
Post-Cure Development of the Degree of Conversion and Mechanical Properties of Dual-Curing Resin Cements

 , ,
, ,  ,
, 
Abstract
:1. Introduction
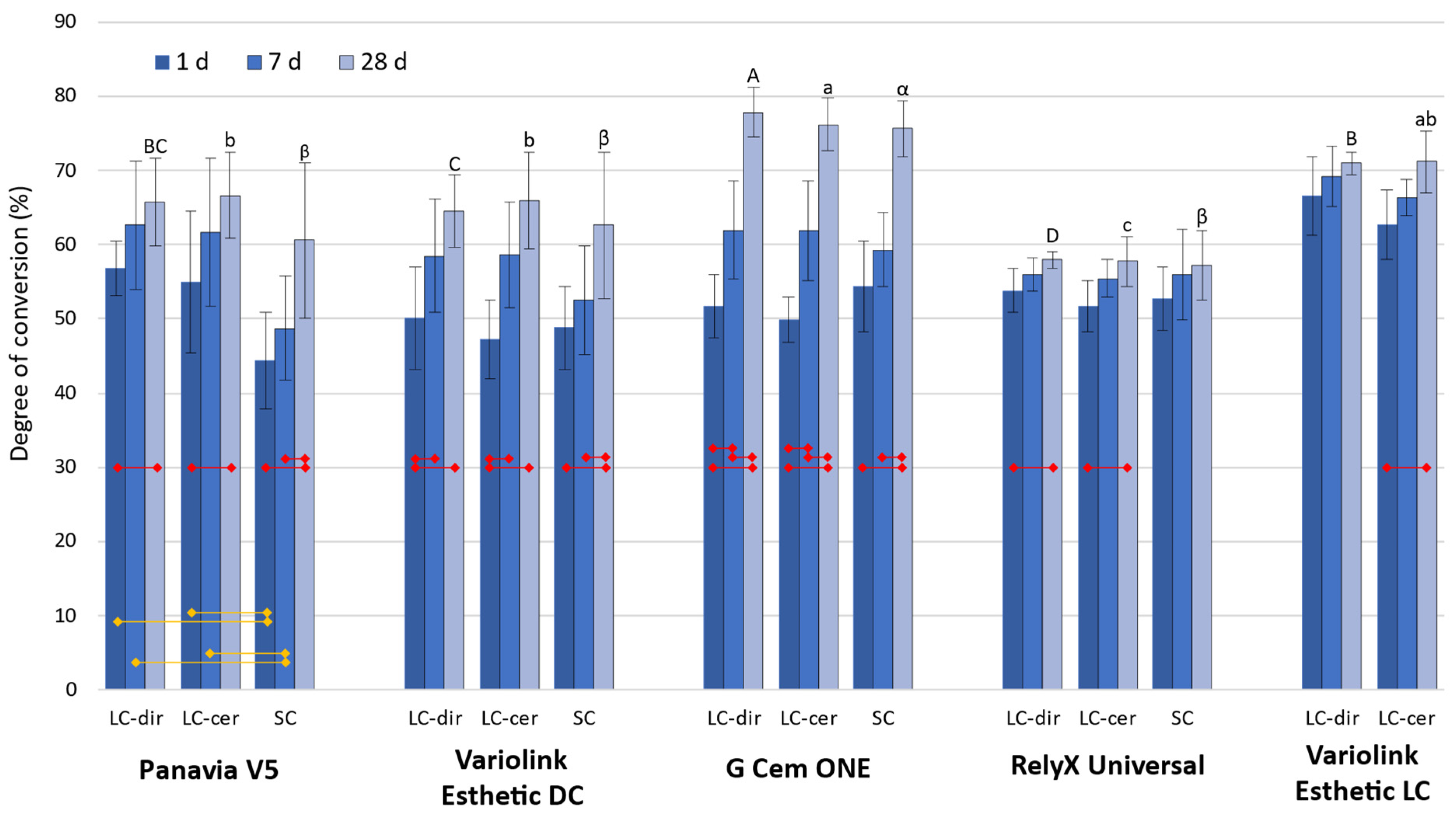
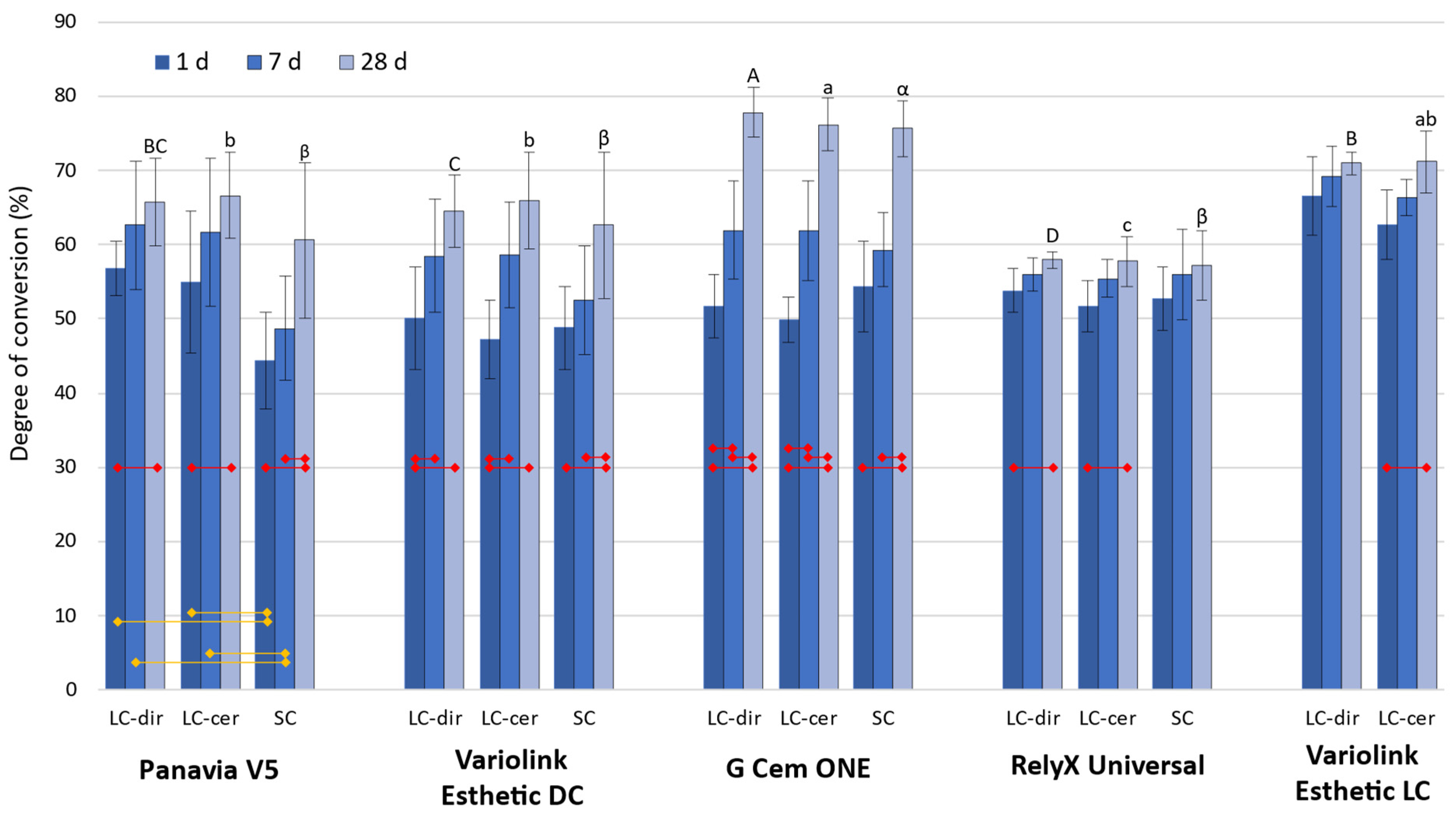
- The DC values and the post-cure DC development over 28 days would not be affected by the curing conditions (direct light-curing, light-curing through ceramics, and self-curing);
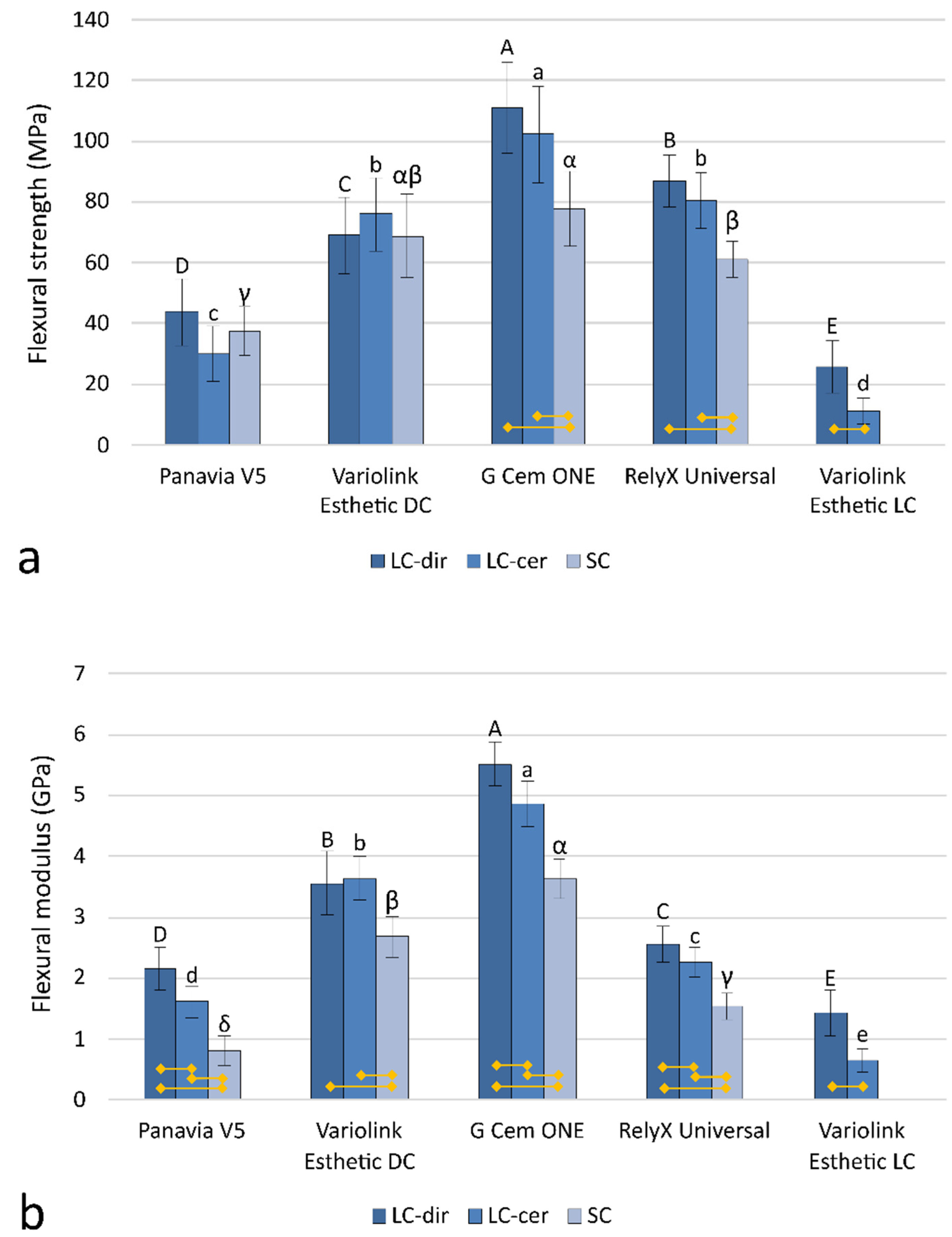
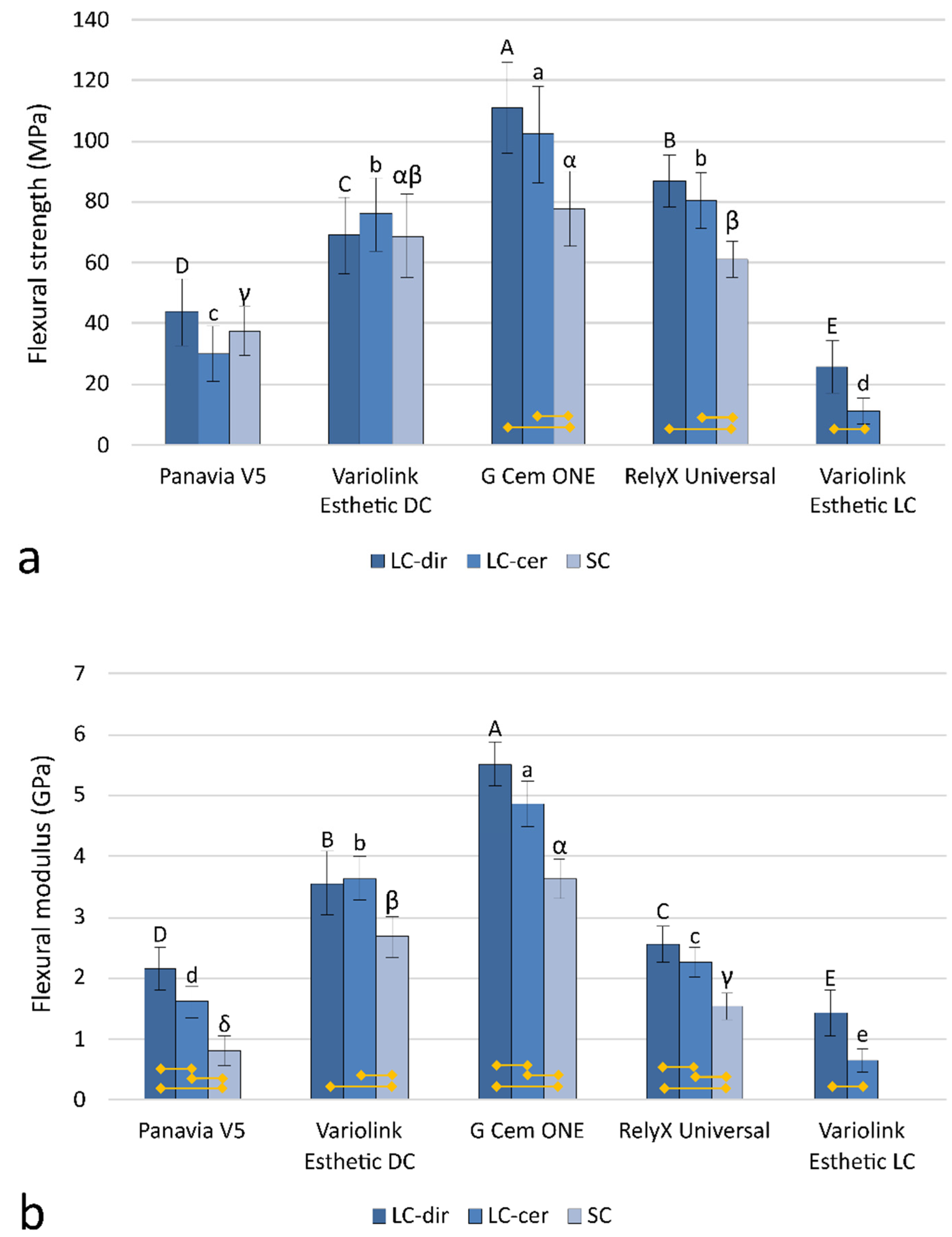
- The mechanical properties measured after 28 days would not be affected by the curing conditions.
2. Materials and Methods
2.1. Composite Cements and Curing Protocols
- LC-dir (Light-cured directly): 1080 mW/cm2 for 20 s by positioning the curing unit light guide tip immediately adjacent to the cement specimen;
- LC-cer (Light-cured through a ceramic layer): 280 mW/cm2 for 20 s due to interposition of a 1-mm layer of lithium disilicate glass-ceramic (IPS e.max Press, shade A2; Ivoclar, Schaan, Liechtenstein) between the curing unit light guide tip and the cement specimen;
- SC (Self-cured): without light illumination.
2.2. Degree of Conversion
2.3. Flexural Strength and Modulus
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ferracane, J.L.; Stansbury, J.W.; Burke, F.J.T. Self-Adhesive Resin Cements-Chemistry, Properties and Clinical Considerations. J. Oral Rehabil. 2011, 38, 295–314. [Google Scholar] [CrossRef] [PubMed]
- Kwon, T.-Y.; Bagheri, R.; Kim, Y.K.; Kim, K.-H.; Burrow, M.F. Cure Mechanisms in Materials for Use in Esthetic Dentistry: Cure Mechanisms in Dentistry. J. Investig. Clin. Dent. 2012, 3, 3–16. [Google Scholar] [CrossRef] [PubMed]
- Hofmann, N.; Papsthart, G.; Hugo, B.; Klaiber, B. Comparison of Photo-Activation versus Chemical or Dual-Curing of Resin-Based Luting Cements Regarding Flexural Strength, Modulus and Surface Hardness. J. Oral Rehabil. 2008, 28, 1022–1028. [Google Scholar] [CrossRef]
- Aguiar, T.R.; de Oliveira, M.; Arrais, C.A.G.; Ambrosano, G.M.B.; Rueggeberg, F.; Giannini, M. The Effect of Photopolymerization on the Degree of Conversion, Polymerization Kinetic, Biaxial Flexure Strength, and Modulus of Self-Adhesive Resin Cements. J. Prosthet. Dent. 2015, 113, 128–134. [Google Scholar] [CrossRef] [PubMed]
- Alovisi, M.; Scotti, N.; Comba, A.; Manzon, E.; Farina, E.; Pasqualini, D.; Michelotto Tempesta, R.; Breschi, L.; Cadenaro, M. Influence of Polymerization Time on Properties of Dual-Curing Cements in Combination with High Translucency Monolithic Zirconia. J. Prosthodont. Res. 2018, 62, 468–472. [Google Scholar] [CrossRef]
- Martins, F.V.; Vasques, W.F.; Fonseca, E.M. How the Variations of the Thickness in Ceramic Restorations of Lithium Disilicate and the Use of Different Photopolymerizers Influence the Degree of Conversion of the Resin Cements: A Systematic Review and Meta-Analysis: Variations of the Thickness in Ceramic Restorations. J. Prosthodont. 2019, 28, e395–e403. [Google Scholar] [CrossRef]
- Shim, J.; Han, S.; Jha, N.; Hwang, S.; Ahn, W.; Lee, J.; Ryu, J. Effect of Irradiance and Exposure Duration on Temperature and Degree of Conversion of Dual-Cure Resin Cement for Ceramic Restorations. Oper. Dent. 2018, 43, E280–E287. [Google Scholar] [CrossRef]
- Tafur-Zelada, C.M.; Carvalho, O.; Silva, F.S.; Henriques, B.; Özcan, M.; Souza, J.C.M. The Influence of Zirconia Veneer Thickness on the Degree of Conversion of Resin-Matrix Cements: An Integrative Review. Clin. Oral Investig. 2021, 25, 3395–3408. [Google Scholar] [CrossRef]
- Pace, L.L.; Hummel, S.K.; Marker, V.A.; Bolouri, A. Comparison of the Flexural Strength of Five Adhesive Resin Cements. J. Prosthodont. 2007, 16, 18–24. [Google Scholar] [CrossRef]
- Ilie, N.; Simon, A. Effect of Curing Mode on the Micro-Mechanical Properties of Dual-Cured Self-Adhesive Resin Cements. Clin. Oral Investig. 2012, 16, 505–512. [Google Scholar] [CrossRef]
- Saskalauskaite, E.; Tam, L.E.; McComb, D. Flexural Strength, Elastic Modulus, and PH Profile of Self-Etch Resin Luting Cements. J. Prosthodont. 2008, 17, 262–268. [Google Scholar] [CrossRef] [PubMed]
- Duymus, Z.Y.; Yanikoğlu, N.D.; Alkurt, M. Evaluation of the Flexural Strength of Dual-Cure Composite Resin Cements. J. Biomed. Mater. Res. B Appl. Biomater. 2013, 101B, 878–881. [Google Scholar] [CrossRef] [PubMed]
- Braga, R.R.; Cesar, P.F.; Gonzaga, C.C. Mechanical Properties of Resin Cements with Different Activation Modes. J. Oral Rehabil. 2002, 29, 257–262. [Google Scholar] [CrossRef] [PubMed]
- Par, M.; Spanovic, N.; Mohn, D.; Attin, T.; Tauböck, T.T.; Tarle, Z. Curing Potential of Experimental Resin Composites Filled with Bioactive Glass: A Comparison between Bis-EMA and UDMA Based Resin Systems. Dent. Mater. 2020, 36, 711–723. [Google Scholar] [CrossRef]
- Fujioka-Kobayashi, M.; Miron, R.J.; Lussi, A.; Gruber, R.; Ilie, N.; Price, R.B.; Schmalz, G. Effect of the Degree of Conversion of Resin-Based Composites on Cytotoxicity, Cell Attachment, and Gene Expression. Dent. Mater. 2019, 35, 1173–1193. [Google Scholar] [CrossRef]
- Arrais, C.A.G.; Giannini, M.; Rueggeberg, F.A. Kinetic Analysis of Monomer Conversion in Auto- and Dual-Polymerizing Modes of Commercial Resin Luting Cements. J. Prosthet. Dent. 2009, 101, 128–136. [Google Scholar] [CrossRef]
- Jang, Y.; Ferracane, J.; Pfeifer, C.; Park, J.; Shin, Y.; Roh, B. Effect of Insufficient Light Exposure on Polymerization Kinetics of Conventional and Self-Adhesive Dual-Cure Resin Cements. Oper. Dent. 2017, 42, E1–E9. [Google Scholar] [CrossRef]
- Egilmez, F.; Ergun, G.; Cekic-Nagas, I.; Vallittu, P.K.; Lassila, L.V.J. Light Transmission of Novel CAD/CAM Materials and Their Influence on the Degree of Conversion of a Dual-Curing Resin Cement. J. Adhes. Dent. 2017, 19, 39–48. [Google Scholar] [CrossRef]
- Flury, S.; Lussi, A.; Hickel, R.; Ilie, N. Light Curing through Glass Ceramics with a Second- and a Third-Generation LED Curing Unit: Effect of Curing Mode on the Degree of Conversion of Dual-Curing Resin Cements. Clin. Oral Investig. 2013, 17, 2127–2137. [Google Scholar] [CrossRef]
- Oliveira, M.; Cesar, P.; Giannini, M.; Rueggeberg, F.; Rodrigues, J.; Arrais, C. Effect of Temperature on the Degree of Conversion and Working Time of Dual-Cured Resin Cements Exposed to Different Curing Conditions. Oper. Dent. 2012, 37, 370–379. [Google Scholar] [CrossRef] [Green Version]
- Scotti, N.; Comba, A.; Cadenaro, M.; Fontanive, L.; Breschi, L.; Monaco, C.; Scotti, R. Effect of Lithium Disilicate Veneers of Different Thickness on the Degree of Conversion and Microhardness of a Light-Curing and a Dual-Curing Cement. Int. J. Prosthodont. 2016, 29, 384–388. [Google Scholar] [CrossRef] [PubMed]
- Aldhafyan, M.; Silikas, N.; Watts, D.C. Influence of Curing Modes on Conversion and Shrinkage of Dual-Cure Resin-Cements. Dent. Mater. 2022, 38, 194–203. [Google Scholar] [CrossRef] [PubMed]
- Bragança, G.F.; Vianna, A.S.; Neves, F.D.; Price, R.B.; Soares, C.J. Effect of Exposure Time and Moving the Curing Light on the Degree of Conversion and Knoop Microhardness of Light-Cured Resin Cements. Dent. Mater. 2020, 36, e340–e351. [Google Scholar] [CrossRef] [PubMed]
- Souza-Junior, E.J.; Borges, B.C.D.; Oliveira, D.C.R.S.; Brandt, W.C.; Hirata, R.; Silva, E.J.N.L.; Sinhoreti, M.A.C. Influence of the Curing Mode on the Degree of Conversion of a Dual-Cured Self-Adhesive Resin Luting Cement beneath Ceramic. Acta Odontol. Scand. 2013, 71, 444–448. [Google Scholar] [CrossRef] [PubMed]
- Passos, S.P.; Kimpara, E.T.; Bottino, M.A.; Santos, G.C.; Rizkalla, A.S. Effect of Ceramic Shade on the Degree of Conversion of a Dual-Cure Resin Cement Analyzed by FTIR. Dent. Mater. 2013, 29, 317–323. [Google Scholar] [CrossRef] [PubMed]
- Faria-e-Silva, A.L.; Pfeifer, C.S. Effectiveness of High-Power LEDs to Polymerize Resin Cements through Ceramics: An in Vitro Study. J. Prosthet. Dent. 2017, 118, 631–636. [Google Scholar] [CrossRef]
- Kelch, M.; Stawarczyk, B.; Mayinger, F. Time-Dependent Degree of Conversion, Martens Parameters, and Flexural Strength of Different Dual-Polymerizing Resin Composite Luting Materials. Clin. Oral Investig. 2022, 26, 1067–1076. [Google Scholar] [CrossRef]
- Yan, Y.L.; Kim, Y.K.; Kim, K.-H.; Kwon, T.-Y. Changes in Degree of Conversion and Microhardness of Dental Resin Cements. Oper. Dent. 2010, 35, 203–210. [Google Scholar] [CrossRef]
- Lanza, M.D.S.; Andreeta, M.R.B.; Pegoraro, T.A.; Pegoraro, L.F.; Carvalho, R.M.D. Influence of Curing Protocol and Ceramic Composition on the Degree of Conversion of Resin Cement. J. Appl. Oral Sci. 2017, 25, 700–707. [Google Scholar] [CrossRef]
- Rizzante, F.A.P.; Locatelli, P.M.; Porto, T.S.; Borges, A.F.S.; Mondelli, R.F.L.; Ishikiriama, S.K. Physico-Mechanical Properties of Resin Cement Light Cured through Different Ceramic Spacers. J. Mech. Behav. Biomed. Mater. 2018, 85, 170–174. [Google Scholar] [CrossRef]
- Shim, J.S.; Lee, S.Y.; Song, S.-Y.; Jha, N.; Ryu, J.J. Polymerization Efficiency of Dental Dual-Cured Resin Cement Light-Cured at Various Times after the Initiation of Chemical Activation. Int. J. Polym. Mater. Polym. Biomater. 2020, 69, 622–628. [Google Scholar] [CrossRef]
- Giannini, M.; Fronza, B.M.; Pecorari, A.; Gallego, V.; Price, R.B. Degree of Conversion of Luting Cements: Two Curing Protocols Compared. J. Adhes. Dent. 2019, 21, 450. [Google Scholar]
- Ilie, N. ISO 4049 versus NIST 4877: Influence of Stress Configuration on the Outcome of a Three-Point Bending Test in Resin-Based Dental Materials and Interrelation between Standards. J. Dent. 2021, 110, 103682. [Google Scholar] [CrossRef] [PubMed]
- Marovic, D.; Par, M.; Macan, M.; Klarić, N.; Plazonić, I.; Tarle, Z. Aging-Dependent Changes in Mechanical Properties of the New Generation of Bulk-Fill Composites. Materials 2022, 15, 902. [Google Scholar] [CrossRef] [PubMed]
- Szczesio-Wlodarczyk, A.; Rams, K.; Kopacz, K.; Sokolowski, J.; Bociong, K. The Influence of Aging in Solvents on Dental Cements Hardness and Diametral Tensile Strength. Mater. Basel Switz. 2019, 12, E2464. [Google Scholar] [CrossRef]
- Andrzejewska, E. Photopolymerization Kinetics of Multifunctional Monomers. Prog. Polym. Sci. 2001, 26, 605–665. [Google Scholar] [CrossRef]
- Gauthier, M.A.; Stangel, I.; Ellis, T.H.; Zhu, X.X. Oxygen Inhibition in Dental Resins. J. Dent. Res. 2005, 84, 725–729. [Google Scholar] [CrossRef]
- Par, M.; Gamulin, O.; Marovic, D.; Klaric, E.; Tarle, Z. Effect of Temperature on Post-Cure Polymerization of Bulk-Fill Composites. J. Dent. 2014, 42, 1255–1260. [Google Scholar] [CrossRef]
- Dickens, S.H.; Stansbury, J.W.; Choi, K.M.; Floyd, C.J.E. Photopolymerization Kinetics of Methacrylate Dental Resins. Macromolecules 2003, 36, 6043–6053. [Google Scholar] [CrossRef]
- Par, M.; Lapas-Barisic, M.; Gamulin, O.; Panduric, V.; Spanovic, N.; Tarle, Z. Long Term Degree of Conversion of Two Bulk-Fill Composites. Acta Stomatol. Croat. 2016, 50, 292–300. [Google Scholar] [CrossRef]
- Schroeder, W.; Vallo, C. Effect of Different Photoinitiator Systems on Conversion Profiles of a Model Unfilled Light-Cured Resin. Dent. Mater. 2007, 23, 1313–1321. [Google Scholar] [CrossRef] [PubMed]
- Aldhafyan, M.; Silikas, N.; Watts, D.C. Influence of Curing Modes on Monomer Elution, Sorption and Solubility of Dual-Cure Resin-Cements. Dent. Mater. 2022, 38, 978–988. [Google Scholar] [CrossRef] [PubMed]
- Raszewski, Z.; Nowakowska-Toporowska, A.; Nowakowska, D.; Więckiewicz, W. Update on Acrylic Resins Used in Dentistry. Mini Rev. Med. Chem. 2021, 21, 2130–2137. [Google Scholar] [CrossRef] [PubMed]
- Bolaños-Carmona, V.; Benavides-Reyes, C.; González-López, S.; González-Rodríguez, P.; Álvarez-Lloret, P. Influence of Spectroscopic Techniques on the Estimation of the Degree of Conversion of Bulk-Fill Composites. Oper. Dent. 2020, 45, 92–103. [Google Scholar] [CrossRef] [PubMed]
- Dimitriadi, M.; Petropoulou, A.; Zafiropoulou, M.; Zinelis, S.; Eliades, G. Degree of Conversion and Mechanical Properties of Modern Self-Adhesive Luting Agents. Appl. Sci. 2021, 11, 12065. [Google Scholar] [CrossRef]
- Dewaele, M.; Asmussen, E.; Peutzfeldt, A.; Munksgaard, E.C.; Benetti, A.R.; Finné, G.; Leloup, G.; Devaux, J. Influence of Curing Protocol on Selected Properties of Light-Curing Polymers: Degree of Conversion, Volume Contraction, Elastic Modulus, and Glass Transition Temperature. Dent. Mater. 2009, 25, 1576–1584. [Google Scholar] [CrossRef]
- Soh, M.S.; Yap, A.U.J. Influence of Curing Modes on Crosslink Density in Polymer Structures. J. Dent. 2004, 32, 321–326. [Google Scholar] [CrossRef]
- Par, M.; Marovic, D.; Attin, T.; Tarle, Z.; Tauböck, T.T. The Effect of Rapid High-Intensity Light-Curing on Micromechanical Properties of Bulk-Fill and Conventional Resin Composites. Sci. Rep. 2020, 10, 10560. [Google Scholar] [CrossRef]
- Schneider, L.; Moraes, R.; Cavalcante, L.; Sinhoreti, M.; Corrersobrinho, L.; Consani, S. Cross-Link Density Evaluation through Softening Tests: Effect of Ethanol Concentration. Dent. Mater. 2008, 24, 199–203. [Google Scholar] [CrossRef]
- Ferracane, J.L. Hygroscopic and Hydrolytic Effects in Dental Polymer Networks. Dent. Mater. 2006, 22, 211–222. [Google Scholar] [CrossRef]
- Blumer, L.; Schmidli, F.; Weiger, R.; Fischer, J. A Systematic Approach to Standardize Artificial Aging of Resin Composite Cements. Dent. Mater. 2015, 31, 855–863. [Google Scholar] [CrossRef] [PubMed]
- Szczesio-Wlodarczyk, A.; Sokolowski, J.; Kleczewska, J.; Bociong, K. Ageing of Dental Composites Based on Methacrylate Resins—A Critical Review of the Causes and Method of Assessment. Polymers 2020, 12, 882. [Google Scholar] [CrossRef] [PubMed]
- Par, M.; Spanovic, N.; Tauböck, T.T.; Attin, T.; Tarle, Z. Degree of Conversion of Experimental Resin Composites Containing Bioactive Glass 45S5: The Effect of Post-Cure Heating. Sci. Rep. 2019, 9, 17245. [Google Scholar] [CrossRef] [PubMed]
- Ilie, N.; Hilton, T.J.; Heintze, S.D.; Hickel, R.; Watts, D.C.; Silikas, N.; Stansbury, J.W.; Cadenaro, M.; Ferracane, J.L. Academy of Dental Materials Guidance—Resin Composites: Part I—Mechanical Properties. Dent. Mater. 2017, 33, 880–894. [Google Scholar] [CrossRef] [PubMed]
- Par, M.; Tarle, Z.; Hickel, R.; Ilie, N. Mechanical Properties of Experimental Composites Containing Bioactive Glass after Artificial Aging in Water and Ethanol. Clin. Oral Investig. 2019, 23, 2733–2741. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Material Type | Material Name | Manufacturer | Composition | Filler Load | Shade/ LOT No. |
|---|---|---|---|---|---|
| Dual-cure resin cement | Panavia V5 | Kuraray Noritake, Tokyo, Japan | Bisphenol A diglycidylmethacrylate, triethyleneglycol dimethacrylate, hydrophobic aromatic dimethacrylate, hydrophilic aliphatic dimethacrylate, initiators, accelerators, silanated barium glass, silanated alminium oxide, silanated fluoroalminosilicate glass, colloidal silica, camphorquinone, pigments | 61 wt%/ 38 vol% | Clear/6P0044 |
| Dual-cure resin cement | Variolink Esthetic DC | Ivoclar, Schaan, Liechtenstein | Urethane dimethacrylate, other methacrylate monomers, are ytterbium trifluoride, spheroid mixed oxide, initiators, stabilizers, pigments | 38 vol% | Neutral/Z029SK |
| Self-adhesive dual-cure resin cement | G-Cem ONE | GC, Tokyo, Japan | Fluoro-alumino-silicate-glass, urethane dimethacrylate, dimethacrylate, phosphoric ester monomer, silicone dioxide, initiators | 70 wt% * | Translucent/2106211 |
| Self-adhesive dual-cure resin cement | RelyX Universal | 3M, St. Paul, MN, USA | Bisphenol-A derivative free dimethacrylate monomers, phosphorylated dimethacrylate adhesion monomers, photoinitiator system, novel amphiphilic redox initiator system, radiopaque fillers and rheological additives, pigments | 52 wt% | TR/8275139 |
| Light-cure resin cement | Variolink Esthetic LC | Ivoclar, Schaan, Liechtenstein | Urethane dimethacrylate, other methacrylate monomers, are ytterbium trifluoride, spheroid mixed oxide, initiators, stabilizers, pigments | 38 vol% | Neutral/Z023VY |
| Factor | p-Value | Partial Eta-Squared |
|---|---|---|
| Material | <0.001 | 0.350 |
| Curing protocol | <0.001 | 0.072 |
| Post-cure time | <0.001 | 0.480 |
| Material × Curing protocol | <0.001 | 0.102 |
| Material × Time post-cure | <0.001 | 0.230 |
| Curing protocol × Time post-cure | 0.16 | N/A |
| Material × Curing protocol × Post-cure time | 0.88 | N/A |
| Factor | p-Value | Partial Eta-Squared | |
|---|---|---|---|
| Flexural strength | Material | <0.001 | 0.858 |
| Curing protocol | <0.001 | 0.268 | |
| Material × Curing protocol | <0.001 | 0.245 | |
| Flexural modulus | Material | <0.001 | 0.938 |
| Curing protocol | <0.001 | 0.700 | |
| Material × Curing protocol | <0.001 | 0.213 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Carek, A.; Dukaric, K.; Miler, H.; Marovic, D.; Tarle, Z.; Par, M. Post-Cure Development of the Degree of Conversion and Mechanical Properties of Dual-Curing Resin Cements. Polymers 2022, 14, 3649. https://doi.org/10.3390/polym14173649
Carek A, Dukaric K, Miler H, Marovic D, Tarle Z, Par M. Post-Cure Development of the Degree of Conversion and Mechanical Properties of Dual-Curing Resin Cements. Polymers. 2022; 14(17):3649. https://doi.org/10.3390/polym14173649
Chicago/Turabian StyleCarek, Andreja, Ksenija Dukaric, Helena Miler, Danijela Marovic, Zrinka Tarle, and Matej Par. 2022. "Post-Cure Development of the Degree of Conversion and Mechanical Properties of Dual-Curing Resin Cements" Polymers 14, no. 17: 3649. https://doi.org/10.3390/polym14173649
APA StyleCarek, A., Dukaric, K., Miler, H., Marovic, D., Tarle, Z., & Par, M. (2022). Post-Cure Development of the Degree of Conversion and Mechanical Properties of Dual-Curing Resin Cements. Polymers, 14(17), 3649. https://doi.org/10.3390/polym14173649