
A Prognostic Role for Circulating microRNAs Involved in Macrophage Polarization in Advanced Non-Small Cell Lung Cancer

 , ,
, , 

Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients’ Characteristics
2.2. Characteristics of the Healthy Blood Donors
2.3. Blood Sample Collection
2.4. RNA Isolation from Plasma Samples
2.5. Quantitative Real-Time PCR Analysis and miRNA Expression
2.6. Statistical Analysis
2.7. KM Plotter Analysis
3. Results
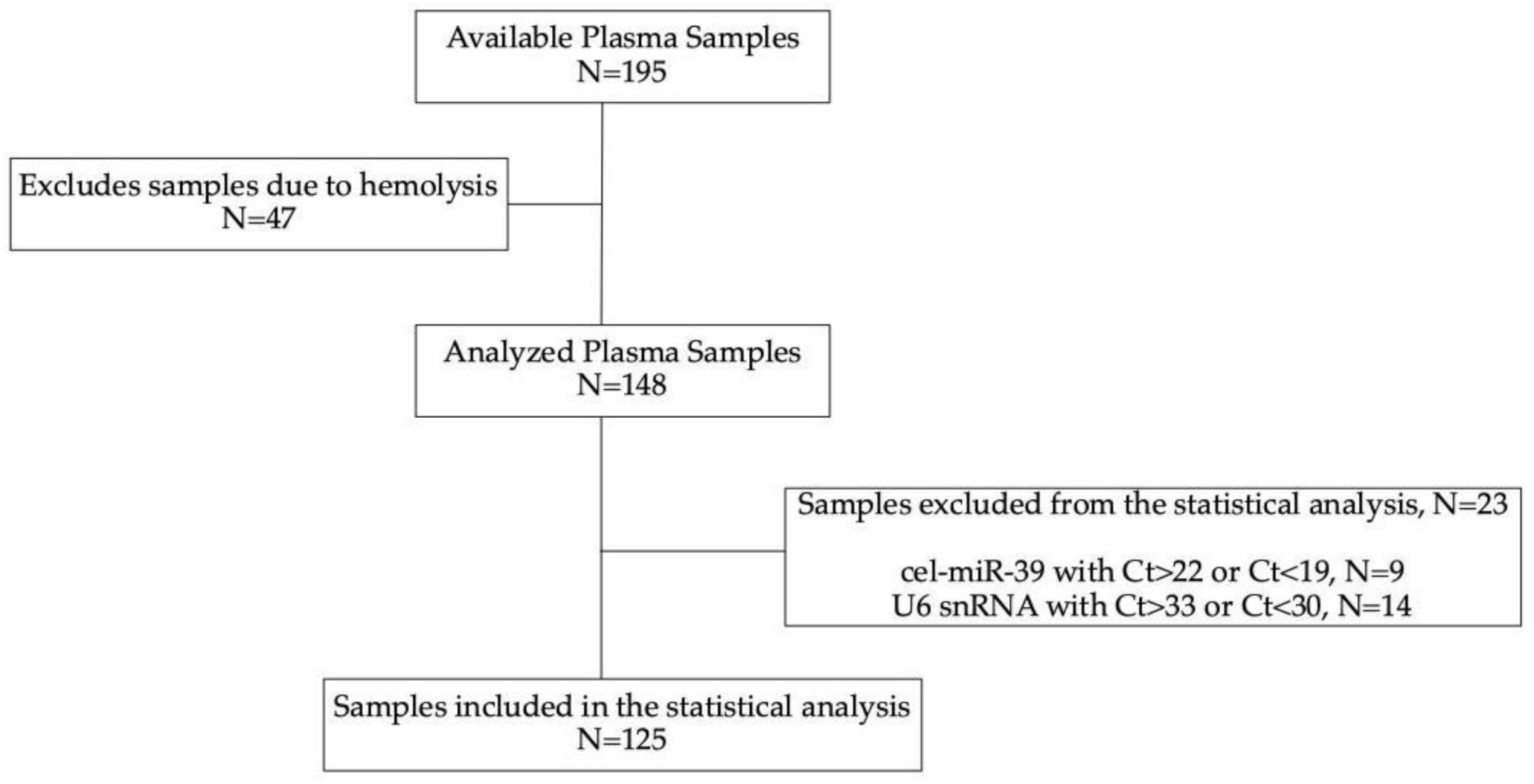
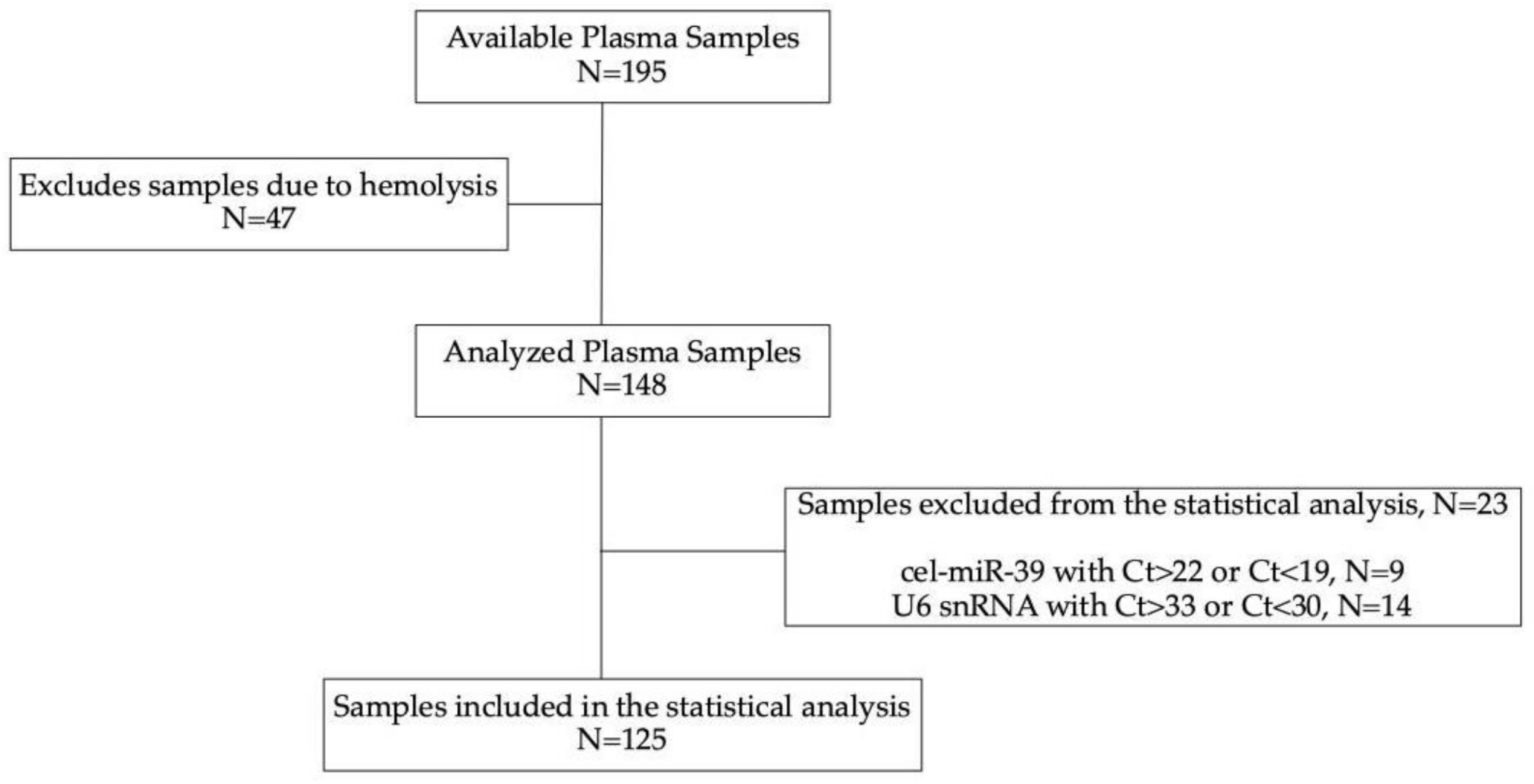
3.1. Patients’ Characteristics and Study Design
3.2. miRNA Expression and Clinicopathological Characteristics
3.3. miRNA Expression and Their Effect on Response to Treatment
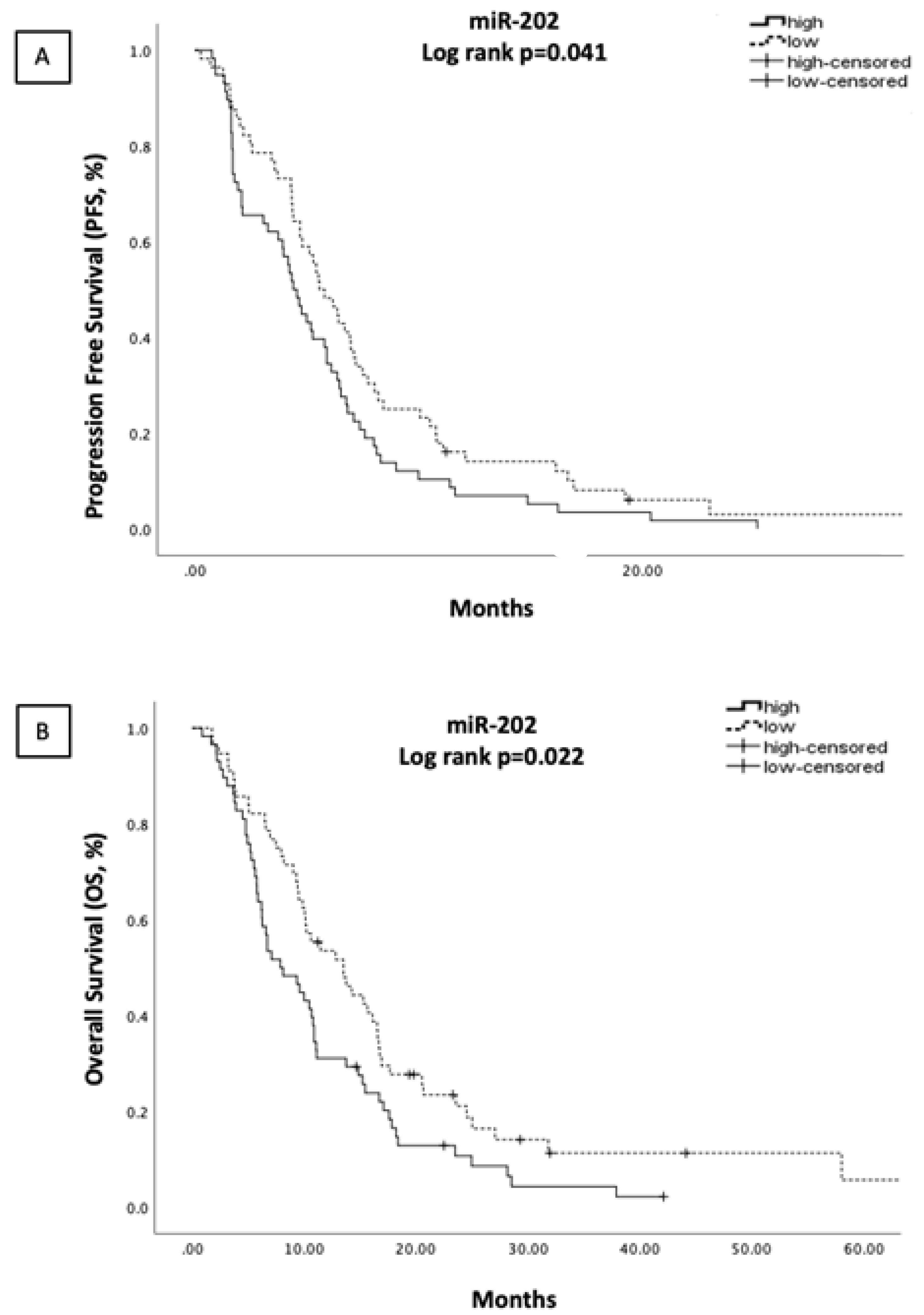
3.4. miRNA Expression and Association with Survival Outcomes
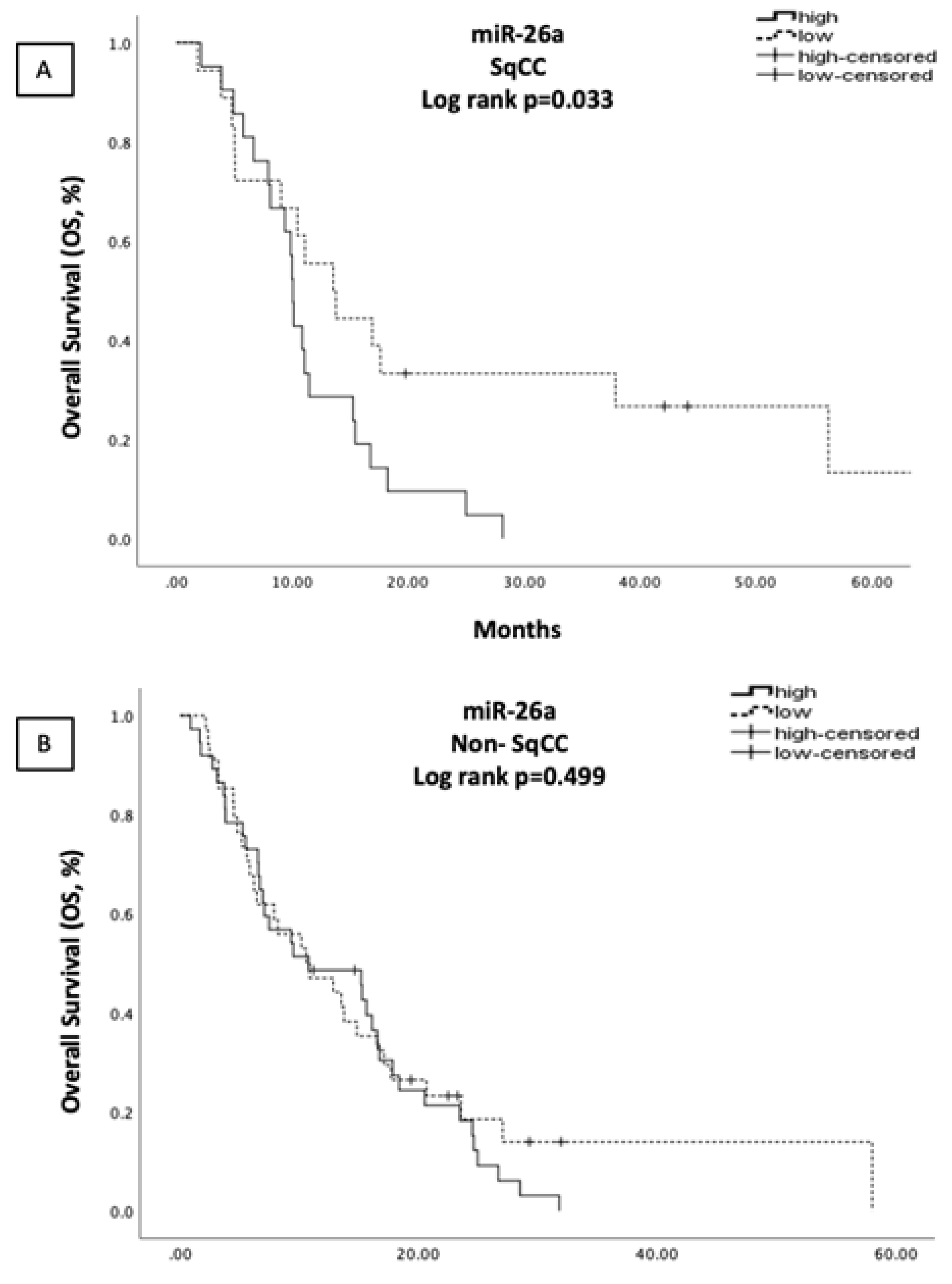
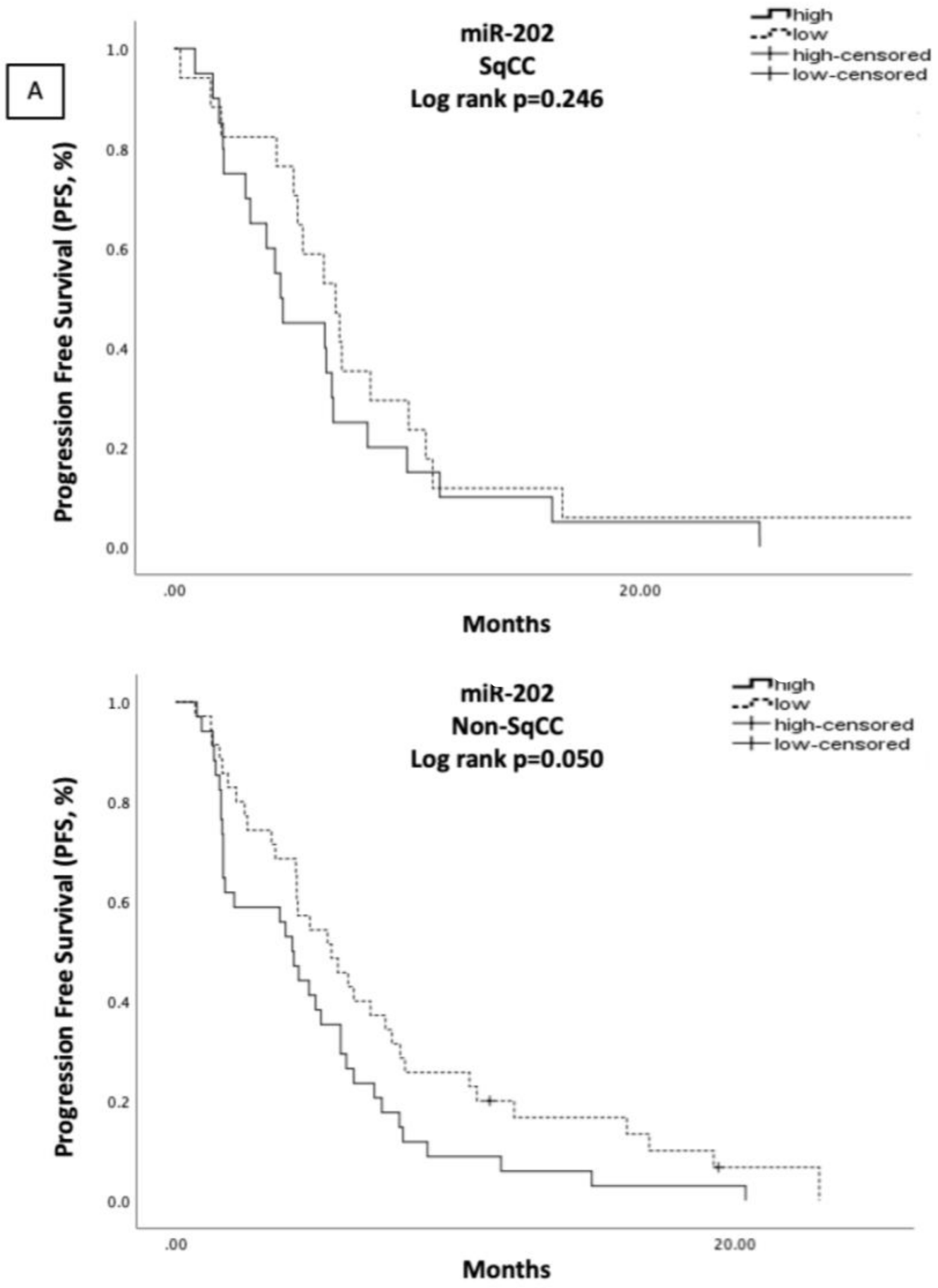
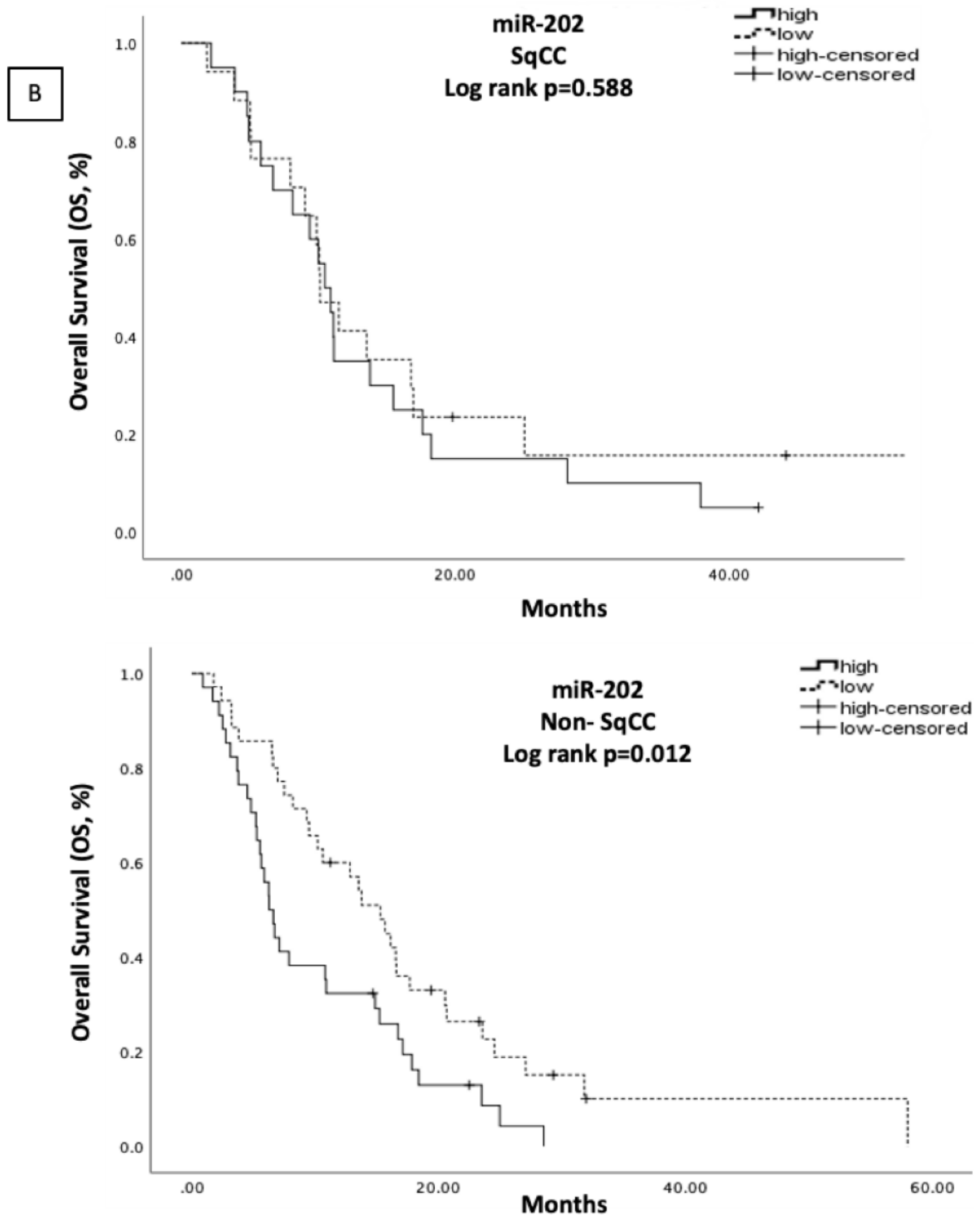
3.5. Correlations of Clinicopathological Characteristics and miRNA Expression with Patient Outcomes According to Histologic Subtype
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| Abbreviation | Definition |
| APCs | Antigen-presenting cells |
| cDNA | Complementary DNA |
| CDDP | Cis-diamminedichloridplatinum, cisplatin |
| CI | Confidence intervals |
| CT | Computed tomogaphy |
| Ct | Cycle threshold |
| CTLs | Cytotoxic T lymphocytes |
| ECOG | Eastern Cooperative Oncology Group |
| EDTA | Ethylenediamenetetraacetic acid |
| Et-OH | Ethanol |
| GALNT7 | N-acetylgalactosaninyltransferase 7 |
| GEM | Gemcitabine |
| HR | Hazard ratio |
| MATN2 | Matrilin 2 |
| miRNAs | microRNAs |
| MRI | Magnetic resonance imaging |
| M-CSF | Macrophage colony-stimulating factor |
| non-SqCC | non-Squamous |
| OS | Overall survival |
| PD | Progression disease |
| PEM | pemetrexed |
| PFS | Progression free survival |
| PR | Partial response |
| PS | Performance status |
| RT-qPCR | Real-time quantative polymerase chain reaction |
| SD | Stable disease |
| SqCC | Squamous |
| STAT3 | Signal transducer and activator of transcription 3 |
| TAMs | Tumor associated macrophages |
| TME | Tumor microenvironment |
| TXT | Taxotere |
References
- Zhang, C.; Leighl, N.B.; Wu, Y.L.; Zhong, W.Z. Emerging therapies for non-small cell lung cancer. J Hematol Oncol 2019, 12, 45. [Google Scholar] [CrossRef] [Green Version]
- Doroshow, D.B.; Sanmamed, M.F.; Hastings, K.; Politi, K.; Rimm, D.L.; Chen, L.; Melero, I.; Schalper, K.A.; Herbst, R.S. Immunotherapy in Non-Small Cell Lung Cancer: Facts and Hopes. Clin. Cancer Res. 2019, 25, 4592–4602. [Google Scholar] [CrossRef] [Green Version]
- Politi, K.; Herbst, R.S. Lung cancer in the era of precision medicine. Clin. Cancer Res. 2015, 21, 2213–2220. [Google Scholar] [CrossRef] [Green Version]
- Schrank, Z.; Chhabra, G.; Lin, L.; Iderzorig, T.; Osude, C.; Khan, N.; Kuckovic, A.; Singh, S.; Miller, R.J.; Puri, N. Current Molecular-Targeted Therapies in NSCLC and Their Mechanism of Resistance. Cancers 2018, 10, 224. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kyakulaga, A.H.; Aqil, F.; Munagala, R.; Gupta, R.C. Synergistic combinations of paclitaxel and withaferin A against human non-small cell lung cancer cells. Oncotarget 2020, 11, 1399–1416. [Google Scholar] [CrossRef] [Green Version]
- Papadaki, C.; Monastirioti, A.; Rounis, K.; Makrakis, D.; Kalbakis, K.; Nikolaou, C.; Mavroudis, D.; Agelaki, S. Circulating MicroRNAs Regulating DNA Damage Response and Responsiveness to Cisplatin in the Prognosis of Patients with Non-Small Cell Lung Cancer Treated with First-Line Platinum Chemotherapy. Cancers 2020, 12, 1282. [Google Scholar] [CrossRef]
- Siddik, Z.H. Cisplatin Mode of cytotoxic action and molecular basis of resistance. Oncogene 2003, 22, 7265–7279. [Google Scholar] [CrossRef] [Green Version]
- De Biasi, A.R.; Villena-Vargas, J.; Adusumilli, P.S. Cisplatin-induced antitumor immunomodulation: A review of preclinical and clinical evidence. Clin. Cancer Res. 2014, 20, 5384–5391. [Google Scholar] [CrossRef] [Green Version]
- Brambilla, E.; Le Teuff, G.; Marguet, S.; Lantuejoul, S.; Dunant, A.; Graziano, S.; Pirker, R.; Douillard, J.Y.; Le Chevalier, T.; Filipits, M.; et al. Prognostic Effect of Tumor Lymphocytic Infiltration in Resectable Non-Small-Cell Lung Cancer. J. Clin. Oncol 2016, 34, 1223–1230. [Google Scholar] [CrossRef]
- Syed, S.N.; Frank, A.C.; Raue, R.; Brune, B. MicroRNA-A Tumor Trojan Horse for Tumor-Associated Macrophages. Cells 2019, 8, 1482. [Google Scholar] [CrossRef] [Green Version]
- Larionova, I.; Cherdyntseva, N.; Liu, T.; Patysheva, M.; Rakina, M.; Kzhyshkowska, J. Interaction of tumor-associated macrophages and cancer chemotherapy. Oncoimmunology 2019, 8, 1596004. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thielmann, C.M.; Costa da Silva, M.; Muley, T.; Meister, M.; Herpel, E.; Muckenthaler, M.U. Iron accumulation in tumor-associated macrophages marks an improved overall survival in patients with lung adenocarcinoma. Sci Rep. 2019, 9, 11326. [Google Scholar] [CrossRef] [Green Version]
- Tamminga, M.; Hiltermann, T.J.N.; Schuuring, E.; Timens, W.; Fehrmann, R.S.; Groen, H.J. Immune microenvironment composition in non-small cell lung cancer and its association with survival. Clin. Transl. Immunol. 2020, 9, e1142. [Google Scholar] [CrossRef]
- Jung, K.Y.; Cho, S.W.; Kim, Y.A.; Kim, D.; Oh, B.C.; Park, D.J.; Park, Y.J. Cancers with Higher Density of Tumor-Associated Macrophages Were Associated with Poor Survival Rates. J. Pathol. Transl. Med. 2015, 49, 318–324. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Remark, R.; Becker, C.; Gomez, J.E.; Damotte, D.; Dieu-Nosjean, M.C.; Sautes-Fridman, C.; Fridman, W.H.; Powell, C.A.; Altorki, N.K.; Merad, M.; et al. The non-small cell lung cancer immune contexture. A major determinant of tumor characteristics and patient outcome. Am. J. Respir. Crit. Care Med. 2015, 191, 377–390. [Google Scholar] [CrossRef]
- Ma, J.; Liu, L.; Che, G.; Yu, N.; Dai, F.; You, Z. The M1 form of tumor-associated macrophages in non-small cell lung cancer is positively associated with survival time. BMC Cancer 2010, 10, 112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ohri, C.M.; Shikotra, A.; Green, R.H.; Waller, D.A.; Bradding, P. Macrophages within NSCLC tumour islets are predominantly of a cytotoxic M1 phenotype associated with extended survival. Eur Respir J. 2009, 33, 118–126. [Google Scholar] [CrossRef] [Green Version]
- Zhang, B.C.; Gao, J.; Wang, J.; Rao, Z.G.; Wang, B.C.; Gao, J.F. Tumor-associated macrophages infiltration is associated with peritumoral lymphangiogenesis and poor prognosis in lung adenocarcinoma. Med. Oncol. 2011, 28, 1447–1452. [Google Scholar] [CrossRef] [PubMed]
- Svoronos, A.A.; Engelman, D.M.; Slack, F.J. OncomiR or Tumor Suppressor? The Duplicity of MicroRNAs in Cancer. Cancer Res. 2016, 76, 3666–3670. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, B.; Gao, T.; Yuan, W.; Zhao, W.; Wang, T.H.; Wu, J. Prognostic Value of Survival of MicroRNAs Signatures in Non-small Cell Lung Cancer. J. Cancer 2019, 10, 5793–5804. [Google Scholar] [CrossRef]
- Fadejeva, I.; Olschewski, H.; Hrzenjak, A. MicroRNAs as regulators of cisplatin-resistance in non-small cell lung carcinomas. Oncotarget 2017, 8, 115754–115773. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mehta, A.; Baltimore, D. MicroRNAs as regulatory elements in immune system logic. Nat. Rev. Immunol 2016, 16, 279–294. [Google Scholar] [CrossRef]
- Cho, S.; Tai, J.W.; Lu, L.F. MicroRNAs and Their Targetomes in Tumor-Immune Communication. Cancers 2020, 12, 2025. [Google Scholar] [CrossRef] [PubMed]
- Squadrito, M.L.; Etzrodt, M.; De Palma, M.; Pittet, M.J. MicroRNA-mediated control of macrophages and its implications for cancer. Trends Immunol. 2013, 34, 350–359. [Google Scholar] [CrossRef] [Green Version]
- Xu, S.J.; Hu, H.T.; Li, H.L.; Chang, S. The Role of miRNAs in Immune Cell Development, Immune Cell Activation, and Tumor Immunity: With a Focus on Macrophages and Natural Killer Cells. Cells 2019, 8, 1140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Banerjee, S.; Xie, N.; Cui, H.; Tan, Z.; Yang, S.; Icyuz, M.; Abraham, E.; Liu, G. MicroRNA let-7c regulates macrophage polarization. J. Immunol. 2013, 190, 6542–6549. [Google Scholar] [CrossRef] [PubMed]
- Lu, L.; McCurdy, S.; Huang, S.; Zhu, X.; Peplowska, K.; Tiirikainen, M.; Boisvert, W.A.; Garmire, L.X. Time Series miRNA-mRNA integrated analysis reveals critical miRNAs and targets in macrophage polarization. Sci. Rep. 2016, 6, 37446. [Google Scholar] [CrossRef] [Green Version]
- Gaziel-Sovran, A.; Segura, M.F.; Di Micco, R.; Collins, M.K.; Hanniford, D.; Vega-Saenz de Miera, E.; Rakus, J.F.; Dankert, J.F.; Shang, S.; Kerbel, R.S.; et al. miR-30b/30d regulation of GalNAc transferases enhances invasion and immunosuppression during metastasis. Cancer Cell 2011, 20, 104–118. [Google Scholar] [CrossRef] [Green Version]
- Lin, X.; Wang, S.; Sun, M.; Zhang, C.; Wei, C.; Yang, C.; Dou, R.; Liu, Q.; Xiong, B. miR-195-5p/NOTCH2-mediated EMT modulates IL-4 secretion in colorectal cancer to affect M2-like TAM polarization. J. Hematol. Oncol. 2019, 12, 20. [Google Scholar] [CrossRef] [Green Version]
- Nishino, M.; Jagannathan, J.P.; Ramaiya, N.H.; Van den Abbeele, A.D. Revised RECIST guideline version 1.1: What oncologists want to know and what radiologists need to know. AJR Am. J. Roentgenol. 2010, 195, 281–289. [Google Scholar] [CrossRef]
- Schmittgen, T.D.; Livak, K.J. Analyzing real-time PCR data by the comparative C(T) method. Nat. Protoc. 2008, 3, 1101–1108. [Google Scholar] [CrossRef]
- McShane, L.M.; Altman, D.G.; Sauerbrei, W.; Taube, S.E.; Gion, M.; Clark, G.M. Reporting recommendations for tumor marker prognostic studies (REMARK). J. Natl. Cancer Inst. 2005, 97, 1180–1184. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gyorffy, B.; Surowiak, P.; Budczies, J.; Lanczky, A. Online survival analysis software to assess the prognostic value of biomarkers using transcriptomic data in non-small-cell lung cancer. PLoS ONE 2013, 8, e82241. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cui, M.; Wang, H.; Yao, X.; Zhang, D.; Xie, Y.; Cui, R.; Zhang, X. Circulating MicroRNAs in Cancer: Potential and Challenge. Front. Genet. 2019, 10, 626. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Von Both, U.; Berk, M.; Agapow, P.M.; Wright, J.D.; Git, A.; Hamilton, M.S.; Goldgof, G.; Siddiqui, N.; Bellos, E.; Wright, V.J.; et al. Mycobacterium tuberculosis Exploits a Molecular Off Switch of the Immune System for Intracellular Survival. Sci. Rep. 2018, 8, 661. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.; Duan, Z.; Xu, F.; Zhang, J.; Shulgina, M.V.; Li, F. Construction and analysis of the transcription factor-microRNA co-regulatory network response to Mycobacterium tuberculosis: A view from the blood. Am. J. Transl. Res. 2017, 9, 1962–1976. [Google Scholar]
- Curtale, G.; Rubino, M.; Locati, M. MicroRNAs as Molecular Switches in Macrophage Activation. Front. Immunol. 2019, 10, 799. [Google Scholar] [CrossRef] [Green Version]
- Zhao, Z.; Lv, B.; Zhang, L.; Zhao, N.; Lv, Y. miR-202 functions as a tumor suppressor in non-small cell lung cancer by targeting STAT3. Mol. Med. Rep. 2017, 16, 2281–2289. [Google Scholar] [CrossRef] [PubMed]
- Andersen, M.N.; Etzerodt, A.; Graversen, J.H.; Holthof, L.C.; Moestrup, S.K.; Hokland, M.; Moller, H.J. STAT3 inhibition specifically in human monocytes and macrophages by CD163-targeted corosolic acid-containing liposomes. Cancer Immunol. Immunother 2019, 68, 489–502. [Google Scholar] [CrossRef]
- Deng, X.; Hou, C.; Liang, Z.; Wang, H.; Zhu, L.; Xu, H. miR-202 Suppresses Cell Proliferation by Targeting FOXR2 in Endometrial Adenocarcinoma. Dis. Markers 2017, 2017, 2827435. [Google Scholar] [CrossRef] [Green Version]
- Gao, S.; Cao, C.; Dai, Q.; Chen, J.; Tu, J. miR-202 acts as a potential tumor suppressor in breast cancer. Oncol. Lett. 2018, 16, 1155–1162. [Google Scholar] [CrossRef]
- Jiang, J.; Huang, J.; Wang, X.R.; Quan, Y.H. MicroRNA-202 induces cell cycle arrest and apoptosis in lung cancer cells through targeting cyclin D1. Eur. Rev. Med. Pharmacol. Sci. 2016, 20, 2278–2284. [Google Scholar]
- Sun, W.; Ping, W.; Tian, Y.; Zou, W.; Liu, J.; Zu, Y. miR-202 Enhances the Anti-Tumor Effect of Cisplatin on Non-Small Cell Lung Cancer by Targeting the Ras/MAPK Pathway. Cell Physiol. Biochem. 2018, 51, 2160–2171. [Google Scholar] [CrossRef]
- Kim, J.; Park, S.; Hwang, D.; Kim, S.I.; Lee, H. Diagnostic Value of Circulating miR-202 in Early-Stage Breast Cancer in South Korea. Medicina 2020, 56, 340. [Google Scholar] [CrossRef] [PubMed]
- Joosse, S.A.; Muller, V.; Steinbach, B.; Pantel, K.; Schwarzenbach, H. Circulating cell-free cancer-testis MAGE-A RNA, BORIS RNA, let-7b and miR-202 in the blood of patients with breast cancer and benign breast diseases. Br. J. Cancer 2014, 111, 909–917. [Google Scholar] [CrossRef] [Green Version]
- Yanaihara, N.; Caplen, N.; Bowman, E.; Seike, M.; Kumamoto, K.; Yi, M.; Stephens, R.M.; Okamoto, A.; Yokota, J.; Tanaka, T.; et al. Unique microRNA molecular profiles in lung cancer diagnosis and prognosis. Cancer Cell 2006, 9, 189–198. [Google Scholar] [CrossRef] [Green Version]
- Chai, Z.T.; Zhu, X.D.; Ao, J.Y.; Wang, W.Q.; Gao, D.M.; Kong, J.; Zhang, N.; Zhang, Y.Y.; Ye, B.G.; Ma, D.N.; et al. microRNA-26a suppresses recruitment of macrophages by down-regulating macrophage colony-stimulating factor expression through the PI3K/Akt pathway in hepatocellular carcinoma. J. Hematol. Oncol. 2015, 8, 56. [Google Scholar] [CrossRef] [Green Version]
- Liu, B.; Wu, X.; Liu, B.; Wang, C.; Liu, Y.; Zhou, Q.; Xu, K. MiR-26a enhances metastasis potential of lung cancer cells via AKT pathway by targeting PTEN. Biochim Biophys Acta 2012, 1822, 1692–1704. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, Y.; Zhang, P.; Zhao, Y.; Yang, J.; Jiang, G.; Fan, J. Decreased MicroRNA-26a expression causes cisplatin resistance in human non-small cell lung cancer. Cancer Biol. Ther. 2016, 17, 515–525. [Google Scholar] [CrossRef] [Green Version]
- ParvizHamidi, M.; Haddad, G.; Ostadrahimi, S.; Ostadrahimi, N.; Sadeghi, S.; Fayaz, S.; Fard-Esfahani, P. Circulating miR-26a and miR-21 as biomarkers for glioblastoma multiform. Biotechnol. Appl. Biochem. 2019, 66, 261–265. [Google Scholar] [CrossRef] [PubMed]
- Pacheco Plaza, M.C.; Kessler Nieto, F.; Orts Rodriguez, M.T.; Ruiz de Temino Malo, P. Ultrasonics in endodontics: Mechanism of action. Rev. Esp Endodoncia 1989, 7, 7–12. [Google Scholar]
- Qiu, X.; Zhu, H.; Liu, S.; Tao, G.; Jin, J.; Chu, H.; Wang, M.; Tong, N.; Gong, W.; Zhao, Q.; et al. Expression and prognostic value of microRNA-26a and microRNA-148a in gastric cancer. J. Gastroenterol. Hepatol. 2017, 32, 819–827. [Google Scholar] [CrossRef] [PubMed]
- Song, Q.; Liu, B.; Li, X.; Zhang, Q.; Cao, L.; Xu, M.; Meng, Z.; Wu, X.; Xu, K. MiR-26a-5p potentiates metastasis of human lung cancer cells by regulating ITGbeta8- JAK2/STAT3 axis. Biochem Biophys Res. Commun. 2018, 501, 494–500. [Google Scholar] [CrossRef]
- Wang, N.; Liang, H.; Zen, K. Molecular mechanisms that influence the macrophage m1-m2 polarization balance. Front. Immunol. 2014, 5, 614. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mohrherr, J.; Uras, I.Z.; Moll, H.P.; Casanova, E. STAT3: Versatile Functions in Non-Small Cell Lung Cancer. Cancers 2020, 12, 1107. [Google Scholar] [CrossRef] [PubMed]
- Chen, G.; Wang, J.; Cui, Q. Could circulating miRNAs contribute to cancer therapy? Trends Mol. Med. 2013, 19, 71–73. [Google Scholar] [CrossRef]
- Becker, N.; Lockwood, C.M. Pre-analytical variables in miRNA analysis. Clin. Biochem. 2013, 46, 861–868. [Google Scholar] [CrossRef] [PubMed]
- McDonald, J.S.; Milosevic, D.; Reddi, H.V.; Grebe, S.K.; Algeciras-Schimnich, A. Analysis of circulating microRNA: Preanalytical and analytical challenges. Clin. Chem. 2011, 57, 833–840. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All Patients | SqCC | Non-SqCC | |||||
|---|---|---|---|---|---|---|---|
| Characteristic | N | % | N | % | N | % | p value |
| Number of patients | 125 | 40 | 32.0 | 85 | 68.0 | ||
| Gender | 0.008 a | ||||||
| Male | 108 | 86.4 | 40 | 100.0 | 68 | 63.0 | |
| Female | 17 | 13.6 | 0 | 0.0 | 17 | 37.0 | |
| Age (years) | 0.339 a | ||||||
| median (range) | 65 (37–88) | 66.5 (46–88) | 63.2 (37–82) | ||||
| ECOG PS | 0.354 a | ||||||
| 0 | 31 | 24.8 | 11 | 27.5 | 20 | 23.5 | |
| 1 | 77 | 61.6 | 22 | 55.0 | 55 | 64.7 | |
| 2 | 13 | 10.4 | 7 | 17.5 | 6 | 7.1 | |
| 3 | 4 | 3.2 | 0 | 0.0 | 4 | 4.7 | |
| Stage at diagnosis | 0.004 a | ||||||
| II | 1 | 0.8 | 1 | 2.5 | 0 | 0.0 | |
| III | 4 | 3.2 | 4 | 10 | 0 | 0.0 | |
| IV | 120 | 96 | 35 | 87.5 | 85 | 100.0 | |
| Histology | Ns a | ||||||
| Adenocarcinoma | 77 | 61.6 | |||||
| Squamous | 40 | 32.0 | |||||
| Others | 8 | 6.4 | |||||
| Number of metastatic sites | 0.073 a | ||||||
| 0 | 15 | 12 | 6 | 15.0 | 9 | 10.6 | |
| 1 | 50 | 40 | 21 | 52.5 | 29 | 34.12 | |
| 2 | 33 | 26.4 | 9 | 22.5 | 24 | 28.23 | |
| ≥3 | 27 | 21.6 | 4 | 10.0 | 23 | 27.05 | |
| Chemotherapy regimens | <0.001 a | ||||||
| CDDP/TXT | 46 | 36.8 | 19 | 47.5 | 27 | 31.76 | |
| CDDP/GEM | 33 | 26.4 | 20 | 50.0 | 13 | 15.3 | |
| CDDP/PEM | 44 | 35.2 | 1 | 2.5 | 43 | 50.59 | |
| CDDP/other | 2 | 1.6 | 2 | 2.35 | |||
| Response | 0.715 a | ||||||
| PR | 33 | 26.4 | 13 | 32.5 | 20 | 23.53 | |
| SD | 49 | 39.2 | 14 | 35.0 | 35 | 41.17 | |
| PD | 43 | 34.4 | 13 | 32.5 | 30 | 35.3 | |
| Univariate Analysis | ||
|---|---|---|
| Binary Logistic Regression | OR (95% CI) | p Value |
| Age (<65 vs. ≥65) | 1.130 (0.537–2.379) | 0.747 |
| Gender (male vs. female) | 1.460 (0.513–4.158) | 0.477 |
| ECOG PS (≥2 vs. 0–1) | 1.460 (0.513–4.158) | 0.477 |
| Stage at Diagnosis (IV vs. <IV) | 1.333 (0.214–8.304) | 0.757 |
| Histology (SqCC vs. non-SqCC) | 1.620 (0.306–8.583) | 0.571 |
| No. of Metastatic Sites (≥3 vs. 0–2) | 2.209 (0.925–5.277) | 0.074 |
| Brain Metastases | 1.014 (0.352–2.924) | 0.979 |
| Liver Metastases | 1.877 (0.801–4.399) | 0.144 |
| Bone Metastases | 1.289 (0.587–2.829) | 0.527 |
| let-7c (high vs. low) | 1.201 (0.552–2.615) | 0.644 |
| miR-26a (high vs. low) | 1.026 (0.476–2.211) | 0.947 |
| miR-30d (high vs. low) | 1.422 (0.662–3.056) | 0.366 |
| miR-98 (high vs. low) | 1.071 (0.445–2.577) | 0.878 |
| miR-195 (high vs. low) | 1.047 (0.480–2.284) | 0.908 |
| miR-202 (high vs. low) | 2.335 (1.038–5.254) | 0.040 * |
| Univariate Analysis | ||
| Cox Regression | HR (95% CI) | p Value |
| Age (<65 vs. ≥65) | 1.179 (0.824–1.688) | 0.368 |
| Gender (male vs. female) | 1.831 (1.089–3.078) | 0.023 * |
| ECOG PS (≥2 vs. 0–1) | 1.210 (0.724–2.025) | 0.467 |
| Stage at Diagnosis (IV vs. <IV) | 1.069 (0.435–2.625) | 0.884 |
| Histology (SqCC vs. non-SqCC) | 1.223 (0.826–1.812) | 0.315 |
| No. of Metastatic Sites (≥3 vs. 0–2) | 2.014 (1.301–3.118) | 0.002 * |
| Brain Metastases (yes vs. no) | 1.226 (0.742–2.028) | 0.426 |
| Liver Metastases (yes vs. no) | 2.192 (1.413–3.402) | <0.001 * |
| Bone Metastases (yes vs. no) | 1.168 (0.796–1.713) | 0.428 |
| let-7c (high vs. low) | 1.206 (0.830–1.752) | 0.327 |
| miR-26a (high vs. low) | 1.110 (0.765–1.610) | 0.584 |
| miR-30d (high vs. low) | 1.113 (0.769–1.610) | 0.571 |
| miR-98 (high vs. low) | 1.086 (0.718–1.641) | 0.696 |
| miR-195 (high vs. low) | 1.086 (0.751–1.571) | 0.662 |
| miR-202 (high vs. low) | 1.455 (1.000–2.118) | 0.048 * |
| Multivariate Analysis | ||
| Cox Regression | HR (95% CI) | p Value |
| Gender (male vs. female) | 2.232 (1.262–3.946) | 0.006 * |
| No. of Metastatic Sites (≥3 vs. 0–2) | 1.537 (0.924–2.556) | 0.097 |
| Liver Metastases (yes vs. no) | 1.877 (1.139–3.094) | 0.014 * |
| miR-202 (high vs. low) | 1.564 (1.068–2.289) | 0.021 * |
| Univariate Analysis | ||
| Cox Regression | HR (95% CI) | p Value |
| Age (<65 vs. ≥65) | 1.214 (0.846–1.742) | 0.292 |
| Gender (male vs. female) | 1.546 (0.933–2.622) | 0.090 |
| ECOG PS (≥2 vs. 0–1) | 2.289 (1.353–3.871) | 0.002 * |
| Stage at Diagnosis (IV vs. <IV) | 1.542 (0.627–3.793) | 0.346 |
| Histology (SqCC vs. non-SqCC) | 1.262 (0.850–1.874) | 0.249 |
| No. of Metastatic Sites (≥3 vs. 0–2) | 1.589 (1.028–2.456) | 0.037 * |
| Brain Metastases (yes vs. no) | 1.082 (0.653–1.793) | 0.759 |
| Liver Metastases (yes vs. no) | 1.826 (1.190–2.802) | 0.006 * |
| Bone Metastases (yes vs. no) | 1.416 (0.965–2.078) | 0.075 |
| let-7c (high vs. low) | 1.050 (0.724–1.524) | 0.797 |
| miR-26a (high vs. low) | 1.329 (0.907–1.946) | 0.145 |
| miR-30d (high vs. low) | 1.251 (0.865–1.809) | 0.235 |
| miR-98 (high vs. low) | 1.101 (0.725–1.673) | 0.651 |
| miR-195 (high vs. low) | 1.307 (0.894–1.911) | 0.167 |
| miR-202 (high vs. low) | 1.596 (1.074–2.292) | 0.020 * |
| Multivariate Analysis | ||
| Cox Regression | HR (95% CI) | p Value |
| ECOG PS (≥2 vs. 0–1) | 2.065 (1.215–3.581) | 0.008 * |
| No. of Metastatic Sites (≥3 vs. 0–2) | 1.230 (0.751–2.016) | 0.410 |
| Liver Metastases (yes vs. no) | 1.666 (1.033–2.687) | 0.036 * |
| miR-202 (high vs. low) | 1.558 (1.060–2.291) | 0.024 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Monastirioti, A.; Papadaki, C.; Rounis, K.; Kalapanida, D.; Mavroudis, D.; Agelaki, S. A Prognostic Role for Circulating microRNAs Involved in Macrophage Polarization in Advanced Non-Small Cell Lung Cancer. Cells 2021, 10, 1988. https://doi.org/10.3390/cells10081988
Monastirioti A, Papadaki C, Rounis K, Kalapanida D, Mavroudis D, Agelaki S. A Prognostic Role for Circulating microRNAs Involved in Macrophage Polarization in Advanced Non-Small Cell Lung Cancer. Cells. 2021; 10(8):1988. https://doi.org/10.3390/cells10081988
Chicago/Turabian StyleMonastirioti, Alexia, Chara Papadaki, Konstantinos Rounis, Despoina Kalapanida, Dimitrios Mavroudis, and Sofia Agelaki. 2021. "A Prognostic Role for Circulating microRNAs Involved in Macrophage Polarization in Advanced Non-Small Cell Lung Cancer" Cells 10, no. 8: 1988. https://doi.org/10.3390/cells10081988
APA StyleMonastirioti, A., Papadaki, C., Rounis, K., Kalapanida, D., Mavroudis, D., & Agelaki, S. (2021). A Prognostic Role for Circulating microRNAs Involved in Macrophage Polarization in Advanced Non-Small Cell Lung Cancer. Cells, 10(8), 1988. https://doi.org/10.3390/cells10081988