
Autologous Stem Cell Therapy for Chronic Lower Extremity Wounds: A Meta-Analysis of Randomized Controlled Trials


Abstract
:1. Introduction
2. Materials and Methods
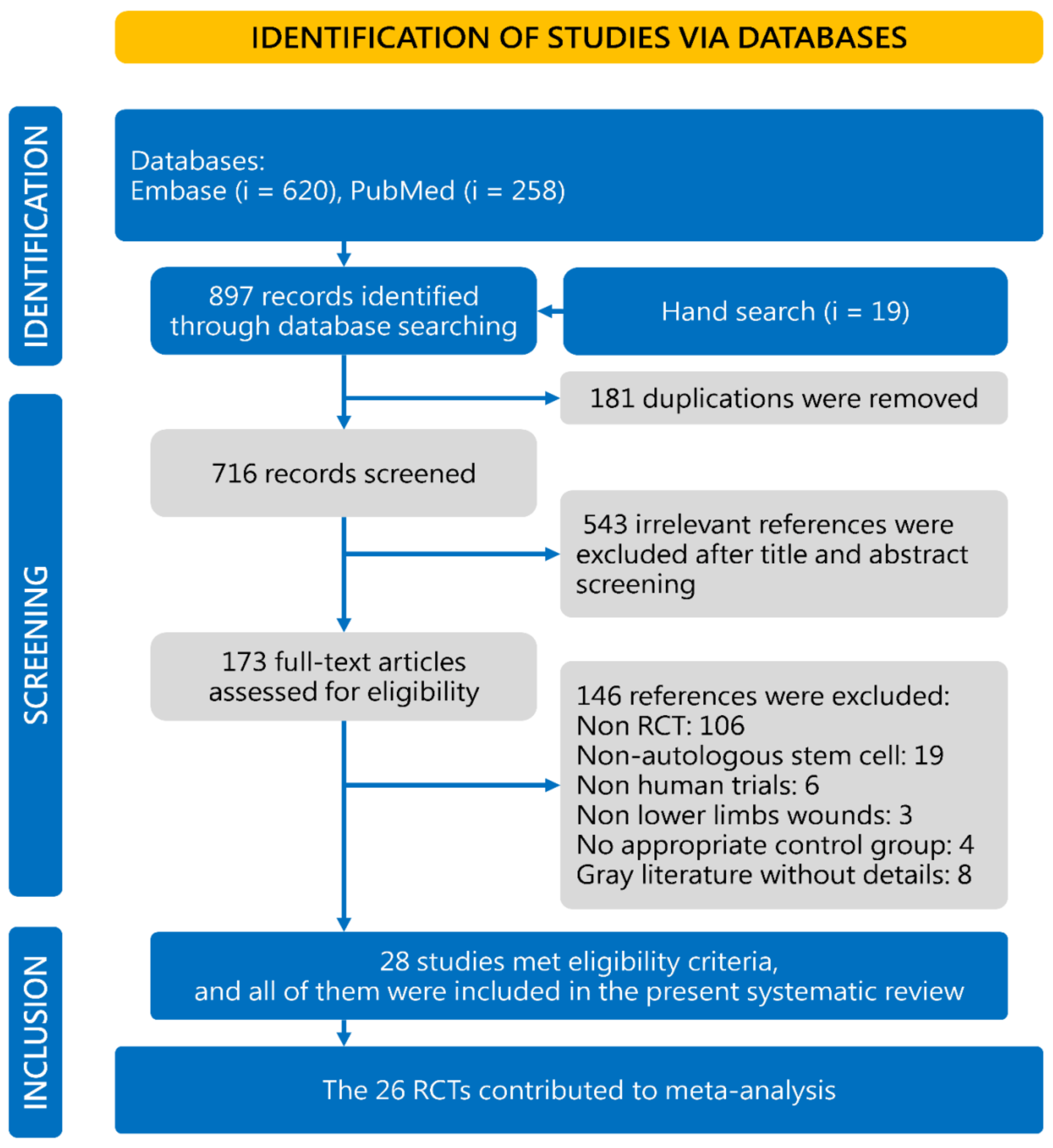
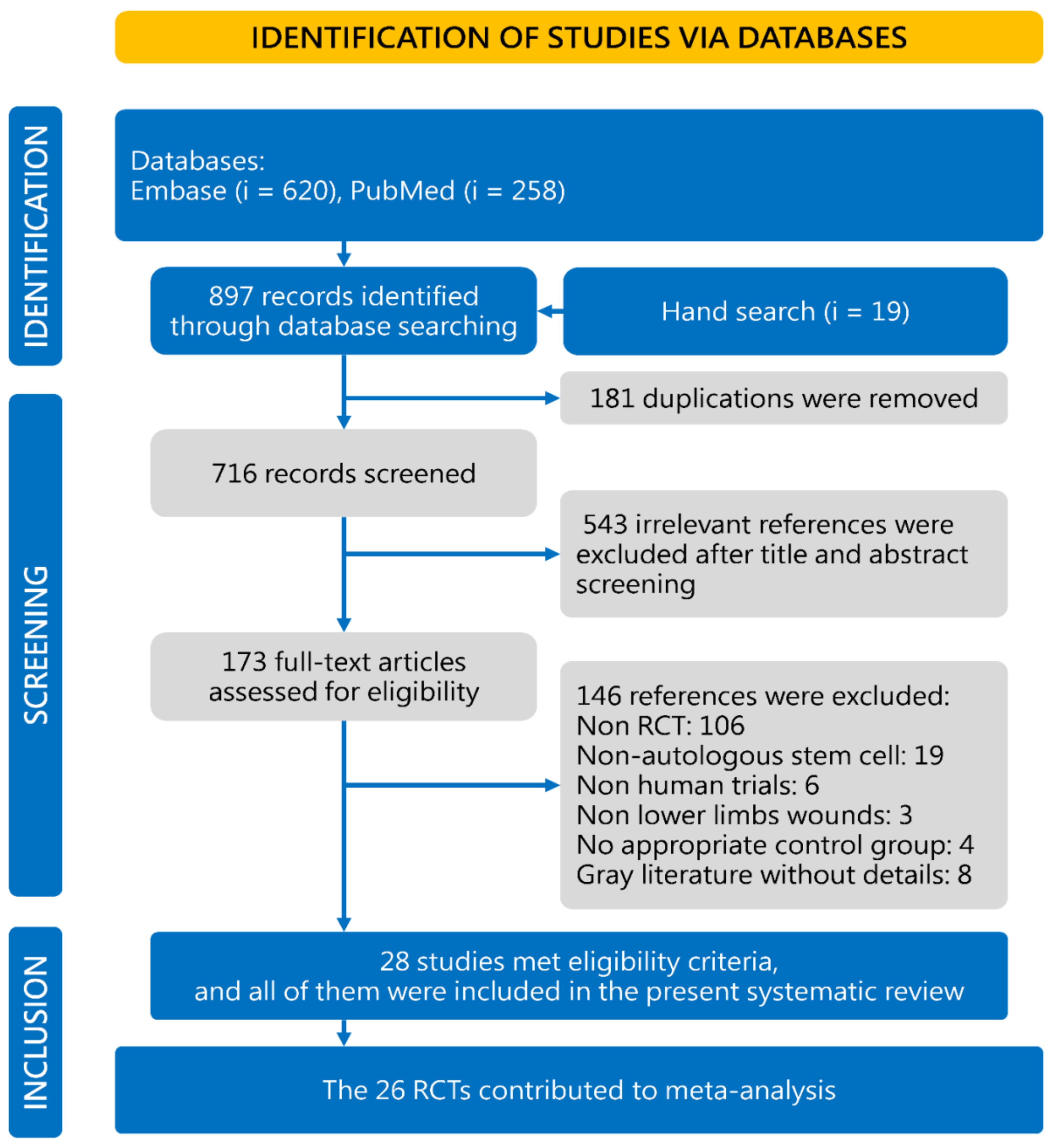
2.1. Literature Search and Study Selection
2.2. Data Extraction and Quality Evaluation
2.3. Analysis and Statistics
3. Results
3.1. Characteristics of Included Studies
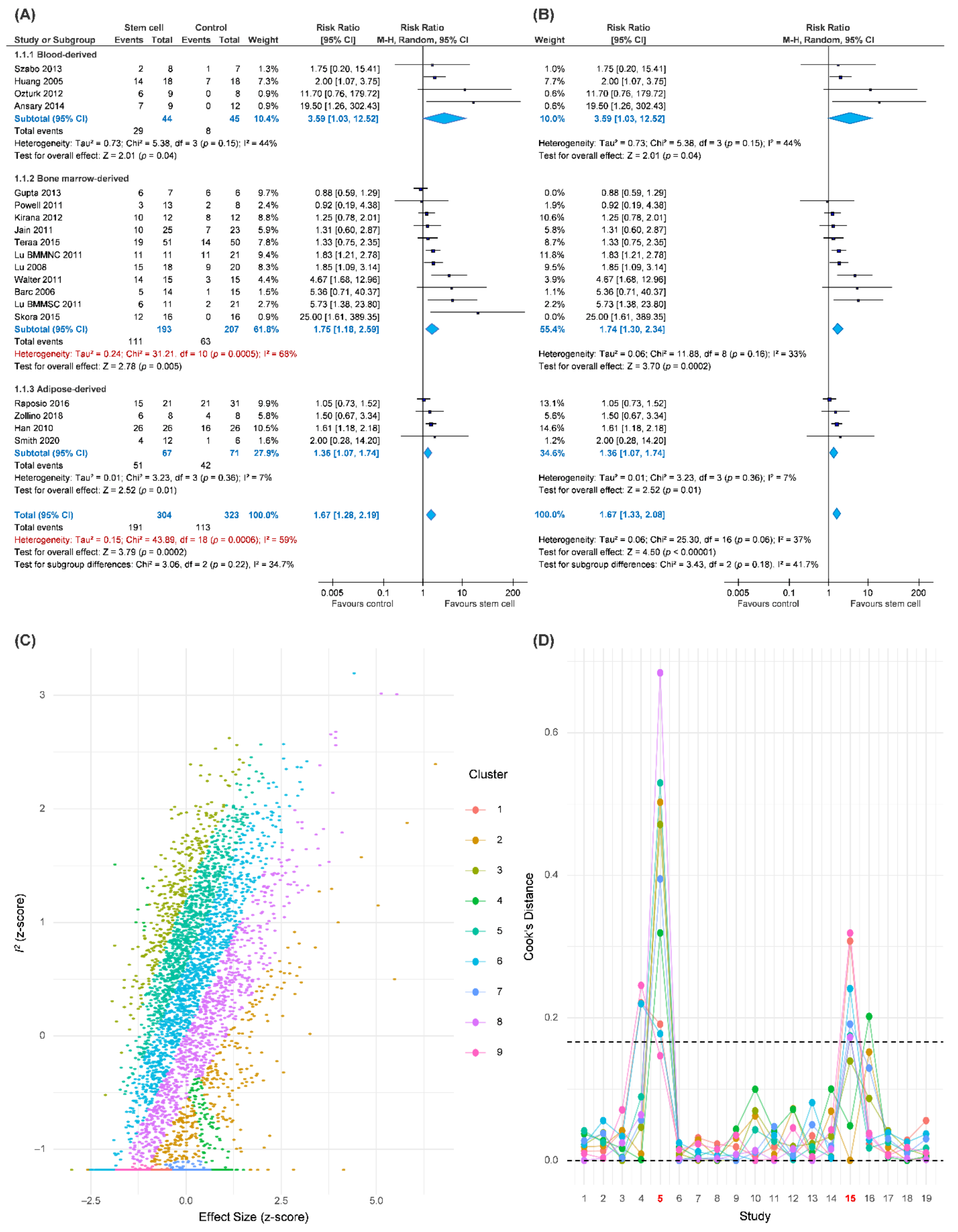
3.2. Complete Wound Healing
3.3. Amputation and Peripheral Circulation
3.4. Safety
4. Discussion
4.1. Key Findings
4.2. Potential Mechanism
4.3. Source of Heterogeneity
4.3.1. Source of Stem Cells
4.3.2. Etiology of Wounds
4.3.3. Mean Follow-Up Time
4.3.4. Cell Markers
4.3.5. Route of Administration
4.4. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- American Society of Surgeons. Evidence-Based Clinical Practice Guideline: Chronic Wounds of the Lower Extremity; American Society of Surgeons: Arlington Hights, IL, USA, 2007. [Google Scholar]
- Anderson, J.L.; Halperin, J.L.; Albert, N.M.; Bozkurt, B.; Brindis, R.G.; Curtis, L.H.; DeMets, D.; Guyton, R.A.; Hochman, J.S.; Kovacs, R.J.; et al. Management of Patients with Peripheral Artery Disease (Compilation of 2005 and 2011 Accf/Aha Guideline Recommendations): A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation 2013, 127, 1425–1443. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bakker, K.; Apelqvist, J.; Schaper, N.C. Practical Guidelines on the Management and Prevention of the Diabetic Foot 2011. Diabetes Metab. Res. Rev. 2012, 28, 225–231. [Google Scholar] [CrossRef] [PubMed]
- Boulton, A.J.M.; Whitehouse, R.W. The Diabetic Foot. In Endotext; Feingold, K.R., Anawalt, B., Boyce, A., Chrousos, G., de Herder, W.W., Dhatariya, K., Dungan, K., Grossman, A., Hershman, J.M., Hofland, J., et al., Eds.; MDText.com, Inc.: South Dartmouth, MA, USA, 2000. [Google Scholar]
- Okonofua, F.E.; Odimegwu, C.; Ajabor, H.; Daru, P.H.; Johnson, A. Assessing the Prevalence and Determinants of Unwanted Pregnancy and Induced Abortion in Nigeria. Stud. Fam. Plan. 1999, 30, 67–77. [Google Scholar] [CrossRef]
- Nehler, M.R.; Duval, S.; Diao, L.; Annex, B.H.; Hiatt, W.R.; Rogers, K.; Zakharyan, A.; Hirsch, A.T. Epidemiology of peripheral arterial disease and critical limb ischemia in an insured national population. J. Vasc. Surg. 2014, 60, 686–695.e2. [Google Scholar] [CrossRef] [Green Version]
- Agarwal, S.; Sud, K.; Shishehbor, M.H. Nationwide Trends of Hospital Admission and Outcomes Among Critical Limb Ischemia Patients. J. Am. Coll. Cardiol. 2016, 67, 1901–1913. [Google Scholar] [CrossRef] [PubMed]
- Hart, C.A.; Tsui, J.; Khanna, A.; Abraham, D.J.; Baker, D.M. Stem cells of the lower limb: Their role and potential in management of critical limb ischemia. Exp. Biol. Med. 2013, 238, 1118–1126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, M.; Sheng, L.; Zhang, T.R.; Li, Q. Stem Cell Therapy for Lower Extremity Diabetic Ulcers: Where Do We Stand? BioMed Res. Int. 2013, 2013, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Kalka, C.; Masuda, H.; Takahashi, T.; Kalka-Moll, W.M.; Silver, M.; Kearney, M.; Li, T.; Isner, J.M.; Asahara, T. Transplantation of Ex Vivo Expanded Endothelial Progenitor Cells for Therapeutic Neovascularization. Proc. Natl. Acad. Sci. USA 2000, 97, 3422–3427. [Google Scholar] [CrossRef]
- Kamihata, H.; Matsubara, H.; Nishiue, T.; Fujiyama, S.; Tsutsumi, Y.; Ozono, R.; Masaki, H.; Mori, Y.; Iba, O.; Tateishi, E.; et al. Implantation of Bone Marrow Mononuclear Cells Into Ischemic Myocardium Enhances Collateral Perfusion and Regional Function via Side Supply of Angioblasts, Angiogenic Ligands, and Cytokines. Circulation 2001, 104, 1046–1052. [Google Scholar] [CrossRef] [Green Version]
- Takahashi, T.; Kalka, C.; Masuda, H.; Chen, D.; Silver, M.; Kearney, M.; Magner, M.; Isner, J.M.; Asahara, T. Ischemia- and cytokine-induced mobilization of bone marrow-derived endothelial progenitor cells for neovascularization. Nat. Med. 1999, 5, 434–438. [Google Scholar] [CrossRef]
- Tateishi-Yuyama, E.; Matsubara, H.; Murohara, T.; Ikeda, U.; Shintani, S.; Masaki, H.; Amano, K.; Kishimoto, Y.; Yoshimoto, K.; Akashi, H.; et al. Therapeutic angiogenesis for patients with limb ischaemia by autologous transplantation of bone-marrow cells: A pilot study and a randomised controlled trial. Lancet 2002, 360, 427–435. [Google Scholar] [CrossRef]
- Rigato, M.; Monami, M.; Fadini, G.P. Autologous Cell Therapy for Peripheral Arterial Disease: Systematic Review and Meta-Analysis of Randomized, Nonrandomized, and Noncontrolled Studies. Circ. Res. 2017, 120, 1326–1340. [Google Scholar] [CrossRef] [PubMed]
- Huang, P.; Li, S.; Han, M.; Xiao, Z.; Yang, R.; Han, Z.C. Autologous Transplantation of Granulocyte Colony-Stimulating Factor-Mobilized Peripheral Blood Mononuclear Cells Improves Critical Limb Ischemia in Diabetes. Diabetes Care 2005, 28, 2155–2160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raposio, E.; Bertozzi, N.; Grignaffini, E.; Simonacci, F.; Grieco, M.P. Adipose-derived stem cells for treatment of chronic cutaneous ulcers in patients with critical limb ischemia: A pilot study. Eur. J. Plast. Surg. 2018, 41, 459–464. [Google Scholar] [CrossRef]
- Dai, J.; Jiang, C.; Chen, H.; Chai, Y. Treatment of Diabetic Foot with Autologous Stem Cells: A Meta-Analysis of Randomized Studies. Stem Cells Int. 2020, 2020, 6748530. [Google Scholar] [CrossRef]
- Wahid, F.S.A.; Ismail, N.A.; Jamaludin, W.F.W.; Muhamad, N.A.; Idris, M.A.M.; Lai, N.M. Efficacy and Safety of Autologous Cell-based Therapy in Patients with No-option Critical Limb Ischaemia: A Meta-Analysis. Curr. Stem Cell Res. Ther. 2018, 13, 265–283. [Google Scholar] [CrossRef] [PubMed]
- Jiang, X.; Zhang, H.; Teng, M. Effectiveness of Autologous Stem Cell Therapy for the Treatment of Lower Extremity Ulcers: A Systematic Review and Meta-Analysis. Medicine 2016, 95, e2716. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.Y.; Suh, W. Stem Cell Therapy for Dermal Wound Healing. Int. J. Stem Cells 2010, 3, 29–31. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C.; et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [Green Version]
- Sidney, L.E.; Branch, M.J.; Dunphy, S.E.; Dua, H.S.; Hopkinson, A. Concise Review: Evidence for CD34 as a Common Marker for Diverse Progenitors. Stem Cells 2014, 32, 1380–1389. [Google Scholar] [CrossRef] [Green Version]
- Tumbar, T.; Guasch, G.; Greco, V.; Blanpain, C.; Lowry, W.E.; Rendl, M.; Fuchs, E. Defining the Epithelial Stem Cell Niche in Skin. Science 2004, 303, 359–363. [Google Scholar] [CrossRef] [Green Version]
- Egger, M.; Smith, G.D.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arai, M.; Misao, Y.; Nagai, H.; Kawasaki, M.; Nagashima, K.; Suzuki, K.; Tsuchiya, K.; Otsuka, S.; Uno, Y.; Takemura, G.; et al. Granulocyte Colony-Stimulating Factor A Noninvasive Regeneration Therapy for Treating Atherosclerotic Peripheral Artery Disease. Circ. J. 2006, 70, 1093–1098. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dash, N.R.; Dash, S.; Routray, P.; Mohapatra, S.; Mohapatra, P.C. Targeting Nonhealing Ulcers of Lower Extremity in Human Through Autologous Bone Marrow-Derived Mesenchymal Stem Cells. Rejuvenation Res. 2009, 12, 359–366. [Google Scholar] [CrossRef] [PubMed]
- Debin, L.; Youzhao, J.; Ziwen, L.; Xiaoyan, L.; Zhonghui, Z.; Bing, C. Autologous Transplantation of Bone Marrow Mesenchymal Stem Cells on Diabetic Patients with Lower Limb Ischemia. J. Med Coll. PLA 2008, 23, 106–115. [Google Scholar] [CrossRef]
- El Ansary, M.; AlAbden, A.Z.; Halim, A.A.; Shafy, S.A.; Hafeez, N.A. Stem cell implantation in the treatment of peripheral vascular disease. Comp. Haematol. Int. 2014, 23, 169–173. [Google Scholar] [CrossRef]
- Gupta, P.K.; Chullikana, A.; Parakh, R.; Desai, S.; Das, A.; Gottipamula, S.; Krishnamurthy, S.; Anthony, N.; Pherwani, A.; Majumdar, A.S. A double blind randomized placebo controlled phase I/II study assessing the safety and efficacy of allogeneic bone marrow derived mesenchymal stem cell in critical limb ischemia. J. Transl. Med. 2013, 11, 143. [Google Scholar] [CrossRef] [Green Version]
- Han, S.-K.; Kim, H.-R.; Kim, W.-K. The treatment of diabetic foot ulcers with uncultured, processed lipoaspirate cells: A pilot study. Wound Repair Regen. 2010, 18, 342–348. [Google Scholar] [CrossRef]
- Iafrati, M.D.; Hallett, J.W.; Geils, G.; Pearl, G.; Lumsden, A.; Peden, E.; Bandyk, D.; Vijayaraghava, K.; Radhakrishnan, R.; Ascher, E.; et al. Early results and lessons learned from a multicenter, randomized, double-blind trial of bone marrow aspirate concentrate in critical limb ischemia. J. Vasc. Surg. 2011, 54, 1650–1655. [Google Scholar] [CrossRef] [Green Version]
- Jain, P.; Perakath, B.; Jesudason, M.R.; Nayak, S. The effect of autologous bone marrow-derived cells on healing chronic lower extremity wounds: Results of a randomized controlled study. Ostomy Wound Manag. 2011, 57, 38–44. [Google Scholar]
- Kirana, S.; Stratmann, B.; Prante, C.; Prohaska, W.; Koerperich, H.; Lammers, D.; Gastens, M.H.; Quast, T.; Negrean, M.; Stirban, O.A.; et al. Autologous stem cell therapy in the treatment of limb ischaemia induced chronic tissue ulcers of diabetic foot patients. Int. J. Clin. Pr. 2012, 66, 384–393. [Google Scholar] [CrossRef] [PubMed]
- Kolvenbach, R.; Kreissig, C.; Ludwig, E.; Cagiannos, C. Stem cell use in critical limb ischemia. J. Cardiovasc. Surg. 2007, 48, 39–44. [Google Scholar]
- Li, M.; Zhou, H.; Jin, X.; Wang, M.; Zhang, S.; Xu, L. Autologous Bone Marrow Mononuclear Cells Transplant in Patients With Critical Leg Ischemia: Preliminary Clinical Results. Exp. Clin. Transplant. 2013, 11, 435–439. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Losordo, D.W.; Kibbe, M.R.; Mendelsohn, F.; Marston, W.; Driver, V.R.; Sharafuddin, M.; Teodorescu, V.; Wiechmann, B.N.; Thompson, C.; Kraiss, L.; et al. A Randomized, Controlled Pilot Study of Autologous CD34+ Cell Therapy for Critical Limb Ischemia. Circ. Cardiovasc. Interv. 2012, 5, 821–830. [Google Scholar] [CrossRef] [Green Version]
- Lu, D.; Chen, B.; Liang, Z.; Deng, W.; Jiang, Y.; Li, S.; Xu, J.; Wu, Q.; Zhang, Z.; Xie, B.; et al. Comparison of bone marrow mesenchymal stem cells with bone marrow-derived mononuclear cells for treatment of diabetic critical limb ischemia and foot ulcer: A double-blind, randomized, controlled trial. Diabetes Res. Clin. Pr. 2011, 92, 26–36. [Google Scholar] [CrossRef]
- Lu, D.; Jiang, Y.; Deng, W.; Zhang, Y.; Liang, Z.; Wu, Q.; Jiang, X.; Zhang, L.; Gao, F.; Cao, Y.; et al. Long-Term Outcomes of BMMSC Compared with BMMNC for Treatment of Critical Limb Ischemia and Foot Ulcer in Patients with Diabetes. Cell Transplant. 2019, 28, 645–652. [Google Scholar] [CrossRef]
- Mohammadzadeh, L.; Samedanifard, S.H.; Keshavarzi, A.; Alimoghaddam, K.; Larijani, B.; Ghavamzadeh, A.; Ahmadi, A.S.; Shojaeifard, A.; Ostadali, M.; Sharifi, A.M.; et al. Therapeutic Outcomes of Transplanting Autologous Granulocyte Colony-stimulating Factor-mobilised Peripheral Mononuclear Cells in Diabetic Patients with Critical Limb Ischaemia. Exp. Clin. Endocrinol. Diabetes 2013, 121, 48–53. [Google Scholar] [CrossRef] [Green Version]
- Ozturk, A.; Kucukardali, Y.; Tangi, F.; Erikci, A.; Uzun, G.; Bashekim, C.; Sen, H.; Terekeci, H.; Narin, Y.; Ozyurt, M.; et al. Therapeutical potential of autologous peripheral blood mononuclear cell transplantation in patients with type 2 diabetic critical limb ischemia. J. Diabetes Its Complicat. 2012, 26, 29–33. [Google Scholar] [CrossRef]
- Pignon, B.; Sevestre, M.-A.; Kanagaratnam, L.; Pernod, G.; Stephan, D.; Emmerich, J.; Clement, C.; Sarlon, G.; Boulon, C.; Tournois, C.; et al. Autologous Bone Marrow Mononuclear Cell Implantation and Its Impact on the Outcome of Patients With Critical Limb Ischemia—Results of a Randomized, Double-Blind, Placebo-Controlled Trial. Circ. J. 2017, 81, 1713–1722. [Google Scholar] [CrossRef] [Green Version]
- Powell, R.J.; Comerota, A.J.; Berceli, S.A.; Guzman, R.; Henry, T.D.; Tzeng, E.; Velazquez, O.; Marston, W.A.; Bartel, R.L.; Longcore, A.; et al. Interim analysis results from the RESTORE-CLI, a randomized, double-blind multicenter phase II trial comparing expanded autologous bone marrow-derived tissue repair cells and placebo in patients with critical limb ischemia. J. Vasc. Surg. 2011, 54, 1032–1041. [Google Scholar] [CrossRef] [Green Version]
- Procházka, V.; Gumulec, J.; Jalůvka, F.; Salounová, D.; Jonszta, T.; Czerný, D.; Krajča, J.; Urbanec, R.; Klement, P.; Martinek, J.; et al. Cell Therapy, a New Standard in Management of Chronic Critical Limb Ischemia and Foot Ulcer. Cell Transplant 2010, 19, 1413–1424. [Google Scholar] [CrossRef] [Green Version]
- Raposio, E.; Bertozzi, N.; Bonomini, S.; Bernuzzi, G.; Formentini, A.; Grignaffini, E.; Pio Grieco, M. Adipose-derived Stem Cells Added to Platelet-rich Plasma for Chronic Skin Ulcer Therapy. Wounds Compend. Clin. Res. Pract. 2016, 28, 126–131. [Google Scholar]
- Raval, A.N.; Schmuck, E.G.; Tefera, G.; Leitzke, C.; Ark, C.V.; Hei, D.; Centanni, J.M.; de Silva, R.; Koch, J.; Chappell, R.G.; et al. Bilateral administration of autologous CD133+ cells in ambulatory patients with refractory critical limb ischemia: Lessons learned from a pilot randomized, double-blind, placebo-controlled trial. Cytotherapy 2014, 16, 1720–1732. [Google Scholar] [CrossRef] [Green Version]
- Skóra, J.; Pupka, A.; Janczak, D.; Barć, P.; Dawiskiba, T.; Korta, K.; Baczynska, D.; Mastalerz-Migas, A.; Garcarek, J. Combined autologous bone marrow mononuclear cell and gene therapy as the last resort for patients with critical limb ischemia. Arch. Med Sci. 2015, 11, 325–331. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, O.J.; Leigh, R.; Kanapathy, M.; Macneal, P.; Jell, G.; Hachach-Haram, N.; Mann, H.; Mosahebi, A. Fat grafting and platelet-rich plasma for the treatment of diabetic foot ulcers: A feasibility-randomised controlled trial. Int. Wound J. 2020, 17, 1578–1594. [Google Scholar] [CrossRef]
- Szabó, G.V.; Kövesd, Z.; Cserepes, J.; Daróczy, J.; Belkin, M.; Acsády, G. Peripheral blood-derived autologous stem cell therapy for the treatment of patients with late-stage peripheral artery disease—results of the short- and long-term follow-up. Cytotherapy 2013, 15, 1245–1252. [Google Scholar] [CrossRef] [PubMed]
- Teraa, M.; Sprengers, R.W.; Schutgens, R.E.; Slaper-Cortenbach, I.C.; van der Graaf, Y.; Algra, A.; van der Tweel, I.; Doevendans, P.A.; Mali, W.P.; Moll, F.L.; et al. Effect of Repetitive Intra-Arterial Infusion of Bone Marrow Mononuclear Cells in Patients with No-Option Limb Ischemia: The Randomized, Double-Blind, Placebo-Controlled Rejuvenating Endothelial Progenitor Cells Via Transcutaneous Intra-Arterial Supplementation (Juventas) Trial. Circulation 2015, 131, 851–860. [Google Scholar] [PubMed] [Green Version]
- Walter, D.H.; Krankenberg, H.; Balzer, J.O.; Kalka, C.; Baumgartner, I.; Schlüter, M.; Tonn, T.; Seeger, F.; Dimmeler, S.; Lindhoff-Last, E.; et al. Intraarterial Administration of Bone Marrow Mononuclear Cells in Patients with Critical Limb Ischemia: A Randomized-Start, Placebo-Controlled Pilot Trial (Provasa). Circ. Cardiovasc. Interv. 2011, 4, 26–37. [Google Scholar] [CrossRef] [Green Version]
- Zollino, I.; Campioni, D.; Sibilla, M.G.; Tessari, M.; Malagoni, A.M.; Zamboni, P. A phase II randomized clinical trial for the treatment of recalcitrant chronic leg ulcers using centrifuged adipose tissue containing progenitor cells. Cytotherapy 2019, 21, 200–211. [Google Scholar] [CrossRef]
- Aboyans, V.; Criqui, M.H.; Abraham, P.; Allison, M.A.; Creager, M.A.; Diehm, C.; Fowkes, F.G.; Hiatt, W.R.; Jönsson, B.; Lacroix, P.; et al. Measurement and Interpretation of the Ankle-Brachial Index: A Scientific Statement from the American Heart Association. Circulation 2012, 126, 2890–2909. [Google Scholar] [CrossRef] [Green Version]
- Apelqvist, J. Diagnostics and treatment of the diabetic foot. Endocrinology 2012, 41, 384–397. [Google Scholar] [CrossRef] [PubMed]
- Rossi, M.; Carpi, A. Skin Microcirculation in Peripheral Arterial Obliterative Disease. Biomed. Pharmacother. 2004, 58, 427–431. [Google Scholar] [CrossRef] [PubMed]
- De Meijer, V.E.; Van’t Sant, H.P.; Spronk, S.; Kusters, F.J.; den Hoed, P.T. Reference Value of Transcutaneous Oxygen Measurement in Diabetic Patients Compared with Nondiabetic Patients. J. Vasc. Surg. 2008, 48, 382–388. [Google Scholar] [CrossRef] [Green Version]
- Spreen, M.I.; Gremmels, H.; Teraa, M.; Sprengers, R.W.; Verhaar, M.C.; van Eps, R.G.S.; de Vries, J.-P.P.; Mali, W.P.; van Overhagen, H. Diabetes Is Associated With Decreased Limb Survival in Patients With Critical Limb Ischemia: Pooled Data From Two Randomized Controlled Trials. Diabetes Care 2016, 39, 2058–2064. [Google Scholar] [CrossRef] [Green Version]
- Verma, M.; Singh, A.K.; Kumar, V.; Mishra, B. Role of Ankle Brachial Index (ABI) in Management of Non-Healing Ulcers of Lower Limb. J. Univers. Surg. 2018, 6, 1–5. [Google Scholar] [CrossRef]
- Dubsky, M.; Jirkovska, A.; Bem, R.; Fejfarova, V.; Pagacova, L.; Sixta, B.; Varga, M.; Langkramer, S.; Sykova, E.; Jude, E.B. Both autologous bone marrow mononuclear cell and peripheral blood progenitor cell therapies similarly improve ischaemia in patients with diabetic foot in comparison with control treatment. Diabetes Metabolism Res. Rev. 2013, 29, 369–376. [Google Scholar] [CrossRef] [PubMed]
- Qin, H.L.; Zhu, X.H.; Zhang, B.; Zhou, L.; Wang, W.Y. Clinical Evaluation of Human Umbilical Cord Mesenchymal Stem Cell Transplantation After Angioplasty for Diabetic Foot. Exp. Clin. Endocrinol. Diabetes 2016, 124, 497–503. [Google Scholar] [CrossRef]
- Tanaka, R.; Masuda, H.; Kato, S.; Imagawa, K.; Kanabuchi, K.; Nakashioya, C.; Yoshiba, F.; Fukui, T.; Ito, R.; Kobori, M.; et al. Autologous G-CSF-Mobilized Peripheral Blood CD34+ Cell Therapy for Diabetic Patients with Chronic Nonhealing Ulcer. Cell Transplant. 2014, 23, 167–179. [Google Scholar] [CrossRef]
- Shu, X.; Shu, S.; Tang, S.; Yang, L.; Liu, D.; Li, K.; Dong, Z.; Ma, Z.; Zhu, Z.; Din, J. Efficiency of stem cell based therapy in the treatment of diabetic foot ulcer: A meta-analysis. Endocr. J. 2018, 65, 403–413. [Google Scholar] [CrossRef] [Green Version]
- Fam, N.P.; Verma, S.; Kutryk, M.; Stewart, D.J. Clinician Guide to Angiogenesis. Circulation 2003, 108, 2613–2618. [Google Scholar] [CrossRef]
- Arnold, F. Exploiting angiogenesis. Lancet 1991, 337, 865–866. [Google Scholar] [CrossRef]
- Arnold, F.; West, D.C. Angiogenesis in Wound Healing. Pharmacol. Ther. 1991, 52, 407–422. [Google Scholar] [CrossRef]
- Wu, Y.; Chen, L.; Scott, P.G.; Tredget, E.E. Mesenchymal Stem Cells Enhance Wound Healing Through Differentiation and Angiogenesis. STEM CELLS 2007, 25, 2648–2659. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tonnesen, M.G.; Feng, X.; Clark, R.A. Angiogenesis in Wound Healing. J. Investig. Dermatol. Symp. Proc. 2000, 5, 40–46. [Google Scholar] [CrossRef] [Green Version]
- Nikol, S.; Baumgartner, I.; Van Belle, E.; Diehm, C.; Visoná, A.; Capogrossi, M.C.; Ferreira-Maldent, N.; Gallino, A.; Wyatt, M.G.; Wijesinghe, L.D.; et al. Therapeutic Angiogenesis With Intramuscular NV1FGF Improves Amputation-free Survival in Patients With Critical Limb Ischemia. Mol. Ther. 2008, 16, 972–978. [Google Scholar] [CrossRef] [PubMed]
- Xie, B.; Luo, H.; Zhang, Y.; Wang, Q.; Zhou, C.; Xu, D. Autologous Stem Cell Therapy in Critical Limb Ischemia: A Meta-Analysis of Randomized Controlled Trials. Stem Cells Int. 2018, 2018, 7528464. [Google Scholar] [CrossRef] [Green Version]
- Iba, O.; Matsubara, H.; Nozawa, Y.; Fujiyama, S.; Amano, K.; Mori, Y.; Kojima, H.; Iwasaka, T. Angiogenesis by Implantation of Peripheral Blood Mononuclear Cells and Platelets Into Ischemic Limbs. Circulation 2002, 106, 2019–2025. [Google Scholar] [CrossRef] [Green Version]
- Al-Khaldi, A.; Al-Sabti, H.; Galipeau, J.; Lachapelle, K. Therapeutic angiogenesis using autologous bone marrow stromal cells: Improved blood flow in a chronic limb ischemia model. Ann. Thorac. Surg. 2003, 75, 204–209. [Google Scholar] [CrossRef]
- Deng, C.; Wang, L.; Feng, J.; Lu, F. Treatment of Human Chronic Wounds with Autologous Extracellular Matrix/Stromal Vascular Fraction Gel: A Strobe-Compliant Study. Medicine 2018, 97, e11667. [Google Scholar] [CrossRef]
- Leblond, A.-L.; O’Sullivan, J.; Caplice, N. Bone marrow mononuclear stem cells: Potential in the treatment of myocardial infarction. Stem Cells Cloning: Adv. Appl. 2009, 2, 11–19. [Google Scholar] [CrossRef] [Green Version]
- Sarasúa, J.G.; López, S.P.; Álvarez-Viejo, M.; Basterrechea, M.P.; Rodríguez, A.F.; Ferrero-Gutierrez, A.; Gala, J.G.; Menéndez, Y.M.; Augusto, D.E.; Arias, A.P.; et al. Treatment of pressure ulcers with autologous bone marrow nuclear cells in patients with spinal cord injury. J. Spinal Cord Med. 2011, 34, 301–307. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tang, J.; Xie, Q.; Pan, G.; Wang, J.; Wang, M. Mesenchymal stem cells participate in angiogenesis and improve heart function in rat model of myocardial ischemia with reperfusion. Eur. J. Cardio-Thoracic Surg. 2006, 30, 353–361. [Google Scholar] [CrossRef] [PubMed]
- Kim, W.-S.; Park, B.-S.; Sung, J.-H.; Yang, J.-M.; Park, S.-B.; Kwak, S.-J.; Park, J.-S. Wound healing effect of adipose-derived stem cells: A critical role of secretory factors on human dermal fibroblasts. J. Dermatol. Sci. 2007, 48, 15–24. [Google Scholar] [CrossRef] [PubMed]
- Bain, B.J. Bone marrow biopsy morbidity: Review of 2003. J. Clin. Pathol. 2005, 58, 406–408. [Google Scholar] [CrossRef]
- Heublein, H.; Bader, A.; Giri, S. Preclinical and clinical evidence for stem cell therapies as treatment for diabetic wounds. Drug Discov. Today 2015, 20, 703–717. [Google Scholar] [CrossRef]
- Lavery, L.A.; Fulmer, J.; Shebetka, K.A.; Regulski, M.; Vayser, D.; Fried, D.; Kashefsky, H.; Owings, T.M.; Nadarajah, J. The Grafix Diabetic Foot Ulcer Study Group The efficacy and safety of Grafix ® for the treatment of chronic diabetic foot ulcers: Results of a multi-centre, controlled, randomised, blinded, clinical trial. Int. Wound J. 2014, 11, 554–560. [Google Scholar] [CrossRef]
- Bura, A.; Planat-Benard, V.; Bourin, P.; Silvestre, J.-S.; Gross, F.; Grolleau, J.-L.; Saint-Lebese, B.; Peyrafitte, J.-A.; Fleury, S.; Gadelorge, M.; et al. Phase I trial: The use of autologous cultured adipose-derived stroma/stem cells to treat patients with non-revascularizable critical limb ischemia. Cytotherapy 2014, 16, 245–257. [Google Scholar] [CrossRef] [Green Version]
- Uzun, E.; Güney, A.; Gönen, Z.B.; Özkul, Y.; Kafadar, I.H.; Günay, M.; Mutlu, M. Intralesional Allogeneic Adipose-Derived Stem Cells Application in Chronic Diabetic Foot Ulcer: Phase I/2 Safety Study. Foot Ankle Surg. 2020, 27, 636–642. [Google Scholar] [CrossRef]
- Falanga, V.; Iwamoto, S.; Chartier, M.; Yufit, T.; Butmarc, J.; Kouttab, N.; Shrayer, D.; Carson, P. Autologous Bone Marrow–Derived Cultured Mesenchymal Stem Cells Delivered in a Fibrin Spray Accelerate Healing in Murine and Human Cutaneous Wounds. Tissue Eng. 2007, 13, 1299–1312. [Google Scholar] [CrossRef]
- Borys, S.; Hohendorff, J.; Koblik, T.; Witek, P.; Ludwig-Słomczyńska, A.H.; Frankfurter, C.; Kiec-Wilk, B.; Malecki, M.T. Negative-pressure wound therapy for management of chronic neuropathic noninfected diabetic foot ulcerations - short-term efficacy and long-term outcomes. Endocrinology 2018, 62, 611–616. [Google Scholar] [CrossRef] [Green Version]
- Butcher, E.C.; Picker, L.J. Lymphocyte Homing and Homeostasis. Science 1996, 272, 60–67. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, J.S.; McNagny, K.M. CD34 is a Key Regulator of Hematopoietic Stem Cell Trafficking to Bone Marrow and Mast Cell Progenitor Trafficking in the Periphery. Microcirculation 2009, 16, 487–496. [Google Scholar] [CrossRef]
- Madeddu, P.; Emanueli, C.; Pelosi, E.; Salis, M.B.; Cerio, A.M.; Bonanno, G.; Patti, M.; Stassi, G.; Condorelli, G.; Peschle, C. Transplantation of low dose CD34 + Kdr + cells promotes vascular and muscular regeneration in ischemic limbs. FASEB J. 2004, 18, 1737–1739. [Google Scholar] [CrossRef] [PubMed]
- Schatteman, G.C.; Hanlon, H.D.; Jiao, C.; Dodds, S.G.; Christy, B.A. Blood-derived angioblasts accelerate blood-flow restoration in diabetic mice. J. Clin. Investig. 2000, 106, 571–578. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andrews, R.G.; Peterson, L.J.; Morris, J.; Potter, J.; Heyward, S.; Gough, M.; Bryant, E.; Kiem, H.-P. Differential engraftment of genetically modified CD34+ and CD34− hematopoietic cell subsets in lethally irradiated baboons. Exp. Hematol. 2000, 28, 508–518. [Google Scholar] [CrossRef]
- Bhatia, M.; Bonnet, D.; Murdoch, B.; Gan, O.I.; Dick, J. A newly discovered class of human hematopoietic cells with SCID-repopulating activity. Nat. Med. 1998, 4, 1038–1045. [Google Scholar] [CrossRef]
- Ishii, M.; Matsuoka, Y.; Sasaki, Y.; Nakatsuka, R.; Takahashi, M.; Nakamoto, T.; Yasuda, K.; Matsui, K.; Asano, H.; Uemura, Y. Development of a high-resolution purification method for precise functional characterization of primitive human cord blood–derived CD34–negative SCID-repopulating cells. Exp. Hematol. 2011, 39, 203–213.e1. [Google Scholar] [CrossRef]
- Lange, C.; Kaltz, C.; Thalmeier, K.; Jochem, H.; Huss, R. Hematopoietic Reconstitution of Syngeneic Mice with a Peripheral Blood-Derived, Monoclonal CD34-, Sca-1+, Thy-1low, c-kit+ Stem Cell Line. J. Hematother. 1999, 8, 335–342. [Google Scholar] [CrossRef]
- Matsuoka, Y.; Nakatsuka, R.; Sumide, K.; Kawamura, H.; Takahashi, M.; Fujioka, T.; Uemura, Y.; Asano, H.; Sasaki, Y.; Inoue, M.; et al. Prospectively Isolated Human Bone Marrow Cell-Derived MSCs Support Primitive Human CD34-Negative Hematopoietic Stem Cells. Stem Cells 2015, 33, 1554–1565. [Google Scholar] [CrossRef]
- Takahashi, M.; Matsuoka, Y.; Sumide, K.; Nakatsuka, R.; Fujioka, T.; Kohno, H.; Sasaki, Y.; Matsui, K.; Asano, H.; Kaneko, K.; et al. CD133 is a positive marker for a distinct class of primitive human cord blood-derived CD34-negative hematopoietic stem cells. Leukemia 2014, 28, 1308–1315. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zanjani, E.D.; Almeida-Porada, G.; Livingston, A.G.; Flake, A.W.; Ogawa, M. Human bone marrow CD34- cells engraft in vivo and undergo multilineage expression that includes giving rise to CD34+ cells. Exp. Hematol. 1998, 26, 353–360. [Google Scholar] [PubMed]
- Huss, R. Perspectives on the Morphology and Biology of CD34-Negative Stem Cells. J. Hematother. 2000, 9, 783–793. [Google Scholar] [CrossRef] [PubMed]
- Bartsch, T.; Brehm, M.; Zeus, T.; Kögler, G.; Wernet, P.; Strauer, B.E. Transplantation of autologous mononuclear bone marrow stem cells in patients with peripheral arterial disease (The TAM-PAD study). Clin. Res. Cardiol. 2007, 96, 891–899. [Google Scholar] [CrossRef]
- Comerota, A.J.; Link, A.; Douville, J.; Burchardt, E.R. Upper extremity ischemia treated with tissue repair cells from adult bone marrow. J. Vasc. Surg. 2010, 52, 723–729. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gholamrezanezhad, A.; Mirpour, S.; Bagheri, M.; Mohamadnejad, M.; Alimoghaddam, K.; Abdolahzadeh, L.; Saghari, M.; Malekzadeh, R. In vivo tracking of 111In-oxine labeled mesenchymal stem cells following infusion in patients with advanced cirrhosis. Nucl. Med. Biol. 2011, 38, 961–967. [Google Scholar] [CrossRef]
- Schrepfer, S.; Deuse, T.; Reichenspurner, H.; Fischbein, M.; Robbins, R.; Pelletier, M. Stem Cell Transplantation: The Lung Barrier. Transplant. Proc. 2007, 39, 573–576. [Google Scholar] [CrossRef]
- Kang, Y.-H.; Jeon, S.H.; Park, J.-Y.; Chung, J.-H.; Choung, Y.-H.; Choung, H.-W.; Kim, E.-S.; Choung, P.-H. Platelet-Rich Fibrin is a Bioscaffold and Reservoir of Growth Factors for Tissue Regeneration. Tissue Eng. Part A 2011, 17, 349–359. [Google Scholar] [CrossRef]
- Siegel, K.R.; Clevenger, T.N.; Clegg, D.O.; Proctor, D.A.; Proctor, C.S. Adipose Stem Cells Incorporated in Fibrin Clot Modulate Expression of Growth Factors. Arthrosc. J. Arthrosc. Relat. Surg. 2018, 34, 581–591. [Google Scholar] [CrossRef] [Green Version]
- Sivan, U.; Jayakumar, K.; Krishnan, L.K. Constitution of Fibrin-Based Niche for In Vitro Differentiation of Adipose-Derived Mesenchymal Stem Cells to Keratinocytes. BioResearch Open Access 2014, 3, 339–347. [Google Scholar] [CrossRef]
- Held, M.; Rahmanian-Schwarz, A.; Schiefer, J.; Rath, R.; Werner, J.-O.; Rahmanian, S.; Schaller, H.-E.; Petersen, W. A Novel Collagen-Gelatin Scaffold for the Treatment of Deep Dermal Wounds—An Evaluation in a Minipig Model. Dermatol. Surg. 2016, 42, 751–756. [Google Scholar] [CrossRef] [PubMed]
- Jung, S.-N.; Rhie, J.W.; Kwon, H.; Jun, Y.J.; Seo, J.-W.; Yoo, G.; Oh, D.Y.; Ahn, S.T.; Woo, J.; Oh, J. In Vivo Cartilage Formation Using Chondrogenic-Differentiated Human Adipose-Derived Mesenchymal Stem Cells Mixed With Fibrin Glue. J. Craniofacial Surg. 2010, 21, 468–472. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.; Hyun, M.R.; Kim, S.W. The Effect of Adipose-Derived Stem Cells on Wound Healing: Comparison of Methods of Application. Stem Cells Int. 2019, 2019, 2745640. [Google Scholar] [CrossRef] [PubMed]
- Reichenberger, M.A.; Mueller, W.; Hartmann, J.; Diehm, Y.; Lass, U.; Koellensperger, E.; Leimer, U.; Germann, G.; Fischer, S. Adscs in a Fibrin Matrix Enhance Nerve Regeneration after Epineural Suturing in a Rat Model. Microsurgery 2016, 36, 491–500. [Google Scholar] [CrossRef]
- Zhang, Y.-S.; Gao, J.-H.; Lu, F.; Zhu, M. Adipose tissue engineering with human adipose-derived stem cells and fibrin glue injectable scaffold. Zhonghua Yi Xue Za Zhi 2008, 88, 2705–2709. (In Chinese) [Google Scholar]
- Hashemi, S.; Mohammadi, A.A.; Kabiri, H.; Hashempoor, M.R.; Mahmoodi, M.; Amini, M.; Mehrabani, D.; Mahmudi, M. The healing effect of Wharton’s jelly stem cells seeded on biological scaffold in chronic skin ulcers: A randomized clinical trial. J. Cosmet. Dermatol. 2019, 18, 1961–1967. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| Author/Year Published | Male % (I/C) | Age (I/C) | Type of Cell Intervention | Route (I/C) | Follow-Up (Months) | CD34 (+/−) | Relevant Outcome |
|---|---|---|---|---|---|---|---|
| Huang, 2005 | 9(64%)/9(64%) | 71.1/70.9 | PBMNC/NCT | IM | 3 | + | ①②④ |
| Arai, 2006 | 11(84%)/7(58%) | 62/68 | BMMNC/NCT | IM | 1 | + | ④⑤ |
| Barc, 2006 | Unclear | Unclear | BMMNC/NCT | IM | 3 and 6 | + | ①② |
| Lu, 2008 | 11(50%)/15(65%) | 66.6/65.5 | BMMSC/NCT | IM | 3 | – | ①②④ |
| Dash, 2009 | Unclear | 40 | BMMSC/NCT | IM+Topical | 3 | – | No data |
| Prochazka, 2010 | 36(86%)/42(78%) | 66.2/64.1 | BMSC/NCT | IA | 4 | + | ② |
| Han, 2010 | 15(58%)/14(54%) | 66.5/68.4 | ASC/NCT | Topical | 2 | ① | |
| Lu, 2011 | 7(39%)/8(42%) | 63/65 | BMMSC/BMMNC/NCT | IM | 6 | – | ①②④⑤ |
| Jain, 2011 | 17(68%)/15(63%) | 54/58 | BMSC/NCT | IM+Topical | 3 | ① | |
| Walter, 2011 | 16(84%)/13(62%) | 64.4/64.5 | BMMNC/NCT | IA | 3 and 6 | + | ①③④⑤ |
| Powell, 2011 | 25(78%)/8(57%) | 68.8/65.9 | BMSC/NCT | IM | 6 and 12 | ①③ | |
| Iafrati, 2011 | 23(68%)/9(64%) | 72.5/65.7 | BMSC/NCT | IM | 3 | ②③ | |
| Losordo, 2012 | 5(71%)/8(89%)/6(50%) | 61.8(low)/69.7(high)/67.1 | PB-CD34+/NCT | IM | 6 and 12 | + | ②③ |
| Ozturk, 2012 | 16(80%)/13(65%) | 71.9/70.8 | PB-CD34+/NCT | IM | 3 | + | ①②④⑤ |
| Kirana, 2012 | 9(75%)/10(83%) | 68.5/70.9 | BM-MNC/TRC | IM or IA | 13 | ①③ | |
| Szabo, 2013 | 8(80%)/5(50%) | 60.6/63.0 | PBSC/NCT | IM | 1 and 3 | + | ①②③⑤ |
| Li, 2013 | 23(76%)/22(79%) | 61/63 | BMMNC/NCT | IM | 6 | ③ | |
| Gupta, 2013 | Unclear | 43/47.6 | BMMSC/NCT | IM | 6 and 24 | – | ①②③④ |
| Mohammadzadeh, 2013 | Unclear | 63.5/64.2 | PBSC/NCT | IM | 3 | ②③④ | |
| Raval, 2014 | 6(86%)/2(66%) | 65/85 | PB-CD133+/NCT | IM | 12 | ②③ | |
| Ansary, 2014 | 9(72%)/8(66%) | 50.5/61.7 | PBMNC/NCT | IM | 3 | + | ①②④ |
| Teraa, 2015 | 57(70%)/51(65%) | 69/65 | BMMNC/NCT | IA | 2 and 6 | + | ①②③④ |
| Skora, 2015 | 11(69%)/10(38%) | 66.7/68.3 | BMMNC/NCT | IM | 3 | + | ①②④ |
| Raposio, 2016 | 11(69%)/10(42%) | 70.7/74.5 | ASC+ PRP/NCT | IM | 18 | ① | |
| Pignon, 2017 | 13(72%)/18(90%) | 72/65 | BMMNC/NCT | IM | 6 and 12 | + | ②③ |
| Zollino, 2018 | 5(63%)/5(63%) | 74/68 | ASC/NCT | IM | 6 | + | ① |
| Lu, 2019 | Unclear | ≧64 | BMMSC/BMMNC/NCT | IM | 36 | No data | |
| Smith, 2020 | 5(92%)/6(100%)/4(66%) | 60.2/55.2 | ASC+PRP/ASC/NCT | Topical | 3 | ① |
| Study | Bias 1 | Bias 2 | Bias 3 | Bias 4 | Bias 5 | Bias 6 |
|---|---|---|---|---|---|---|
| Huang, 2005 | Low | Unclear | High | Unclear | Low | Low |
| Barc, 2006 | Low | Unclear | High | Unclear | Low | Low |
| Arai, 2006 | Low | Unclear | High | Unclear | Low | Low |
| Lu, 2008 | Unclear | Unclear | Unclear | Unclear | Low | Low |
| Dash, 2009 | Low | Low | High | Unclear | Low | High |
| Han, 2010 | Low | Low | Low | Unclear | Low | Unclear |
| Prochazka, 2010 | Low | Unclear | High | Unclear | Low | Low |
| Jain, 2011 | Low | Low | Low | Unclear | Low | Unclear |
| Lu, 2011 | Low | Unclear | Low | Low | Low | High |
| Walter, 2011 | Low | Unclear | Low | Low | Low | High |
| Powell, 2011 | Low | Unclear | Low | Low | High | Low |
| Iafrati, 2011 | Unclear | Low | Low | Low | Low | Low |
| Kirana, 2012 | Low | Unclear | Unclear | Unclear | Low | Unclear |
| Losordo, 2012 | Unclear | Unclear | Low | Low | High | High |
| Ozturk, 2012 | Low | Low | High | High | Low | Low |
| Gupta, 2013 | Low | Low | Low | Low | Low | Low |
| Mohammadzadeh, 2013 | Low | Unclear | Unclear | Unclear | Low | Low |
| Li, 2013 | Low | Unclear | High | Unclear | Low | Low |
| Szabo, 2013 | Low | Unclear | Unclear | Unclear | Low | Low |
| Raval, 2014 | Unclear | High | Low | Low | Low | Low |
| Ansary, 2014 | Unclear | Unclear | Low | Low | Low | Low |
| Skora, 2015 | Low | Unclear | High | Low | Low | Low |
| Teraa, 2015 | Low | Low | Low | Low | High | Low |
| Raposio, 2016 | Unclear | Unclear | Unclear | Unclear | Low | Unclear |
| Pignon, 2017 | Low | Unclear | Low | Low | Unclear | Unclear |
| Zollino, 2018 | Low | Unclear | Unclear | Unclear | Low | Unclear |
| Lu, 2019 | Unclear | Unclear | Low | Unclear | Low | Unclear |
| Smith, 2020 | Low | Low | High | Low | Low | Unclear |
| Outcome | Total Amputation Rate | Major Amputation Rate | Ankle Brachial Index | TcPO2 | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Subgroup | Studies/Cases | RR (95% CI) | I2 | Studies/Cases | RR (95% CI) | I2 | Studies/Cases | RR (95% CI) | I2 | Studies/Cases | RR (95% CI) | I2 | |
| Etiology | |||||||||||||
| CLI | 11/499 | 0.61 (0.45, 0.83) | 22% | 10/462 | 0.66 (0.44, 0.99) | 0% | 6/201 | 0.18 (0.04, 0.32) | 83% | 3/61 | 3.46 (0.23, 6.68) | 0% | |
| DM + CLI | 5/227 | 0.28 (0.11, 0.71) | 1% | 2/45 | 0.76 (0.02, 28.96) | 70% | 5/235 | 0.09 (0.01, 0.160 | 75% | 2/122 | 4.05 (−3.73, 11.84) | 43% | |
| Intervention | |||||||||||||
| Blood-derived | 7/186 | 0.41 (0.25, 0.69) | 1% | 4/75 | 0.40 (0.12, 1.28) | 31% | 4/132 | 0.28 (0.08, 0.49) | 82% | 2/60 | 6.92 (−3.87, 17.71) | 83% | |
| Bone marrow-derived | 9/540 | 0.62 (0.42, 0.890 | 28% | 8/432 | 0.73 (0.46, 1.16) | 0% | 7/304 | 0.06 (0.01, 0.10) | 57% | 3/123 | 2.50 (−0.87, 5.88) | 2% | |
| Follow-up time | |||||||||||||
| Short term (≦3 m) | 10/380 | 0.42 (0.28, 0.630 | 0% | 4/129 | 0.47 (0.11, 2.06) | 51% | 9/342 | 0.13 (0.06, 0.20) | 81% | 5/183 | 3.65 (−0.04, 7.34) | 48% | |
| Medium term (6 m) | 4/320 | 0.62 (0.38, 1.02) | 50% | 5/328 | 0.62 (0.39, 1.01) | 0% | 1/77 | 0.03 (−0.09, 0.15) | - | - | - | - | |
| Long term (≧12 m) | 2/26 | 1.70 (0.52, 5.500 | 0% | 3/50 | 1.349 (0.38, 4.69) | 0% | 1/17 | 0.17 (0.03, 0.31) | - | - | - | - | |
| Tumor marker | |||||||||||||
| CD34+ | 9/476 | 0.54 (0.37, 0.79) | 31% | 4/248 | 0.76 (0.3, 1.93) | 39% | 7/271 | 0.16 (0.05, 0.28) | 79% | 4/101 | 5.78 (0.72, 10.82) | 53% | |
| CD34– | 3/139 | 0.34 (0.04, 2.91) | 59% | 1/20 | 1.00 (0.17, 5.77) | - | 3/144 | 0.06 (−0.02, 0.14) | 79% | 1/82 | 0.10 (−4.29, 4.50) | 0% | |
| Overall | 16/726 | 0.55 (0.40, 0.75) | 25% | 12/507 | 0.66 (0.44, 0.98) | 0% | 11/436 | 0.12 (0.06, 0.18) | 78% | 5/183 | 3.65 (−0.04, 7.34) | 87% | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chiang, K.-J.; Chiu, L.-C.; Kang, Y.-N.; Chen, C. Autologous Stem Cell Therapy for Chronic Lower Extremity Wounds: A Meta-Analysis of Randomized Controlled Trials. Cells 2021, 10, 3307. https://doi.org/10.3390/cells10123307
Chiang K-J, Chiu L-C, Kang Y-N, Chen C. Autologous Stem Cell Therapy for Chronic Lower Extremity Wounds: A Meta-Analysis of Randomized Controlled Trials. Cells. 2021; 10(12):3307. https://doi.org/10.3390/cells10123307
Chicago/Turabian StyleChiang, Kuan-Ju, Li-Cheng Chiu, Yi-No Kang, and Chiehfeng Chen. 2021. "Autologous Stem Cell Therapy for Chronic Lower Extremity Wounds: A Meta-Analysis of Randomized Controlled Trials" Cells 10, no. 12: 3307. https://doi.org/10.3390/cells10123307
APA StyleChiang, K.-J., Chiu, L.-C., Kang, Y.-N., & Chen, C. (2021). Autologous Stem Cell Therapy for Chronic Lower Extremity Wounds: A Meta-Analysis of Randomized Controlled Trials. Cells, 10(12), 3307. https://doi.org/10.3390/cells10123307