
Three-Dimensional Manufacturing of Mandibular Total Edentulous Simulation Model for In Vitro Studies—Concept and Validation

 ,
,  , ,
, ,  and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Materials
2.2.1. Development of the 3D Model Using Stereolithography
- 3D Scanning: The plaster model was scanned using a DS-EX Pro desktop scanner (Shining 3D®, Curitiba, Brazil), and the digital file was exported in STL format.
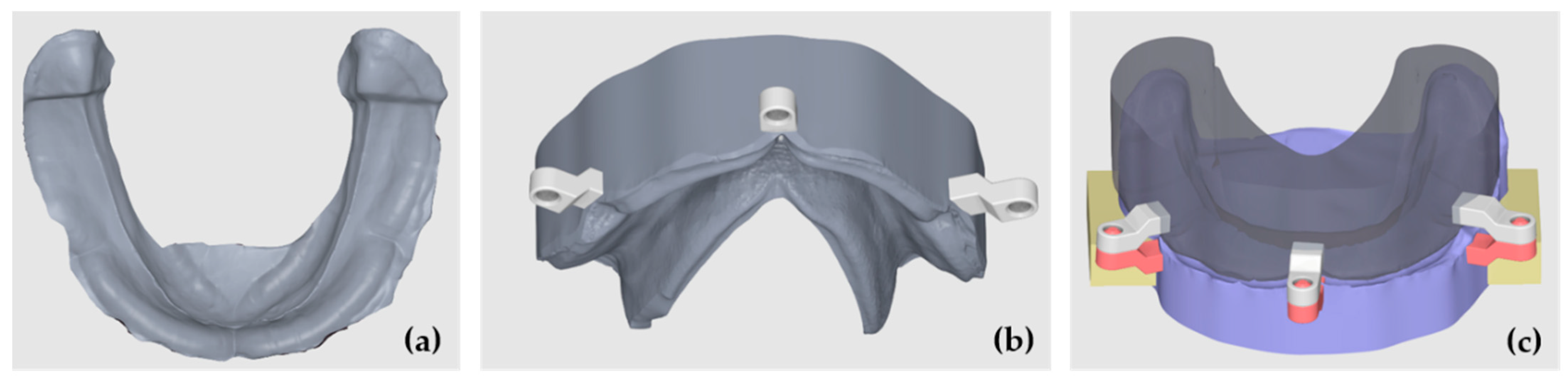
- Initial CAD Preparation: The STL file was imported into Meshmixer® (Autodesk® Inc.), aligned with the XYZ coordinate system, and oriented parallel to the Y-plane to standardize positioning for modeling and comparison (Figure 1a).
- Tooth Library Import and Positioning: A generic STL tooth library was imported containing teeth 47 to 37. The teeth were scaled proportionally and positioned over the crest to represent a standard full-arch tooth setup for a mandibular complete denture. The third molars were ignored and were not included in the section (Figure 1b).
- Digital Model Duplication and Sectioning: The aligned STL model was duplicated. One copy was digitally sectioned in the mesio-distal direction at each edentulous tooth site, corresponding to the tooth axes (e.g., between 47 and 46, 46 and 45, etc.) (Figure 1c).
- The Calculation and Application of Negative Offsets: In each digital section, a negative offset (i.e., inward shrinkage) was applied to simulate the mucosal layer thickness. The offset values were calculated based on the mean soft tissue thicknesses reported by Dong Jian et al. [27] for each specific site of the mandibular crest (e.g., ~2.0 mm anteriorly, ~3.0 mm posteriorly), as detailed in Table 1. This step effectively “reduces” the bone crest in each region by the average mucosal thickness, generating an estimated virtual mucosal profile (Figure 1d).
- Model Recompositing: The offset-modified sections were digitally stitched together to reconstruct a full mandibular arch model with a virtual soft tissue layer removed, thus simulating the underlying bony ridge (Figure 2a).
- Digital Tray Inversion: To generate a negative impression tray of the mucosa, the original (pre-offset) STL model was inverted using Boolean subtraction, resulting in an internal geometry that replicates the gingival surface of the mucosa (Figure 2b).
- Finalization for Printing: The resulting models (reduced bone crest and negative mucosa tray) were made watertight, thickened, and prepared for resin printing. The wall thicknesses were adjusted to ≥2 mm to ensure structural integrity during additive manufacturing.
2.2.2. Simulation Mucosa Elaboration
2.2.3. Validation of 3D Model Stability
2.2.4. Sample Size
2.2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ling, L.; Taremi, N.; Malyala, R. A Novel Low-Shrinkage Resin for 3D Printing. J. Dent. 2022, 118, 103957. [Google Scholar] [CrossRef] [PubMed]
- Blatz, M.B.; Conejo, J. The Current State of Chairside Digital Dentistry and Materials. Dent. Clin. N. Am. 2019, 631, 75–97. [Google Scholar] [CrossRef] [PubMed]
- Rekow, E.D. Digital dentistry: The new state of the art—Is it disruptive or destructive? Dent. Mater. 2020, 36, 9–24. [Google Scholar] [CrossRef] [PubMed]
- Jeong, M.; Radomski, K.; Lopez, D.; Liu, J.T.; Lee, J.D.; Lee, S.J. Materials and Applications of 3D Printing Technology in Dentistry: An Overview. Dent. J. 2024, 12, 1. [Google Scholar] [CrossRef]
- Peng, L.; Chen, L.; Harris, B.T.; Bhandari, B.; Morton, D.; Lin, W.S. Accuracy and reproducibility of virtual edentulous casts created by laboratory impression scan protocols. J. Prosthet. Dent. 2018, 1203, 89–95. [Google Scholar] [CrossRef]
- Nassani, M.Z.; Ibraheem, S.; Shamsy, E.; Darwish, M.; Faden, A.; Kujan, O. A Survey of Dentists’ Perception of Chair-Side CAD/CAM Technology. Healthcare 2021, 9, 68. [Google Scholar] [CrossRef] [PubMed]
- ISO/ASTM 52900-15; Additive Manufacturing—General Principles—Fundamentals and Vocabulary. International Organization for Standardization: Geneva, Switzerland, 2015.
- Kessler, A.; Hickel, R.; Reymus, M. 3D printing in dentistry-state of the art. Oper. Dent. 2020, 45, 30–40. [Google Scholar] [CrossRef]
- Tian, Y.; Chen, C.; Xu, X.; Wang, J.; Hou, X.; Li, K.; Lu, X.; Shi, H.; Lee, E.-S.; Jiang, H.B. A Review of 3D Printing in Dentistry: Technologies, Affecting Factors, and Applications. Scanning 2021, 2021, 9950131. [Google Scholar] [CrossRef]
- Revilla-León, M.; Sadeghpour, M.; Özcan, M. An update on applications of 3D printing technologies used for processing polymers used in implant dentistry. Odontology 2020, 1083, 31–38. [Google Scholar] [CrossRef]
- Ammoun, R.; Elkassaby, H.; Chien, E.C.; Goodacre, B.; Grant, G.T.; Sadid-Zadeh, R. Glossary of Digital Dental Terms, 2nd Edition: American College of Prosthodontists and ACP Education Foundation. J. Prosthodont. 2021, 30, 172–181. [Google Scholar] [CrossRef]
- Nogueira, T.E.; Schimmel, M.; Leles, C.R. Changes in masticatory performance of edentulous patients treated with single-implant mandibular overdentures and conventional complete dentures. J. Oral. Rehabil. 2019, 462, 68–73. [Google Scholar] [CrossRef]
- Thakur, J.; Parlani, S.; Shivakumar, S.; Jajoo, K. Accuracy of marginal fit of an implant-supported framework fabricated by 3D printing versus subtractive manufacturing technique: A systematic review and meta-analysis. J. Prosthet. Dent. 2023, 129, 301–309. [Google Scholar] [CrossRef] [PubMed]
- Banjar, A.; Chen, Y.; Kostagianni, A.; Finkelman, M.; Papathanasiou, A.; Chochlidakis, K.; Papaspyridakos, P. Accuracy of 3D Printed Implant Casts Versus Stone Casts: A Comparative Study in the Anterior Maxilla. J. Prosthodont. 2021, 307, 83–88. [Google Scholar] [CrossRef] [PubMed]
- Emir, F.; Ayyildiz, S. Accuracy evaluation of complete-arch models manufactured by three different 3d printing technologies: A three-dimensional analysis. J. Prosthodont. Res. 2021, 653, 65–70. [Google Scholar] [CrossRef] [PubMed]
- Schweiger, J.; Edelhoff, D.; Güth, J.F. 3D printing in digital prosthetic dentistry: An overview of recent developments in additive manufacturing. J. Clin. Med. 2021, 10, 2010. [Google Scholar] [CrossRef] [PubMed]
- Mehra, P.; Miner, J.; D’Innocenzo, R.; Nadershah, M. Use of 3-D Stereolithographic Models in Oral and Maxillofacial Surgery. J. Maxillofac. Oral Surg. 2011, 10, 6–13. [Google Scholar] [CrossRef]
- Richter, M.; Peter, T.; Rüttermann, S.; Sader, R.; Seifert, L.B. 3D printed versus commercial models in undergraduate conservative dentistry training. Eur. J. Dent. Educ. 2022, 266, 43–51. [Google Scholar] [CrossRef] [PubMed]
- Park, M.E.; Shin, S.Y. Three-dimensional comparative study on the accuracy and reproducibility of dental casts fabricated by 3D printers. J. Prosthet. Dent. 2018, 1198, 861.E1–861.E7. [Google Scholar] [CrossRef]
- Lan, D.; Luo, Y.; Qu, Y.; Man, Y. The three-dimensional stability and accuracy of 3D printing surgical templates: An In Vitro study. J. Dent. 2024, 144, 104936. [Google Scholar] [CrossRef]
- Ellakany, P.; Aly, N.M.; Al-Harbi, F. Accuracy of 3D Printed and Digital Casts Produced from Intraoral and Extraoral Scanners with Different Scanning Technologies: In Vitro Study. J. Prosthodont. 2022, 315, 21–28. [Google Scholar] [CrossRef]
- Papaspyridakos, P.; Chen, Y.-W.; Alshawaf, B.; Kang, K.; Finkelman, M.; Chronopoulos, V.; Weber, H.-P. Digital workflow: In vitro accuracy of 3D printed casts generated from complete-arch digital implant scans. J. Prosthet. Dent. 2020, 1245, 89–93. [Google Scholar] [CrossRef] [PubMed]
- Masumi, S.I.; Makihara, E.; Yamamori, T.; Ohkawa, S. Effectiveness of denture space recording method in the prosthetic treatment of edentulous patients. J. Prosthodont. Res. 2022, 662, 21–25. [Google Scholar] [CrossRef] [PubMed]
- Grender, J.; Klukowska, M.; Milleman, K.; Milleman, J. A randomized crossover trial assessing denture adhesive for prevention of food infiltration among partial denture wearers. Am. J. Dent. 2024, 372, 16–21. [Google Scholar]
- Klukowska, M.; Grender, J.; Gossweiler, A. A randomized controlled trial assessing denture adhesive efficacy on denture retention across 13 hours. J. Prosthodont. 2024, 333, 24–29. [Google Scholar] [CrossRef]
- Ferro, K.J. The Glossary of Prosthodontic Terms: Ninth Edition. J. Prosthet. Dent. 2017, 117, e1–e105. [Google Scholar] [CrossRef]
- Kanazawa, M.; Tanoue, M.; Miyayasu, A.; Takeshita, S.; Sato, D.; Asami, M.; Lam, T.V.; Thu, K.M.; Oda, K.; Komagamine, Y.; et al. The patient general satisfaction of mandibular single-implant overdentures and conventional complete dentures: Study protocol for a randomized crossover trial. Medicine 2018, 97, e10721. [Google Scholar] [CrossRef]
- Polychronakis, N.; Sykaras, N.; Polyzois, G.; Lagouvardos, P. Removal of denture adhesives from PMMA and polyamide denture base materials. J. Appl. Oral Sci. 2021, 29, e20200448. [Google Scholar] [CrossRef]
- Munoz, C.A.; Gendreau, L.; Shanga, G.; Magnuszewski, T.; Fernandez, P.; Durocher, J. A Clinical Study to Evaluate Denture Adhesive Use in Well-Fitting Dentures. J. Prosthodont. 2012, 211, 23–29. [Google Scholar] [CrossRef]
- De Luca Canto, G.; Pachêco-Pereira, C.; Lagravere, M.O.; Flores-Mir, C.; Major, P.W. Intra-arch dimensional measurement validity of laser-scanned digital dental models compared with the original plaster models: A systematic review. Orthod. Craniofac Res. 2015, 186, 5–76. [Google Scholar] [CrossRef]
- Jang, Y.; Sim, J.Y.; Park, J.K.; Kim, W.C.; Kim, H.Y.; Kim, J.H. Accuracy of 3-unit fixed dental prostheses fabricated on 3D-printed casts. J. Prosthet. Dent. 2020, 1231, 35–42. [Google Scholar] [CrossRef]
- Jin, G.; Shin, S.H.; Shim, J.S.; Lee, K.W.; Kim, J.E. Accuracy of 3D printed models and implant-analog positions according to the implant-analog–holder offset, inner structure, and printing layer thickness: An in-vitro study. J. Dent. 2022, 125, 104268. [Google Scholar] [CrossRef] [PubMed]
- Müller, H.-P.; Schaller, N.; Eger, T.; Heinecke, A. Thickness of masticatory mucosa. J. Clin. Periodontol. 2000, 27, 431–436. [Google Scholar] [CrossRef]
- Choi, J.J.E.; Chen, S.; Waddell, J.N. Investigation of dental elastomers as oral mucosa simulant materials. Clin. Exp. Dent. Res. 2021, 77, 54–62. [Google Scholar] [CrossRef] [PubMed]
- Dong, J.; Zhang, F.Y.; Wu, G.H.; Zhang, W.; Yin, J. Measurement of mucosal thickness in denture-bearing area of edentulous mandible. Chin. Med. J. 2015, 1283, 42–47. [Google Scholar] [CrossRef]
- Told, R.; Ujfalusi, Z.; Pentek, A.; Kerenyi, M.; Banfai, K.; Vizi, A.; Szabo, P.; Melegh, S.; Bovari-Biri, J.; Pongracz, J.E.; et al. A state-of-the-art guide to the sterilization of thermoplastic polymers and resin materials used in the additive manufacturing of medical devices. Mater. Des. 2022, 223, 111119. [Google Scholar] [CrossRef]
- Martelli, N.; Serrano, C.; van den Brink, H.; Pineau, J.; Prognon, P.; Borget, I.; El Batti, S. Advantages and disadvantages of 3-dimensional printing in surgery: A systematic review. Surgery 2016, 159, 1485–1500. [Google Scholar] [CrossRef] [PubMed]
- Ballard, D.H.; Trace, A.P.; Ali, S.; Hodgdon, T.; Zygmont, M.E.; DeBenedectis, C.M.; Smith, S.E.; Richardson, M.L.; Patel, M.M.; Decker, S.J.; et al. Clinical applications of 3D printing: Primer for radiologists. Acad. Radiol. 2017, 25, 52–65. [Google Scholar] [CrossRef]
- Afzali, A.; Clark, C.; Dhaliwal, A.; Yu, K.; Puglisi, J. 3D-Printed Anatomical Models Allowing for Customization. Biomed. J. Sci. Tech. Res. 2023, 47, 38146–38148. [Google Scholar] [CrossRef]
- Mendes, J.; Mendes, J.M.; Coelho, L.; Aroso, C.; Brizuela-Velasco, A.; Esteves, J.L.; Manzanares-Céspedes, M.C. Evaluation of Oral Mucosa Elastomers for a 3D Oral Simulation Model. Materials 2025, 18, 2490. [Google Scholar] [CrossRef]
- ELsyad, M.A.; Tella, E.A.E.S.; Mohamed, S.S.; Mahrous, A.I. Within-patient evaluation of chewing efficiency and maximum bite force of conventional dentures, fixed prostheses, and milled bar overdentures used for All-on-4 implant rehabilitation of atrophied mandibular ridges: A short-term randomized trial. Clin. Implant. Dent. Relat. Res. 2022, 24, 522–531. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Lang, A.-G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrence Erlbaum Associates: Hillsdale, NJ, USA, 1998. [Google Scholar]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2025; Available online: https://www.r-project.org/ (accessed on 16 June 2025).
- Johnson, A.; Al-Kaisy, N.; Miller, C.; Martin, N. The Effect of denture design and fixatives on the retention of mandibular complete dentures tested on a novel in-vitro edentulous model. Eur. J. Prosthodont. Rest. Dent. 2013, 216, 4–74. [Google Scholar] [CrossRef]
- Mendes, J.; Mendes, J.M.; Barreiros, P.; Aroso, C.; Silva, A.S. Retention Capacity of Original Denture Adhesives and White Brands for Conventional Complete Dentures: An In Vitro Study. Polymers 2022, 14, 1749. [Google Scholar] [CrossRef]
- Mistry, G.; Charushila Sardar, C.; Pandey, P.; Souza, M.D.; Vibha Kailaje, V.; Sachdev, S.S. 3D printed full-arch versus digital reference dental models: A systematic review. Bioinformation 2024, 20, 1100–1105. [Google Scholar] [CrossRef] [PubMed]
- Petre, A.E.; Pantea, M.; Drafta, S.; Imre, M.; Tâncu, A.M.C.; Liciu, E.M.; Didilescu, A.C. SM Modular Digital and 3D-Printed Dental Models with Applicability in Dental Education. Medicina 2023, 59, 116. [Google Scholar] [CrossRef]
- Abad-Coronel, C.; Pazán, D.P.; Hidalgo, L.; Larriva Loyola, J. Comparative Analysis between 3D-Printed Models Designed with Generic and Dental-Specific Software. Dent. J. 2023, 11, 216. [Google Scholar] [CrossRef]
- Park, J.-M.; Jeon, J.; Koak, J.-Y.; Kim, S.-K.; Heo, S.-J. Dimensional accuracy and surface characteristics of 3D-printed dental casts. J. Prosthet. Dent. 2020, 126, 427–437. [Google Scholar] [CrossRef] [PubMed]
- Bogdanov, T.G.; Hikov, T.A.; Uzunov, T.; Kirov, D.; Milanov, N.; Galeva, H. Evaluation of 3D-Printed Models in Dental Education: Practical Applications and Student Perspectives. Cureus 2025, 17, e81644. [Google Scholar] [CrossRef]
- Alshaibani, R.M.; Fan, Y.; Giordano, R. Effect of different storage conditions on dimensional accuracy of 3D-printed dental models. J. Prosthodont. 2024, 1–9. [Google Scholar] [CrossRef]
- Żmudzki, J.; Chladek, G.; Kasperski, J. Biomechanical factors related to occlusal load transfer in removable complete dentures. Biomech. Model. Mechanobiol. 2015, 146, 79–91. [Google Scholar] [CrossRef]
- Compagnoni, M.A.; Souza, R.F.; Leles, C.R. Kinesiographic study of complete denture movement related to mucosa displacement in edentulous patients. Pesqui. Odontol. Bras. 2003, 173, 56–61. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Dental Position | Means | ||
|---|---|---|---|
| Buccal | Crest | Lingual | |
| Central Incisors | 1.7 | 2.2 | 1.9 |
| Lateral Incisors | 1.8 | 2.3 | 1.7 |
| Cuspid | 1.8 | 2.3 | 1.5 |
| 1° PM | 1.7 | 2.1 | 1.4 |
| 2° PM | 1.7 | 2.3 | 1.3 |
| 1° Molar | 1.8 | 2.4 | 1.3 |
| 2° Molar | 2.0 | 2.6 | 1.6 |
| Attachment | Test 1 | Test 2 | Test 3 | F(2, 4) | p-Value | Partial η2 |
|---|---|---|---|---|---|---|
| Center | 0.0147 (0.0015) | 0.0140 (0.0010) | 0.0133 (0.0012) | F(2, 4) = 16.00 | 0.057 | 0.89 |
| Left | 0.0063 (0.0015) | 0.0060 (0.0010) | 0.0067 (0.0006) | F(2, 4) = 0.25 | 0.667 | 0.11 |
| Right | 0.0050 (0.0010) | 0.0050 (0.0010) | 0.0043 (0.0012) | F(2, 4) = 4.00 | 0.184 | 0.67 |
| N = 9 | M (SD) | Dif = 0 | Dif ≤ 0.005 | Dif ≤ 0.010 | Dif ≤ 0.015 | Dif ≤ 0.020 |
|---|---|---|---|---|---|---|
| Center | 0.0140 (0.0012) | <0.001 | <0.001 | <0.001 | 0.980 | >0.990 |
| Left | 0.0063 (0.001) | <0.001 | 0.002 | >0.990 | >0.990 | >0.990 |
| Right | 0.0048 (0.00098) | <0.00 | 0.256 | >0.990 | >0.990 | >0.990 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mendes, J.; Manzanares-Céspedes, M.C.; Esteves, J.L.; Fonseca, J.; Coelho, L.; Mendes, J.M. Three-Dimensional Manufacturing of Mandibular Total Edentulous Simulation Model for In Vitro Studies—Concept and Validation. Polymers 2025, 17, 1820. https://doi.org/10.3390/polym17131820
Mendes J, Manzanares-Céspedes MC, Esteves JL, Fonseca J, Coelho L, Mendes JM. Three-Dimensional Manufacturing of Mandibular Total Edentulous Simulation Model for In Vitro Studies—Concept and Validation. Polymers. 2025; 17(13):1820. https://doi.org/10.3390/polym17131820
Chicago/Turabian StyleMendes, Joana, Maria Cristina Manzanares-Céspedes, José L. Esteves, João Fonseca, Lara Coelho, and José Manuel Mendes. 2025. "Three-Dimensional Manufacturing of Mandibular Total Edentulous Simulation Model for In Vitro Studies—Concept and Validation" Polymers 17, no. 13: 1820. https://doi.org/10.3390/polym17131820
APA StyleMendes, J., Manzanares-Céspedes, M. C., Esteves, J. L., Fonseca, J., Coelho, L., & Mendes, J. M. (2025). Three-Dimensional Manufacturing of Mandibular Total Edentulous Simulation Model for In Vitro Studies—Concept and Validation. Polymers, 17(13), 1820. https://doi.org/10.3390/polym17131820