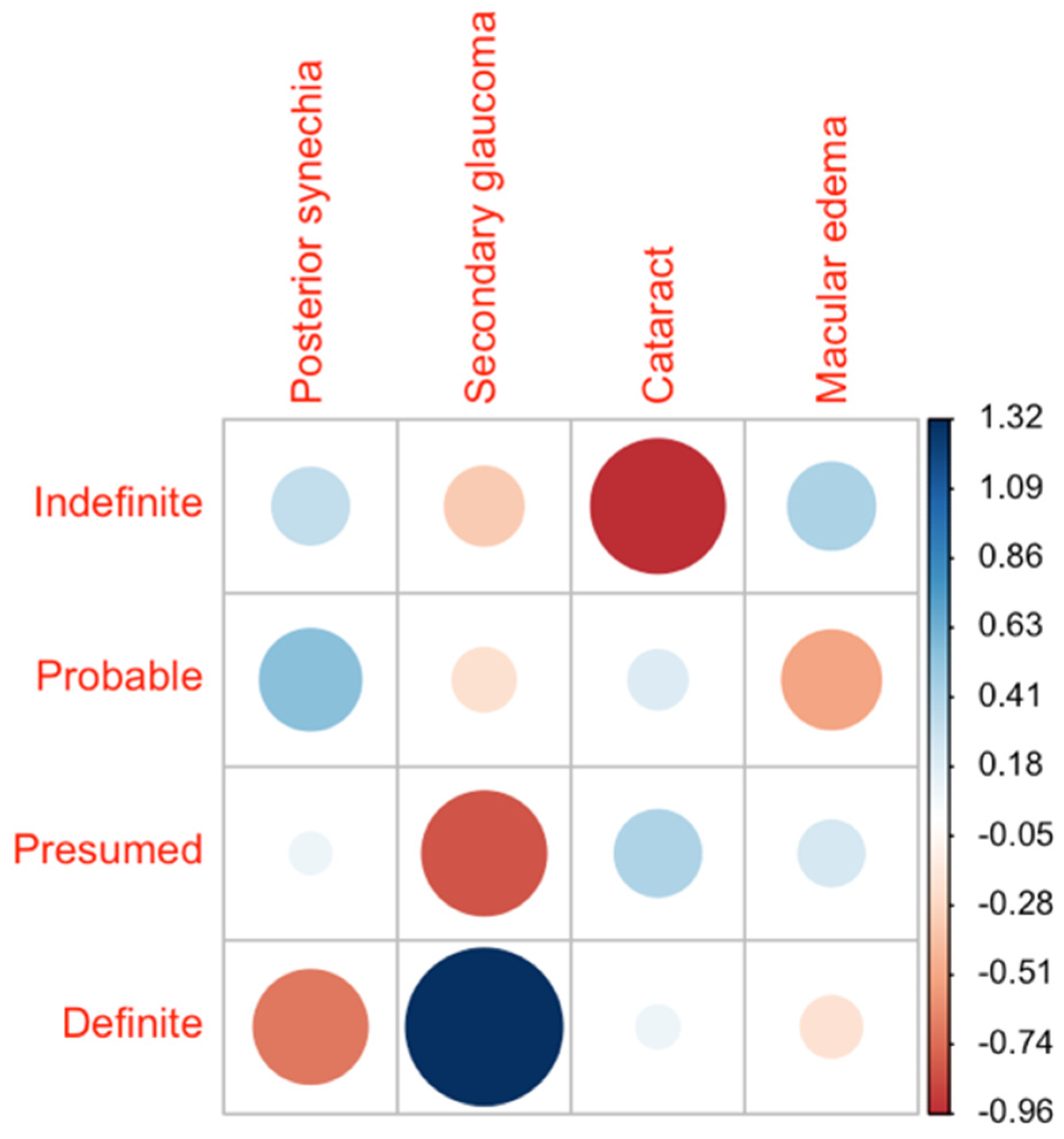
3.2.2. Ocular Complications
3.3. Laboratory Findings
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sève, P.; Pacheco, Y.; Durupt, F.; Jamilloux, Y.; Gerfaud-Valentin, M.; Isaac, S.; Boussel, L.; Calender, A.; Androdias, G.; Valeyre, D.; et al. Sarcoidosis: A Clinical Overview from Symptoms to Diagnosis. Cells 2021, 10, 766. [Google Scholar] [CrossRef] [PubMed]
- Brito-Zerón, P.; Kostov, B.; Superville, D.; Baughman, R.P.; Ramos-Casals, M.; Autoimmune Big Data Study Group. Geoepidemiological big data approach to sarcoidosis: Geographical and ethnic determinants. Clin. Exp. Rheumatol. 2019, 37, 1052–1064. Available online: https://pubmed.ncbi.nlm.nih.gov/31498063 (accessed on 15 November 2021). [PubMed]
- Ohara, K.; Okubo, A.; Sasaki, H.; Kamata, K. Intraocular manifestations of systemic sarcoidosis. Jpn. J. Ophthalmol. 1992, 36, 452–457. Available online: https://pubmed.ncbi.nlm.nih.gov/1289622 (accessed on 15 November 2021). [PubMed]
- Pasadhika, S.; Rosenbaum, J.T. Ocular Sarcoidosis. Clin. Chest Med. 2015, 36, 669–683. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heiligenhaus, A.; Wefelmeyer, D.; Wefelmeyer, E.; Rösel, M.; Schrenk, M. The eye as a common site for the early clinical manifestation of sarcoidosis. Ophthalmic Res. 2011, 46, 9–12. [Google Scholar] [CrossRef]
- Rochepeau, C.; Jamilloux, Y.; Kerever, S.; Febvay, C.; Perard, L.; Broussolle, C.; Burillon, C.; Kodjikian, L.; Seve, P. Long-term visual and systemic prognoses of 83 cases of biopsy-proven sarcoid uveitis. Br. J. Ophthalmol. 2017, 101, 856–861. [Google Scholar] [CrossRef]
- Radosavljević, A.; Jakšić, V.; Pezo, L.; Kovačević-Pavićević, D.; Ilić, A.; Mihailović Vučinić, V. Clinical Features of Ocular Sarcoidosis in Patients with Biopsy-proven Pulmonary Sarcoidosis in Serbia. Ocul. Immunol. Inflamm. 2017, 25, 785–789. [Google Scholar] [CrossRef]
- Ma, S.P.; Rogers, S.L.; Hall, A.J.; Hodgson, L.; Brennan, J.; Stawell, R.J.; Lim, L.L. Sarcoidosis-related Uveitis: Clinical Presentation, Disease Course, and Rates of Systemic Disease Progression After Uveitis Diagnosis. Am. J. Ophthalmol. 2019, 198, 30–36. [Google Scholar] [CrossRef]
- El Jammal, T.; Jamilloux, Y.; Gerfaud-Valentin, M.; Valeyre, D.; Sève, P. Refractory Sarcoidosis: A Review. Ther. Clin. Risk Manag. 2020, 16, 323–345. [Google Scholar] [CrossRef] [Green Version]
- Herbort, C.P.; Rao, N.A.; Mochizuki, M.; members of Scientific Committee of First International Workshop on Ocular Sarcoidosis. International criteria for the diagnosis of ocular sarcoidosis: Results of the first International Workshop on Ocular Sarcoidosis (IWOS). Ocul. Immunol. Inflamm. 2009, 17, 160–169. [Google Scholar] [CrossRef]
- Mochizuki, M.; Smith, J.R.; Takase, H.; Kaburaki, T.; Acharya, N.R.; Rao, N.A. Revised Criteria of International Workshop on Ocular Sarcoidosis (IWOS) for the Diagnosis of Ocular Sarcoidosis. Br. J. Ophthalmol. 2019, 103, 1418–1422. [Google Scholar] [CrossRef]
- Jabs, D.A.; Nussenblatt, R.B.; Rosenbaum, J.T.; Standardization of Uveitis Nomenclature (SUN) Working Group. Standardization of uveitis nomenclature for reporting clinical data. Results of the First International Workshop. Am. J. Ophthalmol. 2005, 140, 509–516. [Google Scholar] [CrossRef] [PubMed]
- Jamilloux, Y.; Kodjikian, L.; Broussolle, C.; Sève, P. Sarcoidosis and uveitis. Autoimmun. Rev. 2014, 13, 840–849. [Google Scholar] [CrossRef]
- Reid, G.; Williams, M.; Compton, M.; Silvestri, G.; McAvoy, C. Ocular sarcoidosis prevalence and clinical features in the Northern Ireland population. Eye 2021. Epub ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Niederer, R.L.; Ma, S.P.; Wilsher, M.L.; Ali, N.Q.; Sims, J.L.; Tomkins-Netzer, O.; Lightman, S.L.; Lim, L.L. Systemic Associations of Sarcoid Uveitis: Correlation With Uveitis Phenotype and Ethnicity. Am. J. Ophthalmol. 2021, 229, 169–175. [Google Scholar] [CrossRef] [PubMed]
- Schupp, J.C.; Freitag-Wolf, S.; Bargagli, E.; Mihailović-Vučinić, V.; Rottoli, P.; Grubanovic, A.; Müller, A.; Jochens, A.; Tittmann, L.; Schnerch, J.; et al. Phenotypes of organ involvement in sarcoidosis. Eur. Respir. J. 2018, 51, 1700991. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dammacco, R.; Biswas, J.; Kivelä, T.T.; Zito, F.A.; Leone, P.; Mavilio, A.; Sisto, D.; Alessio, G.; Dammacco, F. Ocular sarcoidosis: Clinical experience and recent pathogenetic and therapeutic advancements. Int. Ophthalmol. 2020, 40, 3453–3467. [Google Scholar] [CrossRef]
- Acharya, N.R.; Browne, E.N.; Rao, N.; Mochizuki, M.; International Ocular Sarcoidosis Working Group. Distinguishing Features of Ocular Sarcoidosis in an International Cohort of Uveitis Patients. Ophthalmology 2018, 125, 119–126. [Google Scholar] [CrossRef] [Green Version]
- Durrani, O.M.; Tehrani, N.N.; Marr, J.E.; Moradi, P.; Stavrou, P.; Murray, P.I. Degree, duration, and causes of visual loss in uveitis. Br. J. Ophthalmol. 2004, 88, 1159–1162. [Google Scholar] [CrossRef] [Green Version]
- Gundlach, E.; Hoffmann, M.M.; Prasse, A.; Heinzelmann, S.; Ness, T. Interleukin-2 Receptor and Angiotensin-Converting Enzyme as Markers for Ocular Sarcoidosis. PLoS ONE 2016, 11, e0147258. [Google Scholar] [CrossRef] [Green Version]
- Gundlach, E.; Temmesfeld-Wollbrück, B.; Pleyer, U. Ocular sarcoidosis: Diagnosis and therapy. Ophthalmologe 2017, 114, 865–876. [Google Scholar] [CrossRef] [PubMed]
- Takase, H. Characteristics and management of ocular sarcoidosis. Immunol. Med. 2021, 1–10, Epub ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Groen-Hakan, F.; Eurelings, L.; ten Berge, J.C.; van Laar, J.; Ramakers, C.; Dik, W.A.; Rothova, A. Diagnostic Value of Serum-Soluble Interleukin 2 Receptor Levels vs. Angiotensin-Converting Enzyme in Patients With Sarcoidosis-Associated Uveitis. JAMA Ophthalmol. 2017, 135, 1352–1358. [Google Scholar] [CrossRef]
- Papasavvas, I.; Gehrig, B.; Herbort, C.P., Jr. The Comparative Value of Serum Angiotensin Converting Enzyme (ACE) and Lysozyme and the Use of Polyclonal Antibody Activation in the Work-up of Ocular Sarcoidosis. Diagnostics 2021, 11, 608. [Google Scholar] [CrossRef]
- Tomita, H.; Sato, S.; Matsuda, R.; Sugiura, Y.; Kawaguchi, H.; Niimi, T.; Yoshida, S.; Morishita, M. Serum lysozyme levels and clinical features of sarcoidosis. Lung 1999, 177, 161–167. [Google Scholar] [CrossRef]
- Sahin, O.; Ziaei, A.; Karaismailoğlu, E.; Taheri, N. The serum angiotensin converting enzyme and lysozyme levels in patients with ocular involvement of autoimmune and infectious diseases. BMC Ophthalmol. 2016, 16, 19. [Google Scholar] [CrossRef] [Green Version]
- Murakami, K.; Koh, J.; Taruya, J.; Ito, H. Mimicking the Recurrence of Malignant Lymphoma. Case Rep. Neurol. 2021, 13, 605–612. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Intraocular findings |
| 1. Granulomatous keratic precipitates, iris nodules/granulomas (Koeppe/Busacca) |
| 2. Nodules in the trabecular meshwork (TM) and/or tent-like peripheral anterior synechiae |
| 3. Vitreous opacities “snowballs” |
| 4. Peripheral chorioretinal lesions (active and/or atrophic) |
| 5. Segmental periphlebitis (±“candle wax phenomenon”) and/or retinal macro aneurysm in an inflamed eye |
| 6. Optic nerve granulomas and/or solitary choroidal granulomas |
| 7. Mutuality |
| (a) |
| Further diagnostic criteria |
| 1. Chest x-ray or computer tomography findings with bilateral hilar lymphadenopathy (BHL) |
| 2. Negative tuberculin skin test or interferon-gamma releasing assay |
| 3. Elevated serum Angiotensin-converting enzyme (ACE) values |
| 4. Elevated serum lysozyme values |
| 5. CD4/CD8 ratio > 3.5 in bronchoalveolar lavage (BAL) |
| 6. Positive gallium-67 scintigraphy or 18F-fluorodeoxyglucose positron emission tomography (PET) imaging |
| 7. Lymphopenia (<1000 cells/µL) |
| 8. Parenchymal lung changes in line with sarcoidosis |
| 9. Elevated soluble interleukin-2 receptor (sIL-2R) 1 |
| (b) |
| Level of Evidence | Diagnostic Criteria |
|---|---|
| Definite ocular sarcoidosis | Biopsy-confirmed diagnosis with clinically corresponding uveitis |
| Presumed ocular sarcoidosis | Biopsy was not performed or negative; however, chest X-ray/computer tomography findings with hilum changes and 2 positive listed intraocular findings |
| Probable ocular sarcoidosis | Biopsy was not performed or negative; no positive chest X-ray/computer tomography findings, but 3 of the listed intraocular findings and 2 positive laboratory/imaging findings are available |
| Indefinite ocular sarcoidosis | Ocular sarcoidosis suspected intraocular findings or investigations without fitting into a pattern of the above categories |
| Definite | Presumed | Probable | Indefinite | Total | ||
|---|---|---|---|---|---|---|
| Count n (%) | 24 (28.6) | 33 (39.3) | 10 (11.9) | 17 (20.2) | 84 (100) | |
| Gender n (%) | Female | 17 (70.8) | 20 (60.6) | 6 (60.0) | 7 (41.2) | 50 (59.5) |
| Male | 7 (29.1) | 13 (39.4) | 4 (40.0) | 10 (58.8) | 34 (40.5) | |
| Age mean (Range) | 52 (31–77) | 58 (28–78) | 51 (11–87) | 45 (8–87) | 53 (8–87) | |
| Extraocular Manifestations n (%) | Lung | 21 (87.5) | 33 (100.0) | 0 (0.0) | 2 (11.8) | 56 (66.7) |
| Skin | 10 (41.7) | 3 (9.1) | 0 (0.0) | 0 (0.0) | 13 (15.5) | |
| Lymph nodes | 3 (12.5) | 1 (3.0) | 0 (0.0) | 0 (0.0) | 4 (4.8) | |
| Nervous system | 7 (29.2) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 7 (8.3) | |
| Heart | 3 (12.5) | 1 (3.0) | 0 (0.0) | 0 (0.0) | 4 (4.8) | |
| Liver | 2 (8.3) | 1 (3.0) | 0 (0.0) | 0 (0.0) | 3 (3.6) | |
| Spleen | 5 (20.8) | 1 (3.0) | 0 (0.0) | 0 (0.0) | 6 (7.1) | |
| Kidney | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | |
| Joints | 1 (4.2) | 2 (6.1) | 0 (0.0) | 1 (5.9) | 4 (4.8) |
| Definite | Presumed | Probable | Indefinite | Total | ||
|---|---|---|---|---|---|---|
| Number of patients | 24 | 33 | 10 | 17 | 84 | |
| Bilaterality | 79.2% (19/24) | 70.0% (23/33) | 100.0% (10/10) | 58.8% (10/17) | 73.8% (62/84) | |
| Anterior | Total | 25.0% (6/24) | 36.4% (12/33) | 20.0% (2/10) | 35.3% (6/17) | 31.0% (26/84) |
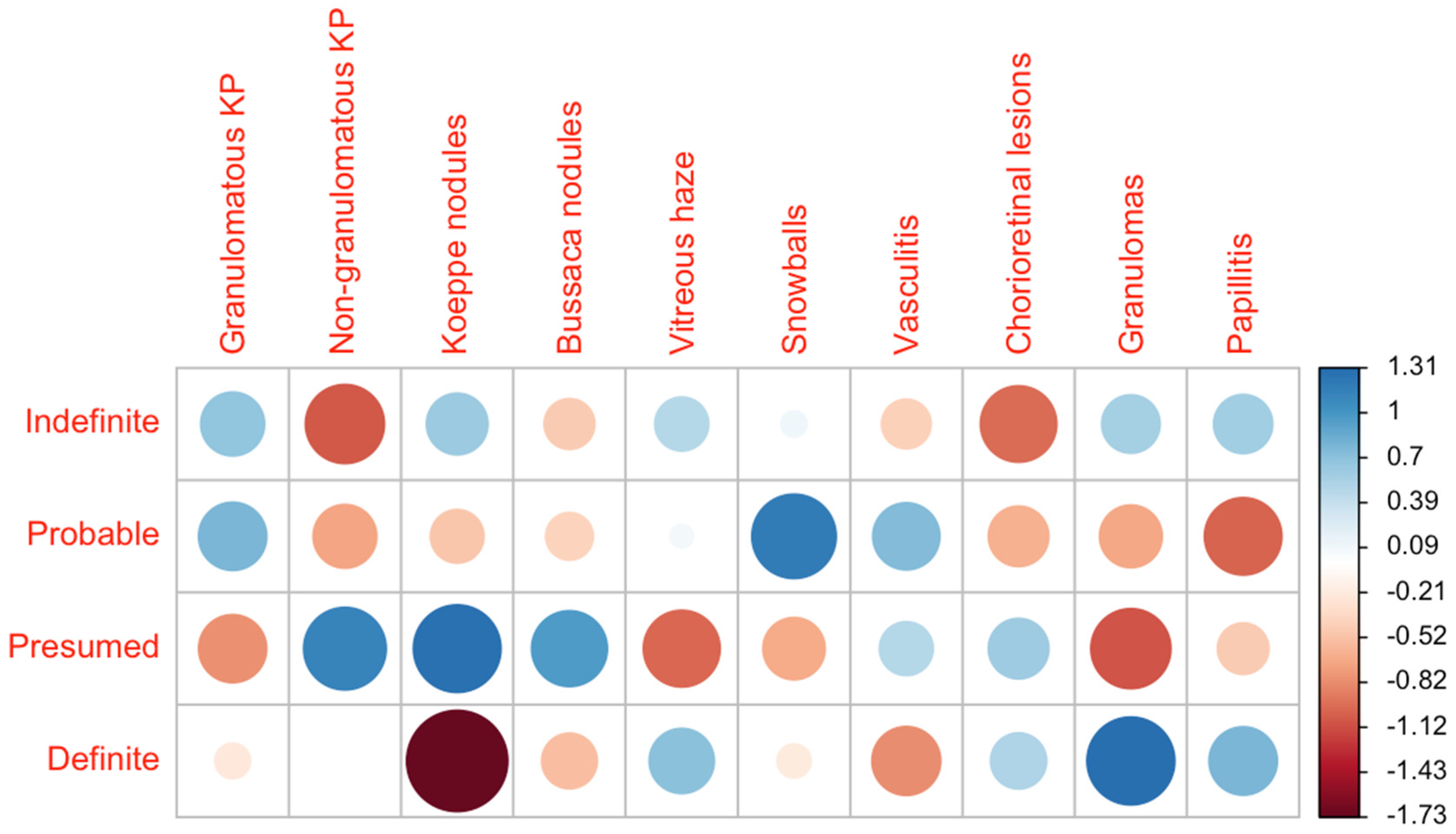
| Granulomatous keratic precipitates (KP) | 25% (6/24) | 21.2% (7/33) | 50.0% (5/10) | 35.3% (6/17) | 28.6% (24/84) | |
| Non-granulomatous KP | 25.0% (6/24) | 36.4% (12/33) | 20.0% (2/10) | 11.8% (2/17) | 26.2% (22/84) | |
| Koeppe nodules | 0.0% (0/24) | 21.2% (7/33) | 10.0% (1/10) | 17.6% (3/17) | 13.1% (11/84) | |
| Bussaca nodules | 0.0% (0/24) | 3.0% (1/33) | 0.0% (0/10) | 29.4% (0/17) | 1.2% (1/84) | |
| Intermediate | Total | 20.8% (5/24) | 30.3% (10/33) | 60.0% (6/10) | 35.3% (6/17) | 32.1% (27/84) |
| Vitreous haze | 37.5% (9/24) | 21.2% (7/33) | 40.0% (4/10) | 35.3% (6/17) | 31.0% (26/84) | |
| Snowballs | 20.8% (5/24) | 18.2% (6/33) | 50.0% (5/10) | 23.5% (4/17) | 23.8% (20/84) | |
| Vasculitis | 4.2% (1/24) | 12.1% (4/33) | 20.0% (2/10) | 5.9% (1/17) | 9.5% (8/84) | |
| Posterior | Total | 29.2% (7/24) | 12.1% (4/33) | 20.0% (2/10) | 5.9% (1/17) | 17.6% (14/84) |
| Chorioretinal lesions | 29.2% (7/24) | 30.3% (10/33) | 20.0% (2/10) | 11.8% (2/17) | 25% (21/84) | |
| Granulomas | 8.3% (2/24) | 0.0% (0/33) | 0.0% (0/10) | 5.9% (1/17) | 3.6% (3/84) | |
| Papillitis | 12.5% (3/24) | 6.1% (2/33) | 0.0% (0/10) | 11.8% (2/17) | 8.3% (7/84) | |
| Panuveitis | Total | 20.8% (5/24) | 21.2% (7/33) | 0.0% (0/10) | 23.5% (4/17) | 19.0% (16/84) |
| Complications | Total | 62.5% (15/24) | 54.5% (18/33) | 60.0% (6/10) | 47.0% (8/17) | 56.0% (47/84) |
| Posterior synechia | 20.8% (5/24) | 27.3% (9/33) | 40.0% (4/10) | 23.5% (4/17) | 26.2% (22/84) | |
| Secondary glaucoma | 20.8% (5/24) | 6.1% (2/33) | 10.0% (1/10) | 5.9% (1/17) | 10.7% (9/84) | |
| Cataract | 8.3% (2/24) | 9.1% (3/33) | 10.0% (1/10) | 0% (0/17) | 7.1% (6/84) | |
| Macular edema | 25.0% (6/24) | 27.3% (9/33) | 20.0% (2/10) | 23.5% (4/17) | 25% (21/84) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
zur Bonsen, L.S.; Pohlmann, D.; Rübsam, A.; Pleyer, U. Findings and Graduation of Sarcoidosis-Related Uveitis: A Single-Center Study. Cells 2022, 11, 89. https://doi.org/10.3390/cells11010089
zur Bonsen LS, Pohlmann D, Rübsam A, Pleyer U. Findings and Graduation of Sarcoidosis-Related Uveitis: A Single-Center Study. Cells. 2022; 11(1):89. https://doi.org/10.3390/cells11010089
Chicago/Turabian Stylezur Bonsen, Lynn S., Dominika Pohlmann, Anne Rübsam, and Uwe Pleyer. 2022. "Findings and Graduation of Sarcoidosis-Related Uveitis: A Single-Center Study" Cells 11, no. 1: 89. https://doi.org/10.3390/cells11010089
APA Stylezur Bonsen, L. S., Pohlmann, D., Rübsam, A., & Pleyer, U. (2022). Findings and Graduation of Sarcoidosis-Related Uveitis: A Single-Center Study. Cells, 11(1), 89. https://doi.org/10.3390/cells11010089