
A Next Generation Sequencing-Based Protocol for Screening of Variants of Concern in Autism Spectrum Disorder

 ,
,  , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Enrollment
2.2. DNA Extraction and WGS
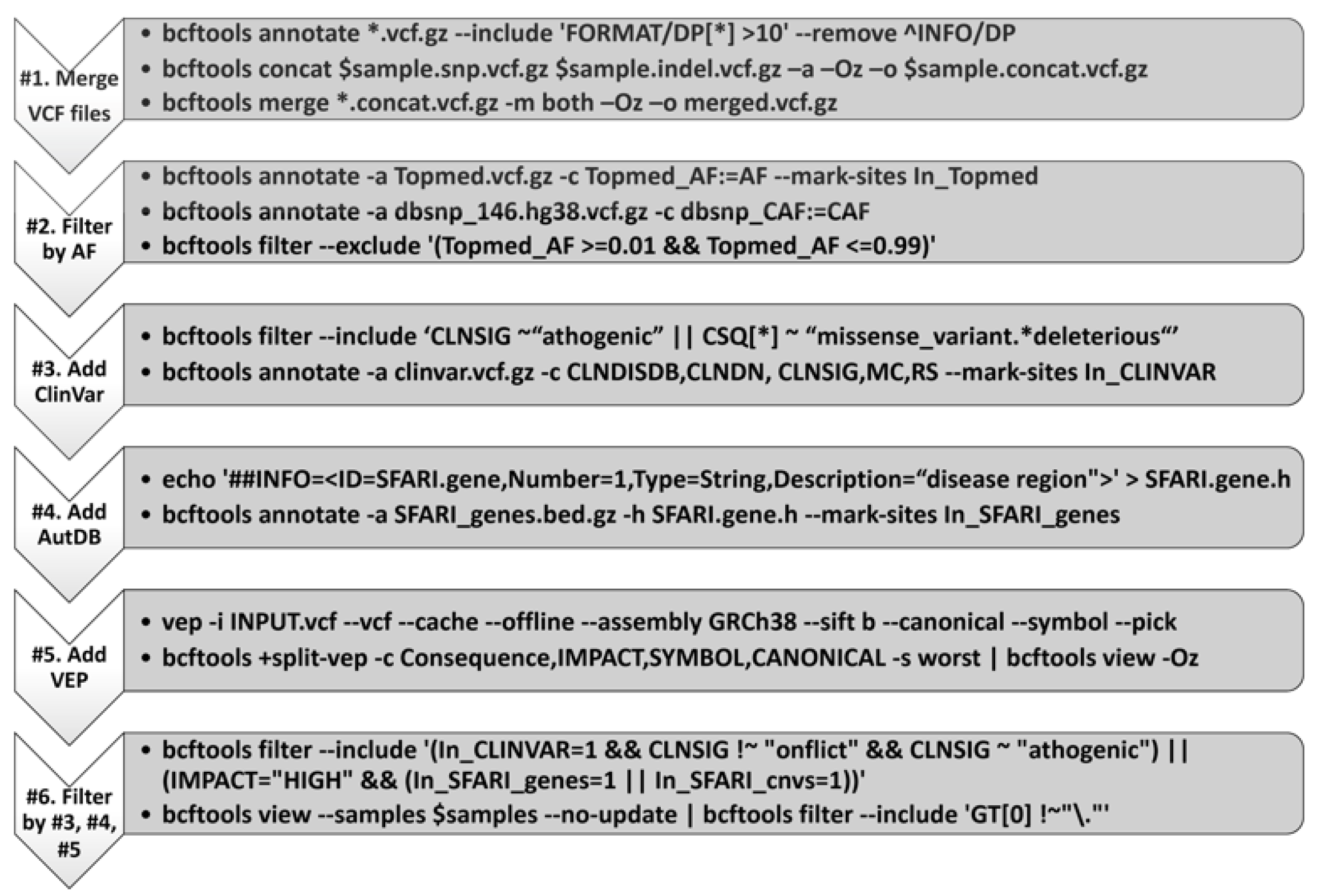
2.3. Sequencing Data Processing and Genetic Variant Discovery
2.4. Discovering Plausible ASD Associated Variants
2.5. Manual Review of Known ASD-Associated Variants
2.6. Sanger Sequencing
3. Results
3.1. Patient Cohort Summary
3.2. Summary of Variants and Sanger Confirmation
3.3. Clinical Synopsis of the Case Series Illustrates the Utility of the Whole Genome Sequencing Test in Understanding ASD Pathophysiology and Comorbidities, Providing Targeted Treatment, and Offering Preventative Guidance
3.4. Genetic Report Design: Summary of Variant Information and Clinical Interpretation in the Patient Cohort
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Subject | Scale of Variant | Gene Name and Location | Variant Type | Encoded Protein | Signaling Pathways/Neuronal Circuitry | Other Conditions Associated with the Variant | Mutation Confirmed by Sanger? |
|---|---|---|---|---|---|---|---|
| #2 | Small | GJB2 (chr13:20189473:C:T) | Missense | Connexin 26, CX26 (gap junction protein, beta 2) | Calcium Signaling Pathway | Hearing impairment; Keratitis-ichthyosis-deafness syndrome, autosomal dominant; Mutilating keratoderma; genetic deafness | Yes |
| #2 | Small | PROKR2 (chr20:5302662:C:G) | Missense | Prokineticin receptor 2 | Mood regulation; Gonadotropin-releasing hormone; Neutrophil dependent inflammation; Hyper nociception; Migration of nerve cells; Neurogenesis | Kallmann syndrome 3 | No |
| #2 | Large | PWRN1 in 15q11.2 (chr15:24521630:A:G) | Deletion-Duplication | N.A. | N.A. | N.A. | N.A. |
| #3 | Small | PROP1 (chr5:177995888:G:A) | Stop gained | Paired-like homeodomain transcription factor | Retinoic acid production and signaling pathway; Regulates neuronal excitability | Pituitary hormone deficiency, combined | Yes |
| #3 | Small | CYP11B1 (chr8:142874995:G:A) | Missense | Enzyme: 11-beta-hydroxylase | Non identified | Adrenal hyperplasia; congenital Hyperaldosteronism, familial, type I | Yes |
| #3 | Small | MRE11 (chr11:94459461:G:A) | Stop gained | Double Strand Break Repair Nuclease | DNA damage signaling; Chromatin stability | Hereditary cancer-predisposing syndrome; Ataxia-telangiectasia-like disorder 1 | N.A. |
| #3 | Large | POLR3E in 16p12.1 (chr16:22305383:GA:G) | Deletion-Duplication | DNA-directed RNA polymerase III subunit RPC5 | RNA Polymerase III Transcription Initiation; Transcription of tRNA. May be important for fighting CNS viral infection | N.A. | N.A. |
| #4 | Small | SLC7A14 (chr3:170480891:C:A) | Missense | Glycosylated, cationic amino acid transporter protein with 14 transmembrane domains | Full-length 771-amino acid SLC7A14 protein has 14 transmembrane domains and an N-glycosylation site in extracellular loop-2 | Retinitis pigmentosa | Yes |
| #4 | Small | GJB2 (chr13:20189473:C:T) | Missense | Connexin 26, CX26 (gap junction protein, beta 2) | Calcium Signaling Pathway | Hearing impairment | Yes |
| #4 | Small | TXNL4A (chr11:94459461:G:A) | Intron | DIM1, U5 snRNP-SPECIFIC PROTEIN, a member of the U5 small ribonucleoprotein particle (snRNP) | Spliceosome pathway | Burn-McKeown syndrome | N.A. |
| #5 | Small | USH2A (chr1:216078088:C:T) | Splice donor | Usherin | USH protein network pathway | Usher syndrome, type 2A; Retinitis pigmentosa 39 | N.A. |
| #5 | Small | SERPINB7 (chr18:63798670:C:CT) | Frameshift | SERPINB7 | Degradation of SERPINB7 protein by 26S proteasome-mediated pathway | Palmoplantar keratoderma, nagashima type | Yes |
| #5 | Small | BSCL2 (chr11:62692671:C:A) | Missense & NMD transcript | Seipin | Critical in pathway of adipogenesis; Affect neurogenesis in hypothalamus; May be involved in hypothalamic pituitary gland axis function | Charcot-Marie-Tooth disease, type 2; Congenital generalized lipodystrophy type 2 | No |
| #5 | Large | MRNIP in 5q35 (chr5:179858784:G:A) | Duplication | MRN- interacting protein | N.A. | N.A. | |
| #6 | Small | MYOC (chr1:171652476:G:A) | Splice region variant & intron variant & NMD transcript variant | Myocilin | Modulator of Wnt signaling pathway; Wild-type MYOC inhibits activation of the IL-1/NF-κB pathway | Glaucoma | Yes |
| #6 | Small | SLCO1B1 (chr12:21196975:C:T) | Stop gained | Organic anion transporting polypeptide 1B1 | Liver-specific member of the organic anion transporter family | Gilbert syndrome; Rotor syndrome | No |
| Gene Name | Modification | Mutation Patient | Mutation Father | Mutation Mother |
|---|---|---|---|---|
| SLC12A5 | chr20:46022977:A:G | yes | no | no |
| AIFM1 | chrX:130136710:T:C | no | yes | no |
| PROP1 | chr5:177995888:G:A | yes | yes | no |
| CYP11B1 | chr8:142874995:G:A | yes | no | yes |
| MYOC | chr1:171652476:G:A | yes | no | yes |
| SLCO1B1 | chr12:21196975:C:T | no | no | no |
| SLC7A14 | chr3:170480891:C:A | yes | yes | no |
| TXNL4A | chr18:79988603:CGCGCGCGCTAGCGCCGTGCGTGCTGACGGCATGT:C | yes | yes | no |
| BSCL2 | chr11:62692671:C:A | no | no | no |
| SERPINB7 | chr18:63798670:C:CT | Mutation present but different than the variant called by pipeline (63798670:TGAATGCT:GGAAAGGG) | no | no |
| GJB2 | chr13:20189473:C:T | yes | no | yes |
| PROKR2 | chr20:5302662:C:G | no | no | no |
References
- Suwinski, P.; Ong, C.; Ling, M.H.T.; Poh, Y.M.; Khan, A.M.; Ong, H.S. Advancing Personalized Medicine Through the Application of Whole Exome Sequencing and Big Data Analytics. Front. Genet. 2019, 10, 49. [Google Scholar] [CrossRef] [PubMed]
- Vassy, J.L.; Christensen, K.D.; Schonman, E.F.; Blout, C.L.; Robinson, J.O.; Krier, J.B.; Diamond, P.M.; Lebo, M.; Machini, K.; Azzariti, D.R.; et al. The Impact of Whole-Genome Sequencing on the Primary Care and Outcomes of Healthy Adult Patients. Ann. Intern. Med. 2017, 167, 159–169. [Google Scholar] [CrossRef] [PubMed]
- De la Torre-Ubieta, L.; Won, H.; Stein, J.L.; Geschwind, D.H. Advancing the Understanding of Autism Disease Mechanisms through Genetics. Nat. Med. 2016, 22, 345–361. [Google Scholar] [CrossRef]
- Maenner, M.J.; Shaw, K.A.; Baio, J.; Washington, A.; Patrick, M.; DiRienzo, M.; Christensen, D.L.; Wiggins, L.D.; Pettygrove, S.; Andrews, J.G.; et al. Prevalence of Autism Spectrum Disorder Among Children Aged 8 Years—Autism and Developmental Disabilities Monitoring Network, 11 Sites, United States. 2016. MMWR Surveill. Summ. 2020, 69, 1–12. [Google Scholar] [CrossRef]
- Sandin, S.; Lichtenstein, P.; Kuja-Halkola, R.; Hultman, C.; Larsson, H.; Reichenberg, A. The Heritability of Autism Spectrum Disorder. JAMA 2017, 318, 1182–1184. [Google Scholar] [CrossRef]
- Tammimies, K.; Marshall, C.R.; Walker, S.; Kaur, G.; Thiruvahindrapuram, B.; Lionel, A.C.; Yuen, R.K.C.; Uddin, M.; Roberts, W.; Weksberg, R.; et al. Molecular Diagnostic Yield of Chromosomal Microarray Analysis and Whole-Exome Sequencing in Children With Autism Spectrum Disorder. JAMA 2015, 314, 895–903. [Google Scholar] [CrossRef] [PubMed]
- Carter, M.T.; Scherer, S.W. Autism Spectrum Disorder in the Genetics Clinic: A Review. Clin. Genet. 2013, 83, 399–407. [Google Scholar] [CrossRef] [PubMed]
- Almandil, N.B.; Alkuroud, D.N.; AbdulAzeez, S.; AlSulaiman, A.; Elaissari, A.; Borgio, J.F. Environmental and Genetic Factors in Autism Spectrum Disorders: Special Emphasis on Data from Arabian Studies. Int. J. Environ. Res. Public Health 2019, 16, 658. [Google Scholar] [CrossRef] [PubMed]
- Miller, D.T.; Adam, M.P.; Aradhya, S.; Biesecker, L.G.; Brothman, A.R.; Carter, N.P.; Church, D.M.; Crolla, J.A.; Eichler, E.E.; Epstein, C.J.; et al. Consensus Statement: Chromosomal Microarray Is a First-Tier Clinical Diagnostic Test for Individuals with Developmental Disabilities or Congenital Anomalies. Am. J. Hum. Genet. 2010, 86, 749–764. [Google Scholar] [CrossRef]
- Grove, J.; Ripke, S.; Als, T.D.; Mattheisen, M.; Walters, R.K.; Won, H.; Pallesen, J.; Agerbo, E.; Andreassen, O.A.; Anney, R.; et al. Identification of Common Genetic Risk Variants for Autism Spectrum Disorder. Nat. Genet. 2019, 51, 431–444. [Google Scholar] [CrossRef]
- Yuen, R.K.C.; Merico, D.; Bookman, M.; Howe, J.L.; Thiruvahindrapuram, B.; Patel, R.V.; Whitney, J.; Deflaux, N.; Bingham, J.; Wang, Z.; et al. Whole Genome Sequencing Resource Identifies 18 New Candidate Genes for Autism Spectrum Disorder. Nat. Neurosci. 2017, 20, 602–611. [Google Scholar] [CrossRef]
- Satterstrom, F.K.; Kosmicki, J.A.; Wang, J.; Breen, M.S.; De Rubeis, S.; An, J.-Y.; Peng, M.; Collins, R.; Grove, J.; Klei, L.; et al. Large-Scale Exome Sequencing Study Implicates Both Developmental and Functional Changes in the Neurobiology of Autism. Cell 2020, 180, 568–584. [Google Scholar] [CrossRef]
- Hoang, N.; Buchanan, J.A.; Scherer, S.W. Heterogeneity in Clinical Sequencing Tests Marketed for Autism Spectrum Disorders. npj Genom. Med. 2018, 3, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Schaaf, C.P.; Betancur, C.; Yuen, R.K.C.; Parr, J.R.; Skuse, D.H.; Gallagher, L.; Bernier, R.A.; Buchanan, J.A.; Buxbaum, J.D.; Chen, C.-A.; et al. A Framework for an Evidence-Based Gene List Relevant to Autism Spectrum Disorder. Nat. Rev. Genet. 2020, 21, 367–376. [Google Scholar] [CrossRef] [PubMed]
- Zhao, S.; Chen, W.-J.; Dhar, S.U.; Eble, T.N.; Kwok, O.-M.; Chen, L.-S. Genetic Testing Experiences Among Parents of Children with Autism Spectrum Disorder in the United States. J. Autism Dev. Disord. 2019, 49, 4821–4833. [Google Scholar] [CrossRef]
- Wagner, K.E.; McCormick, J.B.; Barns, S.; Carney, M.; Middleton, F.A.; Hicks, S.D. Parent Perspectives Towards Genetic and Epigenetic Testing for Autism Spectrum Disorder. J. Autism Dev. Disord. 2020, 50, 3114–3125. [Google Scholar] [CrossRef]
- Jiang, Y.; Yuen, R.K.C.; Jin, X.; Wang, M.; Chen, N.; Wu, X.; Ju, J.; Mei, J.; Shi, Y.; He, M.; et al. Detection of Clinically Relevant Genetic Variants in Autism Spectrum Disorder by Whole-Genome Sequencing. Am. J. Hum. Genet. 2013, 93, 249–263. [Google Scholar] [CrossRef]
- Wood, C.L.; Warnell, F.; Johnson, M.; Hames, A.; Pearce, M.S.; McConachie, H.; Parr, J.R. Evidence for ASD Recurrence Rates and Reproductive Stoppage From Large UK ASD Research Family Databases. Autism Res. 2015, 8, 73–81. [Google Scholar] [CrossRef]
- Busner, J.; Targum, S.D. The Clinical Global Impressions Scale. Psychiatry 2007, 4, 28–37. [Google Scholar]
- Garcia, E.P.; Minkovsky, A.; Jia, Y.; Ducar, M.D.; Shivdasani, P.; Gong, X.; Ligon, A.H.; Sholl, L.M.; Kuo, F.C.; MacConaill, L.E.; et al. Validation of OncoPanel: A Targeted Next-Generation Sequencing Assay for the Detection of Somatic Variants in Cancer. Arch. Pathol. Lab. Med. 2017, 141, 751–758. [Google Scholar] [CrossRef] [PubMed]
- Daghsni, M.; Rima, M.; Fajloun, Z.; Ronjat, M.; Brusés, J.L.; M’rad, R.; Waard, M.D. Autism throughout Genetics: Perusal of the Implication of Ion Channels. Brain Behav. 2018, 8, e00978. [Google Scholar] [CrossRef] [PubMed]
- Chamma, I.; Chevy, Q.; Poncer, J.C.; Levi, S. Role of the Neuronal K-Cl Co-Transporter KCC2 in Inhibitory and Excitatory Neurotransmission. Front. Cell. Neurosci. 2012, 6, 5. [Google Scholar] [CrossRef] [PubMed]
- Tang, X.; Drotar, J.; Li, K.; Clairmont, C.D.; Brumm, A.S.; Sullins, A.J.; Wu, H.; Liu, X.S.; Wang, J.; Gray, N.S.; et al. Pharmacological Enhancement of KCC2 Gene Expression Exerts Therapeutic Effects on Human Rett Syndrome Neurons and Mecp2 Mutant Mice. Sci. Transl. Med. 2019, 11, eaau0164. [Google Scholar] [CrossRef]
- Zhang, L.; Huang, C.-C.; Dai, Y.; Luo, Q.; Ji, Y.; Wang, K.; Deng, S.; Yu, J.; Xu, M.; Du, X.; et al. Symptom Improvement in Children with Autism Spectrum Disorder Following Bumetanide Administration Is Associated with Decreased GABA/Glutamate Ratios. Transl. Psychiatry 2020, 10, 9. [Google Scholar] [CrossRef]
- Feng, J.-Y.; Li, H.-H.; Wang, B.; Shan, L.; Jia, F.-Y. Successive Clinical Application of Vitamin D and Bumetanide in Children with Autism Spectrum Disorder. Medicine 2020, 99, e18661. [Google Scholar] [CrossRef] [PubMed]
- Castro, P.J.S.; Fernandez, C.N.; Subirana, P.Q.; Ortiz, M.P. Vohwinkel Syndrome Secondary to Missense Mutation D66H in GJB2 Gene (Connexin 26) Can Include Epileptic Manifestations. Seizure 2010, 19, 129–131. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Yahyaoui, R.; Pérez-Frías, J. Amino Acid Transport Defects in Human Inherited Metabolic Disorders. Int. J. Mol. Sci. 2020, 21, 119. [Google Scholar] [CrossRef]
- Richards, S.; Aziz, N.; Bale, S.; Bick, D.; Das, S.; Gastier-Foster, J.; Grody, W.W.; Hegde, M.; Lyon, E.; Spector, E.; et al. Standards and Guidelines for the Interpretation of Sequence Variants: A Joint Consensus Recommendation of the American College of Medical Genetics and Genomics and the Association for Molecular Pathology. Genet. Med. 2015, 17, 405–423. [Google Scholar] [CrossRef] [PubMed]
- Li, M.M.; Datto, M.; Duncavage, E.J.; Kulkarni, S.; Lindeman, N.I.; Roy, S.; Tsimberidou, A.M.; Vnencak-Jones, C.L.; Wolff, D.J.; Younes, A.; et al. Standards and Guidelines for the Interpretation and Reporting of Sequence Variants in Cancer: A Joint Consensus Recommendation of the Association for Molecular Pathology, American Society of Clinical Oncology, and College of American Pathologists. J. Mol. Diagn. 2017, 19, 4–23. [Google Scholar] [CrossRef] [PubMed]
- Strande, N.T.; Brnich, S.E.; Roman, T.S.; Berg, J.S. Navigating the Nuances of Clinical Sequence Variant Interpretation in Mendelian Disease. Genet. Med. 2018, 20, 918–926. [Google Scholar] [CrossRef] [PubMed]
- Farmer, G.D.; Gray, H.; Chandratillake, G.; Raymond, F.L.; Freeman, A.L.J. Recommendations for Designing Genetic Test Reports to Be Understood by Patients and Non-Specialists. Eur. J. Hum. Genet. 2020, 28, 885–895. [Google Scholar] [CrossRef] [PubMed]
- Buxbaum, J.D.; Cutler, D.J.; Daly, M.J.; Devlin, B.; Roeder, K.; Sanders, S.J. Not All Autism Genes Are Created Equal: A Response to Myers et Al. Am. J. Hum. Genet. 2020, 107, 1000–1003. [Google Scholar] [CrossRef] [PubMed]
- Myers, S.M.; Challman, T.D.; Bernier, R.; Bourgeron, T.; Chung, W.K.; Constantino, J.N.; Eichler, E.E.; Jacquemont, S.; Miller, D.T.; Mitchell, K.J.; et al. Insufficient Evidence for “Autism-Specific” Genes. Am. J. Hum. Genet. 2020, 106, 587–595. [Google Scholar] [CrossRef]
- Srivastava, S.; Love-Nichols, J.A.; Dies, K.A.; Ledbetter, D.H.; Martin, C.L.; Chung, W.K.; Firth, H.V.; Frazier, T.; Hansen, R.L.; Prock, L.; et al. Meta-Analysis and Multidisciplinary Consensus Statement: Exome Sequencing Is a First-Tier Clinical Diagnostic Test for Individuals with Neurodevelopmental Disorders. Genet. Med. 2019, 21, 2413–2421. [Google Scholar] [CrossRef] [PubMed]
- Salfati, E.L.; Spencer, E.G.; Topol, S.E.; Muse, E.D.; Rueda, M.; Lucas, J.R.; Wagner, G.N.; Campman, S.; Topol, E.J.; Torkamani, A. Re-Analysis of Whole-Exome Sequencing Data Uncovers Novel Diagnostic Variants and Improves Molecular Diagnostic Yields for Sudden Death and Idiopathic Diseases. Genome Med. 2019, 11, 83. [Google Scholar] [CrossRef] [PubMed]
- Williams, S.M.; An, J.Y.; Edson, J.; Watts, M.; Murigneux, V.; Whitehouse, A.J.O.; Jackson, C.J.; Bellgrove, M.A.; Cristino, A.S.; Claudianos, C. An Integrative Analysis of Non-Coding Regulatory DNA Variations Associated with Autism Spectrum Disorder. Mol. Psychiatry 2019, 24, 1707–1719. [Google Scholar] [CrossRef]
- Zhang, R.; He, H.; Yuan, B.; Wu, Z.; Wang, X.; Du, Y.; Chen, Y.; Qiu, Z. An Intronic Variant of CHD7 Identified in Autism Patients Interferes with Neuronal Differentiation and Development. Neurosci. Bull. 2021, 37, 1091–1106. [Google Scholar] [CrossRef] [PubMed]
- An, J.-Y.; Lin, K.; Zhu, L.; Werling, D.M.; Dong, S.; Brand, H.; Wang, H.Z.; Zhao, X.; Schwartz, G.B.; Collins, R.L.; et al. Genome-Wide de Novo Risk Score Implicates Promoter Variation in Autism Spectrum Disorder. Science 2018, 362, eaat6576. [Google Scholar] [CrossRef]
- Cross-Disorder Group of the Psychiatric Genomics Consortium; Lee, S.H.; Ripke, S.; Neale, B.M.; Faraone, S.V.; Purcell, S.M.; Perlis, R.H.; Mowry, B.J.; Thapar, A.; Goddard, M.E.; et al. Genetic Relationship between Five Psychiatric Disorders Estimated from Genome-Wide SNPs. Nat. Genet. 2013, 45, 984–994. [Google Scholar] [CrossRef]
- Gaugler, T.; Klei, L.; Sanders, S.J.; Bodea, C.A.; Goldberg, A.P.; Lee, A.B.; Mahajan, M.; Manaa, D.; Pawitan, Y.; Reichert, J.; et al. Most Genetic Risk for Autism Resides with Common Variation. Nat. Genet. 2014, 46, 881–885. [Google Scholar] [CrossRef]
- Liu, L.; Lei, J.; Sanders, S.J.; Willsey, A.J.; Kou, Y.; Cicek, A.E.; Klei, L.; Lu, C.; He, X.; Li, M.; et al. DAWN: A Framework to Identify Autism Genes and Subnetworks Using Gene Expression and Genetics. Mol. Autism 2014, 5, 22. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.; Deng, L.; Jia, Q.; Huang, S.; Gu, J.; Zhou, F.; Gao, M.; Sun, X.; Feng, C.; Fan, G. DbMDEGA: A Database for Meta-Analysis of Differentially Expressed Genes in Autism Spectrum Disorder. BMC Bioinform. 2017, 18, 494. [Google Scholar] [CrossRef] [PubMed]



| Gene | Chromosomal Regions | |
|---|---|---|
| AHI1 | NLGN4X | 15q11-13 maternal deletion |
| CACNA1C | PTEN | 15q11-13 duplication |
| CHD8 | SHANK3 | 15q11-13 paternal deletion |
| CNTNAP2 | TSC1 | 15q11-13 duplication |
| EIF4E | TSC2 | 1q21.1 |
| FMR1 | UBE3A | 7q11.23 |
| FMR1-AS1 | GABAr | 16p11.2 |
| GBX2 | PCKB1 | 18q12.1 |
| KIF1A | DCHR7 | 22q11.2 |
| MECP2 | OXTR | 22q13 |
| NF1 | SLC6A4 | 17p11.2 |
| NLGN3 | FOLR1 | |
| KIZ | XRN2 | |
| Subject | Age (Year) | BMI | Sex | ASD Severity | Comorbidities |
|---|---|---|---|---|---|
| #1 | 6.6 | 23.6 | Female | Low | Hyperactivity, emotional lability, aggressive/destructive behavior, self-injury, sleep disturbance, premature birth, autoimmunity, allergic rhinitis, eczema, leaky bowel, and GI disturbance |
| #2 | 18.1 | 18.1 | Male | Low | Allergic rhinitis, sinusitis, autoimmunity, erosive ileitis, H.Pylori/GERD; Developed seizures 1 year after this genetic testing |
| #3 | 19.6 | 26.7 | Female | Moderate | OCD, Anxiety, Allergic rhinitis, autoimmunity |
| #4 | 6.9 | 16.5 | Male | High | Allergic rhinitis, GI disturbance, emotional lability |
| #5 | 5.7 | 16.0 | Male | Moderate | Hyperactive, emotional lability, sleep disturbance, allergic rhinitis, eczema, GERD |
| #6 | 3.5 | 16.1 | Male | Low | Hyperactive, emotional lability, aggressive/destructive behavior, sleep disturbance, eczema, anemia, autoimmunity, allergic rhinitis, GI disturbance |
| Gene Name and Location | Variant Type | Annotation on ClinVar or SFARI | Encoded Protein | Signaling Pathways/Neuronal Circuitry | Other Conditions Associated with the Variant | Mutation Confirmation by Sanger |
|---|---|---|---|---|---|---|
| SLC12A5 (chr20:46022977:A:G) | Splice region variant | SFARI risk gene | KCC2 (Type 2 K+-Cl− cotransporter) | Enhancement of the NF-κB/MMP-7 signaling pathway; Glycinergic signaling pathway. Regulates neuronal excitability | Epileptic encephalopathy, early infantile | Yes |
| IER3IP1 (chr18:47156119:A:G) | Splice region variant | Pathogenic on ClinVar | IER3IP1 | Although highly expressed in the brain, its role in the CNS circuitry is unknown | Microcephaly, epilepsy, diabetes syndrome | N.A. |
| AIFM1 (chrX:130136710:T:C) | 3 prime UTR | Likely pathogenic on ClinVar | Mitochondrial flavin adenine dinucleotide-dependent oxidoreductase | Ceramide signaling pathway, innate immunity; has known expression and functionsin the CNS | Mitochondrial encephalopathy | No |
| CEP19 in 3q29 (chr3:196711952:A:G) | SNV | SFARI risk gene | Centrosomal Protein 19 | Ciliary entry of intraflagellar transport; Although highly expressed in the brain, its role in the CNS circuitry is unknown | Delayed development (speech delay), mild or moderate intellectual disability, gastrointestinal disorders, morbid obesity | N.A. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, J.; Liu, J.; Tian, R.; Liu, K.; Zhuang, P.; Sherman, H.T.; Budjan, C.; Fong, M.; Jeong, M.-S.; Kong, X.-J. A Next Generation Sequencing-Based Protocol for Screening of Variants of Concern in Autism Spectrum Disorder. Cells 2022, 11, 10. https://doi.org/10.3390/cells11010010
Huang J, Liu J, Tian R, Liu K, Zhuang P, Sherman HT, Budjan C, Fong M, Jeong M-S, Kong X-J. A Next Generation Sequencing-Based Protocol for Screening of Variants of Concern in Autism Spectrum Disorder. Cells. 2022; 11(1):10. https://doi.org/10.3390/cells11010010
Chicago/Turabian StyleHuang, Jie, Jun Liu, Ruiyi Tian, Kevin Liu, Patrick Zhuang, Hannah Tayla Sherman, Christoph Budjan, Michelle Fong, Min-Seo Jeong, and Xue-Jun Kong. 2022. "A Next Generation Sequencing-Based Protocol for Screening of Variants of Concern in Autism Spectrum Disorder" Cells 11, no. 1: 10. https://doi.org/10.3390/cells11010010
APA StyleHuang, J., Liu, J., Tian, R., Liu, K., Zhuang, P., Sherman, H. T., Budjan, C., Fong, M., Jeong, M.-S., & Kong, X.-J. (2022). A Next Generation Sequencing-Based Protocol for Screening of Variants of Concern in Autism Spectrum Disorder. Cells, 11(1), 10. https://doi.org/10.3390/cells11010010