
Polymeric Scaffolds Used in Dental Pulp Regeneration by Tissue Engineering Approach

 , , ,
, , ,  and
and
Abstract
1. Introduction
2. The Dental Pulp
3. Dental Pulp Regeneration
4. Endodontic Regeneration
5. Tissue Engineering
5.1. Dental Stem Cells
5.2. Growth Factors
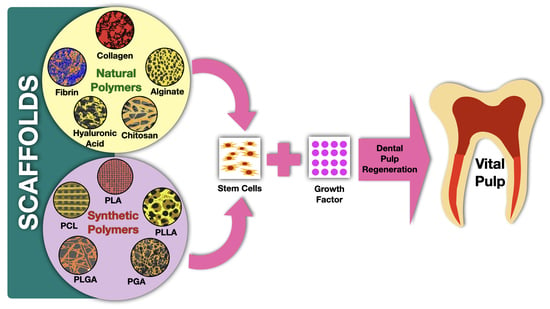
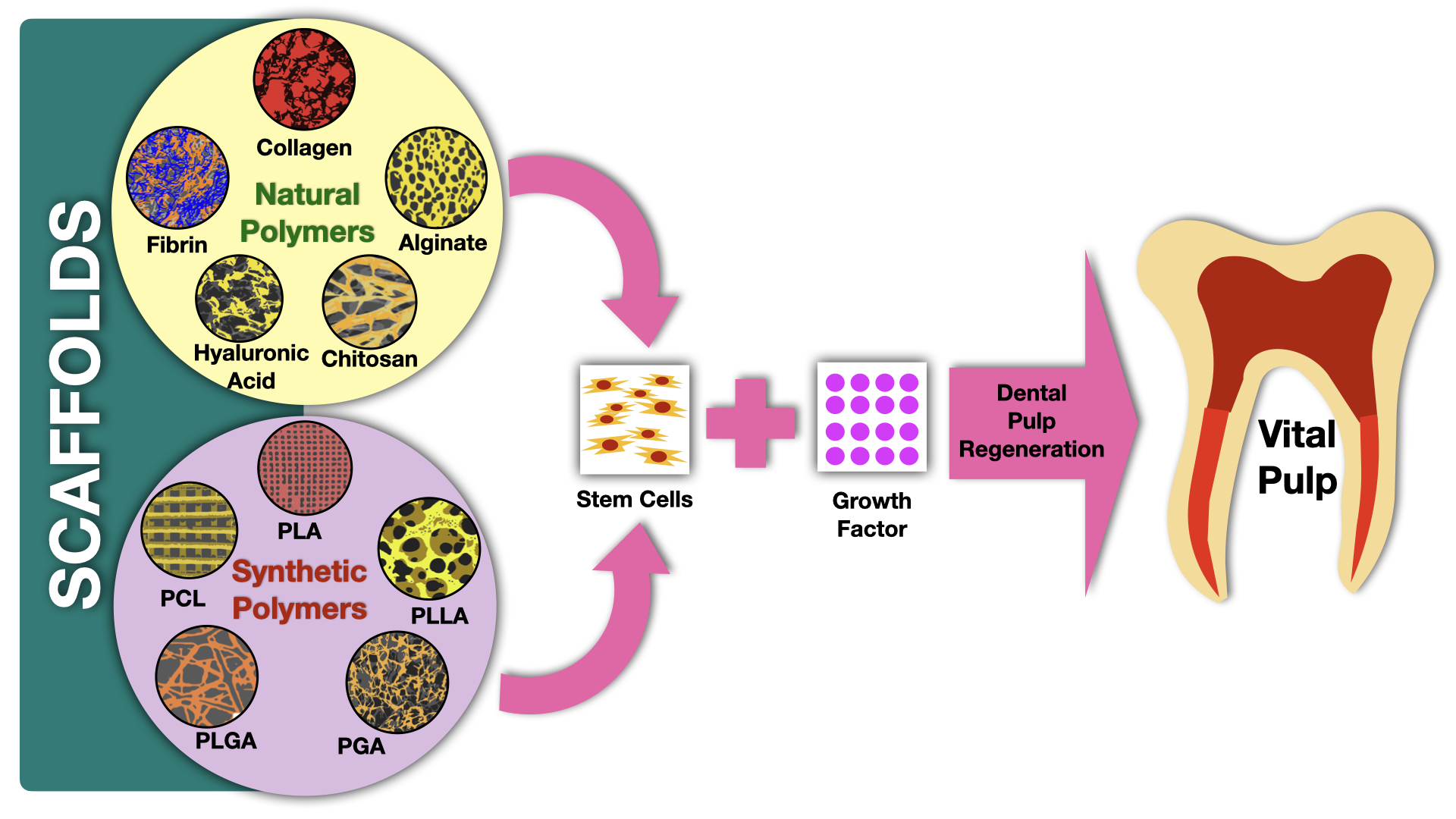
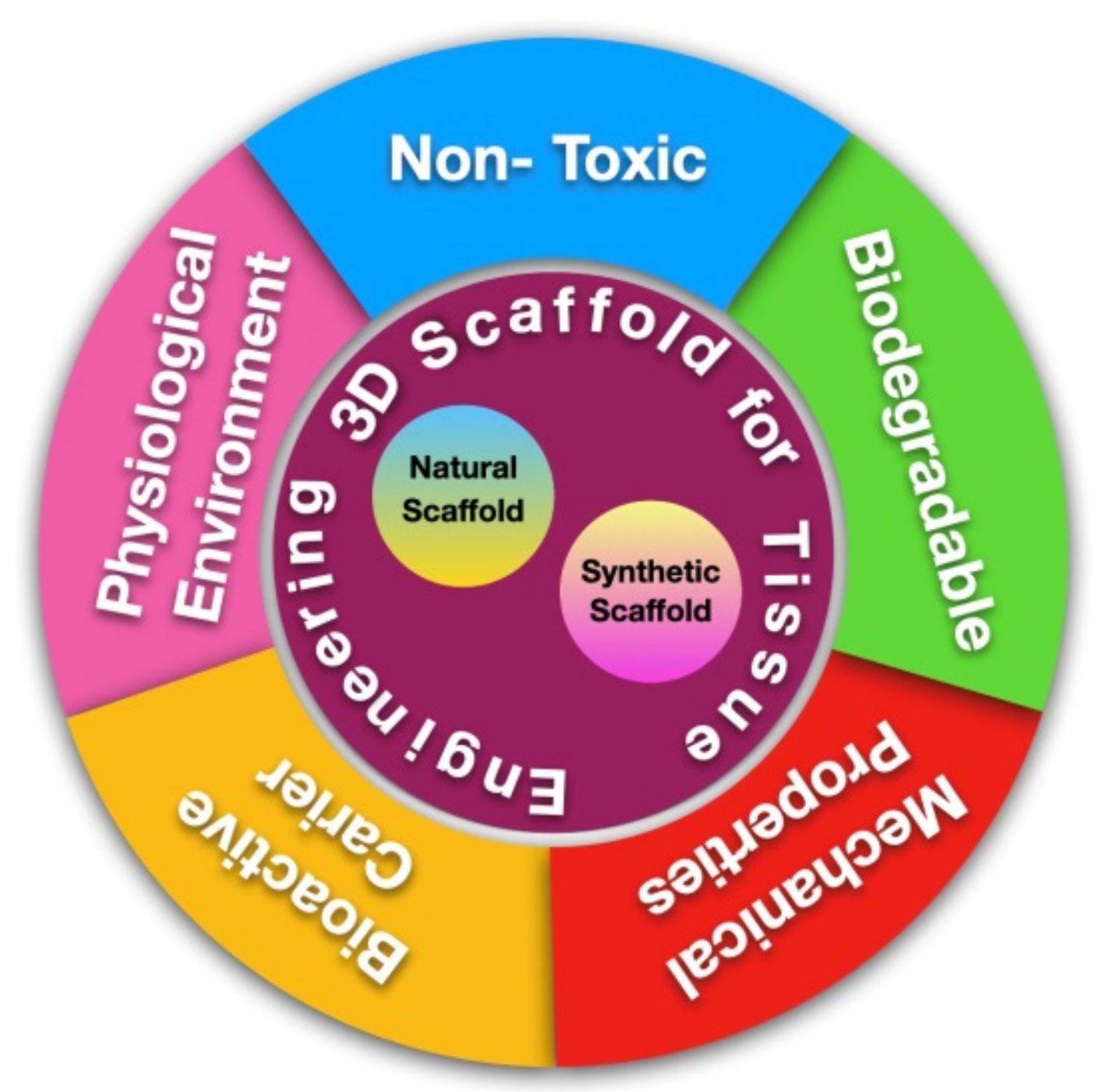
5.3. Scaffolds
5.3.1. Scaffolds Made of Natural Polymers
5.3.2. Scaffolds Made of Synthetic Polymers
6. Conclusions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Farges, J.C.; Alliot-Licht, B.; Renard, E.; Ducret, M.; Gaudin, A.; Smith, A.J.; Cooper, P.R. Dental Pulp Defence and Repair Mechanisms in Dental Caries. Mediat. Inflamm. 2015, 2015, 230251. [Google Scholar] [CrossRef] [PubMed]
- Xie, Z.; Shen, Z.; Zhan, P.; Yang, J.; Huang, Q.; Huang, S.; Chen, L.; Lin, Z. Functional dental pulp regeneration: Basic research and clinical translation. Int. J. Mol. Sci. 2021, 22, 8991. [Google Scholar] [CrossRef] [PubMed]
- Kwack, K.H.; Lee, H.W. Clinical Potential of Dental Pulp Stem Cells in Pulp Regeneration: Current Endodontic Progress and Future Perspectives. Front. Cell Dev. Biol. 2022, 10, 734. [Google Scholar] [CrossRef] [PubMed]
- Srivastava, S. Current and future perspectives for dentin-pulp tissue engineering—An update. S. Afr. Dent. J. 2019, 74, 110–114. [Google Scholar] [CrossRef]
- Sugiaman, V.K.; Djuanda, R.; Pranata, N.; Naliani, S.; Demolsky, W.L.; Jeffrey. Tissue Engineering with Stem Cell from Human Exfoliated Deciduous Teeth (SHED) and Collagen Matrix, Regulated by Growth Factor in Regenerating the Dental Pulp. Polymers 2022, 14, 3712. [Google Scholar] [CrossRef]
- Retana-Lobo, C. Dental Pulp Regeneration: Insights from Biological Processes. Odovtos-Int. J. Dent. Sci. 2017, 20, 10–16. [Google Scholar] [CrossRef]
- Zakrzewski, W.; Dobrzyński, M.; Szymonowicz, M.; Rybak, Z. Fuel Cells: Past, Present and Future. IEEJ Trans. Fundam. Mater. 2019, 128, 329–332. [Google Scholar] [CrossRef]
- Ayavoo, T.; Murugesan, K.; Gnanasekaran, A. Roles and mechanisms of stem cell in wound healing. Stem Cell Investig. 2021, 8, 1–9. [Google Scholar] [CrossRef]
- Kulebyakin, K.Y.; Nimiritsky, P.P.; Makarevich, P.I. Growth Factors in Regeneration and Regenerative Medicine: “The Cure and the Cause”. Front. Endocrinol. 2020, 11, 384. [Google Scholar] [CrossRef]
- Li, Z.; Liu, L.; Wang, L.; Song, D. The effects and potential applications of concentrated growth factor in dentin–pulp complex regeneration. Stem Cell Res. Ther. 2021, 12, 357. [Google Scholar] [CrossRef]
- Krupiñska, A.M.; Skoœkiewicz-Malinowska, K.; Staniowski, T. Different approaches to the regeneration of dental tissues in regenerative endodontics. Appl. Sci. 2021, 11, 1699. [Google Scholar] [CrossRef]
- Park, Y.; Huh, K.M.; Kang, S.W. Applications of biomaterials in 3d cell culture and contributions of 3D cell culture to drug development and basic biomedical research. Int. J. Mol. Sci. 2021, 22, 2491. [Google Scholar] [CrossRef] [PubMed]
- Jazayeri, H.E.; Lee, S.M.; Kuhn, L.; Fahimipour, F.; Tahriri, M.; Tayebi, L. Polymeric scaffolds for dental pulp tissue engineering: A review. Dent. Mater. 2020, 36, e47–e58. [Google Scholar] [CrossRef] [PubMed]
- Dhivya, S.; Keshav Narayan, A.; Logith Kumar, R.; Viji Chandran, S.; Vairamani, M.; Selvamurugan, N. Proliferation and differentiation of mesenchymal stem cells on scaffolds containing chitosan, calcium polyphosphate and pigeonite for bone tissue engineering. Cell Prolif. 2018, 51, e12408. [Google Scholar] [CrossRef]
- Sharma, S.; Srivastava, D.; Grover, S.; Sharma, V. Biomaterials in tooth tissue engineering: A review. J. Clin. Diagn. Res. 2014, 8, 309–315. [Google Scholar] [CrossRef]
- Ricucci, D.; Loghin, S.; Lin, L.M.; Spångberg, L.S.W.; Tay, F.R. Is hard tissue formation in the dental pulp after the death of the primary odontoblasts a regenerative or a reparative process? J. Dent. 2014, 42, 1156–1170. [Google Scholar] [CrossRef]
- Yang, J.; Yuan, G.; Chen, Z. Pulp regeneration: Current approaches and future challenges. Front. Physiol. 2016, 7, 58. [Google Scholar] [CrossRef]
- Huang, C.; Narayanan, R.; Warshawsky, N. Dual ECM Biomimetic Scaffolds for Dental Pulp Regenerative Applications. Front. Physiol. 2018, 9, 495. [Google Scholar] [CrossRef]
- Gaje, P.N.; Ceausu, R.A. Cell types of the dental pulp behind the odontoblast. Res. Clin. Med. 2020, 4, 16–18. [Google Scholar]
- Erdek, Ö.; Bloch, W.; Rink-Notzon, S.; Roggendorf, H.C.; Uzun, S.; Meul, B.; Koch, M.; Neugebauer, J.; Deschner, J.; Korkmaz, Y. Inflammation of the Human Dental Pulp Induces Phosphorylation of eNOS at Thr495 in Blood Vessels. Biomedicines 2022, 10, 1586. [Google Scholar] [CrossRef]
- Huang, X.; Li, Z.; Liu, A.; Liu, X.; Guo, H.; Wu, M.; Yang, X.; Han, B.; Xuan, K. Microenvironment Influences Odontogenic Mesenchymal Stem Cells Mediated Dental Pulp Regeneration. Front. Physiol. 2021, 12, 656588. [Google Scholar] [CrossRef]
- Fawzy El-Sayed, K.M.; Jakusz, K.; Jochens, A.; Dörfer, C.; Schwendicke, F. Stem cell transplantation for pulpal regeneration: A systematic review. Tissue Eng.-Part B Rev. 2015, 21, 451–460. [Google Scholar] [CrossRef]
- Kökten, T.; Bécavin, T.; Keller, L.; Weickert, J.L.; Kuchler-Bopp, S.; Lesot, H. Immunomodulation stimulates the innervation of engineered tooth organ. PLoS ONE 2014, 9, e86011. [Google Scholar] [CrossRef]
- Goldberg, M.; Njeh, A.; Uzunoglu, E. Is Pulp Inflammation a Prerequisite for Pulp Healing and Regeneration? Mediat. Inflamm. 2015, 2015, 347649. [Google Scholar] [CrossRef]
- Stamnitz, S.; Klimczak, A. Bone Repair: From Research Perspectives to Clinical Practice. Cells 2021, 10, 1925. [Google Scholar] [CrossRef]
- Kim, I.H.; Jeon, M.; Cheon, K.; Kim, S.H.; Jung, H.S.; Shin, Y.; Kang, C.M.; Kim, S.O.; Choi, H.J.; Lee, H.S.; et al. In vivo evaluation of decellularized human tooth scaffold for dental tissue regeneration. Appl. Sci. 2021, 11, 8472. [Google Scholar] [CrossRef]
- Wei, X.; Yang, M.; Yue, L.; Huang, D.; Zhou, X.; Wang, X.; Zhang, Q.; Qiu, L.; Huang, Z.; Wang, H.; et al. Expert consensus on regenerative endodontic procedures. Int. J. Oral Sci. 2022, 14, 55. [Google Scholar] [CrossRef]
- Colombo, J.S.; Moore, A.N.; Hartgerink, J.D.; D’Souza, R.N. Scaffolds to control inflammation and facilitate dental pulp regeneration. J. Endod. 2014, 40, S6–S12. [Google Scholar] [CrossRef] [PubMed]
- Osman, Z.F.; Ahmad, A.; Noordin, K.B.A.A. Naturally derived scaffolds for dental pulp regeneration: A review. Gulhane Med. J. 2019, 61, 81–88. [Google Scholar] [CrossRef]
- Smojver, I.; Katalinić, I.; Bjelica, R.; Gabrić, D.; Matišić, V.; Molnar, V.; Primorac, D. Mesenchymal Stem Cells Based Treatment in Dental Medicine: A Narrative Review. Int. J. Mol. Sci. 2022, 23, 1662. [Google Scholar] [CrossRef] [PubMed]
- Olaru, M.; Sachelarie, L.; Calin, G. Hard dental tissues regeneration—Approaches and challenges. Materials 2021, 14, 2558. [Google Scholar] [CrossRef]
- Sándor, G. Tissue engineering: Propagating the wave of change. Ann. Maxillofac. Surg. 2013, 3, 1–2. [Google Scholar] [CrossRef] [PubMed]
- Samiei, M.; Fathi, M.; Barar, J.; Fathi, N.; Amiryaghoubi, N.; Omidi, Y. Bioactive hydrogel-based scaffolds for the regeneration of dental pulp tissue. J. Drug Deliv. Sci. Technol. 2021, 64, 102600. [Google Scholar] [CrossRef]
- Dissanayaka, W.L.; Zhang, C. The Role of Vasculature Engineering in Dental Pulp Regeneration. J. Endod. 2017, 43, S102–S106. [Google Scholar] [CrossRef] [PubMed]
- Sun, H.H.; Chen, B.; Zhu, Q.L.; Kong, H.; Li, Q.H.; Gao, L.N.; Xiao, M.; Chen, F.M.; Yu, Q. Investigation of dental pulp stem cells isolated from discarded human teeth extracted due to aggressive periodontitis. Biomaterials 2014, 35, 9459–9472. [Google Scholar] [CrossRef]
- Yang, J.W.; Zhang, Y.F.; Sun, Z.Y.; Song, G.T.; Chen, Z. Dental pulp tissue engineering with bFGF-incorporated silk fibroin scaffolds. J. Biomater. Appl. 2015, 30, 221–229. [Google Scholar] [CrossRef]
- Yang, J.W.; Zhang, Y.F.; Wan, C.Y.; Sun, Z.Y.; Nie, S.; Jian, S.J.; Zhang, L.; Song, G.T.; Chen, Z. Autophagy in SDF-1α-mediated DPSC migration and pulp regeneration. Biomaterials 2015, 44, 11–23. [Google Scholar] [CrossRef]
- Caracappa, J.D.; Vincent, S. The future in dental medicine: Dental stem cells are a promising source for tooth and tissue engineering. J. Stem Cell Res. Ther. Rev. 2019, 5, 30–36. [Google Scholar] [CrossRef]
- Staniowski, T.; Zawadzka-Knefel, A.; Skośkiewicz-Malinowska, K. Therapeutic potential of dental pulp stem cells according to different transplant types. Molecules 2021, 26, 7423. [Google Scholar] [CrossRef]
- Morotomi, T.; Washio, A.; Kitamura, C. Current and future options for dental pulp therapy. Jpn. Dent. Sci. Rev. 2019, 55, 5–11. [Google Scholar] [CrossRef]
- Dang, M.; Saunders, L.; Niu, X.; Fan, Y.; Ma, P.X. Biomimetic delivery of signals for bone tissue engineering. Bone Res. 2018, 6, 25. [Google Scholar] [CrossRef] [PubMed]
- Moussa, D.G.; Aparicio, C. Present and future of tissue engineering scaffolds for dentin-pulp complex regeneration. J. Tissue Eng. Regen. Med. 2019, 13, 58–75. [Google Scholar] [CrossRef] [PubMed]
- Suamte, L.; Tirkey, A.; Babu, P.J. Design of 3D smart scaffolds using natural, synthetic and hybrid derived polymers for skin regenerative applications. Smart Mater. Med. 2023, 4, 243–256. [Google Scholar] [CrossRef]
- Tran, T.T.; Hamid, Z.A.; Cheong, K.Y. A Review of Mechanical Properties of Scaffold in Tissue Engineering: Aloe Vera Composites. J. Phys. Conf. Ser. 2018, 1082, 012080. [Google Scholar] [CrossRef]
- Wu, D.T.; Munguia-Lopez, J.G.; Cho, Y.W.; Ma, X.; Song, V.; Zhu, Z.; Tran, S.D. Polymeric scaffolds for dental, oral, and craniofacial regenerative medicine. Molecules 2021, 26, 7043. [Google Scholar] [CrossRef] [PubMed]
- Echeverria Molina, M.I.; Malollari, K.G.; Komvopoulos, K. Design Challenges in Polymeric Scaffolds for Tissue Engineering. Front. Bioeng. Biotechnol. 2021, 9, 617141. [Google Scholar] [CrossRef] [PubMed]
- Putra, R.U.; Basri, H.; Prakoso, A.T.; Chandra, H.; Ammarullah, M.I.; Akbar, I.; Syahrom, A.; Kamarul, T. Level of Activity Changes Increases the Fatigue Life of the Porous Magnesium Scaffold, as Observed in Dynamic Immersion Tests, over Time. Sustainability 2023, 15, 823. [Google Scholar] [CrossRef]
- Zhang, H.; Zhou, L.; Zhang, W. Control of scaffold degradation in tissue engineering: A review. Tissue Eng.-Part B Rev. 2014, 20, 492–502. [Google Scholar] [CrossRef]
- Van Bochove, B.; Grijpma, D.W. Photo-crosslinked synthetic biodegradable polymer networks for biomedical applications. J. Biomater. Sci. Polym. Ed. 2019, 30, 77–106. [Google Scholar] [CrossRef]
- Jang, J.H.; Moon, J.H.; Kim, S.G.; Kim, S.Y. Pulp regeneration with hemostatic matrices as a scaffold in an immature tooth minipig model. Sci. Rep. 2020, 10, 12536. [Google Scholar] [CrossRef]
- Erisken, C.; Kalyon, D.M.; Zhou, J.; Kim, S.G.; Mao, J.J. Viscoelastic properties of dental pulp tissue and ramifications on biomaterial development for pulp regeneration. J. Endod. 2015, 41, 1711–1717. [Google Scholar] [CrossRef] [PubMed]
- Raddall, G.; Mello, I.; Leung, B.M. Biomaterials and Scaffold Design Strategies for Regenerative Endodontic Therapy. Front. Bioeng. Biotechnol. 2019, 7, 317. [Google Scholar] [CrossRef]
- Yu, H.; Zhang, X.; Song, W.; Pan, T.; Wang, H.; Ning, T.; Wei, Q.; Xu, H.H.K.; Wu, B.; Ma, D. Effects of 3-dimensional Bioprinting Alginate/Gelatin Hydrogel Scaffold Extract on Proliferation and Differentiation of Human Dental Pulp Stem Cells. J. Endod. 2019, 45, 706–715. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Lu, J.; Jiang, Q.; Haapasalo, M.; Qian, J.; Tay, F.R.; Shen, Y. Biomaterial scaffolds for clinical procedures in endodontic regeneration: Biomaterial scaffolds in endodontic regeneration. Bioact. Mater. 2022, 12, 257–277. [Google Scholar] [CrossRef]
- Palma, P.J.; Ramos, J.C.; Martins, J.B.; Diogenes, A.; Figueiredo, M.H.; Ferreira, P.; Viegas, C.; Santos, J.M. Histologic Evaluation of Regenerative Endodontic Procedures with the Use of Chitosan Scaffolds in Immature Dog Teeth with Apical Periodontitis. J. Endod. 2017, 43, 1279–1287. [Google Scholar] [CrossRef]
- Nowicka, A.; Miller-Burchacka, M.; Lichota, D.; Metlerska, J.; Gońda-Domin, M. Tissue engineering application in regenerative endodontics. Pomeranian J. Life Sci. 2021, 67, 10–17. [Google Scholar] [CrossRef]
- Nosrat, A.; Kolahdouzan, A.; Khatibi, A.H.; Verma, P.; Jamshidi, D.; Nevins, A.J.; Torabinejad, M. Clinical, Radiographic, and Histologic Outcome of Regenerative Endodontic Treatment in Human Teeth Using a Novel Collagen-hydroxyapatite Scaffold. J. Endod. 2019, 45, 136–143. [Google Scholar] [CrossRef]
- De Araújo, L.; Goulart, T.S.; Gil, A.C.K.; Schuldt, D.P.V.; Coelho, B.S.; Figueiredo, D.D.R.; Garcia, L.D.F.R.; De Almeida, J. Do alternative scaffolds used in regenerative endodontics promote better root development than that achieved with blood clots? Braz. Dent. J. 2022, 33, 22–32. [Google Scholar] [CrossRef] [PubMed]
- Jung, C.; Kim, S.; Sun, T.; Cho, Y.B.; Song, M. Pulp-dentin regeneration: Current approaches and challenges. J. Tissue Eng. 2019, 10. [Google Scholar] [CrossRef] [PubMed]
- Ayala-Ham, A.; López-Gutierrez, J.; Bermúdez, M.; Aguilar-Medina, M.; Sarmiento-Sánchez, J.I.; López-Camarillo, C.; Sanchez-Schmitz, G.; Ramos-Payan, R. Hydrogel-Based Scaffolds in Oral Tissue Engineering. Front. Mater. 2021, 8, 708945. [Google Scholar] [CrossRef]
- Ducret, M.; Costantini, A.; Gobert, S.; Farges, J.C.; Bekhouche, M. Fibrin-based scaffolds for dental pulp regeneration: From biology to nanotherapeutics. Eur. Cells Mater. 2021, 41, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Moreira, M.S.; Sarra, G.; Carvalho, G.L.; Gonçalves, F.; Caballero-Flores, H.V.; Pedroni, A.C.F.; Lascala, C.A.; Catalani, L.H.; Marques, M.M. Physical and Biological Properties of a Chitosan Hydrogel Scaffold Associated to Photobiomodulation Therapy for Dental Pulp Regeneration: An in Vitro and in Vivo Study. Biomed Res. Int. 2021, 2021, 6684667. [Google Scholar] [CrossRef] [PubMed]
- Sharma, S.; Mittal, N. A comparative evaluation of natural and artificial scaffolds in regenerative endodontics: A clinical study. Saudi Endod. J. 2016, 6, 9–15. [Google Scholar] [CrossRef]
- Rojo, L.; Vazquez, B.; Roman, J.S. Synthetic Polymers for Tissue Engineering Scaffolds: Biological Design, Materials, and Fabrication Biomaterials for Scaffolds: Synthetic Polymers. In Scaffolds for Tissue Engineering; CRC Press: Boca Raton, FL, USA, 2014; pp. 263–300. [Google Scholar]
- Nikolova, M.P.; Chavali, M.S. Recent advances in biomaterials for 3D scaffolds: A review. Bioact. Mater. 2019, 4, 271–292. [Google Scholar] [CrossRef] [PubMed]
- Dissanayaka, W.L.; Zhang, C. Scaffold-based and Scaffold-free Strategies in Dental Pulp Regeneration. J. Endod. 2020, 46, S81–S89. [Google Scholar] [CrossRef] [PubMed]
- Joshi, S.R.; Pendyala, G.S.; Shah, P.; Mopagar, V.P.; Padmawar, N.; Padubidri, M. Scaffolds-The Ground for Regeneration: A Narrative Review. J. Int. Soc. Prev. Community Dent. 2020, 10, 692–699. [Google Scholar] [CrossRef]
- Azaman, F.A.; Zhou, K.; Del Blanes-Martínez, M.M.; Brennan Fournet, M.; Devine, D.M. Bioresorbable Chitosan-Based Bone Regeneration Scaffold Using Various Bioceramics and the Alteration of Photoinitiator Concentration in an Extended UV Photocrosslinking Reaction. Gels 2022, 8, 696. [Google Scholar] [CrossRef]
- Liu, X.; Holzwarth, J.M.; Ma, P.X. Functionalized Synthetic Biodegradable Polymer Scaffolds for Tissue Engineering. Macromol. Biosci. 2012, 12, 911–919. [Google Scholar] [CrossRef]
- Dos Santos Gomes, D.; De Sousa Victor, R.; De Sousa, B.V.; De Araújo Neves, G.; De Lima Santana, L.N.; Menezes, R.R. Ceramic Nanofiber Materials for Wound Healing and Bone Regeneration: A Brief Review. Materials 2022, 15, 3909. [Google Scholar] [CrossRef]
- Nuge, T.; Liu, Z.; Liu, X.; Ang, B.C.; Andriyana, A.; Metselaar, H.S.C.; Hoque, M.E. Recent advances in scaffolding from natural-based polymers for volumetric muscle injury. Molecules 2021, 26, 699. [Google Scholar] [CrossRef]
- Kim, S.G.; Zhou, J.; Ye, L.; Cho, S.; Suzuki, T.; Fu, S.Y.; Yang, R.; Zhou, X.; Mao, J.J. Regenerative Endodontics: Barriers and Strategies for Clinical Translation. Dent. Clin. N. Am. 2014, 56, 639–649. [Google Scholar] [CrossRef]
- Amini, S.; Salehi, H.; Setayeshmehr, M.; Ghorbani, M. Natural and synthetic polymeric scaffolds used in peripheral nerve tissue engineering: Advantages and disadvantages. Polym. Adv. Technol. 2021, 32, 2267–2289. [Google Scholar] [CrossRef]
- Reddy, M.S.B.; Ponnamma, D.; Choudhary, R.; Sadasivuni, K.K. A comparative review of natural and synthetic biopolymer composite scaffolds. Polymers 2021, 13, 1105. [Google Scholar] [CrossRef] [PubMed]
- Gathani, K.M.; Raghavendra, S.S. Scaffolds in regenerative endodontics: A review. Dent. Res. J. 2016, 13, 379–386. [Google Scholar] [CrossRef]
- Banerjee, A.; Chatterjee, K.; Madras, G. Enzymatic degradation of polymers: A brief review. Mater. Sci. Technol. 2014, 30, 567–573. [Google Scholar] [CrossRef]
- Gentile, P.; Chiono, V.; Carmagnola, I.; Hatton, P.V. An overview of poly(lactic-co-glycolic) Acid (PLGA)-based biomaterials for bone tissue engineering. Int. J. Mol. Sci. 2014, 15, 3640–3659. [Google Scholar] [CrossRef]
- Prakasam, M.; Silvain, J.F.; Largeteau, A. Innovative high-pressure fabrication processes for porous biomaterials—A review. Bioengineering 2021, 8, 170. [Google Scholar] [CrossRef]
- Rizk, A.; Rabie, A.B.M. Human dental pulp stem cells expressing transforming growth factor β3 transgene for cartilage-like tissue engineering. Cytotherapy 2013, 15, 712–725. [Google Scholar] [CrossRef]
- Danhier, F.; Ansorena, E.; Silva, J.M.; Coco, R.; Le Breton, A.; Préat, V. PLGA-based nanoparticles: An overview of biomedical applications. J. Control. Release 2012, 161, 505–522. [Google Scholar] [CrossRef]
- Jammalamadaka, U.; Tappa, K. Recent advances in biomaterials for 3D printing and tissue engineering. J. Funct. Biomater. 2018, 9, 22. [Google Scholar] [CrossRef]
- Bencherif, S.A.; Braschler, T.M.; Renaud, P. Advances in the design of macroporous polymer scaffolds for potential applications in dentistry. J. Periodontal Implant Sci. 2013, 43, 251–261. [Google Scholar] [CrossRef] [PubMed]
- Zhang, B.; Bian, X.; Xiang, S.; Li, G.; Chen, X. Synthesis of PLLA-based block copolymers for improving melt strength and toughness of PLLA by in situ reactive blending. Polym. Degrad. Stab. 2017, 136, 58–70. [Google Scholar] [CrossRef]
- Śmigiel-Gac, N.; Pamuła, E.; Krok-Borkowicz, M.; Smola-Dmochowska, A.; Dobrzyński, P. Synthesis and properties of bioresorbable block copolymers of l-lactide, glycolide, butyl succinate and butyl citrate. Polymers 2020, 12, 213. [Google Scholar] [CrossRef] [PubMed]
- Haugen, H.J.; Basu, P.; Sukul, M.; Mano, J.F.; Reseland, J.E. Injectable biomaterials for dental tissue regeneration. Int. J. Mol. Sci. 2020, 21, 3442. [Google Scholar] [CrossRef]
- Kaliva, M.; Georgopoulou, A.; Dragatogiannis, D.A.; Charitidis, C.A.; Chatzinikolaidou, M.; Vamvakaki, M. Biodegradable Chitosan-graft-Poly(l-lactide) Copolymers For Bone Tissue Engineering. Polymers 2020, 12, 316. [Google Scholar] [CrossRef]
- Chocholata, P.; Kulda, V.; Babuska, V. Fabrication of scaffolds for bone-tissue regeneration. Materials 2019, 12, 568. [Google Scholar] [CrossRef]
- Wei, S.; Ma, J.X.; Xu, L.; Gu, X.S.; Ma, X.L. Biodegradable materials for bone defect repair. Mil. Med. Res. 2020, 7, 54. [Google Scholar] [CrossRef]
- Svobodová, J.; Proks, V.; Karabiyik, Ö.; Çalıkoğlu Koyuncu, A.C.; Torun Köse, G.; Rypáček, F.; Studenovská, H. Poly (Amino Acid)-Base fibrous scaffold modified with surface-pendant eptides for cartilage tissue engineering. J. Tissue Eng. Regen. Med. 2017, 11, 831–842. [Google Scholar] [CrossRef]
- Li, T.; Lu, X.M.; Zhang, M.R.; Hu, K.; Li, Z. Peptide-based nanomaterials: Self-assembly, properties and applications. Bioact. Mater. 2022, 11, 268–282. [Google Scholar] [CrossRef]
- Galler, K.M.; Hartgerink, J.D.; Cavender, A.C.; Schmalz, G.; D’Souza, R.N. A customized self-assembling peptide hydrogel for dental pulp tissue engineering. Tissue Eng.-Part A 2012, 18, 176–184. [Google Scholar] [CrossRef]
- Khanna-Jain, R.; Mannerström, B.; Vuorinen, A.; Sándor, G.K.B.; Suuronen, R.; Miettinen, S. Osteogenic differentiation of human dental pulp stem cells on β-tricalcium phosphate/poly (l-lactic acid/caprolactone) three-dimensional scaffolds. J. Tissue Eng. 2012, 3, 2041731412467998. [Google Scholar] [CrossRef] [PubMed]
- Alaribe, F.N.; Manoto, S.L.; Motaung, S.C.K.M. Scaffolds from biomaterials: Advantages and limitations in bone and tissue engineering. Biologia 2016, 71, 353–366. [Google Scholar] [CrossRef]
- Farzamfar, S.; Esmailpour, F.; Rahmati, M.; Vaez, A.; Mirzaii, M.; Garmabi, B.; Shayannia, A.; Ebrahimi, E.; Vahedi, H.; Salehi, M. Poly-lactic Acid/Gelatin Nanofiber (PLA/GTNF) Conduits Containing Platelet-Rich Plasma for Peripheral Nerve Regeneration. Int. J. Health Stud. 2017, 3, 29–32. [Google Scholar] [CrossRef]
- Gaaz, T.S.; Sulong, A.B.; Akhtar, M.N.; Kadhum, A.A.H.; Mohamad, A.B.; Al-amiery, A.A. Properties and Applications of Polyvinyl Alcohol, Halloysite Nanotubes and Their Nanocomposites. Molecules 2015, 20, 22833–22847. [Google Scholar] [CrossRef] [PubMed]
- Zhai, H.; Wu, Y. Research and progress of cartilage tissue-engineering scaffold materials. Discuss. Clin. Cases 2015, 2, 51–54. [Google Scholar] [CrossRef]
- Barroca, N.; Marote, A.; Vieira, S.I.; Almeida, A.; Fernandes, M.H.; Vilarinho, P.M.; Silva, O.A.D.C.E. Electrically polarized PLLA nanofibers as neural tissue engineering scaffolds with improved neuritogenesis. Colloids Surf. B Biointerfaces 2018, 167, 93–103. [Google Scholar] [CrossRef]
- Saini, P.; Arora, M.; Kumar, M.N.V.R. Poly(lactic acid) Blends in Biomedical Applications. Adv. Drug Deliv. Rev. 2016, 107, 47–59. [Google Scholar] [CrossRef]
- Sisson, A.L.; Ekinci, D.; Lendlein, A. The contemporary role of ε-caprolactone chemistry to create advanced polymer architectures. Polymer 2015, 54, 4333–4350. [Google Scholar] [CrossRef]
- Mir, M.; Ahmed, N.; Rehman, A. Recent Applications of Plga Based Nanostructures in Drug Delivery. Colloids Surf. B Biointerfaces 2017, 159, 217–231. [Google Scholar] [CrossRef]
- Prakoso, A.T.; Basri, H.; Adanta, D.; Yani, I.; Ammarullah, M.I.; Akbar, I.; Ghazali, F.A.; Syahrom, A.; Kamarul, T. The Effect of Tortuosity on Permeability of Porous Scaffold. Biomedicines 2023, 11, 427. [Google Scholar] [CrossRef]
- Guerreiro, R.; Pires, T.; Guedes, J.M.; Fernandes, P.R.; Castro, A.P.G. On the Tortuosity of TPMS Scaffolds for Tissue Engineering. Symmetry 2020, 12, 596. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Article (Author, Year) | Type Scaffold | Properties | Advantages | Disadvantages |
|---|---|---|---|---|
| Alaribe, 2016; Jang, 2020; Ducret, 2021 [50,61,93] | Fibrin | Biodegradation, protein natural blood clot, hydrogel base, stimulates the formation of odontoblast | High adhesion to surface, good cytocompatibility and biodegradability, nontoxic, easy to inject | Produced by the body after an injury |
| Alaribe, 2016; Palma, 2017; Moreira, 2021; Raddal, 2019 [52,55,62,93] | Chitosan | Easier to process, hydrogels, films, fibers or sponges, gel-forming abilities; chitosan hydrogels: low viscosity, high adsorption capability. Chitosan, which is the cationic polymer of chitin, has the attractive properties of biodegradability. | It has been used extensively, can support the differentiation of stem cells, noncytotoxicity, biocompatible, biodegradable, antitumor, antifungal, antibacterial activity, nonimmunogenicity, Easily processes, enhances proliferation and cell attachment, hemostatic, noncarcinogenic | Hard use; high crystalline structure: limited application |
| Amini, 2021; Erisken, 2015; Nosrat, 2019; Ayala-Ham, 2021; Raddal, 2019; Liu, 2022 [51,52,54,57,60,73] | Collagen | It lacks structural stability, good mechanical properties, and a material that is comparable to soft dental pulp’s viscoelastic properties, more recommended in combination with a blood clot, hydrogel-based: mimics interactions between cells and ECM in vivo, type 1 collagen is most used. | Low antigenicity, high biocompatibility; biodegradability, bioactivity, and good cell adhesion, high mechanical strength, the ability to cross-link | Problems with controlling space and the rate of degradation, as well as difficulties with sterilization and processing, pathogen transmission low mechanical properties, irregular biodegradation, risks immunogenicity |
| Amini, 2021; Wu, 2021; Raddal, 2019; Yu, 2019; Nowicka, 2021 [45,52,53,56,73] | Alginate | Requires a multistep purification procedure to achieve extremely high purity, natural polymer from algae; alginate hydrogels: crosslinking polysaccharides and divalent cations, the mechanical properties can be adjusted (alginate hydrogels) | High biocompatibility and biodegradability, low toxicity, chelating properties, and non-antigenicity, cheap price, low toxicity optimal structure for exchange nutrition | Endotoxins, heavy metals, polyphenolic and protein compounds, as well as compounds derived from marine sources, are among the naturally occurring impurities; poor mechanical properties. It must be combined with other polymers. |
| Amini, 2021; Ayala, 2021; Raddal, 2019; Wu, 2021; Nowicka, 2021 [45,52,56,60,73] | Hyaluronic Acid | Nanofibrous scaffolds, water insolubility, modified biopolymer; in dental pulp, the amount decreases according to the process of odontogenesis, contains d-glucuronic acid and N-acetyl-D-glucosamine, available in liquid injection form. | Excellent biocompatibility, high water content, suitable viscoelastic properties for many tissue types, capacity to degrade into safe products, and the capability to join to the specific cell surface receptors, reparative dentin stimulation, 3D sponge shape suitable for blood vessel proliferation and stem cell differentiation | It is impossible for the cells to adhere to the surface, low mechanical properties, hypersensitivity reactions, and minor biodegradability |
| Amini, 2021; Farzamfar, 2017; Gathani KM, 2016; Dissanayaka WL, 2020 [66,73,75,94] | Poly (lactic acid) (PLA) | Good mechanical strength | Biocompatibility, processability, biodegradability; planting human exfoliated deciduous teeth stem cells (SHED) on dentin disks with PLA resulted in the structure of odontoblast-like cells, new dentin, and vascularized pulp-like tissue | Low impact toughness, hydrophobicity, and a slow rate of degradation |
| Amini, 2021; Gaaz, 2015; Gathani KM, 2016; Dissanayaka WL, 2020; Liu X, 2012 [66,69,73,75,95] | Poly (l-lactic acid) (PLLA) | Excellent porosity, a high surface-to-volume ratio, nanofibers, and a variety of pore-size distributions | Biodegradable, promotes cell attachment and differentiation, PLLA scaffolds encouraged the development of endothelial cells from dental pulp cells and odontoblasts | During degradation, hydrophilicity, biocompatibility, and mechanical properties are all poor |
| Zhai, 2015; Gathani KM, 2016; Dissanayaka WL, 2020; Liu X, 2012 [66,69,75,96] | Poly (glycolic acid) (PGA) | Highly crystalline and hydrophilic linear polyester, better solubility in water, degradation half-life is about 2 weeks | Help attachment cell | Degradation rate is too high |
| Barroca, 2018; Amini, 2021; Saini, 2016; Santoro M, 2016; Dissanayaka WL, 2020; Rizk A, 2013; Danhier F, 2012 [66,73,79,80,97,98] | Polyethylene glycol (PEG), Copolymer poly [(lactic acid)-co-(glycolic acid)] (PLGA), | Crystallinity, glass transition temperature, good mechanical Strength | Biodegradable, biocompatible, low toxicity/swelling; these artificial polymer scaffolds have also been utilized to convey a range of substances, including anti-inflammatory drugs, growth hormones, and sticky proteins, and support cell growth and proliferation, reduce pulpitis and aid in pulpal healing | The degradation pattern of PLGA is highly dependent on the sequence of monomers that make up its structure, which liberates acidic products |
| Mir M, 2017; Amini, 2021; Sisson, 2013; Gathani KM, 2016 [73,75,99,100] | Poly-epsilon caprolactone (PCL) | Good mechanical properties, high elasticity, high strength | Biocompatible, biodegradable, low toxicity, slowly disintegrating polymer, has been utilized in bone tissue engineering projects either by itself or in conjunction with hydroxyapatite | Hydrophobicity, slow degradation, lack of functional groups |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sugiaman, V.K.; Jeffrey; Naliani, S.; Pranata, N.; Djuanda, R.; Saputri, R.I. Polymeric Scaffolds Used in Dental Pulp Regeneration by Tissue Engineering Approach. Polymers 2023, 15, 1082. https://doi.org/10.3390/polym15051082
Sugiaman VK, Jeffrey, Naliani S, Pranata N, Djuanda R, Saputri RI. Polymeric Scaffolds Used in Dental Pulp Regeneration by Tissue Engineering Approach. Polymers. 2023; 15(5):1082. https://doi.org/10.3390/polym15051082
Chicago/Turabian StyleSugiaman, Vinna K., Jeffrey, Silvia Naliani, Natallia Pranata, Rudy Djuanda, and Rosalina Intan Saputri. 2023. "Polymeric Scaffolds Used in Dental Pulp Regeneration by Tissue Engineering Approach" Polymers 15, no. 5: 1082. https://doi.org/10.3390/polym15051082
APA StyleSugiaman, V. K., Jeffrey, Naliani, S., Pranata, N., Djuanda, R., & Saputri, R. I. (2023). Polymeric Scaffolds Used in Dental Pulp Regeneration by Tissue Engineering Approach. Polymers, 15(5), 1082. https://doi.org/10.3390/polym15051082