
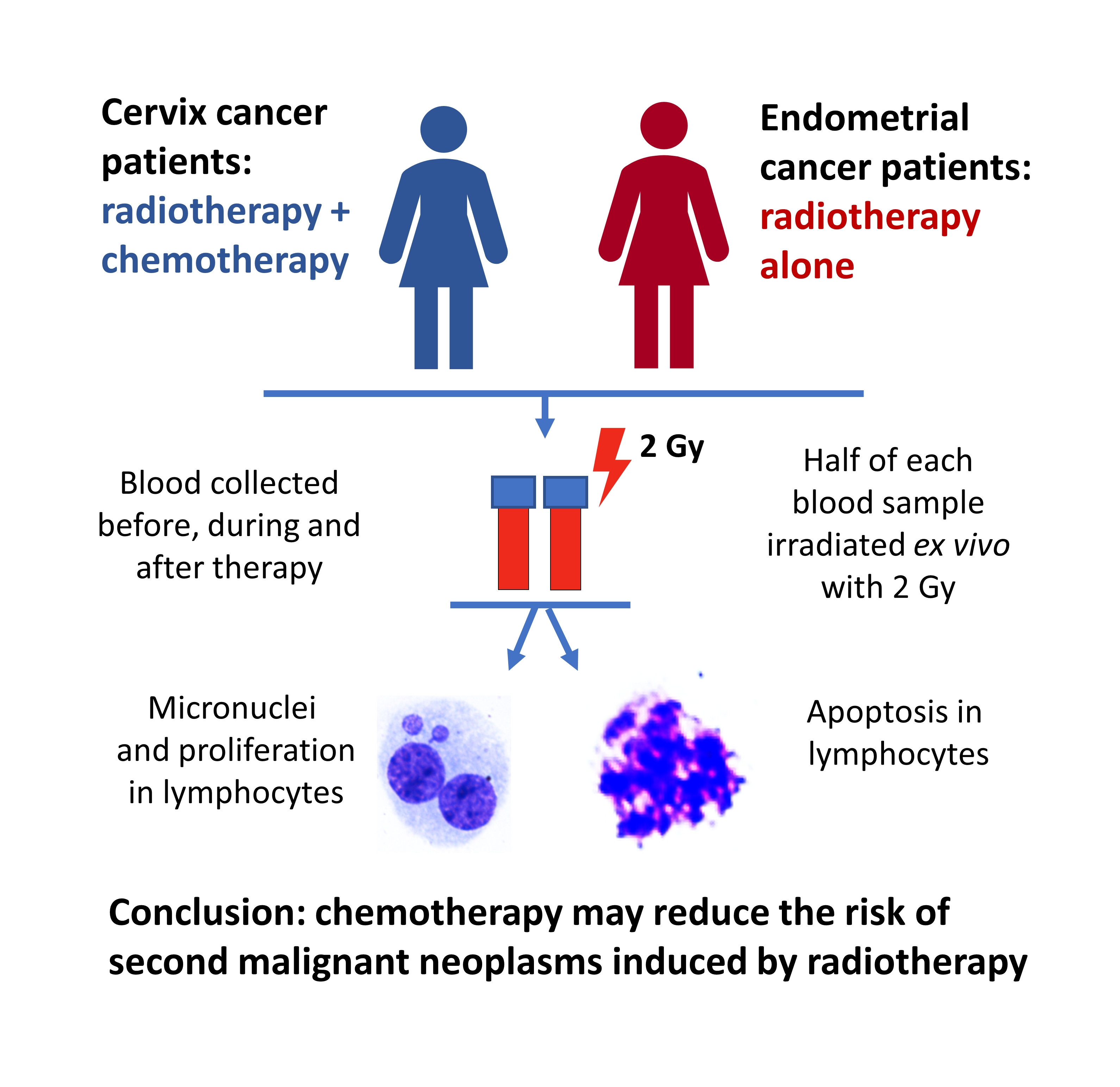
Cisplatin Reduces the Frequencies of Radiotherapy-Induced Micronuclei in Peripheral Blood Lymphocytes of Patients with Gynaecological Cancer: Possible Implications for the Risk of Second Malignant Neoplasms

 , , , and
, , , and
Abstract

1. Introduction
2. Materials and Methods
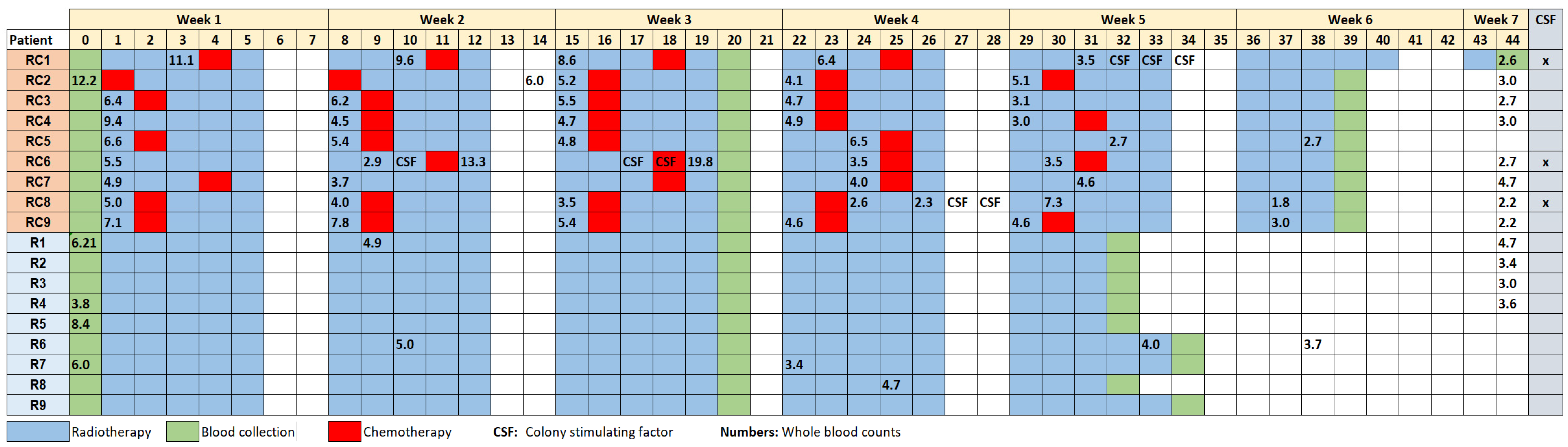
2.1. Cervix and Endometrial Cancer Patients
2.2. Blood Sample Processing and Ex Vivo Irradiation
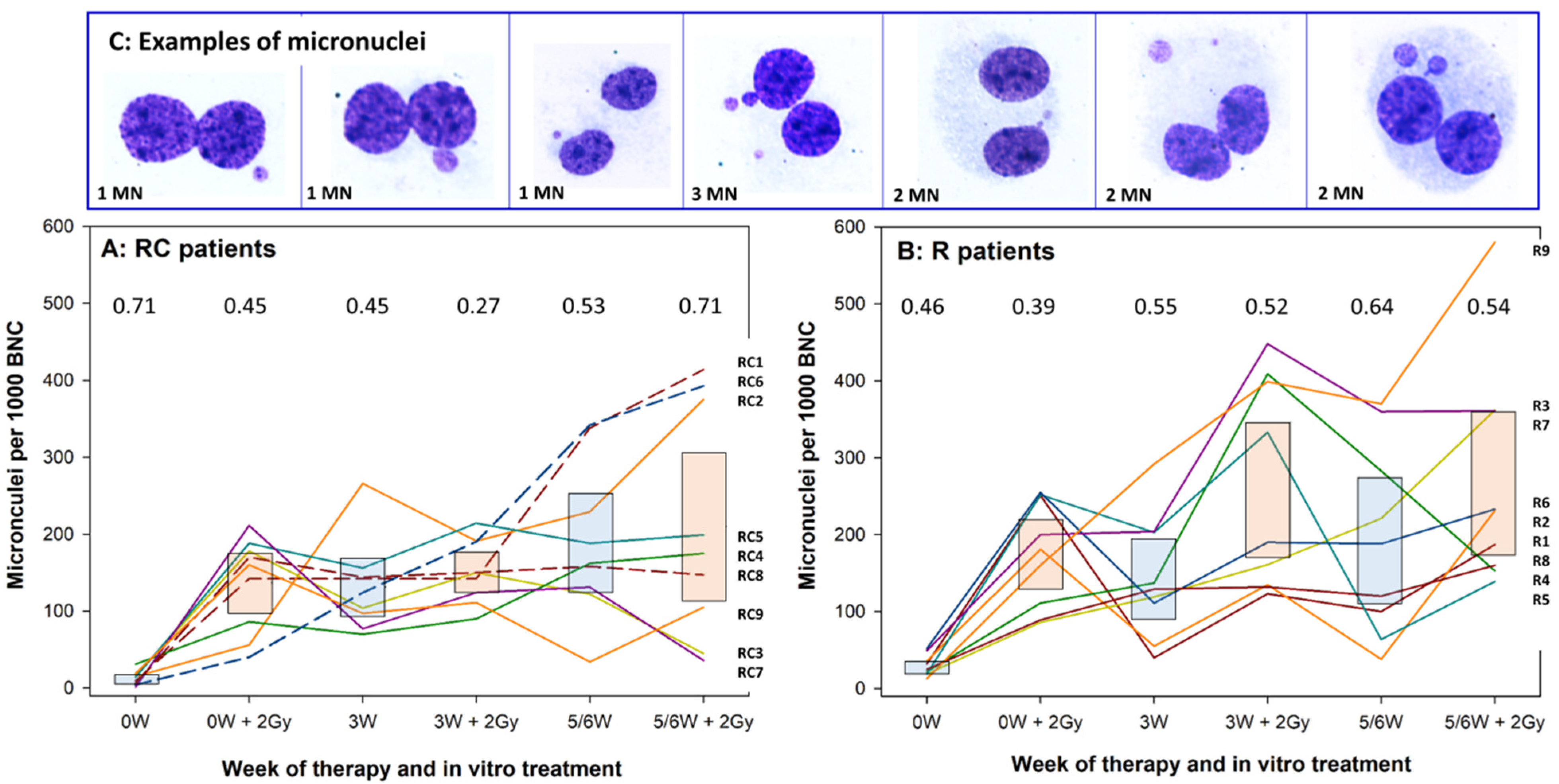
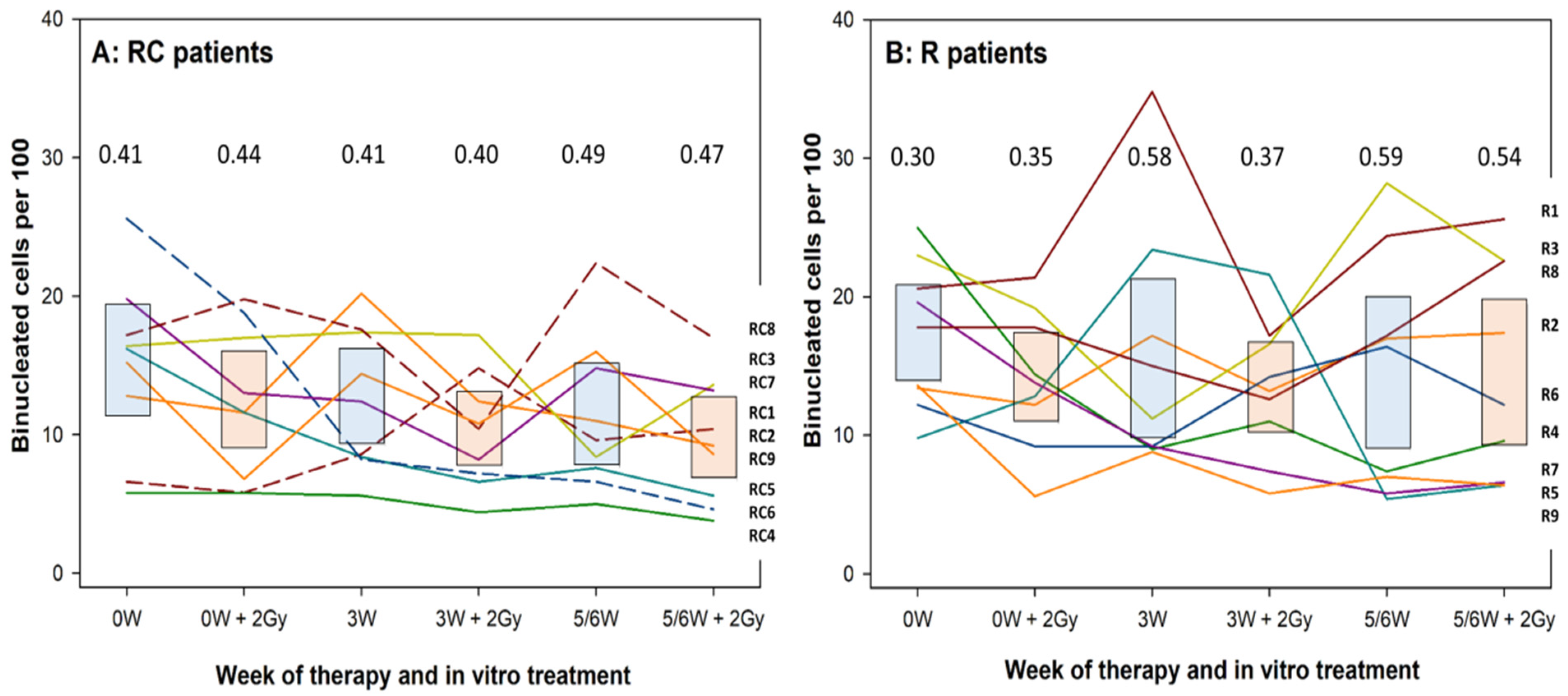
2.3. Cell Culture and the Micronucleus Assay
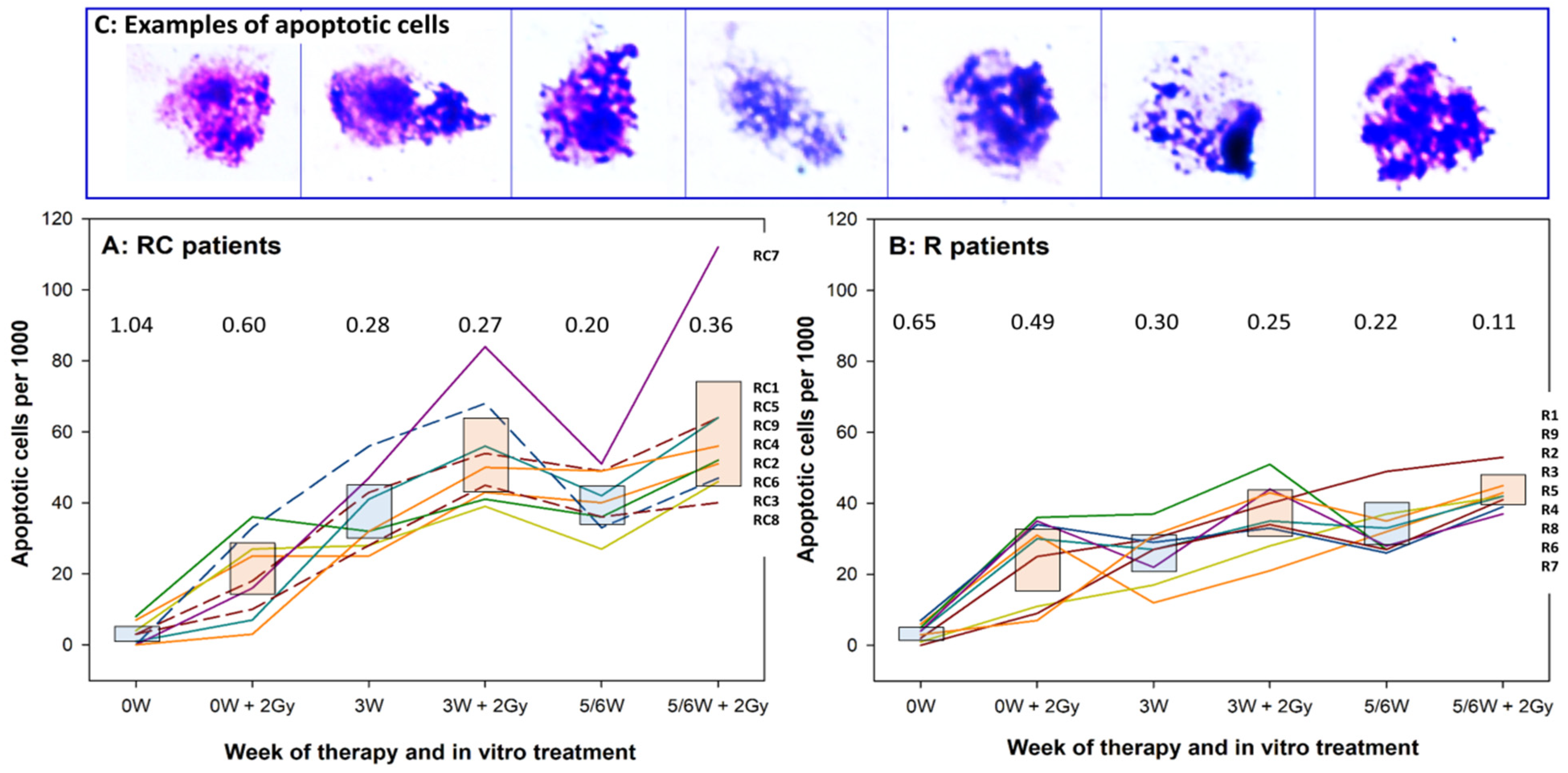
2.4. Morphological Observation of Apoptotic Cells
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Miller, K.D.; Nogueira, L.; Mariotto, A.B.; Rowland, J.H.; Yabroff, K.R.; Alfano, C.M.; Jemal, A.; Kramer, J.L.; Siegel, R.L. Cancer treatment and survivorship statistics, 2019. CA Cancer J. Clin. 2019, 69, 363–385. [Google Scholar] [CrossRef] [PubMed]
- Morton, L.M.; Onel, K.; Curtis, R.E.; Hungate, E.A.; Armstrong, G.T. The rising incidence of second cancers: Patterns of occurrence and identification of risk factors for children and adults. Am. Soc. Clin. Oncol. Educ. Book 2014, e57–e67. [Google Scholar] [CrossRef] [PubMed]
- Gray, L.H. Cellular Radiation Biology: A Symposium Considering Radiation Effects in the Cell and Possible Implications for Cancer Therapy; A Collection of Papers Presented at the 18. Annual Symposium on Fundamental Cancer Research, 1964; Williams and Wilkins: Philadelphia, PA, USA, 1965. [Google Scholar]
- Upton, A.C. The dose-response relation in radiation-induced cancer. Cancer Res. 1961, 21, 717–729. [Google Scholar]
- Dasu, A.; Toma-Dasu, I. Models for the risk of secondary cancers from radiation therapy. Phys. Med. 2017, 42, 232–238. [Google Scholar] [CrossRef] [PubMed]
- Sachs, R.K.; Brenner, D.J. Solid tumor risks after high doses of ionizing radiation. Proc. Natl. Acad. Sci. USA 2005, 102, 13040–13045. [Google Scholar] [CrossRef]
- Diallo, I.; Haddy, N.; Adjadj, E.; Samand, A.; Quiniou, E.; Chavaudra, J.; Alziar, I.; Perret, N.; Guerin, S.; Lefkopoulos, D.; et al. Frequency distribution of second solid cancer locations in relation to the irradiated volume among 115 patients treated for childhood cancer. Int. J. Radiat. Oncol. Biol. Phys. 2009, 74, 876–883. [Google Scholar] [CrossRef]
- Dorr, W.; Herrmann, T. Cancer induction by radiotherapy: Dose dependence and spatial relationship to irradiated volume. J. Radiol. Prot. 2002, 22, A117–A121. [Google Scholar] [CrossRef]
- Schneider, U.; Walsh, L.; Newhauser, W. Tumour size can have an impact on the outcomes of epidemiological studies on second cancers after radiotherapy. Radiat. Environ. Biophys. 2018, 57, 311–319. [Google Scholar] [CrossRef]
- Boice, J.D., Jr.; Engholm, G.; Kleinerman, R.A.; Blettner, M.; Stovall, M.; Lisco, H.; Moloney, W.C.; Austin, D.F.; Bosch, A.; Cookfair, D.L.; et al. Radiation dose and second cancer risk in patients treated for cancer of the cervix. Radiat. Res. 1988, 116, 3–55. [Google Scholar] [CrossRef]
- Boffetta, P.; Kaldor, J.M. Secondary malignancies following cancer chemotherapy. Acta Oncol. 1994, 33, 591–598. [Google Scholar] [CrossRef]
- Morton, L.M.; Dores, G.M.; Tucker, M.A.; Kim, C.J.; Onel, K.; Gilbert, E.S.; Fraumeni, J.F., Jr.; Curtis, R.E. Evolving risk of therapy-related acute myeloid leukemia following cancer chemotherapy among adults in the United States, 1975-2008. Blood 2013, 121, 2996–3004. [Google Scholar] [CrossRef]
- Liang, F.; Zhang, S.; Xue, H.; Chen, Q. Risk of second primary cancers in cancer patients treated with cisplatin: A systematic review and meta-analysis of randomized studies. BMC Cancer 2017, 17, 871. [Google Scholar] [CrossRef]
- Teepen, J.C.; van Leeuwen, F.E.; Tissing, W.J.; van Dulmen-den Broeder, E.; van den Heuvel-Eibrink, M.M.; van der Pal, H.J.; Loonen, J.J.; Bresters, D.; Versluys, B.; Neggers, S.; et al. Long-Term Risk of Subsequent Malignant Neoplasms After Treatment of Childhood Cancer in the DCOG LATER Study Cohort: Role of Chemotherapy. J. Clin. Oncol. 2017, 35, 2288–2298. [Google Scholar] [CrossRef] [PubMed]
- Pedersen-Bjergaard, J.; Daugaard, G.; Hansen, S.W.; Philip, P.; Larsen, S.O.; Rorth, M. Increased risk of myelodysplasia and leukaemia after etoposide, cisplatin, and bleomycin for germ-cell tumours. Lancet 1991, 338, 359–363. [Google Scholar] [CrossRef]
- Veiga, L.H.; Curtis, R.E.; Morton, L.M.; Withrow, D.R.; Howell, R.M.; Smith, S.A.; Weathers, R.E.; Oeffinger, K.C.; Moskowitz, C.S.; Henderson, T.O.; et al. Association of Breast Cancer Risk After Childhood Cancer With Radiation Dose to the Breast and Anthracycline Use: A Report From the Childhood Cancer Survivor Study. JAMA Pediatr. 2019, 173, 1171–1179. [Google Scholar] [CrossRef] [PubMed]
- Turcotte, L.M.; Liu, Q.; Yasui, Y.; Henderson, T.O.; Gibson, T.M.; Leisenring, W.; Arnold, M.A.; Howell, R.M.; Green, D.M.; Armstrong, G.T. Chemotherapy and risk of subsequent malignant neoplasms in the Childhood Cancer Survivor Study cohort. J. Clin. Oncol. 2019, 37, 3310. [Google Scholar] [CrossRef]
- Preston, R.J. Can radiation research impact the estimation of risk? Int. J. Radiat. Biol. 2017, 93, 1009–1014. [Google Scholar] [CrossRef] [PubMed]
- Solomon, E.; Borrow, J.; Goddard, A.D. Chromosome aberrations and cancer. Science 1991, 254, 1153–1160. [Google Scholar] [CrossRef]
- Savage, J.R.K. Classification and relationship of induced chromosomal structural changes. J. Med. Genet. 1975, 12, 103–122. [Google Scholar]
- Fenech, M. The in vitro micronucleus technique. Mutat. Res. 2000, 455, 81–95. [Google Scholar] [CrossRef]
- Fenech, M. Cytokinesis-block micronucleus cytome assay. Nat. Protoc. 2007, 2, 1084–1104. [Google Scholar] [CrossRef]
- Gantenberg, H.-W.; Wuttke, K.; Streffer, C.; Müller, W.-U. Micronuclei in human lymphocytes irradiated in vitro or in vivo. Radiat. Res. 1991, 128, 276–281. [Google Scholar] [CrossRef]
- Johannes, C.; Dixius, A.; Pust, M.; Hentschel, R.; Buraczewska, I.; Staaf, E.; Brehwens, K.; Haghdoost, S.; Nievaart, S.; Czub, J.; et al. The yield of radiation-induced micronuclei in early and late-arising binucleated cells depends on radiation quality. Mutat. Res. 2010, 701, 80–85. [Google Scholar] [CrossRef]
- Wuttke, K.; Muller, W.U.; Streffer, C. The sensitivity of the in vitro cytokinesis-blocked micronucleus assay in lymphocytes for different and combined radiation qualities. Strahlenther. Onkol. 1998, 174, 262–268. [Google Scholar] [CrossRef]
- Fenech, M.; Crott, J.; Turner, J.; Brown, S. Necrosis, apoptosis, cytostasis and DNA damage in human lymphocytes measured simultaneously within the cytokinesis-block micronucleus assay: Description of the method and results for hydrogen peroxide. Mutagenesis 1999, 14, 605–612. [Google Scholar] [CrossRef] [PubMed]
- Dronkert, M.L.G.; Kanaar, R. Repair of DNA interstrand cross-links. Mutat. Res. DNA Repair 2001, 486, 217–247. [Google Scholar] [CrossRef]
- Basourakos, S.P.; Li, L.; Aparicio, A.M.; Corn, P.G.; Kim, J.; Thompson, T.C. Combination Platinum-based and DNA Damage Response-targeting Cancer Therapy: Evolution and Future Directions. Curr. Med. Chem. 2017, 24, 1586–1606. [Google Scholar] [CrossRef]
- Krishnaswamy, G.; Dewey, W.C. Cisplatin induced cell killing and chromosomal aberrations in CHO cells: Treated during G1 or S phase. Mutat. Res. 1993, 293, 161–172. [Google Scholar] [CrossRef]
- Rjiba-Touati, K.; Ayed-Boussema, I.; Skhiri, H.; Belarbia, A.; Zellema, D.; Achour, A.; Bacha, H. Induction of DNA fragmentation, chromosome aberrations and micronuclei by cisplatin in rat bone-marrow cells: Protective effect of recombinant human erythropoietin. Mutat. Res. 2012, 747, 202–206. [Google Scholar] [CrossRef] [PubMed]
- Sak, A.; Grehl, S.; Engelhard, M.; Wierlemann, A.; Kaelberlah, H.P.; Erichsen, P.; Pottgen, C.; Groneberg, M.; Stuschke, M. Long-term in vivo effects of cisplatin on gamma-H2AX foci signaling in peripheral lymphocytes of tumor patients after irradiation. Clin. Cancer Res. 2009, 15, 2927–2934. [Google Scholar] [CrossRef] [PubMed]
- Liu, M.; Ma, S.; Liu, M.; Hou, Y.; Liang, B.; Su, X.; Liu, X. Synergistic killing of lung cancer cells by cisplatin and radiation via autophagy and apoptosis. Oncol. Lett. 2014, 7, 1903–1910. [Google Scholar] [CrossRef] [PubMed]
- Bergs, J.W.; Franken, N.A.; ten Cate, R.; van Bree, C.; Haveman, J. Effects of cisplatin and gamma-irradiation on cell survival, the induction of chromosomal aberrations and apoptosis in SW-1573 cells. Mutat. Res. 2006, 594, 148–154. [Google Scholar] [CrossRef] [PubMed]
- Schwachofer, J.H.; Crooijmans, R.P.; Hoogenhout, J.; Kal, H.B.; Theeuwes, A.G. Effectiveness in inhibition of recovery of cell survival by cisplatin and carboplatin: Influence of treatment sequence. Int. J. Radiat. Oncol. Biol. Phys. 1991, 20, 1235–1241. [Google Scholar] [CrossRef]
- Diggle, C.P.; Bentley, J.; Knowles, M.A.; Kiltie, A.E. Inhibition of double-strand break non-homologous end-joining by cisplatin adducts in human cell extracts. Nucleic Acids Res. 2005, 33, 2531–2539. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Wilson, G.D.; Bentzen, S.M.; Harari, P.M. Biologic basis for combining drugs with radiation. Semin. Radiat. Oncol. 2006, 16, 2–9. [Google Scholar] [CrossRef]
- Sears, C.R.; Turchi, J.J. Complex cisplatin-double strand break (DSB) lesions directly impair cellular non-homologous end-joining (NHEJ) independent of downstream damage response (DDR) pathways. J. Biol. Chem. 2012, 287, 24263–24272. [Google Scholar] [CrossRef]
- Boeckman, H.J.; Trego, K.S.; Turchi, J.J. Cisplatin sensitizes cancer cells to ionizing radiation via inhibition of nonhomologous end joining. Mol. Cancer Res. 2005, 3, 277–285. [Google Scholar] [CrossRef]
- Turchi, J.J.; Henkels, K.M.; Zhou, Y. Cisplatin-DNA adducts inhibit translocation of the Ku subunits of DNA-PK. Nucleic Acids Res. 2000, 28, 4634–4641. [Google Scholar] [CrossRef]
- Begg, A.C.; van der Kolk, P.J.; Dewit, L.; Bartelink, H. Radiosensitization by cisplatin of RIF1 tumour cells in vitro. Int. J. Radiat. Biol. Relat. Stud. Phys. Chem. Med. 1986, 50, 871–884. [Google Scholar] [CrossRef]
- Dewit, L. Combined treatment of radiation and cisdiamminedichloroplatinum (II): A review of experimental and clinical data. Int. J. Radiat. Oncol. Biol. Phys. 1987, 13, 403–426. [Google Scholar] [CrossRef]
- Urbanik, W.; Kukolowicz, P.; Kuszewski, T.; Gozdz, S.; Wojcik, A. Modelling the frequencies of chromosomal aberrations in peripheral lymphocytes of patients undergoing radiotherapy. Nukleonika 2003, 48, 3–8. [Google Scholar]
- De Berrington, G.A.; Curtis, R.E.; Kry, S.F.; Gilbert, E.; Lamart, S.; Berg, C.D.; Stovall, M.; Ron, E. Proportion of second cancers attributable to radiotherapy treatment in adults: A cohort study in the US SEER cancer registries. Lancet Oncol. 2011, 12, 353–360. [Google Scholar] [CrossRef]
- Zwahlen, D.R.; Ruben, J.D.; Jones, P.; Gagliardi, F.; Millar, J.L.; Schneider, U. Effect of intensity-modulated pelvic radiotherapy on second cancer risk in the postoperative treatment of endometrial and cervical cancer. Int. J. Radiat. Oncol. Biol. Phys. 2009, 74, 539–545. [Google Scholar] [CrossRef] [PubMed]
- Hemminki, K.; Dong, C.H.; Vaittinen, P. Second primary cancer after in situ and invasive cervical cancer. Epidemiology 2000, 11, 457–461. [Google Scholar] [CrossRef] [PubMed]
- Kleinerman, R.A.; Boice, J.D., Jr.; Storm, H.H.; Sparen, P.; Andersen, A.; Pukkala, E.; Lynch, C.F.; Hankey, B.F.; Flannery, J.T. Second primary cancer after treatment for cervical cancer. An international cancer registries study. Cancer 1995, 76, 442–452. [Google Scholar] [CrossRef]
- Arnold, M.; Liu, L.; Kenter, G.G.; Creutzberg, C.L.; Coebergh, J.W.; Soerjomataram, I. Second primary cancers in survivors of cervical cancer in The Netherlands: Implications for prevention and surveillance. Radiother. Oncol. 2014, 111, 374–381. [Google Scholar] [CrossRef]
- D’Angio, G.J.; Meadows, A.; Mike, V.; Harris, C.; Evans, A.; Jaffe, N.; Newton, W.; Schweisguth, O.; Sutow, W.; Morris-Jones, P. Decreased risk of radiation-associated second malignant neoplasms in actinomycin-D-treated patients. Cancer 1976, 37, 1177–1185. [Google Scholar] [CrossRef]
- Breslow, N.E.; Takashima, J.R.; Whitton, J.A.; Moksness, J.; D’Angio, G.J.; Green, D.M. Second malignant neoplasms following treatment for Wilm’s tumor: A report from the National Wilms’ Tumor Study Group. J. Clin. Oncol. 1995, 13, 1851–1859. [Google Scholar] [CrossRef] [PubMed]
- Guerin, S.; Guibout, C.; Shamsaldin, A.; Dondon, M.G.; Diallo, I.; Hawkins, M.; Oberlin, O.; Hartmann, O.; Michon, J.; Le Deley, M.C.; et al. Concomitant chemo-radiotherapy and local dose of radiation as risk factors for second malignant neoplasms after solid cancer in childhood: A case-control study. Int. J. Cancer 2007, 120, 96–102. [Google Scholar] [CrossRef]
- Haddy, N.; Le Deley, M.C.; Samand, A.; Diallo, I.; Guerin, S.; Guibout, C.; Oberlin, O.; Hawkins, M.; Zucker, J.M.; de Vathaire, F. Role of radiotherapy and chemotherapy in the risk of secondary leukaemia after a solid tumour in childhood. Eur. J. Cancer 2006, 42, 2757–2764. [Google Scholar] [CrossRef]
- Spensley, S.; Hunter, R.D.; Livsey, J.E.; Swindell, R.; Davidson, S.E. Clinical outcome for chemoradiotherapy in carcinoma of the cervix. Clin. Oncol. 2009, 21, 49–55. [Google Scholar] [CrossRef] [PubMed]
- Fridman, W.H.; Zitvogel, L.; Sautes-Fridman, C.; Kroemer, G. The immune contexture in cancer prognosis and treatment. Nat. Rev. Clin. Oncol. 2017, 14, 717–734. [Google Scholar] [CrossRef] [PubMed]
- Schaapveld, M.; Visser, O.; Louwman, M.J.; de Vries, E.G.E.; Willemse, P.H.B.; Otter, R.; van der Graaf, W.T.A.; Coebergh, J.W.W.; van Leeuwen, F.E. Risk of new primary nonbreast cancers after breast cancer treatment: A Dutch population-based study. J. Clin. Oncol. 2008, 26, 1239–1246. [Google Scholar] [CrossRef]
- Li, D.; Weng, S.S.; Zhong, C.H.; Tang, X.J.; Zhu, N.; Cheng, Y.; Xu, D.; Yuan, Y. Risk of Second Primary Cancers Among Long-Term Survivors of Breast Cancer. Front. Oncol. 2020, 9. [Google Scholar] [CrossRef] [PubMed]
- Travis, L.B.; Hill, D.A.; Dores, G.M.; Gospodarowicz, M.; van Leeuwen, F.E.; Holowaty, E.; Glimelius, B.; Andersson, M.; Wiklund, T.; Lynch, C.F.; et al. Breast cancer following radiotherapy and chemotherapy among young women with Hodgkin disease. JAMA 2003, 290, 465–475. [Google Scholar] [CrossRef]
- Schaapveld, M.; Aleman, B.M.; van Eggermond, A.M.; Janus, C.P.; Krol, A.D.; van der Maazen, R.W.; Roesink, J.; Raemaekers, J.M.; de Boer, J.P.; Zijlstra, J.M.; et al. Second Cancer Risk Up to 40 Years after Treatment for Hodgkin’s Lymphoma. N. Engl. J. Med. 2015, 373, 2499–2511. [Google Scholar] [CrossRef]
- Hanahan, D.; Weinberg, R.A. Hallmarks of cancer: The next generation. Cell 2011, 144, 646–674. [Google Scholar] [CrossRef]
- Fouad, Y.A.; Aanei, C. Revisiting the hallmarks of cancer. Am. J. Cancer Res. 2017, 7, 1016–1036. [Google Scholar]
- Blagosklonny, M.V. Carcinogenesis, cancer therapy and chemoprevention. Cell Death Differ. 2005, 12, 592–602. [Google Scholar] [CrossRef]
- Zitvogel, L.; Apetoh, L.; Ghiringhelli, F.; Kroemer, G. Immunological aspects of cancer chemotherapy. Nat. Rev. Immunol. 2008, 8, 59–73. [Google Scholar] [CrossRef]
- Inskip, P.D.; Sigurdson, A.J.; Veiga, L.; Bhatti, P.; Ronckers, C.; Rajaraman, P.; Boukheris, H.; Stovall, M.; Smith, S.; Hammond, S.; et al. Radiation-Related New Primary Solid Cancers in the Childhood Cancer Survivor Study: Comparative Radiation Dose Response and Modification of Treatment Effects. Int. J. Radiat. Oncol. Biol. Phys. 2016, 94, 800–807. [Google Scholar] [CrossRef]
- Rajaraman, P.; Hauptmann, M.; Bouffler, S.; Wojcik, A. Human individual radiation sensitivity and prospects for prediction. Ann. ICRP 2018. [Google Scholar] [CrossRef] [PubMed]
- Applegate, K.E.; Ruhm, W.; Wojcik, A.; Bourguignon, M.; Brenner, A.; Hamasaki, K.; Imai, T.; Imaizumi, M.; Imaoka, T.; Kakinuma, S.; et al. Individual response of humans to ionising radiation: Governing factors and importance for radiological protection. Radiat. Environ. Biophys. 2020. [Google Scholar] [CrossRef]
- Gomolka, M.; Blyth, B.; Bourguignon, M.; Badie, C.; Schmitz, A.; Talbot, C.; Hoeschen, C.; Salomaa, S. Potential screening assays for individual radiation sensitivity and susceptibility and their current validation state. Int. J. Radiat. Biol. 2020, 96, 280–296. [Google Scholar] [CrossRef] [PubMed]
- Vral, A.; Thierens, H.; Baeyens, A.; De Ridder, L. Chromosomal aberrations and in vitro radiosensitivity: Intra-individual versus inter-individual variability. Toxicol. Lett. 2004, 149, 345–352. [Google Scholar] [CrossRef] [PubMed]
- Vinnikov, V.; Hande, M.P.; Wilkins, R.; Wojcik, A.; Zubizarreta, E.; Belyakov, O. Prediction of the Acute or Late Radiation Toxicity Effects in Radiotherapy Patients Using Ex Vivo Induced Biodosimetric Markers: A Review. J. Pers. Med. 2020, 10, 285. [Google Scholar] [CrossRef]
- Heuser, M.; Ganser, A.; Bokemeyer, C.; American Society of Clinical Oncology; National Comprehensive Cancer Network; European Organization for Research and Treatment of Cancer. Use of colony-stimulating factors for chemotherapy-associated neutropenia: Review of current guidelines. Semin. Hematol. 2007, 44, 148–156. [Google Scholar] [CrossRef]
- Müller, W.-U.; Streffer, C. Micronucleus assays. Adv. Mutagen. Res. 1994, 5, 1–134. [Google Scholar]
- Padjas, A.; Lesisz, D.; Lankoff, A.; Banasik, A.; Lisowska, H.; Bakalarz, R.; Gozdz, S.; Wojcik, A. Cytogenetic damage in lymphocytes of patients undergoing therapy for small cell lung cancer and ovarian carcinoma. Toxicol. Appl. Pharmacol. 2005, 209, 183–191. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Code | Age (Years) | FIGO Stage | Total Dose/Number of Fractions/Technique | Field Number/Mean Field Size (cm2) | CDDP Cycles | CSF |
|---|---|---|---|---|---|---|
| RC1 | 54 | III | 50.4 Gy/28 fractions + 5.4 Gy/3 fractions/3D-B | 3/344 ± 48 | 4 | yes |
| RC2 | 53 | IIB | 50.4 Gy/28 fractions/3D-MLC | 5/373 ± 190 | 5 | no |
| RC3 | 43 | IIB | 50.4 Gy/28 fractions/3D-B | 5/312 ± 145 | 4 | no |
| RC4 | 71 | IIB | 50.4 Gy/28 fractions/3D-B | 4/185 ± 168 | 4 | no |
| RC5 | 54 | IB | 50.4 Gy/28 fractions/3D-B | 3/376 ± 41 | 4 | no |
| RC6 | 53 | IB | 50.4 Gy/28 fractions/3D-MLC | 5/235 ± 172 | 4 | yes |
| RC7 | 76 | IIB | 50.4 Gy/28 fractions/3D-B | 4/267 ± 143 | 3 | no |
| RC8 | 52 | I | 50.4 Gy/28 fractions/3D-B | 4/262 ± 146 | 4 | yes |
| RC9 | 54 | III | 50.4 Gy/28 fractions/3D-MLC | 4/328 ± 173 | 5 | no |
| R1 | 59 | II | 46.0 Gy/23 fractions/3D-MLC | 6/188 ± 130 | ||
| R2 | 66 | I | 46.0 Gy/23 fractions/3D-B | 5/188 ± 130 | ||
| R3 | 63 | I | 46.0 Gy/23 fractions/3D-B | 5/186 ± 144 | ||
| R4 | 63 | IB | 46.0 Gy/23 fractions/3D-B | 4/274 ± 163 | ||
| R5 | 67 | I | 46.0 Gy/23 fractions/3D-B | 4/239 ± 57 | ||
| R6 | 76 | I | 50.0 Gy/25 fractions/3D-MLC | 5/255 ± 204 | ||
| R7 | 55 | III | 50.0 Gy/25 fractions/3D-MLC | 5/255 ± 196 | ||
| R8 | 68 | I | 46.0 Gy/23 fractions/3D-MLC | 6/179 ± 116 | ||
| R9 | 44 | I | 50.0 Gy/25 fractions/3D-MLC | 5/308 ± 168 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Węgierek-Ciuk, A.; Lankoff, A.; Lisowska, H.; Kędzierawski, P.; Akuwudike, P.; Lundholm, L.; Wojcik, A. Cisplatin Reduces the Frequencies of Radiotherapy-Induced Micronuclei in Peripheral Blood Lymphocytes of Patients with Gynaecological Cancer: Possible Implications for the Risk of Second Malignant Neoplasms. Cells 2021, 10, 2709. https://doi.org/10.3390/cells10102709
Węgierek-Ciuk A, Lankoff A, Lisowska H, Kędzierawski P, Akuwudike P, Lundholm L, Wojcik A. Cisplatin Reduces the Frequencies of Radiotherapy-Induced Micronuclei in Peripheral Blood Lymphocytes of Patients with Gynaecological Cancer: Possible Implications for the Risk of Second Malignant Neoplasms. Cells. 2021; 10(10):2709. https://doi.org/10.3390/cells10102709
Chicago/Turabian StyleWęgierek-Ciuk, Aneta, Anna Lankoff, Halina Lisowska, Piotr Kędzierawski, Pamela Akuwudike, Lovisa Lundholm, and Andrzej Wojcik. 2021. "Cisplatin Reduces the Frequencies of Radiotherapy-Induced Micronuclei in Peripheral Blood Lymphocytes of Patients with Gynaecological Cancer: Possible Implications for the Risk of Second Malignant Neoplasms" Cells 10, no. 10: 2709. https://doi.org/10.3390/cells10102709
APA StyleWęgierek-Ciuk, A., Lankoff, A., Lisowska, H., Kędzierawski, P., Akuwudike, P., Lundholm, L., & Wojcik, A. (2021). Cisplatin Reduces the Frequencies of Radiotherapy-Induced Micronuclei in Peripheral Blood Lymphocytes of Patients with Gynaecological Cancer: Possible Implications for the Risk of Second Malignant Neoplasms. Cells, 10(10), 2709. https://doi.org/10.3390/cells10102709