
Combined Analysis of Early CD4+ T Cell Counts and CMV Serostatus May Improve CMV Risk Assessment after Allogeneic Hematopoietic Cell Transplantation

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Population
2.2. Patient Assessment
2.3. CMV Monitoring
2.4. Flow Cytometry
2.5. Unsupervised Clustering of CD4+ Helper T Cells
2.6. Statistical Analysis
3. Results
3.1. Patient Characteristics
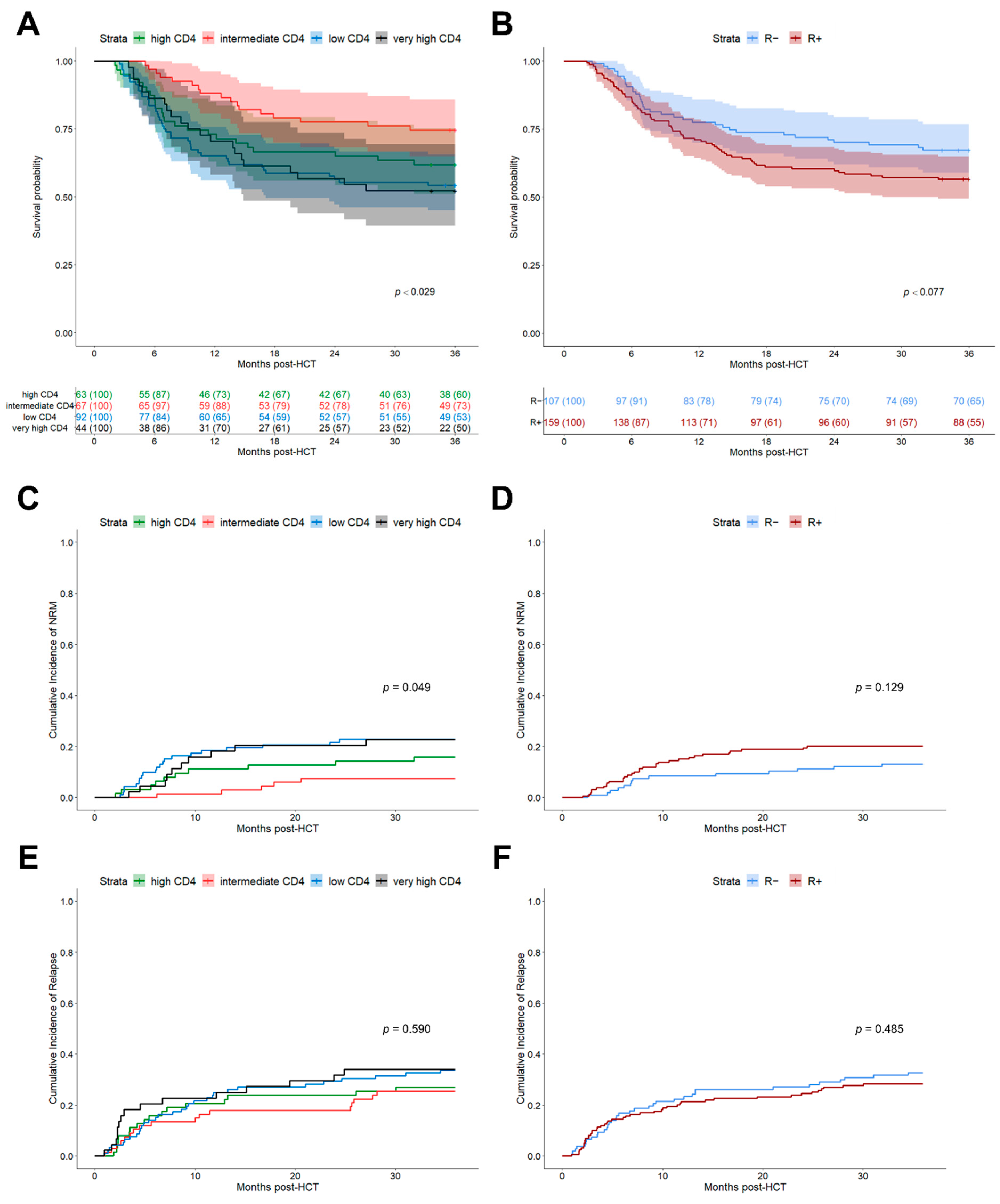
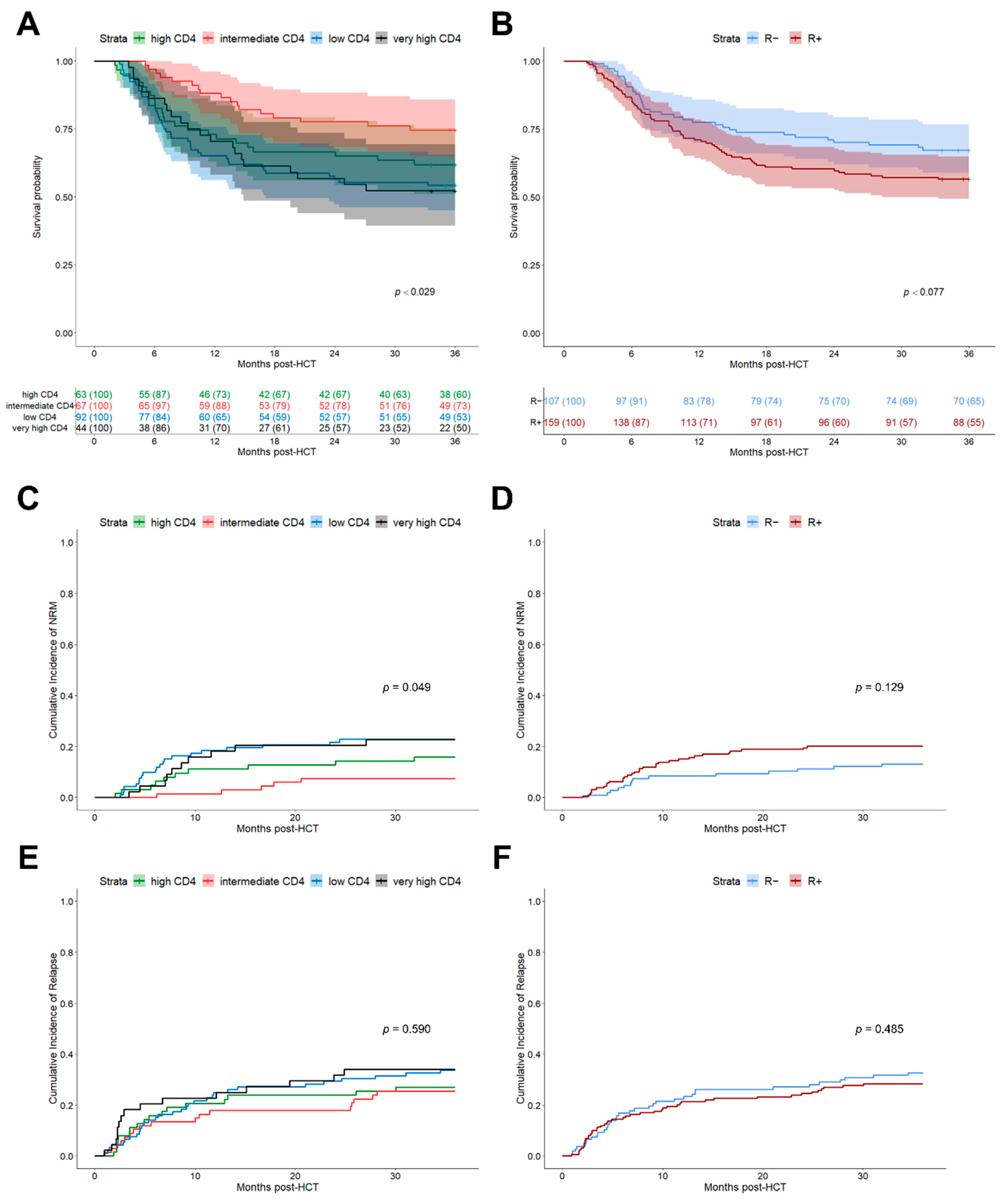
3.2. Improved Outcome Prognosis Based on K-Means CD4+ Helper T Cell Clusters
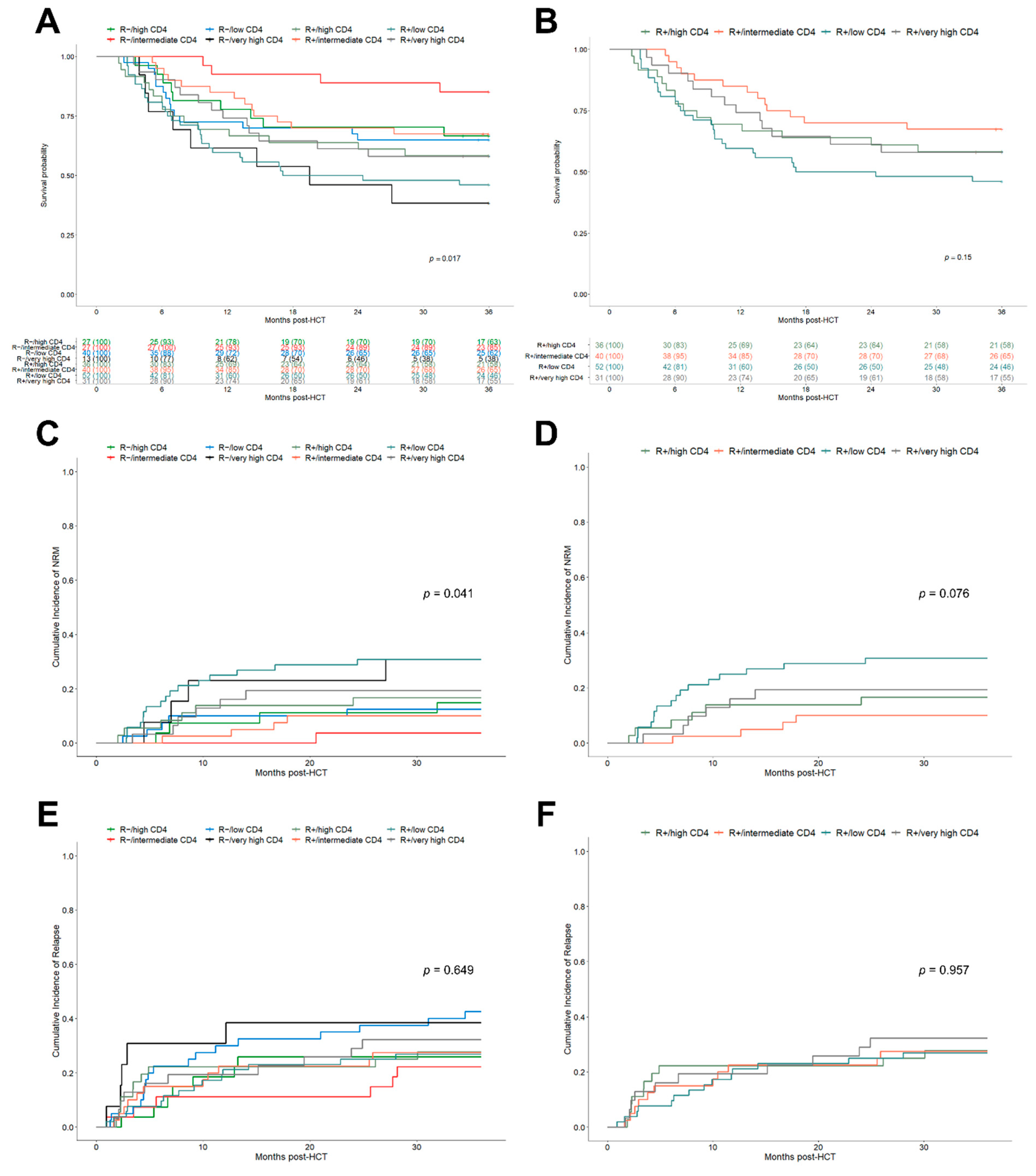
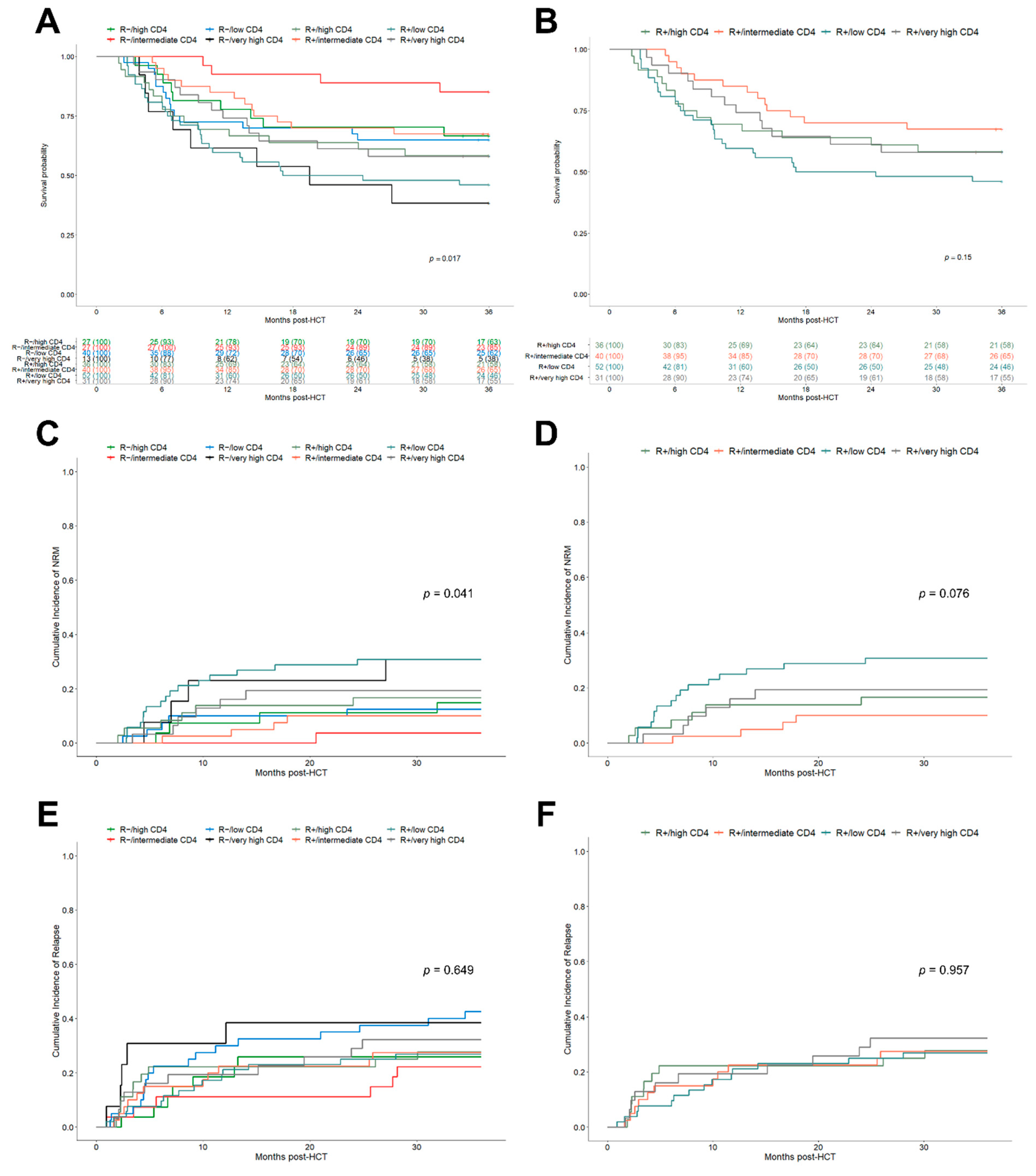
3.3. Stratification of Helper T Cell Clusters by Recipient Serostatus Further Improves Clinical Prognosis
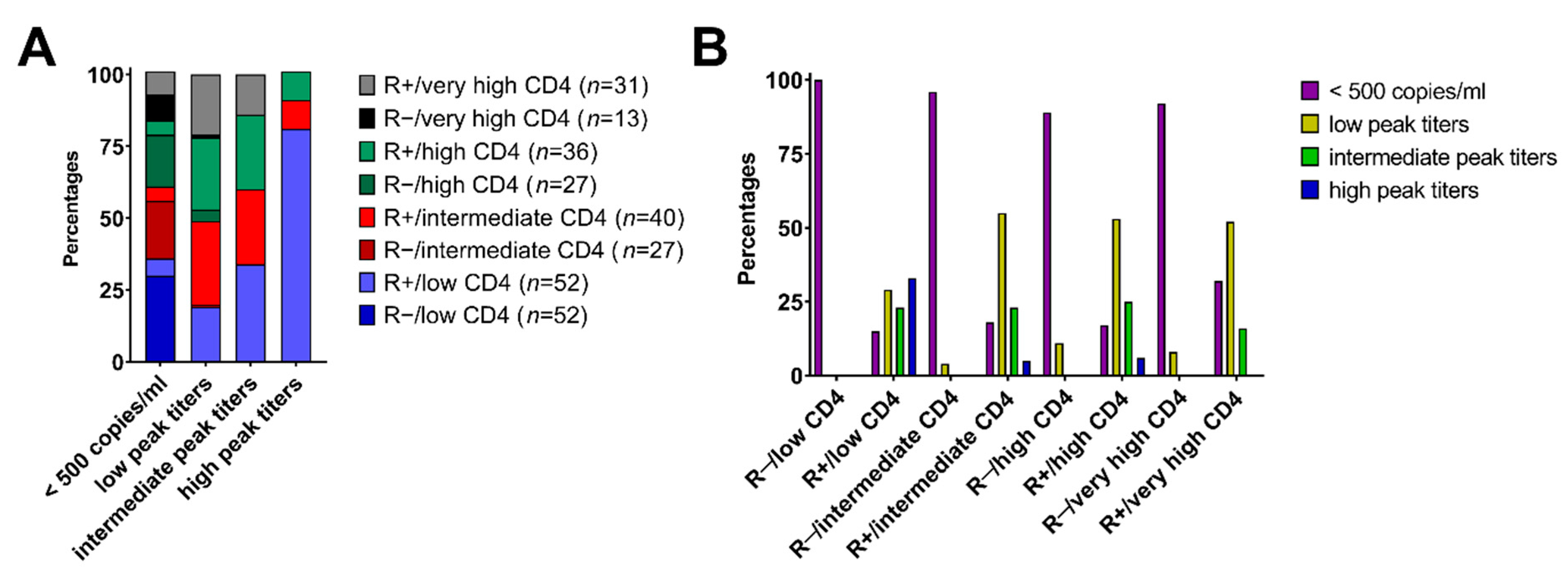
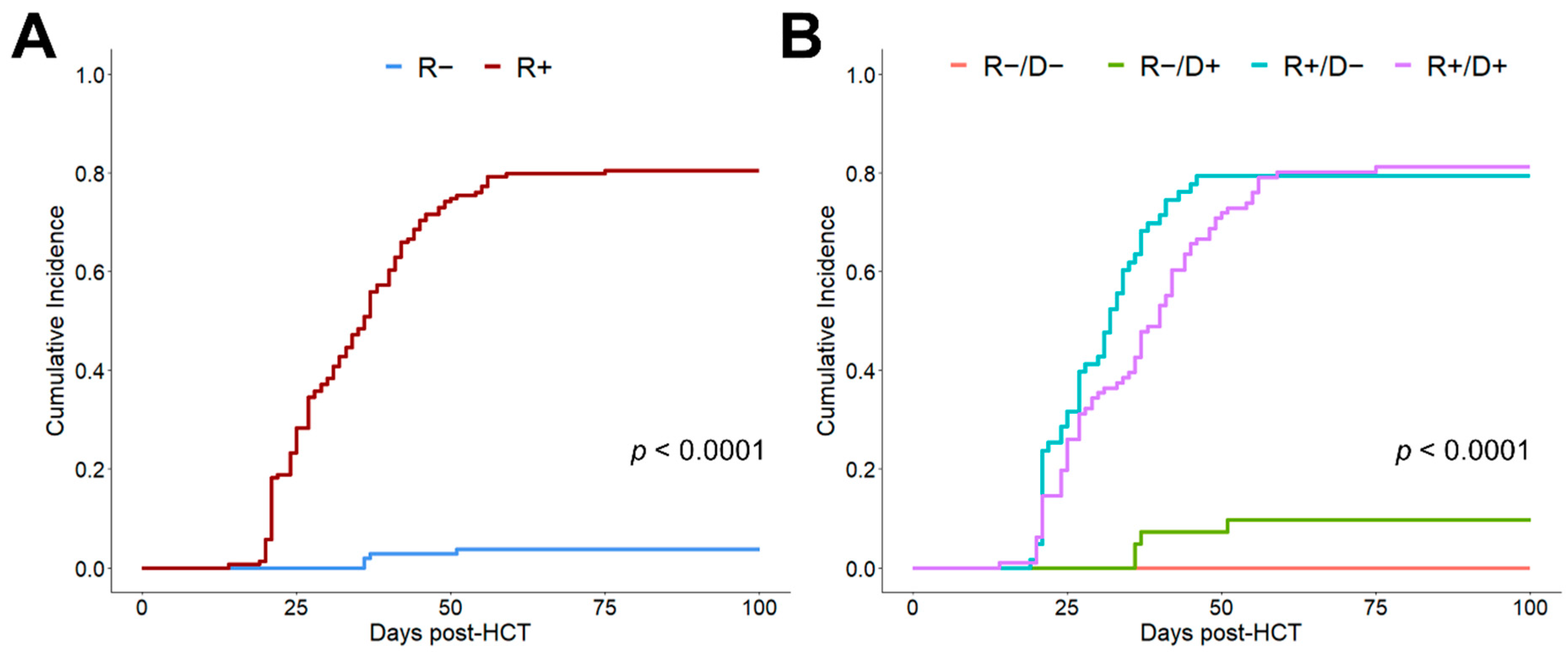
3.4. Combined R Serostatus/Helper T Cell Clusters Associate with Clinically Relevant CMV Reactivation
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Einsele, H.; Ljungman, P.T.; Boeckh, M.J. How I treat CMV reactivation after allogeneic hematopoietic stem cell transplantation. Blood 2020, 135, 1619–1629. [Google Scholar] [CrossRef] [PubMed]
- Marty, F.; Ljungman, P.; Chemaly, R.F.; Maertens, J.; Dadwal, S.S.; Duarte, R.F.; Haider, S.; Ullmann, A.J.; Katayama, Y.; Brown, J.; et al. Letermovir Prophylaxis for Cytomegalovirus in Hematopoietic-Cell Transplantation. N. Engl. J. Med. 2017, 377, 2433–2444. [Google Scholar] [CrossRef] [PubMed]
- Emerson, R.; DeWitt, W.S.; Vignali, M.; Gravley, J.; Hu, J.K.; Osborne, E.J.; Desmarais, C.; Klinger, M.; Carlson, C.S.; A Hansen, J.; et al. Immunosequencing identifies signatures of cytomegalovirus exposure history and HLA-mediated effects on the T cell repertoire. Nat. Genet. 2017, 49, 659–665. [Google Scholar] [CrossRef]
- Suessmuth, Y.; Mukherjee, R.; Watkins, B.; Koura, D.; Finstermeier, K.; Desmarais, C.; Stempora, L.; Horan, J.; Langston, A.; Qayed, M.; et al. CMV reactivation drives post-transplant T cell reconstitution and results in defects in the underlying TCRβ repertoire. Blood 2015, 125, 3835–3850. [Google Scholar] [CrossRef]
- Leserer, S.; Bayraktar, E.; Trilling, M.; Bogdanov, R.; Arrieta-Bolaños, E.; Tsachakis-Mück, N.; Crivello, P.; Koldehoff, M.; Maaßen, F.; Ross, R.S.; et al. Cytomegalovirus kinetics after hematopoietic cell transplantation reveal peak titers with differential impact on mortality, relapse and immune reconstitution. Am. J. Hematol. 2021, 96, 436–445. [Google Scholar] [CrossRef]
- Duke, E.R.; Williamson, B.D.; Borate, B.; Golob, J.L.; Wychera, C.; Stevens-Ayers, T.; Huang, M.-L.; Cossrow, N.; Wan, H.; Mast, T.C.; et al. CMV viral load kinetics as surrogate endpoints after allogeneic transplantation. J. Clin. Investig. 2021, 131. [Google Scholar] [CrossRef]
- Stern, A.; Su, Y.; Dumke, H.; Fang, J.; Tamari, R.; Jakubowski, A.; Cho, C.; Giralt, S.; Perales, M.-A.; A Papanicolaou, G. Cytomegalovirus Viral Load Kinetics Predict Cytomegalovirus End-Organ Disease and Mortality After Hematopoietic Cell Transplant. J. Infect. Dis. 2021, 224, 620–631. [Google Scholar] [CrossRef] [PubMed]
- Fabrizio, V.A.; Rodriguez-Sanchez, M.I.; Mauguen, A.; Dahi, P.B.; Doubrovina, E.; O’Reilly, R.J.; Prockop, S.E. Adoptive therapy with CMV-specific cytotoxic T lymphocytes depends on baseline CD4+ immunity to mediate durable responses. Blood Adv. 2021, 5, 496–503. [Google Scholar] [CrossRef]
- Teira, P.; Battiwalla, M.; Ramanathan, M.; Barrett, A.J.; Ahn, K.W.; Chen, M.; Green, J.S.; Saad, A.; Antin, J.H.; Savani, B.N.; et al. Early cytomegalovirus reactivation remains associated with increased transplant-related mortality in the current era: A CIBMTR analysis. Blood 2016, 127, 2427–2438. [Google Scholar] [CrossRef]
- Ljungman, P.; Brand, R.; Hoek, J.; de la Camara, R.; Cordonnier, C.; Einsele, H.; Styczynski, J.; Ward, K.N.; Cesaro, S. Donor Cytomegalovirus Status Influences the Outcome of Allogeneic Stem Cell Transplant: A Study by the European Group for Blood and Marrow Transplantation. Clin. Infect. Dis. 2014, 59, 473–481. [Google Scholar] [CrossRef] [Green Version]
- Bartelink, I.H.; Belitser, S.V.; Knibbe, C.A.; Danhof, M.; de Pagter, A.J.; Egberts, T.; Boelens, J.J. Immune Reconstitution Kinetics as an Early Predictor for Mortality using Various Hematopoietic Stem Cell Sources in Children. Biol. Blood Marrow Transplant. 2013, 19, 305–313. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Small, T.N.; Papadopoulos, E.B.; Boulad, F.; Black, P.; Castro-Malaspina, H.; Childs, B.H.; Collins, N.; Gillio, A.; George, D.; Jakubowski, A.; et al. Comparison of Immune Reconstitution after Unrelated and Related T-Cell–Depleted Bone Marrow Transplantation: Effect of Patient Age and Donor Leukocyte Infusions. Blood 1999, 93, 467–480. [Google Scholar] [CrossRef]
- Ogonek, J.; Juric, M.K.; Ghimire, S.; Varanasi, P.; Holler, E.; Greinix, H.; Weissinger, E. Immune Reconstitution after Allogeneic Hematopoietic Stem Cell Transplantation. Front. Immunol. 2016, 7, 507. [Google Scholar] [CrossRef] [Green Version]
- Admiraal, R.; Lindemans, C.A.; van Kesteren, C.; Bierings, M.B.; Versluijs, A.B.; Nierkens, S.; Boelens, J.J. Excellent T-cell reconstitution and survival depend on low ATG exposure after pediatric cord blood transplantation. Blood 2016, 128, 2734–2741. [Google Scholar] [CrossRef] [Green Version]
- de Koning, C.; Prockop, S.; van Roessel, I.; Kernan, N.; Klein, E.; Langenhorst, J.; Szanto, C.; Belderbos, M.; Bierings, M.; Boulad, F.; et al. CD4+ T-cell reconstitution predicts survival outcomes after acute graft-versus-host-disease: A dual-center validation. Blood 2021, 137, 848–855. [Google Scholar] [CrossRef]
- Waller, E.K.; Logan, B.R.; Fei, M.; Lee, S.J.; Confer, D.; Howard, A.; Chandrakasan, S.; Anasetti, C.; Fernando, S.M.; Giver, C.R. Kinetics of immune cell reconstitution predict survival in allogeneic bone marrow and G-CSF–mobilized stem cell transplantation. Blood Adv. 2019, 3, 2250–2263. [Google Scholar] [CrossRef]
- Storb, R.; Deeg, H.J.; Whitehead, J.; Appelbaum, F.; Beatty, P.; Bensinger, W.; Buckner, C.D.; Clift, R.; Doney, K.; Farewell, V.; et al. Methotrexate and Cyclosporine Compared with Cyclosporine Alone for Prophylaxis of Acute Graft versus Host Disease after Marrow Transplantation for Leukemia. N. Engl. J. Med. 1986, 314, 729–735. [Google Scholar] [CrossRef]
- Beelen, D.W.; Quabeck, K.; Kaiser, B.; Wiefelopütz, J.; Scheulen, M.E.; Graeven, U.; Grosse-Wilde, H.; Sayer, H.G.; Schaefer, U.W. Six Weeks of Continuous Intravenous Cyclosporine and Short-Course Methotrexate as Prophylaxis for Acute Graft-Versus-Host Disease after Allogeneic Bone Marrow Transplantation. Transplantation 1990, 50, 421–426. [Google Scholar] [CrossRef]
- Przepiorka, D.; Weisdorf, D.; Martin, P.; Klingemann, H.G.; Beatty, P.; Hows, J.; Thomas, E.D. 1994 Consensus Conference on Acute GVHD Grading. Bone Marrow Transplant. 1995, 15, 825–828. [Google Scholar] [PubMed]
- Kaplan, E.L.; Meier, P. Nonparametric Estimation from Incomplete Observations. J. Am. Stat. Assoc. 1958, 53, 457–481. [Google Scholar] [CrossRef]
- Cox, D.R. Regression Models and Life-Tables. J. R. Stat. Soc. Series B Stat. Methodol. 1972, 34, 187–220. [Google Scholar] [CrossRef]
- Fine, J.P.; Gray, R.J. A Proportional Hazards Model for the Subdistribution of a Competing Risk. J. Am. Stat. Assoc. 1999, 94, 496. [Google Scholar] [CrossRef]
- R: A Language and Environment for Statistical Computing, version 4.0.4; R Core Team, R Foundation for Statistical Computing: Vienna, Austria, 2021.
- A Package for Survival Analysis in R, version 3.2-11; Therneau, T. (Ed.) R Foundation for Statistical Computing: Vienna, Austria, 2021. [Google Scholar]
- Survminer: Drawing Survival Curves Using ′ggplot2′, R package version 0.4.9; Kassambara, A.; Kosinski, M.; Biecek, P. (Eds.) R Foundation for Statistical Computing: Vienna, Austria, 2021. [Google Scholar]
- cmprsk: Subdistribution Analysis of Competing Risks, R package version 2.2-10; Gray, B. (Ed.) R Foundation for Statistical Computing: Vienna, Austria, 2020. [Google Scholar]
- Wickham, H. ggplot2: Elegant Graphics for Data Analysis; Springer: New York, NY, USA, 2016. [Google Scholar]
- Schmidt-Hieber, M.; Labopin, M.; Beelen, D.; Volin, L.; Ehninger, G.; Finke, J.; Socié, G.; Schwerdtfeger, R.; Kröger, N.; Ganser, A.; et al. CMV serostatus still has an important prognostic impact in de novo acute leukemia patients after allogeneic stem cell transplantation: A report from the Acute Leukemia Working Party of EBMT. Blood 2013, 122, 3359–3364. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, D.H.; Sohn, S.K.; Won, D.I.; Lee, N.Y.; Suh, J.S.; Lee, K.B. Rapid helper T-cell recovery above 200 x 10 6/l at 3 months correlates to successful transplant outcomes after allogeneic stem cell transplantation. Bone Marrow Transplant. 2006, 37, 1119–1128. [Google Scholar] [CrossRef] [Green Version]
- Peric, Z.; Wilson, J.; Durakovic, N.; Ostojic, A.; Desnica, L.; Vranjes, V.R.; Marekovic, I.; Serventi-Seiwerth, R.; Vrhovac, R. Early human cytomegalovirus reactivation is associated with lower incidence of relapse of myeloproliferative disorders after allogeneic hematopoietic stem cell transplantation. Bone Marrow Transplant. 2018, 53, 1450–1456. [Google Scholar] [CrossRef] [PubMed]
- Admiraal, R.; de Koning, C.; Lindemans, C.A.; Bierings, M.B.; Wensing, A.M.; Versluys, A.B.; Wolfs, T.F.; Nierkens, S.; Boelens, J.J. Viral reactivations and associated outcomes in the context of immune reconstitution after pediatric hematopoietic cell transplantation. J. Allergy Clin. Immunol. 2017, 140, 1643–1650.e9. [Google Scholar] [CrossRef] [Green Version]
- Bejanyan, N.; Brunstein, C.G.; Cao, Q.; Lazaryan, A.; Luo, X.; Curtsinger, J.; Mehta, R.S.; Warlick, E.; Cooley, S.A.; Blazar, B.R.; et al. Delayed immune reconstitution after allogeneic transplantation increases the risks of mortality and chronic GVHD. Blood Adv. 2018, 2, 909–922. [Google Scholar] [CrossRef]
- Fedele, R.; Martino, M. The impact of early CD4+ lymphocyte recovery on the outcome of patients who undergo allogeneic bone marrow or peripheral blood stem cell transplantation. Blood Transfus. 2012, 10, 174–180. [Google Scholar] [CrossRef]
- van Roessel, I.; Prockop, S.; Klein, E.; Boulad, F.; Scaradavou, A.; Spitzer, B.; Kung, A.; Curran, K.; O’Reilly, R.J.; Kernan, N.A.; et al. Early CD4+ T cell reconstitution as predictor of outcomes after allogeneic hematopoietic cell transplantation. Cytotherapy 2020, 22, 503–510. [Google Scholar] [CrossRef]
- Admiraal, R.; van Kesteren, C.; Jol-van der Zijde, C.M.; Lankester, A.C.; Bierings, M.B.; Egberts, T.C.G.; van Tol, M.J.D.; Knibbe, C.A.J.; Bredius, R.G.M.; Boelens, J.J. Association between anti-thymocyte globulin exposure and CD4+ immune reconstitution in paediatric haemopoietic cell transplantation: A multicentre, retrospective pharmacodynamic cohort analysis. Lancet Haematol. 2015, 2, e194–e203. [Google Scholar] [CrossRef]
- Stern, L.; Withers, B.; Avdic, S.; Gottlieb, D.; Abendroth, A.; Blyth, E.; Slobedman, B. Human Cytomegalovirus Latency and Reactivation in Allogeneic Hematopoietic Stem Cell Transplant Recipients. Front. Microbiol. 2019, 10, 1186. [Google Scholar] [CrossRef] [Green Version]
- Ghimire, S.; Weber, D.; Mavin, E.; Wang, X.N.; Dickinson, A.M.; Holler, E. Pathophysiology of GvHD and Other HSCT-Related Major Complications. Front. Immunol. 2017, 8, 79. [Google Scholar] [CrossRef] [Green Version]
- Turki, A.T.; Klisanin, V.; Bayraktar, E.; Kordelas, L.; Trenschel, R.; Ottinger, H.; Steckel, N.K.; Tsachakis-Mück, N.; Leserer, S.; Ditschkowski, M.; et al. Optimizing anti-T-lymphocyte globulin dosing to improve long-term outcome after unrelated hematopoietic cell transplantation for hematologic malignancies. Arab. Archaeol. Epigr. 2019, 20, 677–688. [Google Scholar] [CrossRef]
- Martins, J.P.; Andoniou, C.E.; Fleming, P.; Kuns, R.D.; Schuster, I.S.; Voigt, V.; Daly, S.; Varelias, A.; Tey, S.K.; Degli-Esposti, M.A.; et al. Strain-specific antibody therapy prevents cytomegalovirus reactivation after transplantation. Science 2019, 363, 288–293. [Google Scholar] [CrossRef] [Green Version]
- Raanani, P.; Gafter-Gvili, A.; Paul, M.; Ben-Bassat, I.; Leibovici, L.; Shpilberg, O. Immunoglobulin Prophylaxis in Hematopoietic Stem Cell Transplantation: Systematic Review and Meta-Analysis. J. Clin. Oncol. 2009, 27, 770–781. [Google Scholar] [CrossRef] [Green Version]
- Tomblyn, M.; Chiller, T.; Einsele, H.; Gress, R.; Sepkowitz, K.; Storek, J.; Wingard, J.R.; Young, J.-A.; Boeckh, M.A. Guidelines for Preventing Infectious Complications among Hematopoietic Cell Transplantation Recipients: A Global Perspective. Biol. Blood Marrow Transplant. 2009, 15, 1143–1238. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Swain, S.L.; McKinstry, K.K.; Strutt, T.M. Expanding roles for CD4+ T cells in immunity to viruses. Nat. Rev. Immunol. 2012, 12, 136–148. [Google Scholar] [CrossRef]
- Schmidt-Hieber, M.; Tridello, G.; Ljungman, P.; Mikulska, M.; Knelange, N.; Blaise, D.; Socié, G.; Volin, L.; Blijlevens, N.; Fegueux, N.; et al. The prognostic impact of the cytomegalovirus serostatus in patients with chronic hematological malignancies after allogeneic hematopoietic stem cell transplantation: A report from the Infectious Diseases Working Party of EBMT. Ann. Hematol. 2019, 98, 1755–1763. [Google Scholar] [CrossRef] [PubMed]
- Flach, P.A. ROC Analysis. In Encyclopedia of Machine Learning and Data Mining; Sammut, C., Webb, G.I., Eds.; Springer: Boston, MA, USA, 2016; pp. 1–8. [Google Scholar]
- Petersen, S.L.; Ryder, L.P.; Björk, P.; O Madsen, H.; Heilmann, C.; Jacobsen, N.; Sengelov, H.; Vindeløv, L.L. A comparison of T-, B- and NK-cell reconstitution following conventional or nonmyeloablative conditioning and transplantation with bone marrow or peripheral blood stem cells from human leucocyte antigen identical sibling donors. Bone Marrow Transplant. 2003, 32, 65–72. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | n | % |
|---|---|---|
| Total enrolled and treated | 266 | 100 |
| Median age at transplantation (range) | 53 | (18–76) |
| Female sex | 115 | 43 |
| Disease | ||
| Acute myeloid leukemia | 117 | 44 |
| Myelodysplastic syndrome | 21 | 8 |
| Acute lymphoblastic leukemia | 29 | 11 |
| Chronic myeloid leukemia | 12 | 5 |
| Chronic lymphocytic leukemia | 5 | 2 |
| Chronic myelomonocytic leukemia | 4 | 2 |
| Non-Hodgkin lymphoma | 30 | 11 |
| Hodgkin lymphoma | 5 | 2 |
| Multiple myeloma | 17 | 6 |
| Myeloproliferative disorders | 18 | 7 |
| Other hematologic disorders | 8 | 3 |
| Graft source | ||
| PBSC | 254 | 95 |
| BM | 12 | 5 |
| Donor Type | ||
| MRD | 70 | 26 |
| MMRD | 2 | 1 |
| MUD | 153 | 58 |
| MMUD | 41 | 15 |
| Recipient/Donor sex constellation | ||
| Female/Female | 62 | 23 |
| Male/Male | 115 | 43 |
| Female/Male | 53 | 20 |
| Male/Female | 36 | 14 |
| CMV Serostatus | ||
| R+/D− | 63 | 24 |
| R+/D+ | 96 | 36 |
| R−/D+ | 41 | 15 |
| R−/D− | 66 | 25 |
| Conditioning | ||
| MAC | 110 | 41 |
| RIC | 156 | 59 |
| TBI | 101 | 38 |
| ATG | 189 | 71 |
| Low CD4+ n (%) | Intermediate CD4+ n (%) | High CD4+ n (%) | Very High CD4+ n (%) | p | |
|---|---|---|---|---|---|
| No aGVHD | 10 (11) | 11 (16) | 7 (11) | 11 (25) | 0.132 |
| aGVHD | 82 (89) | 56 (84) | 56 (89) | 33 (75) | |
| No aGVHD | 10 (11) | 11 (16) | 7 (11) | 11 (25) | 0.341 |
| Grade I | 32 (35) | 24 (36) | 28 (44) | 15 (34) | |
| Grade II | 40 (43) | 27 (40) | 24 (38) | 16 (36) | |
| Grade III | 7 (8) | 5 (7) | 1 (2) | 1 (2) | |
| Grade IV | 3 (3) | 0 (0) | 3 (5) | 1 (2) |
| Outcome | n (%) | Competing Risk Regression | ||
|---|---|---|---|---|
| SHR | 95% CI | p | ||
| Relapse ‡ | ||||
| R−/intermediate CD4 | 27 (10) | — | — | — |
| R−/low CD4 | 40 (15) | 2.18 | 0.89–5.38 | 0.090 |
| R+/low CD4 | 52 (20) | 1.27 | 0.50–3.23 | 0.620 |
| R+/intermediate CD4 | 40 (15) | 1.32 | 0.50–3.52 | 0.570 |
| R−/high CD4 | 27 (10) | 1.21 | 0.42–3.51 | 0.720 |
| R+/high CD4 | 36 (14) | 1.38 | 0.50–3.76 | 0.530 |
| R−/very high CD4 | 13 (5) | 2.20 | 0.64–7.57 | 0.210 |
| R+/very high CD4 | 31 (12) | 1.60 | 0.59–4.31 | 0.360 |
| NRM ‡ | ||||
| R−/intermediate CD4 | 27 (10) | — | — | — |
| R−/low CD4 | 40 (15) | 3.64 | 0.44–30.40 | 0.230 |
| R+/low CD4 | 52 (20) | 10.1 | 1.38–73.80 | 0.023 |
| R+/intermediate CD4 | 40 (15) | 2.78 | 0.32–23.90 | 0.350 |
| R−/high CD4 | 27 (10) | 4.22 | 0.49–36.40 | 0.190 |
| R+/high CD4 | 36 (14) | 4.97 | 0.61–40.20 | 0.130 |
| R−/very high CD4 | 13 (5) | 9.57 | 1.12–81.90 | 0.039 |
| R+/very high CD4 | 31 (12) | 5.71 | 0.71–45.80 | 0.100 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Leserer, S.; Arrieta-Bolaños, E.; Buttkereit, U.; Beelen, D.W.; Turki, A.T. Combined Analysis of Early CD4+ T Cell Counts and CMV Serostatus May Improve CMV Risk Assessment after Allogeneic Hematopoietic Cell Transplantation. Cells 2021, 10, 3318. https://doi.org/10.3390/cells10123318
Leserer S, Arrieta-Bolaños E, Buttkereit U, Beelen DW, Turki AT. Combined Analysis of Early CD4+ T Cell Counts and CMV Serostatus May Improve CMV Risk Assessment after Allogeneic Hematopoietic Cell Transplantation. Cells. 2021; 10(12):3318. https://doi.org/10.3390/cells10123318
Chicago/Turabian StyleLeserer, Saskia, Esteban Arrieta-Bolaños, Ulrike Buttkereit, Dietrich W. Beelen, and Amin T. Turki. 2021. "Combined Analysis of Early CD4+ T Cell Counts and CMV Serostatus May Improve CMV Risk Assessment after Allogeneic Hematopoietic Cell Transplantation" Cells 10, no. 12: 3318. https://doi.org/10.3390/cells10123318
APA StyleLeserer, S., Arrieta-Bolaños, E., Buttkereit, U., Beelen, D. W., & Turki, A. T. (2021). Combined Analysis of Early CD4+ T Cell Counts and CMV Serostatus May Improve CMV Risk Assessment after Allogeneic Hematopoietic Cell Transplantation. Cells, 10(12), 3318. https://doi.org/10.3390/cells10123318