
Development of 3D Printed Biodegradable Mesh with Antimicrobial Properties for Pelvic Organ Prolapse

 , , , ,
, , , ,
Abstract
1. Introduction
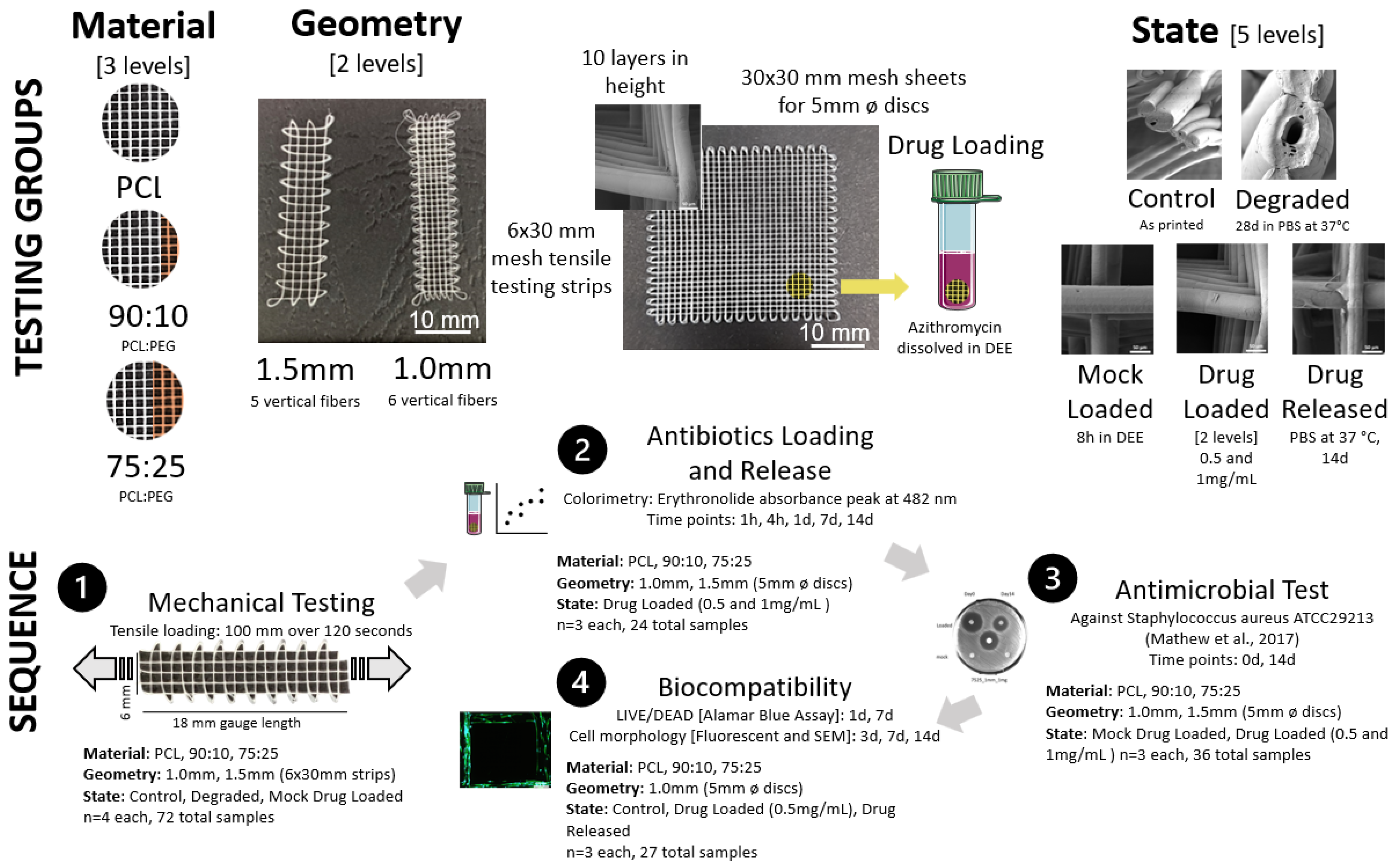
2. Materials and Methods
2.1. PCL/PEG Composite Preparation
2.2. Melt-Electrowriting of PCL and PCL/PEG Meshes
2.3. Mesh Degradation
2.3.1. Physiological Condition Degradation
2.3.2. Accelerated Degradation
2.4. Mechanical Testing
2.5. Antibiotics Loading and Release Profile
2.5.1. Antibiotics Loading
2.5.2. Antibiotics Loading Efficiency
2.5.3. Antibiotics Release Profile
2.6. Antimicrobial Test
2.7. Biocompatibility Test
2.7.1. Cell Seeding
2.7.2. Cell Viability Assessment: LIVE/DEAD and alamarBlue Assays
2.7.3. Cell Morphology: Fluorescent Microscopy and SEM
2.8. Statistical Analysis
3. Results
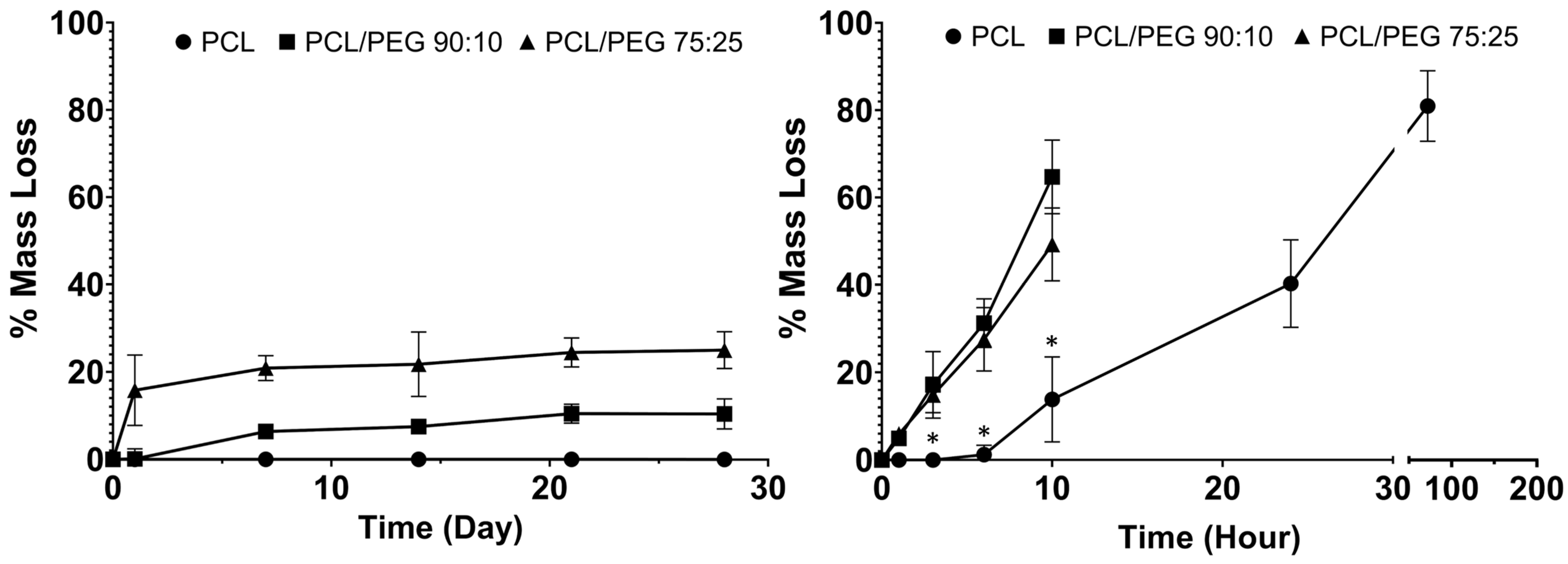
3.1. Degradation Test
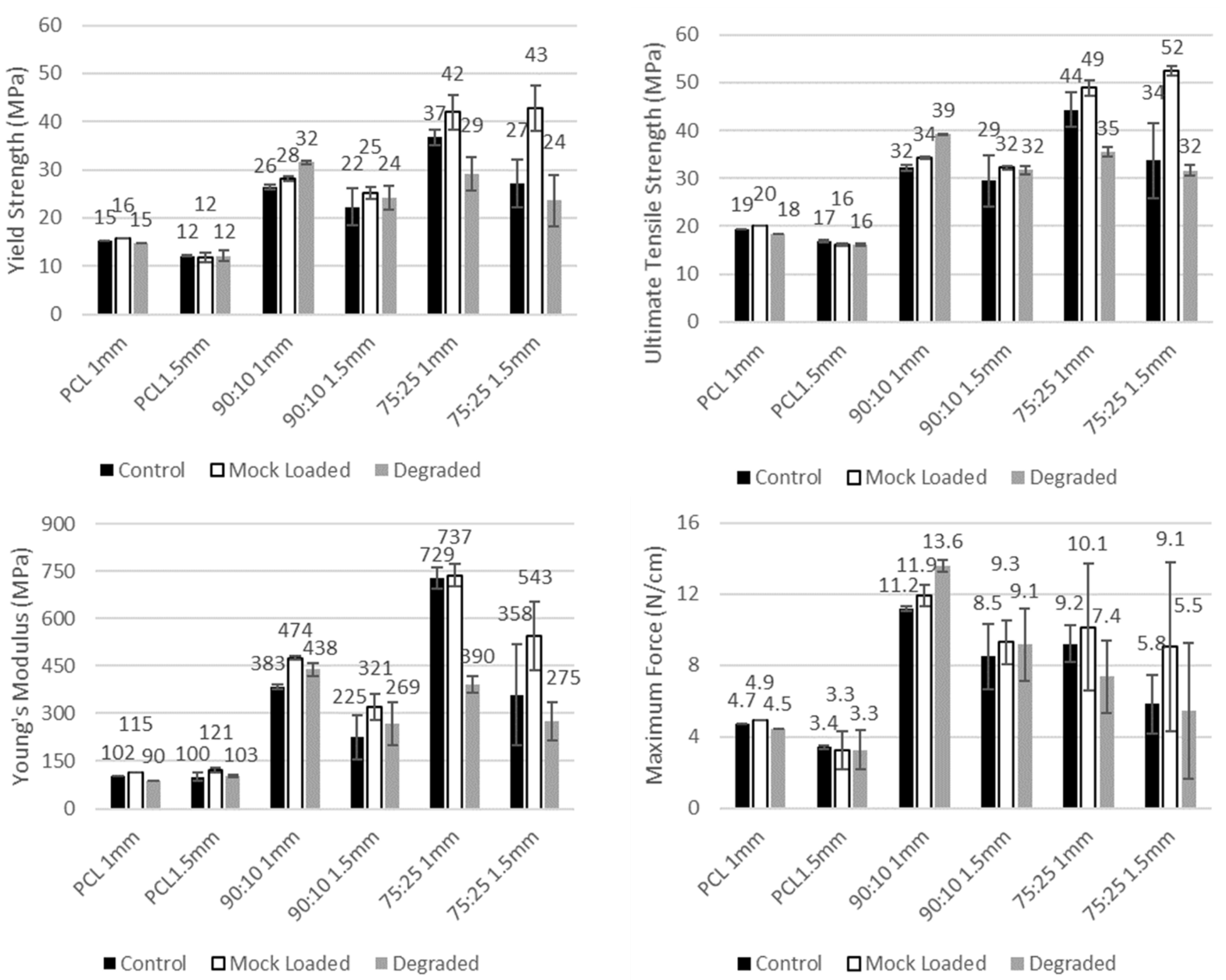
3.2. Mechanical Testing
3.3. Antibiotics Release
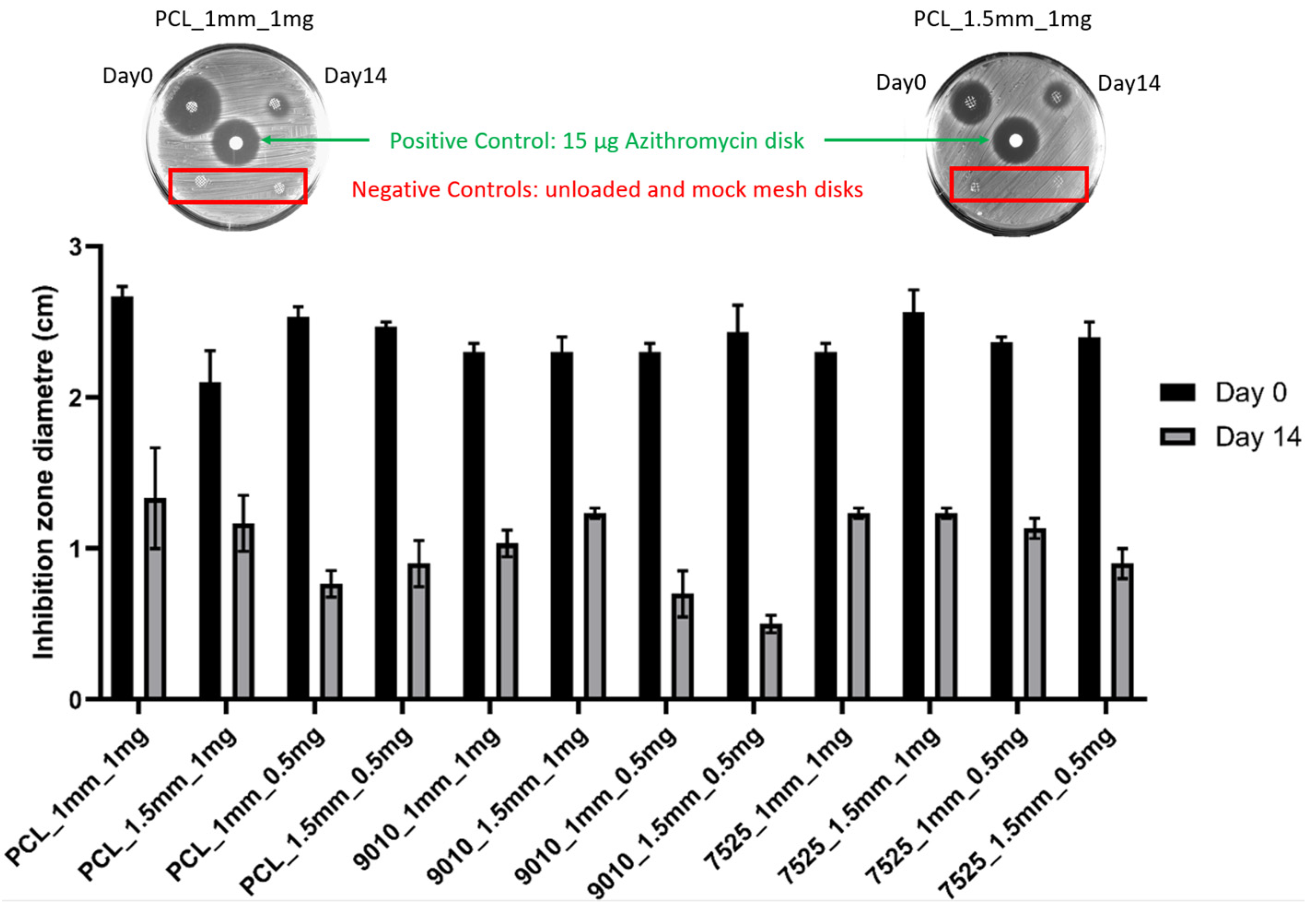
3.4. Antimicrobial Test
3.5. Biocompatibility Test
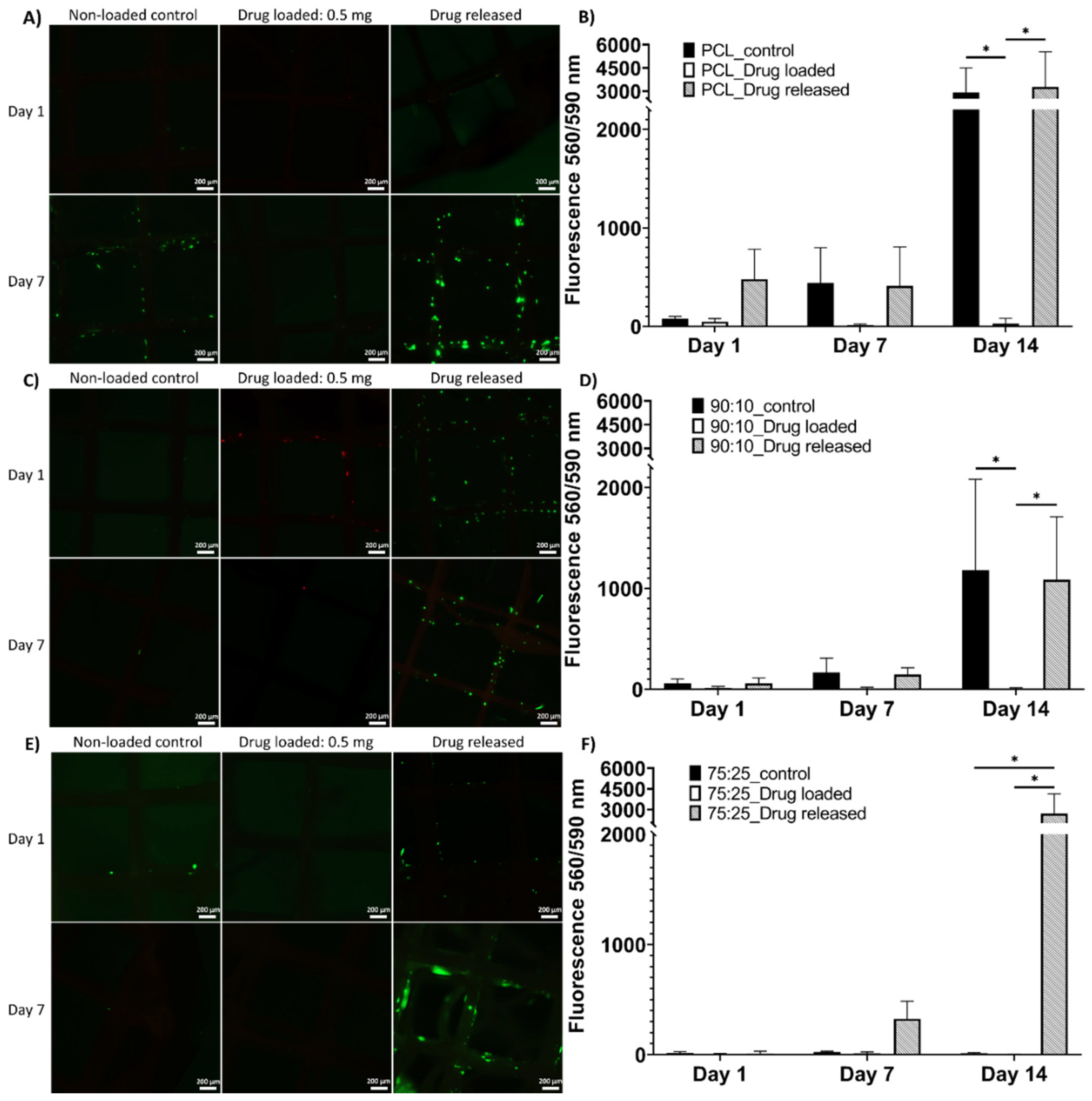
3.5.1. LIVE/DEAD and alamarBlue Assay
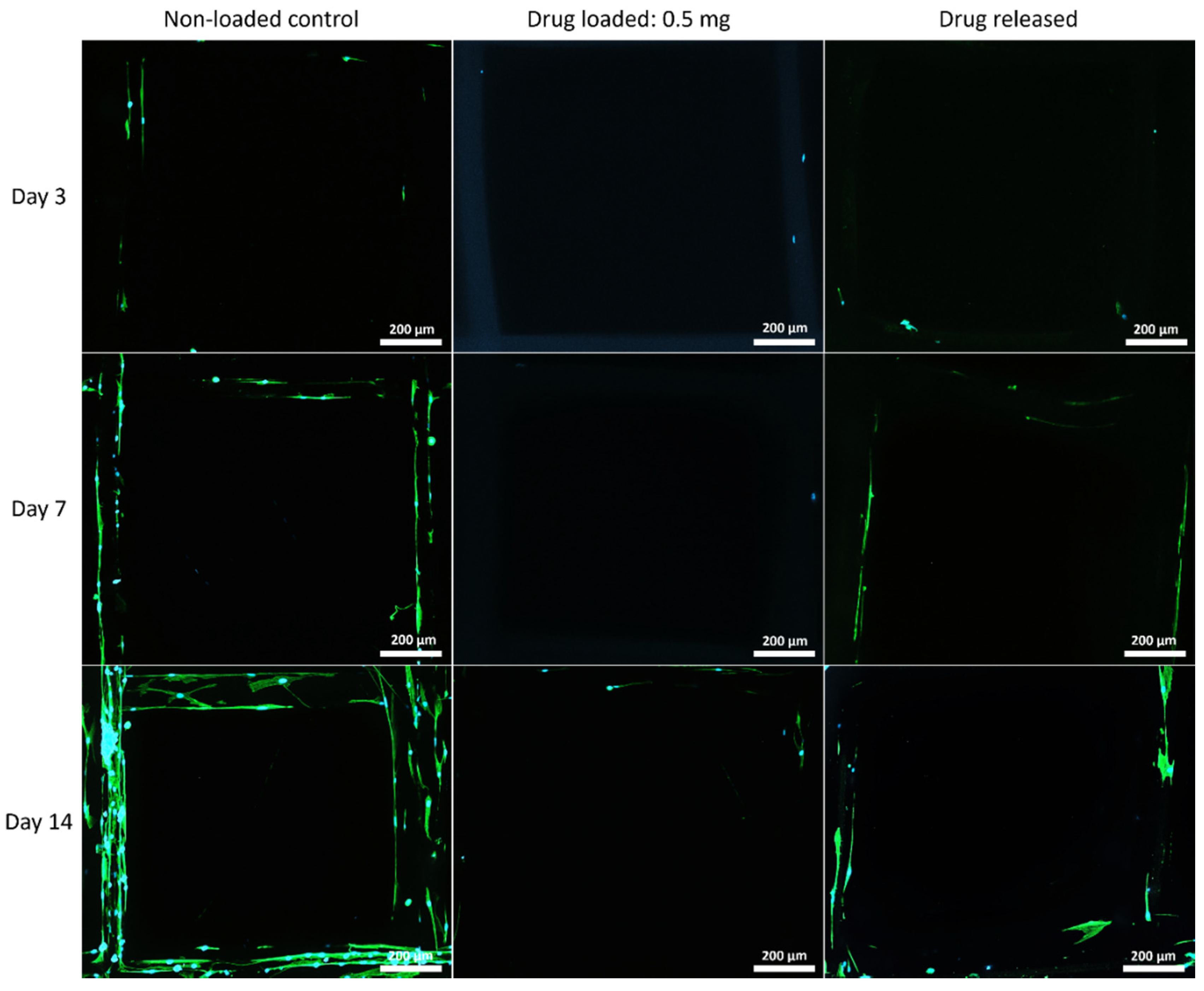
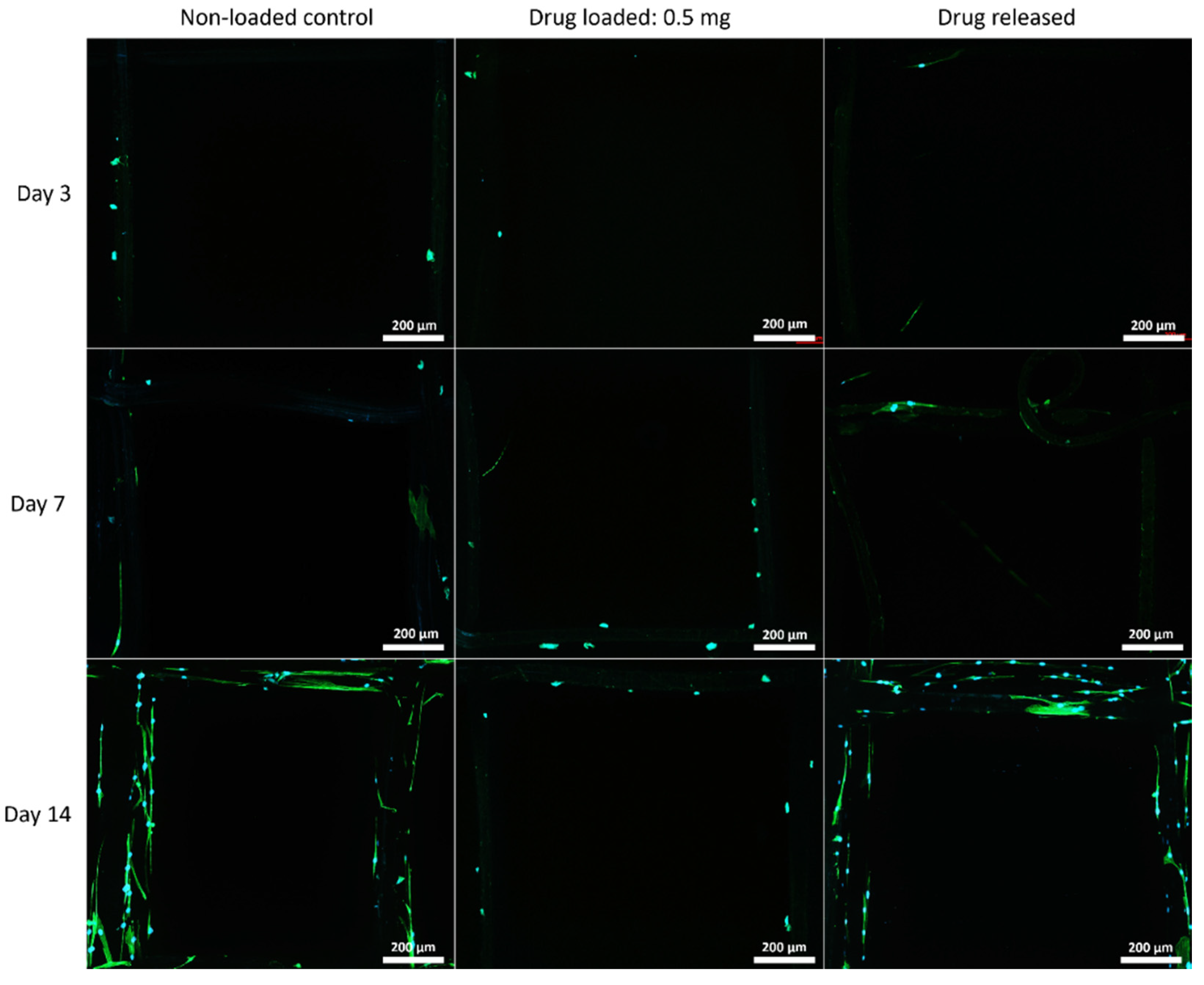
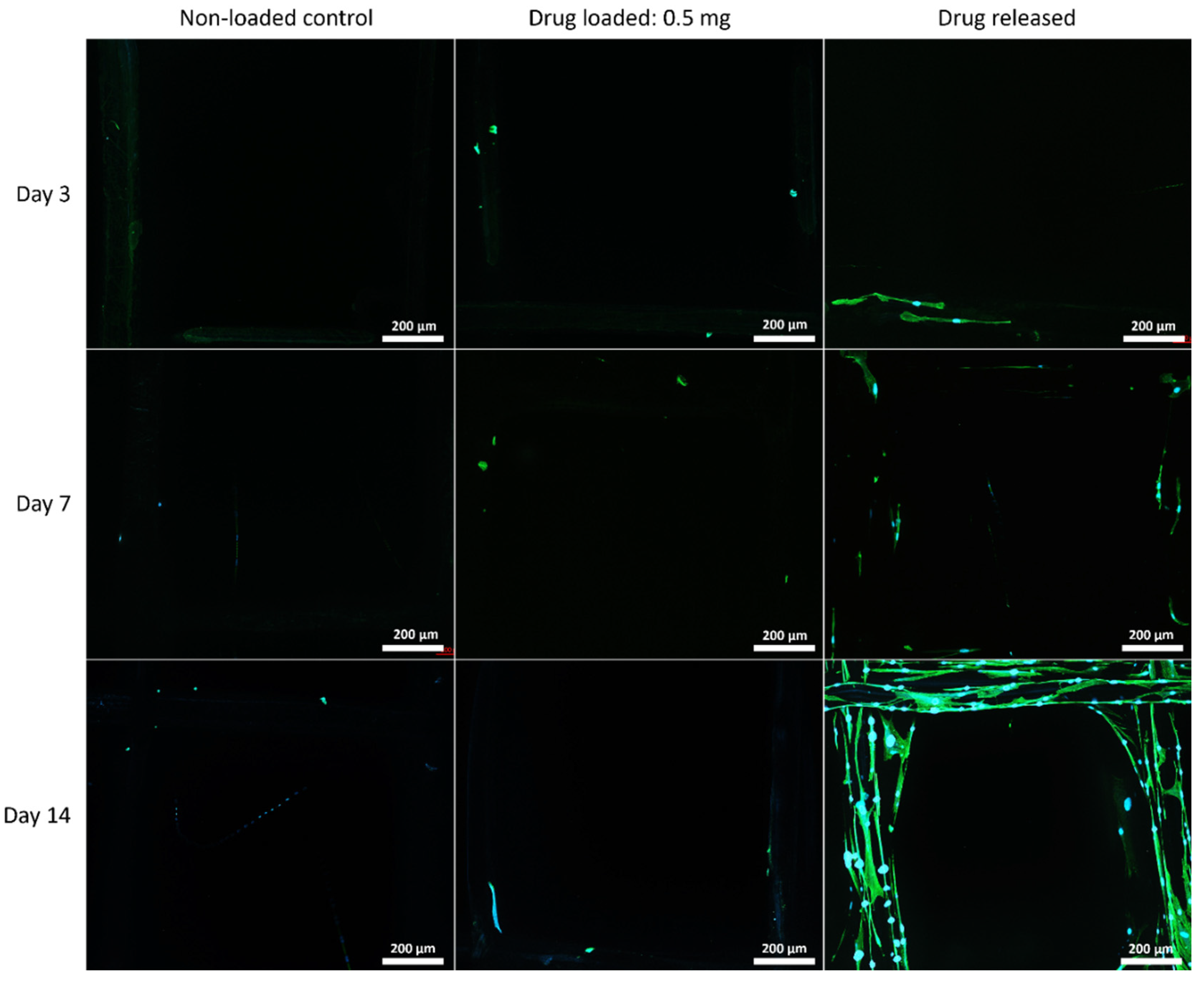
3.5.2. Cell Morphology by Fluorescent Microscopy
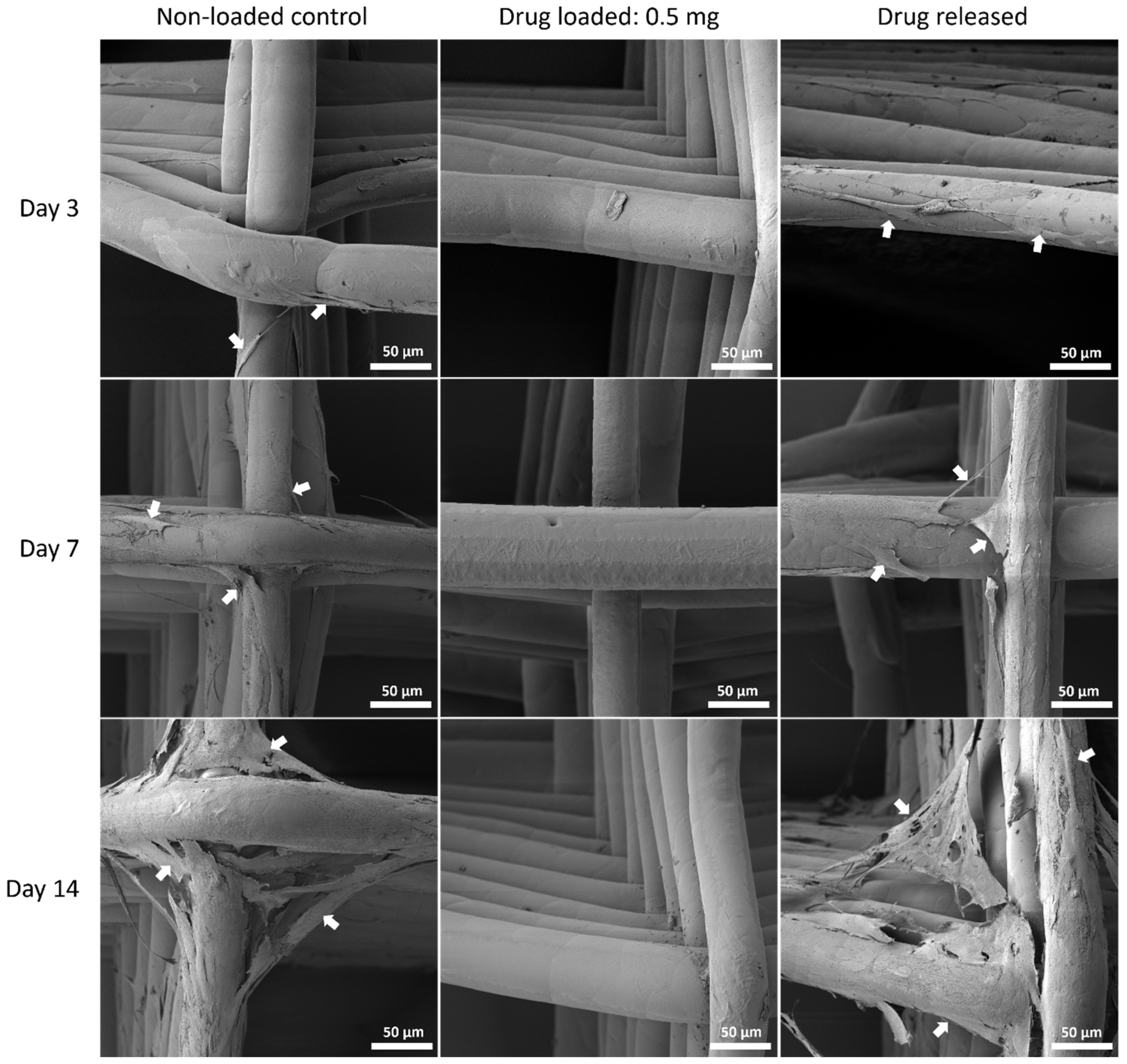
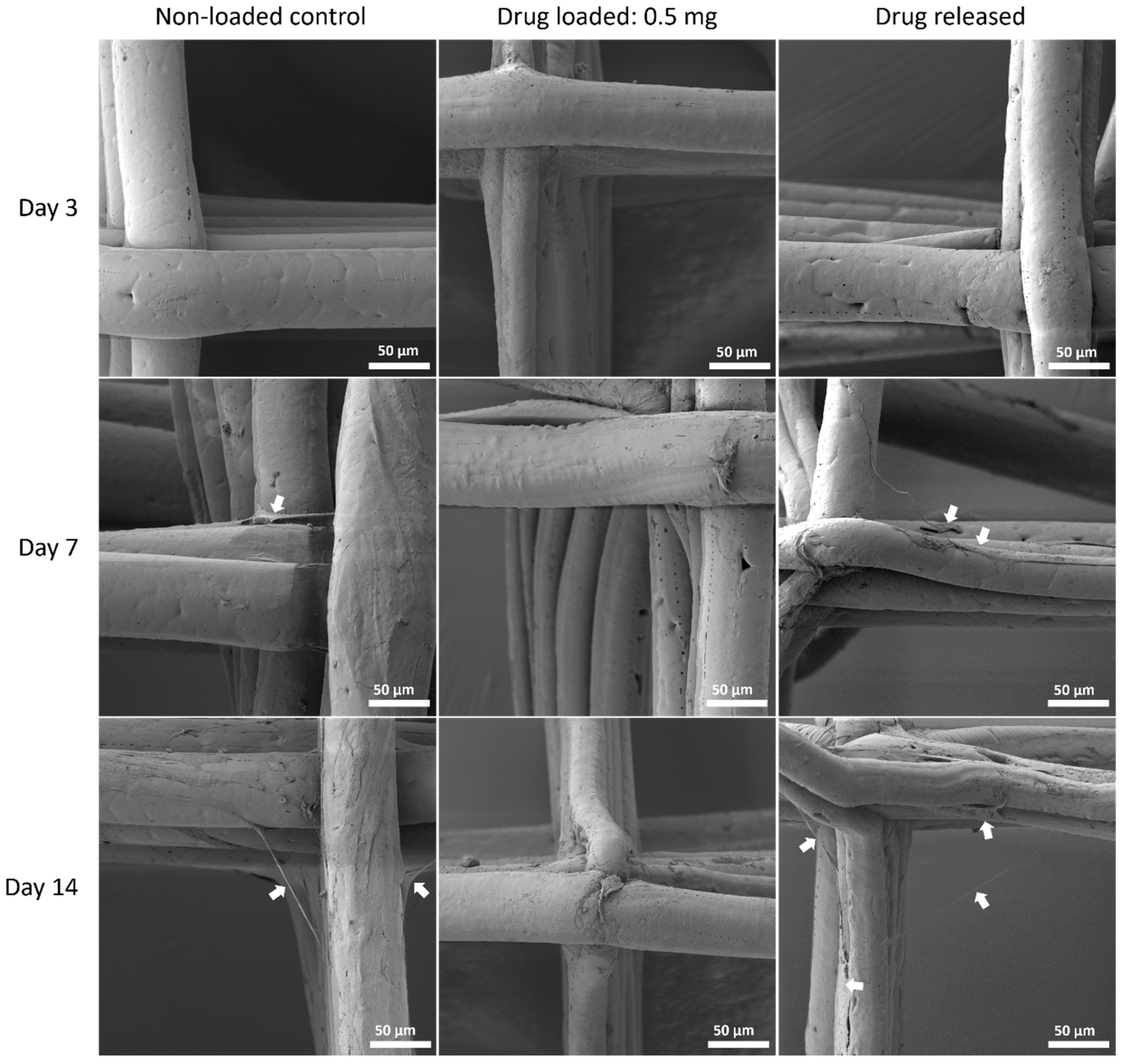
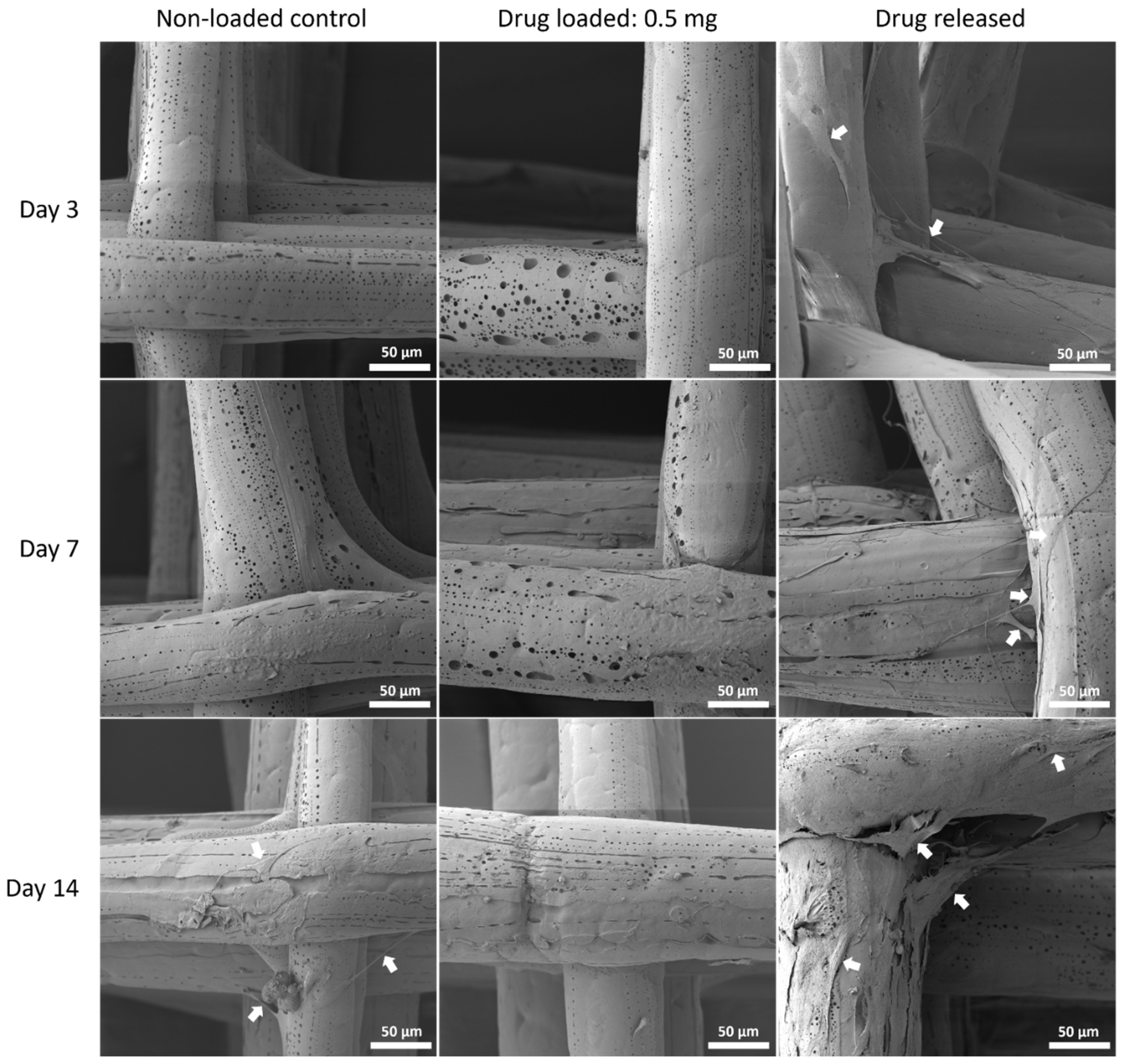
3.5.3. Cell Morphology by SEM
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Khron, A.; Llewellyn, G. Sterilisation; Community Affairs References Committee: Canberra, Australia, 2013.
- Gibson, W.; Wagg, A. Are older women more likely to receive surgical treatment for stress urinary incontinence since the introduction of the mid-urethral sling? An examination of Hospital Episode Statistics data. BJOG Int. J. Obstet. Gynaecol. 2015, 123, 1386–1392. [Google Scholar] [CrossRef] [PubMed]
- Funk, M.J.; Edenfield, A.L.; Pate, V.; Visco, A.G.; Weidner, A.C.; Wu, J.M. Trends in use of surgical mesh for pelvic organ prolapse. Am. J. Obstet. Gynecol. 2012, 208, 79.e1–79.e7. [Google Scholar] [CrossRef] [PubMed]
- The Senate Community Affairs Reference Committee. Number of Women in Australia Who Have Had Transvaginal Mesh Implants and Related Matters. 2018. Available online: https://www.health.gov.au/resources/publications/the-number-of-women-in-australia-who-have-had-transvaginal-mesh-implants-and-related-matters (accessed on 10 January 2022).
- Keltie, K.; Elneil, S.; Monga, A.; Patrick, H.; Powell, J.; Campbell, B.; Sims, A.J. Complications following vaginal mesh procedures for stress urinary incontinence: An 8 year study of 92,246 women. Sci. Rep. 2017, 7, 12015. [Google Scholar] [CrossRef] [PubMed]
- Sedrakyan, A.; Chughtai, B.; Mao, J. Regulatory warnings and use of surgical mesh in pelvic organ prolapse. JAMA Intern. Med. 2016, 176, 275–277. [Google Scholar] [CrossRef] [PubMed]
- Edwards, S.L.; Werkmeister, J.A.; Rosamilia, A.; Ramshaw, J.A.; White, J.F.; Gargett, C.E. Characterisation of clinical and newly fabricated meshes for pelvic organ prolapse repair. J. Mech. Behav. Biomed. Mater. 2013, 23, 53–61. [Google Scholar] [CrossRef]
- Mangir, N.; Dikici, B.A.; Chapple, C.R.; MacNeil, S. Landmarks in vaginal mesh development: Polypropylene mesh for treatment of SUI and POP. Nat. Rev. Urol. 2019, 16, 675–689. [Google Scholar] [CrossRef] [PubMed]
- Marcus-Braun, N.; von Theobald, P. Mesh removal following transvaginal mesh placement: A case series of 104 operations. Int. Urogynecol. J. 2010, 21, 423–430. [Google Scholar] [CrossRef]
- De Tayrac, R.; Letouzey, V. Basic science and clinical aspects of mesh infection in pelvic floor reconstructive surgery. Int. Urogynecol. J. 2011, 22, 775–780. [Google Scholar] [CrossRef]
- Feola, A.; Barone, W.; Moalli, P.; Abramowitch, S. Characterizing the ex vivo textile and structural properties of synthetic prolapse mesh products. Int. Urogynecol. J. 2013, 24, 559–564. [Google Scholar] [CrossRef]
- De Maria, C.; Santoro, V.; Vozzi, G. Biomechanical, Topological and Chemical Features That Influence the Implant Success of an Urogynecological Mesh: A Review. Biomed Res. Int. 2016, 2016, 1267521. [Google Scholar] [CrossRef]
- Paxton, N.C.; Ren, J.; Ainsworth, M.; Solanki, A.K.; Jones, J.R.; Allenby, M.C.; Stevens, M.M.; Woodruff, M.A. Rheological Characterization of Biomaterials Directs Additive Manufacturing of Strontium-Substituted Bioactive Glass/Polycaprolactone Microfibers. Macromol. Rapid Commun. 2019, 40, 1900019. [Google Scholar] [CrossRef] [PubMed]
- Pang, L.; Paxton, N.C.; Ren, J.; Liu, F.; Zhan, H.; Woodruff, M.A.; Bo, A.; Gu, Y. Development of Mechanically Enhanced Polycaprolactone Composites by a Functionalized Titanate Nanofiller for Melt Electrowriting in 3D Printing. ACS Appl. Mater. Interfaces 2020, 12, 47993–48006. [Google Scholar] [CrossRef] [PubMed]
- Lam, C.X.F.; Savalani, M.M.; Teoh, S.-H.; Hutmacher, D.W. Dynamics of in vitro polymer degradation of polycaprolactone-based scaffolds: Accelerated versus simulated physiological conditions. Biomed. Mater. 2008, 3, 034108. [Google Scholar] [CrossRef] [PubMed]
- Mathew, A.; Vaquette, C.; Hashimi, S.; Rathnayake, I.; Huygens, F.; Hutmacher, D.W.; Ivanovski, S. Antimicrobial and Immunomodulatory Surface-Functionalized Electrospun Membranes for Bone Regeneration. Adv. Health Mater. 2017, 6, 1601345. [Google Scholar] [CrossRef]
- Sultana, N.; Arayne, M.S.; Hussain, F.; Fatima, A. Degradation studies of azithromycin and its spectrophotometric determination in pharmaceutical dosage forms. Pak. J. Pharm. Sci. 2006, 19, 98–103. [Google Scholar]
- Gräfe, D.; Gernhardt, M.; Ren, J.; Blasco, E.; Wegener, M.; Woodruff, M.A.; Barner-Kowollik, C. Enzyme-Degradable 3D Multi-Material Microstructures. Adv. Funct. Mater. 2021, 31, 2006998. [Google Scholar] [CrossRef]
- Ren, J.; Blackwood, K.A.; Doustgani, A.; Poh, P.P.; Steck, R.; Stevens, M.M.; Woodruff, M.A. Melt-electrospun polycaprolactone strontium-substituted bioactive glass scaffolds for bone regeneration. J. Biomed. Mater. Res. Part A 2013, 102, 3140–3153. [Google Scholar] [CrossRef]
- Mirjavan, M.; Asayesh, A.; Jeddi, A.A.A. The effect of fabric structure on the mechanical properties of warp knitted surgical mesh for hernia repair. J. Mech. Behav. Biomed. Mater. 2017, 66, 77–86. [Google Scholar] [CrossRef]
- Lu, Y.; Fu, S.; Zhou, S.; Chen, G.; Zhu, C.; Li, N.; Ma, Y. Preparation and biocompatibility evaluation of polypropylene mesh coated with electrospinning membrane for pelvic defects repair. J. Mech. Behav. Biomed. Mater. 2018, 81, 142–148. [Google Scholar] [CrossRef]
- Mangır, N.; Hillary, C.J.; Chapple, C.R.; MacNeil, S. Oestradiol-releasing Biodegradable Mesh Stimulates Collagen Production and Angiogenesis: An Approach to Improving Biomaterial Integration in Pelvic Floor Repair. Eur. Urol. Focus 2017, 5, 280–289. [Google Scholar] [CrossRef]
- Vashaghian, M.; Zandieh-Doulabi, B.; Roovers, J.-P.; Smit, T.H. Electrospun Matrices for Pelvic Floor Repair: Effect of Fiber Diameter on Mechanical Properties and Cell Behavior. Tissue Eng. Part A 2016, 22, 1305–1316. [Google Scholar] [CrossRef] [PubMed]
- Paul, K.; Darzi, S.; McPhee, G.; Del Borgo, M.P.; Werkmeister, J.A.; Gargett, C.E.; Mukherjee, S. 3D bioprinted endometrial stem cells on melt electrospun poly ε-caprolactone mesh for pelvic floor application promote anti-inflammatory responses in mice. Acta Biomater. 2019, 97, 162–176. [Google Scholar] [CrossRef] [PubMed]
- Mancuso, E.; Downey, C.; Doxford-Hook, E.; Bryant, M.G.; Culmer, P. The use of polymeric meshes for pelvic organ prolapse: Current concepts, challenges, and future perspectives. J. Biomed. Mater. Res. Part B Appl. Biomater. 2019, 108, 771–789. [Google Scholar] [CrossRef] [PubMed]
- Vashaghian, M.; Ruiz-Zapata, A.; Kerkhof, M.H.; Doulabi, B.Z.; Werner, A.; Roovers, J.P.; Smit, T.H. Toward a new generation of pelvic floor implants with electrospun nanofibrous matrices: A feasibility study. Neurourol. Urodynamics 2016, 36, 565–573. [Google Scholar] [CrossRef] [PubMed]
- Woodruff, M.; Hutmacher, D.W. The return of a forgotten polymer—Polycaprolactone in the 21st century. Prog. Polym. Sci. 2010, 35, 1217–1256. [Google Scholar] [CrossRef]
- Guazzelli, E.; Galli, G.; Martinelli, E. The Effect of Poly(ethylene glycol) (PEG) Length on the Wettability and Surface Chemistry of PEG-Fluoroalkyl-Modified Polystyrene Diblock Copolymers and Their Two-Layer Films with Elastomer Matrix. Polymers 2020, 12, 1236. [Google Scholar] [CrossRef] [PubMed]
- Shi, L.; Zhang, J.; Zhao, M.; Tang, S.; Cheng, X.; Zhang, W.; Li, W.; Liu, X.; Peng, H.; Wang, Q. Effects of polyethylene glycol on the surface of nanoparticles for targeted drug delivery. Nanoscale 2021, 13, 10748–10764. [Google Scholar] [CrossRef] [PubMed]
- Lins, L.C.; Wianny, F.; Livi, S.; Hidalgo, I.A.; Dehay, C.; Duchet-Rumeau, J.; Gérard, J.-F. Development of Bioresorbable Hydrophilic–Hydrophobic Electrospun Scaffolds for Neural Tissue Engineering. Biomacromolecules 2016, 17, 3172–3187. [Google Scholar] [CrossRef] [PubMed]
- Salimi, S.; Wu, Y.; Barreiros, M.I.E.; Natfji, A.A.; Khaled, S.; Wildman, R.; Hart, L.R.; Greco, F.; Clark, E.A.; Roberts, C.; et al. A 3D printed drug delivery implant formed from a dynamic supramolecular polyurethane formulation. Polym. Chem. 2020, 11, 3453–3464. [Google Scholar] [CrossRef]
- Ranganathan, S.I.; Kohama, C.; Mercurio, T.; Salvatore, A.; Benmassaoud, M.M.; Kim, T.W.B. Effect of temperature and ultraviolet light on the bacterial kill effectiveness of antibiotic-infused 3D printed implants. Biomed. Microdevices 2020, 22, 1–14. [Google Scholar] [CrossRef]
- Stewart, S.A.; Domínguez-Robles, J.; McIlorum, V.J.; Gonzalez, Z.; Utomo, E.; Mancuso, E.; Lamprou, D.A.; Donnelly, R.F.; Larrañeta, E. Poly(caprolactone)-Based Coatings on 3D-Printed Biodegradable Implants: A Novel Strategy to Prolong Delivery of Hydrophilic Drugs. Mol. Pharm. 2020, 17, 3487–3500. [Google Scholar] [CrossRef] [PubMed]
- Lanaro, M.; Luu, A.; Lightbody-Gee, A.; Hedger, D.; Powell, S.K.; Holmes, D.W.; Woodruff, M.A. Systematic design of an advanced open-source 3D bioprinter for extrusion and electrohydrodynamic-based processes. Int. J. Adv. Manuf. Technol. 2021, 113, 2539–2554. [Google Scholar] [CrossRef]
- Nguyen Tri, P.; Prud’Homme, R.E. Crystallization and Segregation Behavior at the Submicrometer Scale of PCL/PEG Blends. Macromolecules 2018, 51, 7266–7273. [Google Scholar] [CrossRef]
- Vieira, A.; Guedes, R.; Marques, A. Degradation and Viscoelastic Properties of PLA-PCL, PGA-PCL, PDO and PGA Fibres. Mater. Sci. Forum 2010, 636–637, 825–832. [Google Scholar] [CrossRef]
- Clavé, A.; Yahi, H.; Hammou, J.-C.; Montanari, S.; Gounon, P.; Clavé, H. Polypropylene as a reinforcement in pelvic surgery is not inert: Comparative analysis of 100 explants. Int. Urogynecol. J. 2010, 21, 261–270. [Google Scholar] [CrossRef]
- Douglas, P.; Albadarin, A.; Sajjia, M.; Mangwandi, C.; Kuhs, M.; Collins, M.N.; Walker, G. Effect of poly ethylene glycol on the mechanical and thermal properties of bioactive poly(ε-caprolactone) melt extrudates for pharmaceutical applications. Int. J. Pharm. 2016, 500, 179–186. [Google Scholar] [CrossRef]
- Powers, S.; Burleson, L.K.; Hannan, J.L. Managing female pelvic floor disorders: A medical device review and appraisal. Interface Focus 2019, 9, 20190014. [Google Scholar] [CrossRef]
- Liang, R.; Abramowitch, S.; Knight, K.M.; Palcsey, S.; Nolfi, A.; Feola, A.; Stein, S.; Moalli, P.A. Vaginal degeneration following implantation of synthetic mesh with increased stiffness. BJOG: Int. J. Obstet. Gynaecol. 2012, 120, 233–243. [Google Scholar] [CrossRef]
- Mistrangelo, E.; Mancuso, S.; Nadalini, C.; Lijoi, D.; Costantini, S. Rising use of synthetic mesh in transvaginal pelvic reconstructive surgery: A review of the risk of vaginal erosion. J. Minim. Invasive Gynecol. 2007, 14, 564–569. [Google Scholar] [CrossRef]
- Visco, A.G.; Weidner, A.C.; Barber, M.D.; Myers, E.R.; Cundiff, G.W.; Bump, R.C.; Addison, W. Vaginal mesh erosion after abdominal sacral colpopexy. Am. J. Obstet. Gynecol. 2001, 184, 297–302. [Google Scholar] [CrossRef]
- Ding, J.; Deng, M.; Song, X.-C.; Chen, C.; Lai, K.-L.; Wang, G.-S.; Yuan, Y.-Y.; Xu, T.; Zhu, L. Nanofibrous biomimetic mesh can be used for pelvic reconstructive surgery: A randomized study. J. Mech. Behav. Biomed. Mater. 2016, 61, 26–35. [Google Scholar] [CrossRef] [PubMed]
- Pott, P.P.; Schwarz, M.L.R.; Gundling, R.; Nowak, K.; Hohenberger, P.; Roessner, E.D. Mechanical Properties of Mesh Materials Used for Hernia Repair and Soft Tissue Augmentation. PLoS ONE 2012, 7, e46978. [Google Scholar] [CrossRef] [PubMed]
- Weyhe, D.; Cobb, W.; Lecuivre, J.; Alves, A.; Ladet, S.; Lomanto, D.; Bayon, Y. Large pore size and controlled mesh elongation are relevant predictors for mesh integration quality and low shrinkage—Systematic analysis of key parameters of meshes in a novel minipig hernia model. Int. J. Surg. 2015, 22, 46–53. [Google Scholar] [CrossRef]
- Lake, S.; Ray, S.; Zihni, A.M.; Thompson, D.M.; Gluckstein, J.; Deeken, C.R. Pore size and pore shape—But not mesh density—Alter the mechanical strength of tissue ingrowth and host tissue response to synthetic mesh materials in a porcine model of ventral hernia repair. J. Mech. Behav. Biomed. Mater. 2015, 42, 186–197. [Google Scholar] [CrossRef]
- Solovieva, A.; Miroshnichenko, S.; Kovalskii, A.; Permyakova, E.; Popov, Z.; Dvořáková, E.; Kiryukhantsev-Korneev, P.; Obrosov, A.; Polčák, J.; Zajickova, L.; et al. Immobilization of Platelet-Rich Plasma onto COOH Plasma-Coated PCL Nanofibers Boost Viability and Proliferation of Human Mesenchymal Stem Cells. Polymers 2017, 9, 736. [Google Scholar] [CrossRef] [PubMed]
- Gu, W.; Hong, X.; Le Bras, A.; Nowak, W.; Bhaloo, S.I.; Deng, J.; Xie, Y.; Hu, Y.; Ruan, X.Z.; Xu, Q. Smooth muscle cells differentiated from mesenchymal stem cells are regulated by microRNAs and suitable for vascular tissue grafts. J. Biol. Chem. 2018, 293, 8089–8102. [Google Scholar] [CrossRef]
- Khaki, M.; Salmanian, A.H.; Abtahi, H.; Ganji, A.; Mosayebi, G. Mesenchymal Stem Cells Differentiate to Endothelial Cells Using Recombinant Vascular Endothelial Growth Factor -A. Rep. Biochem. Mol. Biol. 2018, 6, 144–150. [Google Scholar]
- Beckermann, B.M.; Kallifatidis, G.; Groth, A.; Frommhold, D.; Apel, A.; Mattern, J.; Salnikov, A.V.; Moldenhauer, G.; Wagner, W.; Diehlmann, A.; et al. VEGF expression by mesenchymal stem cells contributes to angiogenesis in pancreatic carcinoma. Br. J. Cancer 2008, 99, 622–631. [Google Scholar] [CrossRef]
- Pittenger, M.F.; Discher, D.E.; Péault, B.M.; Phinney, D.G.; Hare, J.M.; Caplan, A.I. Mesenchymal stem cell perspective: Cell biology to clinical progress. NPJ Regen. Med. 2019, 4, 22. [Google Scholar] [CrossRef]
- Scanu, M.; Mancuso, L.; Cao, G. Evaluation of the use of human Mesenchymal Stem Cells for acute toxicity tests. Toxicol. Vitr. 2011, 25, 1989–1995. [Google Scholar] [CrossRef]
- Briggs, T.; Treiser, M.D.; Holmes, P.F.; Kohn, J.; Moghe, P.V.; Arinzeh, T.L. Osteogenic differentiation of human mesenchymal stem cells on poly(ethylene glycol)-variant biomaterials. J. Biomed. Mater. Res. Part A 2008, 91A, 975–984. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Feng, Y.; Fang, Z.; Yuan, W.; Khan, M. Co-electrospun blends of PU and PEG as potential biocompatible scaffolds for small-diameter vascular tissue engineering. Mater. Sci. Eng. C 2012, 32, 2306–2315. [Google Scholar] [CrossRef]
- Dowling, D.; Miller, I.; Ardhaoui, M.; Gallagher, W. Effect of Surface Wettability and Topography on the Adhesion of Osteosarcoma Cells on Plasma-modified Polystyrene. J. Biomater. Appl. 2010, 26, 327–347. [Google Scholar] [CrossRef] [PubMed]
- Hao, L.; Yang, H.; Du, C.; Fu, X.; Zhao, N.; Xu, S.; Cui, F.; Mao, C.; Wang, Y. Directing the fate of human and mouse mesenchymal stem cells by hydroxyl–methyl mixed self-assembled monolayers with varying wettability. J. Mater. Chem. B 2014, 2, 4794–4801. [Google Scholar] [CrossRef] [PubMed]
- Sezer, U.A.; Sanko, V.; Gulmez, M.; Aru, B.; Sayman, E.; Aktekin, A.; Aker, F.V.; Demirel, G.Y.; Sezer, S. Polypropylene composite hernia mesh with anti-adhesion layer composed of polycaprolactone and oxidized regenerated cellulose. Mater. Sci. Eng. C 2019, 99, 1141–1152. [Google Scholar] [CrossRef]
- Nolfi, A.L.; Brown, B.N.; Liang, R.; Palcsey, S.L.; Bonidie, M.J.; Abramowitch, S.D.; Moalli, P.A. Host response to synthetic mesh in women with mesh complications. Am. J. Obstet. Gynecol. 2016, 215, 206.e1–206.e8. [Google Scholar] [CrossRef]
- Bakheit, A.H.; Al-Hadiya, B.M.; Abd-Elgalil, A.A. Azithromycin. Profiles Drug Subst. Excip. Relat. Methodol. 2014, 39, 1–40. [Google Scholar] [CrossRef]
- Parnham, M.J.; Haber, V.E.; Giamarellos-Bourboulis, E.J.; Perletti, G.; Verleden, G.M.; Vos, R. Azithromycin: Mechanisms of action and their relevance for clinical applications. Pharmacol. Ther. 2014, 143, 225–245. [Google Scholar] [CrossRef]
- Rowland, K.; Ewigman, B. Azithromycin for PID beats doxycycline on all counts. J. Fam. Pract. 2007, 56, 1006–1009. [Google Scholar]
- Kurnia, S. Biocompatibility of Azitromicyn on Connective Tissue. Indones. J. Trop. Infect. Dis. 2015, 2, 42–45. [Google Scholar] [CrossRef][Green Version]
- Cosson, M.; Debodinance, P.; Boukerrou, M.; Chauvet, M.P.; Lobry, P.; Ego, A. Mechanical properties of synthetic implants used in the repair of prolapse and urinary incontinence in women: Which is the ideal material? Int. Urogynecol. J. 2003, 14, 169–178. [Google Scholar] [CrossRef] [PubMed]
- Goel, V.K.; Lim, T.-H.; Gwon, J.; Chen, J.-Y.; Winterbottom, J.M.; Park, J.B.; Weinstein, J.N.; Ahn, J.-Y. Effects of Rigidity of an Internal Fixation Device A Comprehensive Biomechanical Investigation. Spine 1991, 16, S155–S161. [Google Scholar] [CrossRef] [PubMed]
- Huiskes, H.R.; Weinans, H.; Grootenboer, H.J.; Dalstra, M.M.; Fudala, B.; Slooff, T.T. Adaptive bone-remodeling theory applied to prosthetic-design analysis. J. Biomech. 1987, 20, 1135–1150. [Google Scholar] [CrossRef]
- Rumian, A.P.; Draper, E.R.C.; Wallace, A.L.; Goodship, A.E. The influence of the mechanical environment on remodelling of the patellar tendon. J. Bone Jt. Surg. Br. Vol. 2009, 91, 557–564. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, E.; Hayashi, K.; Yamamoto, N. Effects of stress shielding on the transverse mechanical properties of rabbit patellar tendons. J. Biomech. Eng. 2000, 122, 608–614. [Google Scholar] [CrossRef] [PubMed]













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Mesh Type | Voltage (kV) | Temperature (°C) | Tip to Collector Distance (mm) | Needle Gauge | Air Pressure (MPa) | Plate Speed |
|---|---|---|---|---|---|---|
| PCL/PEG 90:10 | 4.5 | 95 | 5 | 21 | 0.08 | 300 |
| PCL/PEG 75:25 | 4.5 | 95 | 5 | 21 | 0.08 | 300 |
| PCL (Control) | 6 | 90 | 5 | 21 | 0.05 | 600 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ren, J.; Murray, R.; Wong, C.S.; Qin, J.; Chen, M.; Totsika, M.; Riddell, A.D.; Warwick, A.; Rukin, N.; Woodruff, M.A. Development of 3D Printed Biodegradable Mesh with Antimicrobial Properties for Pelvic Organ Prolapse. Polymers 2022, 14, 763. https://doi.org/10.3390/polym14040763
Ren J, Murray R, Wong CS, Qin J, Chen M, Totsika M, Riddell AD, Warwick A, Rukin N, Woodruff MA. Development of 3D Printed Biodegradable Mesh with Antimicrobial Properties for Pelvic Organ Prolapse. Polymers. 2022; 14(4):763. https://doi.org/10.3390/polym14040763
Chicago/Turabian StyleRen, Jiongyu, Rebecca Murray, Cynthia S. Wong, Jilong Qin, Michael Chen, Makrina Totsika, Andrew D. Riddell, Andrea Warwick, Nicholas Rukin, and Maria A. Woodruff. 2022. "Development of 3D Printed Biodegradable Mesh with Antimicrobial Properties for Pelvic Organ Prolapse" Polymers 14, no. 4: 763. https://doi.org/10.3390/polym14040763
APA StyleRen, J., Murray, R., Wong, C. S., Qin, J., Chen, M., Totsika, M., Riddell, A. D., Warwick, A., Rukin, N., & Woodruff, M. A. (2022). Development of 3D Printed Biodegradable Mesh with Antimicrobial Properties for Pelvic Organ Prolapse. Polymers, 14(4), 763. https://doi.org/10.3390/polym14040763